
Abstract
Background
Artificial intelligence (AI) is transforming healthcare delivery, particularly in psychiatric and addiction treatment. Enhancing nurses’ AI competence and perceptions is crucial for improving patient care and advancing AI-driven healthcare.
Aim
This study assessed the efficacy of an educational program aimed at improving nurses’ understanding and perceptions of AI in mental health and addiction services.
Methods
A quantitative quasi-experimental approach was employed, involving a purposive sample of nurses working in a psychiatric hospital in Jeddah, Saudi Arabia. The study included nurses from the psychiatric services department who met the inclusion criteria and agreed to participate. Data collection was conducted between February and April 2024 using three validated and reliable instruments: demographic, knowledge, and attitude questionnaires.
Results
The findings demonstrated the effectiveness of the intervention. Participants exhibited significant knowledge improvement, with post-knowledge scores increasing from 115.22 to 131.71. Additionally, a positive shift in attitudes was observed, with post-attitude scores rising from 72.61 to 83.31.
Conclusion
The intervention successfully enhanced nurses’ knowledge and attitudes, emphasizing the importance of continuous professional development to ensure high-quality care for patients with addiction and mental health issues.
Recommendations
Implementing similar interventions in other healthcare settings could further improve nurses’ AI-related knowledge and attitudes, ultimately enhancing the quality of care for patients with addiction and mental health conditions.
Keywords
Introduction
The integration of artificial intelligence (AI) in psychiatric healthcare offers transformative potential for enhancing patient outcomes, yet its success hinges on the competence and attitudes of psychiatric nurses globally. AI, defined as systems capable of performing tasks requiring human intelligence, 1 is increasingly utilized in mental health diagnostics, personalized therapy, and predictive analytics. However, nurses’ readiness to adopt AI remains inconsistent, influenced by disparities in training, infrastructure, and ethical concerns—a challenge echoed in diverse healthcare systems worldwide.2,3
Globally, psychiatric nurses face dual pressures: adapting to AI-driven tools like chatbots, virtual assistants, and electronic handover systems, 4 while addressing ethical dilemmas such as data privacy, accountability, and algorithmic bias. 5 For instance, studies in the UAE and Egypt highlight nurses’ limited AI knowledge and fears of job displacement, contrasting with European reports of improved care efficiency post-training.6,7 Similarly, Asian research underscores infrastructure gaps, where hospitals lack AI-compatible systems despite nurses’ openness to technology. 8 These disparities reflect a broader need for standardized, culturally sensitive AI education to bridge competence gaps and foster positive attitudes.
Psychiatric nurses’ unique role—combining clinical expertise with patient advocacy—positions them as critical stakeholders in AI integration. Their input ensures AI tools align with patient-centered care, mitigating risks of dehumanization. 9 For example, AI's ability to analyze speech patterns and physiological data can augment diagnostic accuracy, yet nurses’ interpretative skills remain vital to contextualize AI outputs. 10 International frameworks, however, lag in providing ethical guidelines, leaving nurses unprepared for AI-related challenges. 5
Educational interventions show promise in addressing these gaps. Quasi-experimental studies in Egypt demonstrated significant improvements in nurses’ AI knowledge and attitudes post-training, 7 while Jordanian programs revealed lingering skepticism about AI's ethical use. 11 Such mixed outcomes underscore the necessity of tailored, continuous learning initiatives that address both technical and ethical dimensions.
This study evaluates an educational program designed to cultivate AI competence and shape attitudes among psychiatric nurses in a resource-constrained setting. By aligning with global efforts to harmonize AI innovation with nursing practice, this research aims to inform strategies that empower nurses to navigate AI's evolving role, ultimately advancing mental healthcare delivery worldwide.
Conceptual foundation
This study integrates three complementary theoretical frameworks—Technology Acceptance Model (TAM), Competency-Based Education (CBE), and Psychological Empowerment Theory to systematically explore how AI proficiency shapes psychiatric nurses’ perspectives, job satisfaction, and patient care outcomes. The relationships between variables are mapped to the research aim of evaluating how educational interventions cultivate AI competence and attitudes (Figure 1).

Integrated theoretical framework.
Figure 1. The model illustrates how the educational intervention (independent variable) enhances AI proficiency (CBE), which subsequently influences nurses’ perceived ease of use and perceived usefulness (TAM) and fosters psychological empowerment. These factors collectively shape nurses’ perspectives on AI (dependent variable), job satisfaction, and patient care outcomes.
Grounded in CBE, AI proficiency—encompassing technical skills (e.g., interpreting AI-generated data) and ethical discernment (e.g., mitigating algorithmic bias)—serves as the foundational predictor variable, directly enhancing nurses’ confidence in utilizing AI tools. 11 This proficiency mediates the relationship between training and TAM constructs: perceived ease of use (simplicity) and usefulness (benefit), which act as critical mediators by reducing perceived complexity and amplifying perceived advantages of AI adoption (e.g., chatbots or diagnostic algorithms). 12 These TAM factors, in turn, foster psychological empowerment—defined by autonomy, competence, impact, and meaning—enabling nurses to autonomously integrate AI insights into personalized care plans while addressing ethical dilemmas. 13 Empowered nurses report higher job satisfaction and drive improved patient outcomes through ethically informed, AI-augmented practices (e.g., risk assessment tools), creating a reinforcing feedback loop where empowerment sustains positive attitudes toward AI. 14 For instance, a nurse trained in AI-driven tools (CBE) may perceive them as intuitive (TAM), advocate for AI-enhanced interventions (empowerment), and achieve greater job satisfaction due to reduced diagnostic delays and safer patient care. By interlinking these theories, the framework clarifies how training bridges technical-ethical competence, why empowered nurses embrace AI, and which mechanisms (e.g., autonomy, perceived usefulness) mediate AI's impact on mental healthcare delivery, ultimately aligning with the research aim of evaluating educational strategies to harmonize AI integration with nursing practice.
Significance of the study
This study addresses critical gaps in the global integration of AI within psychiatric nursing, a field pivotal to advancing mental healthcare yet underexplored in low-resource settings. While AI applications—such as predictive analytics, chatbots, and electronic health tools—are increasingly adopted in high-income countries (e.g., the US and EU) to enhance diagnostics and reduce workload,14,15 psychiatric nurses in resource-constrained regions remain underprepared due to inadequate training and infrastructure. 16 For instance, studies in the UAE and Jordan reveal nurses’ limited AI literacy and skepticism about ethical risks, such as data privacy breaches and algorithmic bias,17,18 while European interventions highlight improved care efficiency post-training. 19 This disparity underscores a global research gap: the lack of culturally adaptable frameworks to equip nurses with both technical competence and ethical discernment for AI use.
Psychiatric nurses’ roles extend beyond technical AI utilization; they are vital in contextualizing AI outputs (e.g., interpreting speech-pattern analyses or emotion-recognition algorithms) to preserve patient-centered care. 20 However, existing training programs, as noted in Egypt and South Korea, often prioritize technical skills over ethical preparedness, leaving nurses ill-equipped to navigate dilemmas like accountability for AI-driven errors. 21 This study directly responds to these gaps by evaluating an educational initiative that integrates technical AI proficiency (e.g., using diagnostic tools) with ethical decision-making (e.g., addressing bias in AI algorithms), tailored for a psychiatric hospital in a resource-limited context.
The aim of the study
To examine the effects of an educational intervention on developing artificial intelligence (AI) competence and shaping the attitudes of nursing professionals employed at Erada Complex for Mental Health and Addiction in Jeddah, Saudi Arabia.
Research questions
What are the participants’ levels of knowledge and attitudes related to artificial intelligence (AI) before and after the educational program?
What is the association between the demographic background of participants and the variables of knowledge and attitude related to artificial intelligence?
Hypothesis
Null Hypothesis (H₀): There is no statistically significant difference in artificial intelligence competence and attitudes toward artificial intelligence among psychiatric hospital nurses before and after the educational intervention.
Alternative Hypothesis (H₁): There is a statistically significant improvement in artificial intelligence competence and attitudes toward artificial intelligence among psychiatric hospital nurses after the educational intervention compared to before the intervention.
H2: There is a significant association between knowledge and attitude toward artificial intelligence among psychiatric nurses.”
Materials and methods
Research design
Quasi-experimental quantitative design was employed as a valuable tool particularly when traditional experimental methods are impractical or ethically challenging. Although these studies lack random assignment, they are specifically structured to assess interventions and establish causal relationships. As noted by Harris, 22 this approach often involves data collection before and after the intervention, sometimes incorporating control groups that are not randomly selected. Quasi-experimental designs allow researchers to examine causal relationships in settings where full experimental control is unattainable, providing a systematic framework for evaluating intervention impacts in real-world conditions.
Study setting
The investigation utilized data from the Erada Complex of Mental Health and Addiction in Jeddah, Saudi Arabia. This facility provides comprehensive addiction treatment, integrating medical, psychological, social, and religious methodologies. It also encompasses departments for treating psychiatric disorders. The institution comprised six inpatient units accommodating both male and female patients, offered outpatient services for adults and children, and maintained an emergency department.
Study participants
The study participants were selected through convenience sampling from nurses employed in psychiatric services at Eradah Complex for Mental Health and Addiction Hospital in Jeddah, affiliated with the Ministry of Health, Saudi Arabia. Participants who met the eligibility criteria and provided informed consent were included. The Reosoft program (www.reosoft.com) was employed to determine the sample size, based on a total population of 247 healthcare providers in the selected setting. A minimum of 151 participants was required, allowing for a 5% margin of error and a 95% confidence interval. The margin of error represented the acceptable level of imprecision, while the confidence interval indicated the permissible degree of uncertainty. The calculation also accounted for potential participant unavailability due to factors such as leave, illness, or refusal to participate.



where N is the population size, r is the fraction of responses that you are interested in, and Z(c/100) is the critical value for the confidence level c.
Study tools (data collection instruments)
To achieve the objective of the current study, three tools were utilized as follows:
This section inquired about participants’ age, marital status, years of experience, attendance at AI workshops, level of education, and gender, among other factors. Developed by Sabra.
23
The scale developed by the researchers of the current study through a comprehensive literature review comprises 30 statements designed for responses on a 5-point Likert scale, ranging from “Strongly Agree” (5) to “Strongly Disagree” (1). The instrument's primary objective is to evaluate the knowledge and awareness of psychiatric nurses concerning Artificial Intelligence (AI) within the domain of psychiatric nursing. The scale is structured into eight domains, encompassing AI's definition, its role in healthcare and psychiatric nursing, applications in psychiatric nursing, data analysis, patient data privacy and security, ethical considerations, AI in psychiatric assessment, types of AI, and AI's impact on patient behavior.
Scores on the scale can range from a minimum of 30 (if participants consistently select “1” for all statements) to a maximum of 150 (if participants consistently select “5”).
Scoring system for knowledge levels: Score ranges were determined through consensus among AI and psychiatric nursing experts, guided by best practices in Likert-scale interpretation.
24
Low knowledge (score 30–59): Indicates a very limited understanding of AI in psychiatric nursing, with a preference for lower Likert scale values. Moderate knowledge (score 60–89): Suggests a limited understanding of AI in psychiatric nursing, with a tendency towards lower Likert scale values. Good knowledge (score 90–119): Demonstrates a moderate understanding of AI in psychiatric nursing, with responses distributed across the Likert scale. Very good knowledge (score 120–150): Highlights an excellent comprehension of AI in psychiatric nursing, with a consistent selection of the highest Likert scale value (5) for all statements.
These knowledge levels provide insight into individuals’ familiarity and awareness of AI in psychiatric nursing based on their responses to the 30 assessment statements.
Validity and reliability
To ensure the validity of the developed scale, both content and face validity were evaluated through a thorough review by five nursing experts, whose feedback and suggestions were integrated into the final version.
2. The construct validity of the Psychiatric Nurses’ Knowledge of AI Scale was established through a detailed validation process as follows: An Exploratory Factor Analysis (EFA) was conducted to uncover the scale's structure, categorizing items into coherent dimensions. The Kaiser–Meyer–Olkin (KMO) measure and Bartlett's test of sphericity confirmed the data's appropriateness for factor analysis. Factors with eigenvalues greater than 1 were retained, and factor loadings above 0.40 were deemed acceptable. After EFA, Confirmatory Factor Analysis (CFA) assessed the proposed model using Structural Equation Modeling (SEM). Model fit was evaluated with indices such as the Comparative Fit Index (CFI > 0.90) and the Root Mean Square Error of Approximation (RMSEA < 0.08).
Convergent and discriminant validity were also evaluated. Convergent validity was confirmed by a positive correlation with established AI literacy assessments, with an Average Variance Extracted (AVE) exceeding 0.5. Discriminant validity was established by ensuring the square root of AVE was greater than inter-factor correlations, indicating the scale measures a distinct construct. Criterion-related validity was examined by comparing scores between psychiatric nurses with and without AI training (known-groups validity) and by assessing if higher scores predicted better performance in AI-integrated psychiatric care settings (predictive validity). The results support the scale's construct validity, demonstrating its effectiveness in assessing psychiatric nurses’ knowledge of AI.
Since Arabic is the primary language of the participants, the scale was translated and back translated to ensure accuracy. The Arabic version was then reviewed by a panel of nursing experts who provided additional suggestions for improvements. To assess reliability, a pilot study was conducted with 10% of participants to evaluate speech intelligibility and the time required to complete the questionnaire. The knowledge scale demonstrated high reliability and internal consistency, with a reported Cronbach's alpha coefficient of .887.3.
Attitude questionnaire towards artificial intelligence: (AI) scale assessing participants’ attitudes towards the use of AI in psychiatric practices. The scale was developed by Hussein et al. 23 developed. It uses 20 statements and is divided into five categories based on a five-point Likert scale, where 1 means completely agree, 2 means disagree, 3 means neutral, 4 means agree, and 5 means completely agree. After the cut of 60%, negative 60 means a negative attitude and positive 61 means a positive attitude. The validity and reliability of the tools have been confirmed by the lead developer. Regarding the reliability coefficient, the nurses’ attitude was also α=0.897, showing strong tool reliability. 26
Data collection process
The data collection commenced following the acquisition of official permission from the KAIMRC and IRB. An additional IRB No. (Ao1849) approval was obtained from the Ministry of Health, Jeddah, KSA. Subsequently, participants were invited to take part in the study through informational leaflets and concise discussions or explanations. Approval was sought from both the nurses and the manager of the Erada mental health complex, as well as the nursing managers for each ward.
The total number of nurses, 157, were divided into five groups: three groups of 31 nurses and two groups of 32 nurses.
Each nurse was assigned a code number for identification purposes. This code number was utilized for allocating participants to the pretest and was subsequently employed in the post-test.
The training was conducted by the PI and researchers involved in this study using PowerPoint presentations and handouts. The researchers, who also served as facilitators, implemented measures to control experimenter bias. These measures included completing the initial assessment on the completed questionnaire, reviewing the informed consent and IRB approval, and ensuring that participants in the experimental group brought their assigned code to the training sessions for data compilation.
The educational program
The educational intervention for artificial intelligence was implemented in three main phases as follows:
Phase one: Preparation of the program contents
Drawing from relevant literature on artificial intelligence research, the researchers conducted an extensive review of various dimensions of artificial intelligence to develop a comprehensive understanding. They subsequently designed the content for the intervention sessions, utilizing technology that facilitates the presentation of information, data, and visual aids during these sessions. Additionally, the researchers created informative flyers that were distributed to the participating nurses, serving as a self-learning guide. In collaboration with hospital administrators, the researchers identified a suitable location within the hospital premises for the educational intervention.
The researchers established an AI educational intervention for the study participants, following these outlined steps:
Setting program objectives
The general aim of the program is to enhance nurses’ knowledge and foster positive attitudes toward artificial intelligence by demonstrating its applications across various healthcare settings, including inpatient, emergency, and outpatient departments, with a particular focus on its role in psychiatric nursing care.
Phase two: Research implementation phase
The program was conducted by the researchers in the chosen settings. The participating nurses were divided into groups, and each session had specific goals and titles based on the content. The duration of the program was one group per day for approximately six weeks based on the nurses’ schedules and availability. Each training day consisted of four-hour sessions, with each session lasting 45–60 minutes. For afternoon and night shift nurses, online sessions were arranged, providing them with the same opportunity for training and asking questions.
The content was tailored to match the nurses’ comprehension level, available time, and the focus of the session. Uniform content was presented to all nurses, and various teaching methods were employed, including lectures, small group discussions, and the distribution of informative brochures and booklets.
A PowerPoint presentation supported the health education program, and nurses viewed videos via the provided links. Debriefings were conducted after viewing the videos to delve deeper into the content. Researchers offered guidance and facilitated discussions to help nurses gain knowledge and provide feedback. To encourage continued learning, visually engaging booklets with clear, concise information were distributed through scanned barcodes for all resources, which served as reference materials for nurses.
Each session commenced with a content summary and an explanation of the session's objectives, adjusting the language to align with the nurses’ understanding. Throughout the sessions, positive reinforcement methods, including praise, were utilized to promote active participation and enhance the learning experience.
Program structure and content overview
The educational initiative was designed to be thorough and adaptable, enabling nurses to keep pace with the evolving landscape of AI in psychiatric care. By blending theoretical knowledge with hands-on skills, the program aimed to equip nurses with the confidence and ethical understanding needed to utilize AI for improved patient care and outcomes. The curriculum covered a wide array of topics to ensure nurses were well-prepared to incorporate AI into their daily practice.
Session 1: AI fundamentals in healthcare and psychiatric nursing
AI's role and importance in healthcare. 27
Study introduction and goals.
AI-related ethical and legal issues. 28
Session 2: AI applications in psychiatric nursing
Specific AI tools for psychiatric care. 29
Mental health applications of chatbots, predictive analytics, and data analysis. 30
Session 3: Building AI competencies
Developing practical AI skills for patient assessment and care. 31
AI-assisted psychiatric evaluation. 32
Session 4: AI in pharmacology and genomics
AI applications in medication selection, dosing, and personalized treatment. 33
Genetic testing's role in psychiatric care. 34
Session 5: AI-enhanced communication and patient-centered care
Effectively communicating AI-based assessments and interventions to patients. 35
Maintaining patient-focused care while integrating AI technologies. 36
Session 6: Addressing challenges and ethical considerations
Tactics for overcoming resistance to AI adoption among psychiatric nursing staff. 37
Ethical guidelines and best practices for AI integration. 38
Phase three: conclusion and evaluation
To conclude, participants were asked to provide program feedback and complete post-test questionnaires.
Data management and analysis plan
The collected data were coded and analyzed using the latest version of the statistical software SPSS. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were calculated to summarize the data. Independent sample t-tests were conducted to compare the item means of knowledge evaluation between the pre- and post-program assessments among study participants. Additionally, paired t-tests were performed to analyze the changes in total knowledge and attitudes scores within the participants’ responses from the pre-test to the post-test. The Spearman test was employed to assess the association between the participants’ sociodemographic variables and the study variables, with a significance level set at P < .05.
Results
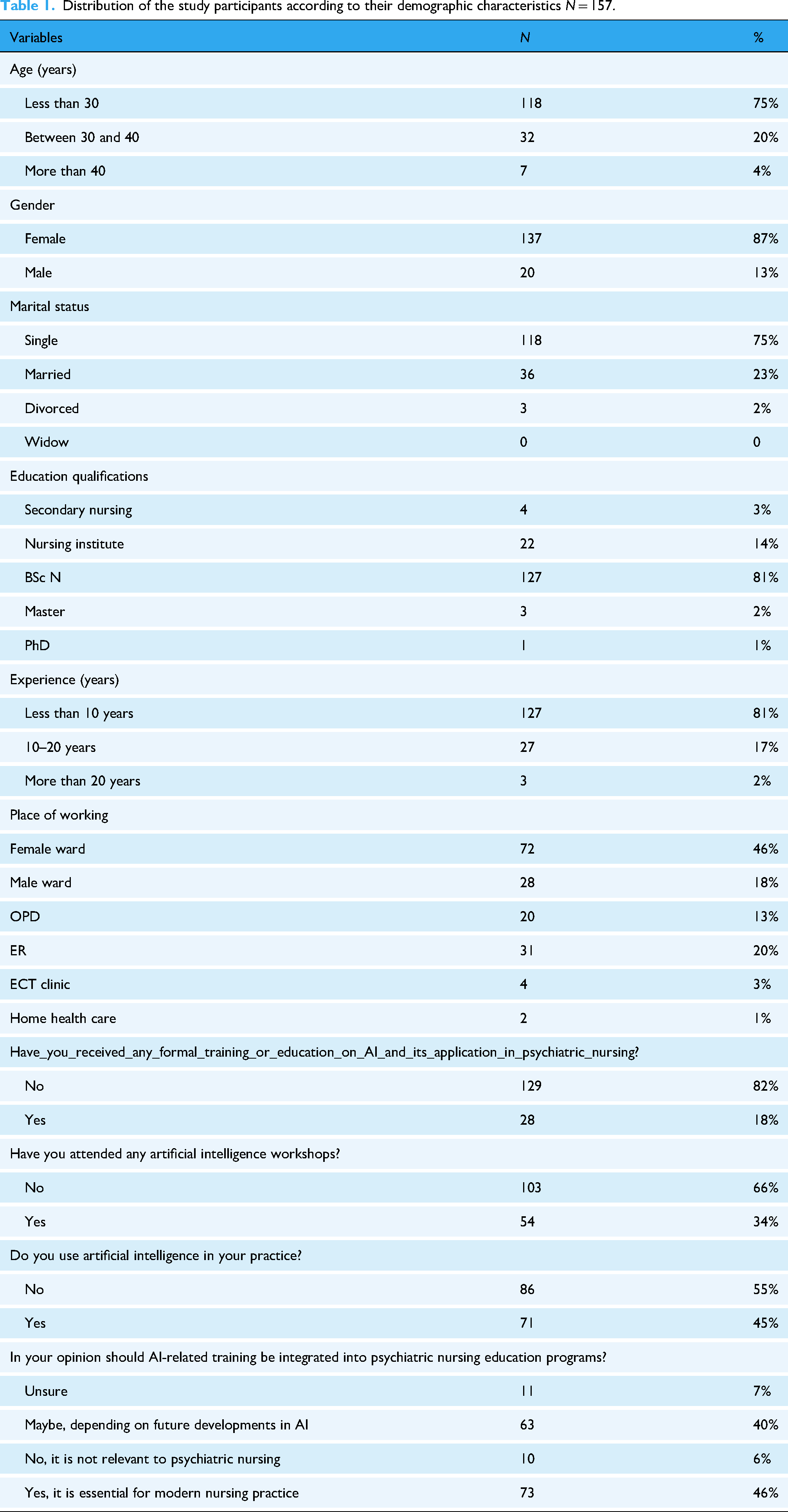
Table 1 displays the demographic distribution which indicates that a significant portion of the participants are younger than 30 years, making up 75% of the group, with a notable majority being female at 87%. A large number are single, accounting for 75%, and most possess a Bachelor of Science in Nursing, which represents 81% of the participants. Additionally, a considerable share has less than a decade of experience in the field, also at 81%. The predominant workplace for these individuals is in female wards, comprising 46% of the total. Interestingly, a vast majority have not undergone formal training or education regarding AI in psychiatric nursing, with 82% lacking this background, and 66% have not participated in AI workshops. Nevertheless, almost half of the respondents, 45%, are currently utilizing AI in their professional practice. Furthermore, a strong majority, 46%, advocate for the inclusion of AI training in psychiatric nursing education, underscoring the growing recognition of AI's role in contemporary nursing.
Distribution of the study participants according to their demographic characteristics N = 157.
As illustrated in Table 2, the intervention led to significant improvements in participants’ understanding, particularly regarding the concept that “AI is a field focused on creating intelligent machines.” The percentage of respondents who strongly agreed with this statement increased dramatically from 29.3% pre-intervention to 65% post-intervention, indicating a substantial enhancement in comprehension of this key concept. However, some areas showed only marginal gains. For instance, the statement “Support Groups and Peer Counseling AI applications connect individuals with similar mental health experiences” saw an increase in strong agreement from 28% to 55.4%. Similarly, the notion that “AI's primary purpose is making predictions and decisions” experienced a modest uptick from 30.6% to 51.6%, while agreement with the statement “Narrow or Weak AI is task-specific” rose from 27.4% to 50.3%. These specific topics may require additional emphasis in future educational programs to ensure a more thorough understanding.
Distribution of studied participants on the knowledge scale pre- and post-intervention program N = 157.

Table 3 displays a significant shift in participants’ attitudes toward artificial intelligence (AI) after an educational program. The percentage of respondents who strongly agreed that “Technical Artificial Intelligence can create new economic opportunities” jumped from 29.9% to 53.5% post-intervention, indicating a substantial positive shift in perspective. Similarly, those who strongly concurred with the statement “I would like to utilize Artificial Intelligence in my work” increased from 29.3% to 52.9%, while strong agreement with “Artificially intelligent systems can enhance Nurses’ happiness” rose from 26.1% to 54.8%. Moreover, negative perceptions decreased; for instance, strong agreement with “AI is dangerous” dropped from 21.7% to 45.2% after the intervention, and those strongly agreeing “AI can positively impact nurses’ well-being” increased from 26.1% to 56.7%. These results suggest that the educational program effectively promoted more positive views of AI while diminishing apprehensions about its impact on both professional and personal spheres.
Distribution of studied participants according to their attitude scale in pre- and post-intervention N = 157.

The bar chart (Figure 2) illustrates the variations in the knowledge and attitudes of participants before and after an educational intervention focused on artificial intelligence in psychiatric nursing, involving a total of 157 individuals. The data reveals a significant enhancement in both knowledge and attitudes after the intervention. Specifically, the average knowledge score improved from 115.2 before the intervention to 131.8 afterward, indicating a marked advancement. Likewise, the attitude score experienced an increase from 72.6 to 83.3 post-intervention. This upward trajectory in both areas underscores the success of the educational intervention in improving participants’ comprehension and viewpoints regarding the use of AI in psychiatric nursing.

Difference between participants’ knowledge, and attitudes score pre- and post-educational initiatives N = 157.
Table 4 shows a strong positive correlation between pre-knowledge and pre-attitude scores (r = .861, P < .001) and between post-knowledge and post-attitude scores (r = .777, P < .001), indicating that higher knowledge levels are associated with better attitudes both before and after the intervention. Additionally, there is a modest correlation between pre-knowledge and post-knowledge scores (r = .177, P = .027), as well as between pre-attitude and post-attitude scores (r = .223, P = .005). The weak correlation between pre-knowledge and post-attitude scores (r = .055, P = .491) suggests minimal direct influence, highlighting that significant improvements in attitudes occur after the intervention as knowledge increases.
Pearson correlation between knowledge and attitudes in pre- and post-intervention N = 157.

*Correlation is significant at the 0.05 level (2-tailed).
**Correlation is significant at the 0.01 level (2-tailed).
Table 5 compares scores before and after an intervention, focusing on knowledge and attitudes regarding AI in psychiatric nursing. The findings reveal a notable enhancement in knowledge, with average scores increasing from 115.2 ± 23.4 to 131.7 ± 18.7 following the intervention (t = 88.1, P = .001). The magnitude of improvement in knowledge is considerable, with the effect size growing from 4.9 pre-intervention to 7 post-intervention, suggesting a powerful impact of the educational program. Likewise, attitude scores showed significant improvement, with mean values rising from 3.6 ± 0.75 to 83.3 ± 14.7 after the intervention (t = 70.8, P = .001). The effect size for attitude also exhibited a substantial increase from 4.8 to 5.6, indicating a meaningful shift in participants’ perspectives toward AI following the educational initiative. These outcomes demonstrate the efficacy of the intervention in significantly enhancing both knowledge and attitudes concerning AI in the field of psychiatric nursing.
Comparison between pre- and post-intervention in relation to participants’ knowledge and attitudes with the effect size N = 157.

Table 6 offers a comprehensive examination of how an educational program influenced knowledge and perceptions of AI in psychiatric nursing across various demographic groups. Significant knowledge enhancements were noted after the intervention among those with prior AI education or training (P = .001), with average knowledge scores increasing from 109.92 ± 21.71 to 139.32 ± 17.58. Similarly, AI workshop attendees showed considerable knowledge improvements, with scores rising from 109.35 ± 23.50 to 132.81 ± 17.25 (P = .001). Gender analysis revealed that males experienced a significant increase in knowledge post-intervention (P = .039), though attitude changes were not statistically significant (P = .205). The intervention's effectiveness was consistent across experience levels, as participants with varying years of service showed no significant differences in knowledge or attitude improvement. However, clinical placement in specific areas, such as the ECT clinic, resulted in notable attitude improvements towards AI, with mean scores increasing from 66.75 ± 16.99 to 83.00 ± 17.64 (P = .005). Participants who integrated AI into their work demonstrated significant knowledge gains (P = .001), emphasizing the role of practical application in enhancing understanding. Furthermore, those who considered AI training crucial for contemporary nursing practice exhibited significant increases in both knowledge and attitude scores, with P values of 0.001 and 0.003, respectively. These results highlight the positive effects of targeted educational interventions on improving AI-related knowledge and attitudes in psychiatric nursing, with a total of nine significant changes observed across different variables.
Correlation between participants’ knowledge and attitudes with their demographic characteristics in pre- and post-intervention (N = 157).

Discussion
This research marks a groundbreaking initiative in the realm of psychiatric nursing in Saudi Arabia, aiming to assess the effects of an educational program on nurses’ understanding and perceptions of artificial intelligence (AI). The findings revealed notable enhancements in both knowledge (mean score: 115.2 before the intervention compared to 131.7 afterward) and attitudes (72.61 vs. 83.3), underscoring the effectiveness of structured AI training programs. These results add to the expanding conversation on AI literacy in healthcare, aligning with Hasan et al. 39 while also presenting nuanced challenges to Sabra et al. 40 previous studies.
Concerning the Knowledge Gaps and Post-Intervention Improvements, initial results indicated that most psychiatric nurses possessed limited knowledge about AI's role in nursing tasks such as diagnosis, planning, and assessment. This closely mirrors the findings of Castagno and Khalifa, 41 where healthcare workers expressed concerns about AI-induced job loss and showed an incomplete grasp of AI concepts. However, our post-intervention outcomes differed significantly: nurses displayed enhanced knowledge scores, indicating that focused education can alleviate fears and close knowledge gaps. This contradicts Castagno and Khalifa's 41 assertion that fear persists due to insufficient training opportunities, highlighting the importance of structured interventions in changing perceptions.
Similarly, our results partially align with Hussain et al.'s 42 observation of mixed opinions among nurses in Jeddah, where some feared job loss while others recognized AI's advantages. After the intervention, our group showed a stronger agreement on AI's positive impact (e.g., 80% agreeing AI enhances job satisfaction and reduces errors), reflecting Sabra et al. 43 and Mohammed et al., 44 who noted improved AI literacy and acceptance following training programs. This consistency emphasizes the universal benefit of educational interventions in promoting AI readiness among nurses.
Regarding Attitudes Toward AI Balancing Optimism and Concerns, post-intervention attitudes showed strong optimism: over 80% of nurses agreed AI could boost job satisfaction, lessen workloads, and create economic opportunities. These findings resonate with Sabra et al., 43 who found nurses believed AI could decrease medical errors and enhance clinical data quality, and with Jiang et al., 45 who highlighted AI's transformative potential in healthcare. However, our study also identified ongoing concerns about workforce displacement and ethical risks, echoing the Royal Society Working Group's 46 report on public ambivalence toward AI. This duality reflects a broader tension in healthcare: enthusiasm for AI's efficiency gains coexists with anxiety about its societal impact. Interestingly, our findings differ from those of Abuzaid et al. 47 in Sharjah, where nurses predominantly engaged in self-directed learning (51%) over formal training (20%). In contrast, our group primarily utilized workshops and online resources, indicating regional differences in AI education infrastructure. This variation underscores the necessity for tailored strategies to improve AI literacy. Regarding Demographic Influences and AI Competency, gender was a significant predictor of post-intervention knowledge scores, consistent with Sabra et al., 43 who identified gender-based differences in AI perceptions. However, unlike Elsayed and Sleem, 48 who found that occupational roles and seniority affected attitudes, our study showed no significant correlation with age and experience. This inconsistency may be due to cultural or institutional variations in training accessibility. The notable difference in pre-knowledge scores between nurses who used AI and those who did not (P < .05) supports Shiners et al.'s 49 claim that practical experience enhances competency. This also builds on Trivedi et al.'s 50 research on AI's diagnostic utility by illustrating its impact on nurses’ confidence and attitudes. Furthermore, concerning the Broader Implications, the current study corroborates Hussain et al.'s 43 finding that educational programs improve AI knowledge, while also offering new insights: even short interventions can transform attitudes from skepticism to cautious optimism. This challenges Castagno and Khalifa's 42 pessimistic view, suggesting that fear of AI arises from limited exposure rather than inherent dangers.
Limitations
Although the results of the study yield significant insights into the understanding, and perspectives, of psychiatric nurses in Saudi Arabia concerning artificial intelligence technologies, which could guide forthcoming educational strategies and policies aimed at facilitating the proficient integration of AI in psychiatric care, it is imperative to acknowledge these limitations:
The quasi-experimental framework, while pragmatic, lacks the rigor associated with a randomized controlled trial, which may hinder the capacity to definitively correlate the educational intervention with the observed alterations in knowledge, attitudes, and perceived challenges. The study's confinement to a single-site location in Jeddah, Saudi Arabia may impose constraints on the external validity of the findings concerning other psychiatric care environments and geographical contexts. Furthermore, although the sample size was adequate, it may be influenced by participant attrition or non-response, thereby impacting the statistical power and the capacity to identify significant associations. The dependence on self-reported data from the nursing participants carries the risk of response biases, including social desirability bias, notwithstanding the application of standardized measurement tools.
Conclusions
The educational intervention demonstrated significant efficacy in enhancing psychiatric nurses’ knowledge, attitudes, and confidence regarding the application of artificial intelligence (AI) in daily practice. Nurses in the intervention group reported reduced difficulty in AI implementation and acknowledged its potential to augment and enhance clinical decision-making, resulting in a more comprehensive understanding of its benefits for patient care. This study underscores the crucial role of education in addressing knowledge deficits and negative attitudes that frequently impede the integration of AI into psychiatric practice. By mitigating these barriers, the intervention facilitated AI adoption, positioning it as a valuable tool for optimizing work processes and improving patient outcomes in psychiatric care.
Recommendations of the study
Implement a comprehensive educational initiative comprising workshops and training courses to enhance psychiatric nurses’ understanding and utilization of AI in practice. The program should encompass AI fundamentals, applications in psychiatric care, data privacy, ethical considerations, and practical skills for utilizing AI-based tools and decision support systems.
To address the challenges and concerns, the training should focus on fostering positive attitudes by emphasizing AI's potential benefits, such as improved diagnostic accuracy, personalized treatment, and enhanced decision-making. Addressing ethical issues and providing guidance on mitigating risks may help reduce resistance.
Collaboration between psychiatric nurses, AI experts, and healthcare providers should be encouraged to bridge gaps in AI expertise and develop resources, guidelines, and tools for effective, ethical AI utilization. Ongoing research and pilot projects should be promoted to provide insights into successful AI integration, with continuous evaluation to refine the programs and address emerging challenges.
Nursing implications
The research results provide several crucial nursing implications that can enhance practice, patient care, and the incorporation of artificial intelligence (AI) in psychiatric nursing:
The study emphasizes the necessity for continuous education to boost nurses’ technical proficiency, as increasing their AI knowledge and confidence will better equip them to utilize AI tools effectively. This will enhance their capacity to evaluate, diagnose, and manage psychiatric conditions more accurately. Integrating AI into nursing practice can result in more individualized and evidence-based care. Nurses trained in AI can harness these tools for precise care planning and treatment interventions, thereby improving patient outcomes and delivering more customized, patient-focused care. The research underlines the significance of addressing nurses’ perspectives on AI. Educational interventions can promote greater acceptance and willingness to adopt new technologies by highlighting AI's benefits in clinical decision-making and alleviating nurses’ concerns, leading to smoother transitions in clinical practice. As AI technologies become more widespread, nurses must be cognizant of ethical considerations and data privacy issues. The study's recommendations emphasize the need for training that covers these areas, helping nurses practice safely while safeguarding patient confidentiality and adhering to legal and ethical standards. Interdisciplinary Collaboration: The study accentuates the importance of collaboration between nurses, AI specialists, and other healthcare providers. This approach can enhance nurses’ ability to incorporate AI into their practice by cultivating a supportive environment where they can seek guidance and exchange knowledge, ultimately improving patient care quality. Ongoing education on AI can enhance nurses’ adaptability to future technological advancements, creating a more resilient nursing workforce better equipped to meet evolving healthcare demands. This continuous professional development can help maintain high standards of care in psychiatric nursing practice.
Through the implementation of these nursing implications, healthcare institutions can foster a workforce that is not only proficient in artificial intelligence but also equipped to utilize these technological advancements to deliver safe, efficient, and patient-centered psychiatric care.
Footnotes
Acknowledgments
The authors express their sincere gratitude to the administration and nursing staff of the psychiatric hospital for their valuable participation and support throughout this study. Furthermore, we acknowledge the expert guidance and insights provided by the research unit teams at King Saud bin Abdulaziz University for Health Sciences, whose contributions were instrumental in the successful completion of this project.
Ethical Considerations
This proposal went through a rigorous approval process starting with KAIMRC and the Institutional Review Board (IRB SP23J-166-11). Subsequently, a second IRB approval was obtained from the Ministry of Health in KSA, Jeddah, which then forwarded the approval directly to the Erada Complex for Mental Health and Addiction (a mental health service provider) to facilitate the data collection process. The research team emphasized ethical considerations, including securing informed consent, protecting participant privacy, and minimizing potential harm. They strive to obtain IRB approval and ensure that the potential benefits of the research far outweigh the risks involved. Throughout the study, researchers respect participants’ autonomy, handle data responsibly, and accurately report their results. In addition, the possibility of offering post-study support to participants was considered. All documents related to data collection were stored securely at the MNGHA premises. By steadfastly adhering to these ethical principles, the research maintained its integrity and upheld ethical behavior both now and, in the future,
Consent to Participate
All participants provided written informed consent after receiving a detailed explanation of the study's objectives and procedures. No adverse effects or unintended consequences were reported during this study.
Author Contributions
AIK contributed to conceptualizing, methodology, writing the original and final draft, data collection, data entry, and editing the manuscript. JB, DA, RA, RA, and MH contributed to writing the original and final draft, data collection, and data entry. AIK contributed to data analysis, curation, and results.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Further data is available from the corresponding author on reasonable request.