
Abstract
Objective
Depression is a major challenge for many people and societies, also accelerated by the COVID-19 pandemic. Around 300 million people worldwide are affected by a depressive disorder. Health insurances encourage patients to use applications (“apps”) to tackle, for example, mild and moderate depression. The advantages of these depression apps are well understood, but their dissemination and adoption rates among intended users leave room for improvement. To enhance their uptake, we provide a holistic view regarding critical design aspects of depression apps and develop design principles (DPs) for depression apps.
Methods
We use a qualitative approach with 58 semistructured interviews between March 2021 and August 2022 with different stakeholders (healthcare providers, patients with mild and moderate depression, app developers and operators, and health insurance companies) to derive our DPs to provide a holistic view of the crucial design factors of depression apps. We then evaluated our DPs derived from four individuals from the health sector in terms of appropriateness and completeness.
Results
Following this approach, we examine seven meta-requirements (MRs) like “quality” and “simplicity” to deduce 16 corresponding DPs for depression apps. Our prescriptive design knowledge enables us to carve out interrelations and contributes to the literature on depression app design knowledge. Generally, our MRs and DPs derived were evaluated positively.
Conclusions
Our research ignites a structured discussion among stakeholders in the healthcare sector, for example, scientists and practitioners, about the importance of specific design aspects of depression apps and the overall development process from planning to dissemination.
Introduction
About 300 million people worldwide are affected by a depressive disorder. 1 Accordingly, depression is a major challenge for many people, affecting their lives, social participation, and quality of life.2,3 The COVID-19 pandemic has further increased the global burden. As a result, the prevalence of depression has increased by 28% on average. 4 One problem with managing depressive disorders is the long waiting time for treatment. Because of insufficient capacity, patients seeking help have to wait many weeks for an appointment for an initial consultation with a psychotherapist. In Germany, for example, the waiting time is about 3 weeks until the initial consultation and another 20 weeks until the start of therapy. 5 This also requires asking different therapists for appointments, which can burden individuals. 6
Against this backdrop, health insurance today encourages using and deploying Information Technology (IT) to tackle mild and moderate depression. Patients are encouraged to use applications (“apps”) to support—or in some cases to replace—face-to-face depression therapies to provide leverage effects and to bridge long waiting times. 7 These self-help interventions are delivered through mobile and web apps on patients’ smartphones, tablets, and computers. Unless the advantages and functionalities of these depression apps (For the case of clarity, we use the collective term “depression apps” or “apps for depression” to include all web and mobile apps that deliver healthcare interventions for mild or moderate depression through a web and/or a mobile app.) are understood from a theoretical point of view,8,9 the use and deployment of such apps, for example, in Germany, leave room for improvement. 10 Characteristics, contents, similarities, and differences, that is, design patterns, of depression apps have already been studied, 9 for example, through taxonomic approaches, 11 acceptance research, 12 or market observations. 13 Depression apps are equipped with various functions such as self-monitoring of health data, disease detection, or remote monitoring systems.9,14 However, an interdisciplinary, holistic view, including all stakeholders’ opinions regarding the design and structure of depression apps that could enhance the dissemination, is still missing and is proposed as a research avenue, for example, by Mayer et al. 15 Also, the pre-requisite for successful mobile medical app development is the integration of developers and medical professionals. It can lead to more appropriate digital solutions that better fit the stakeholders’ needs. 14 Those stakeholders include patients, healthcare professionals, health insurance, and developers since they are involved in the overall lifecycle of depression apps, that is, from their development to their dissemination to their usage.
Research regarding indication-specific, that is, depression-specific, design principles (DPs) is scarce. Kenny et al. 16 establish specific DPs for developing health apps. These principles are for apps that elderly patients with age-related macular degeneration can use. Based on previous research, they derive four DPs, that is, the appropriate interface for the target group or the integration of the application into the routine of patients and physicians. However, they are not tailored to the depression-specific context. On a more general view, Mathews et al. 17 focus on the validation of digital health solutions and provide a framework to guide the evolution of general health apps. Also, Murray et al. 18 design an evaluation strategy to support the development and deployment of digital health apps. Their research concerns the quality and effectiveness of digital health implications rather than specific design features. Most recently, a study by Wierenga et al. 19 examined specific design aspects of mobile apps for peripartum depression. Their mixed-methods approach reveals that fewer survey moments, more reminders, and a need for more unique content compared to commercially available apps are crucial for app design in the special case of peripartum depression.
To sum up, past research was mainly concerned with the characteristics and functionalities of depression apps with different methodologies like randomized control trails and focused, for example, on acceptance 20 or medical 21 results on dedicated stakeholder groups. However, to our knowledge, studies would need to incorporate the views of various stakeholder groups and synthesize them into DPs, since the literature agrees that this would be beneficial. We have not found such a study so far. It is well known that design features are important to improve app adoption and encourage usage in a healthcare context. 22
Consequently, we systematically examine crucial design factors, that is, meta-requirements (MRs) from interviews with relevant stakeholders, and identify a representative set of the most important DPs for depression apps. Based on 58 stakeholder interviews, the prescriptive collected design knowledge enables us to deduce design patterns, an established strategy in Information Systems Research. It carves interrelations within a design phenomenon and contributes to depression apps’ design knowledge production.23,24,25,26 Practitioners, for example, project managers or developers, can use our derived DPs as actionable, straightforward advice, and focus on what is most important to consider for developing and disseminating depression apps successfully. As a result, this can reduce development costs and lower the complexity of the overall development process.27,28,29 This process can be made more stakeholder-centric since it aims to develop depression apps that suit the needs and interests of the intended stakeholders. Based on these motivations, we address the research question (RQ):
“What are the critical design principles for successful depression app development?”
To answer our RQ, we follow the well-established Design Science Research (DSR) methodology proposed by Peffers et al. 30 Our problem-centered initiation procedure examines important DPs, that is, artifacts for depression apps that can help deliver better services to tackle mild and moderate depression. To construct DPs, we use qualitative data, qualitative content analysis techniques, 29 and recent DP construction guidelines. 24 We discussed our DPs with scientists and practitioners to evaluate and iterate our findings according to the different evaluation criteria31,32 and examine the usefulness of our artifacts.
The rest of this article is structured as follows: first, we provide theoretical foundations on apps for depression and the importance of their design. Then, we describe our methodology and data collection. We present and discuss our MRs and DPs subsequently and discuss implications and contributions for theory and practice. Lastly, we provide limitations, future research directions, and concluding remarks.
Methods
We deduce theoretically grounded and empirically examined MRs, DPs, and their interrelations to guide the design and development of depression apps as the ultimate goal of our research. We build on the structured approach of DSR studies proposed by Peffers et al. 30 We use a problem-centered initiation as an entry point in our research inquiry. The definition of the problem and its importance are shown in the first section of this article and further elaborated in our theoretical foundation section. The motivation for this article arises from the observation that despite the great burden of depressive disorders, there is low use of apps for depression. This reveals major problems and unused opportunities in the (non-)usage of these apps. Consequently, the RQ conceptualizes crucial design factors to develop a useful and successful solution, that is, an app for depression. In the second step, according to Peffers et al., 30 we define the objectives of the solution. Our MRs and DPs can be used to develop and establish depression apps more successfully. DPs can be interpreted as meta-artifacts that belong to the type of theory for design and action. 33 As meta-artifacts, they enable the categorization of design knowledge and make it reusable in different applications. 24 In our case, DPs enable knowledge reuse for, for example, developers, potential investors, or project management to allow efficient and successful IT-based services for depression through stakeholder-oriented apps. 24 Also, DPs are intended to improve the quality of already existing apps. 24 Led by current research on the functionalities of depression apps and e-health and m-health apps, we initiated the next stage of the DSR methodology process model.
To examine MRs and construct crucial DPs, we use a qualitative approach within the third stage of the procedure model by Peffers et al. 30 Interviews with different stakeholders will help to derive our DPs to provide a holistic view of the crucial design factors of depression apps. Existing and well-established procedures for DP generation guide our DPs deduction. According to Gregor et al., 24 a complete design principle specifies the goal, context, and mechanism (including rationale, if appropriate). In addition, it considers the role of the stakeholders in the relationships between these elements, which will be discussed in later sections. Our interviews were conducted with an interview guideline with four main question blocks, namely (a) (non-)successful functionalities, (b) design elements of depression apps, (c) depression apps’ general relevance for a healthcare system, and (d) an outlook on the topic. Our question blocks were inspired by examining related literature on depression apps, their design aspects and functionalities, and possible acceptance factors for such artifacts’ (non-)usage. With the usage of (semi-)open questions within the interview guidelines, we avoid potential response biases in the interview situations. 34 Also, this literature review allowed us to go into the field with basic knowledge about the research area. 35 Interview guidelines were slightly adapted for the specific stakeholder group since practitioners and patients with mild or moderate depression show different levels of knowledge on the topic. The interview guidelines were pretested with (post-)doctoral students regarding the understandability of the questions. We recruited interview partners through our research and professional networks, e-mail, or relevant social media. Interviews were conducted online and/or face-to-face (in Lower-Saxony, Germany) with healthcare providers and health insurance companies. Patients with mild and moderate depression were interviewed within the locations of the Hanover Medical School in Hanover, Lower-Saxony, Germany. App developers were interviewed online with Webex. Our data collection occurred between March 2021 and August 2022 and was saturated as no new topics emerged from new interview situations. In total, we conducted 58 (n = 58) interviews among 21 (n = 21) healthcare providers that can be divided into four subgroups: patients with mild or moderate depression (n = 19), app developers and operators (n = 10), and health insurance companies (n = 8). With our purposive sampling technique to avoid potential sampling biases, we made sure that we received meaningful responses to answer our RQ. 34 With this composition of the collection of different stakeholders’ opinions, we received a holistic view of the chances and challenges that arise with depression apps. Table 1 summarizes our data collection and composition:
Data collection and composition.
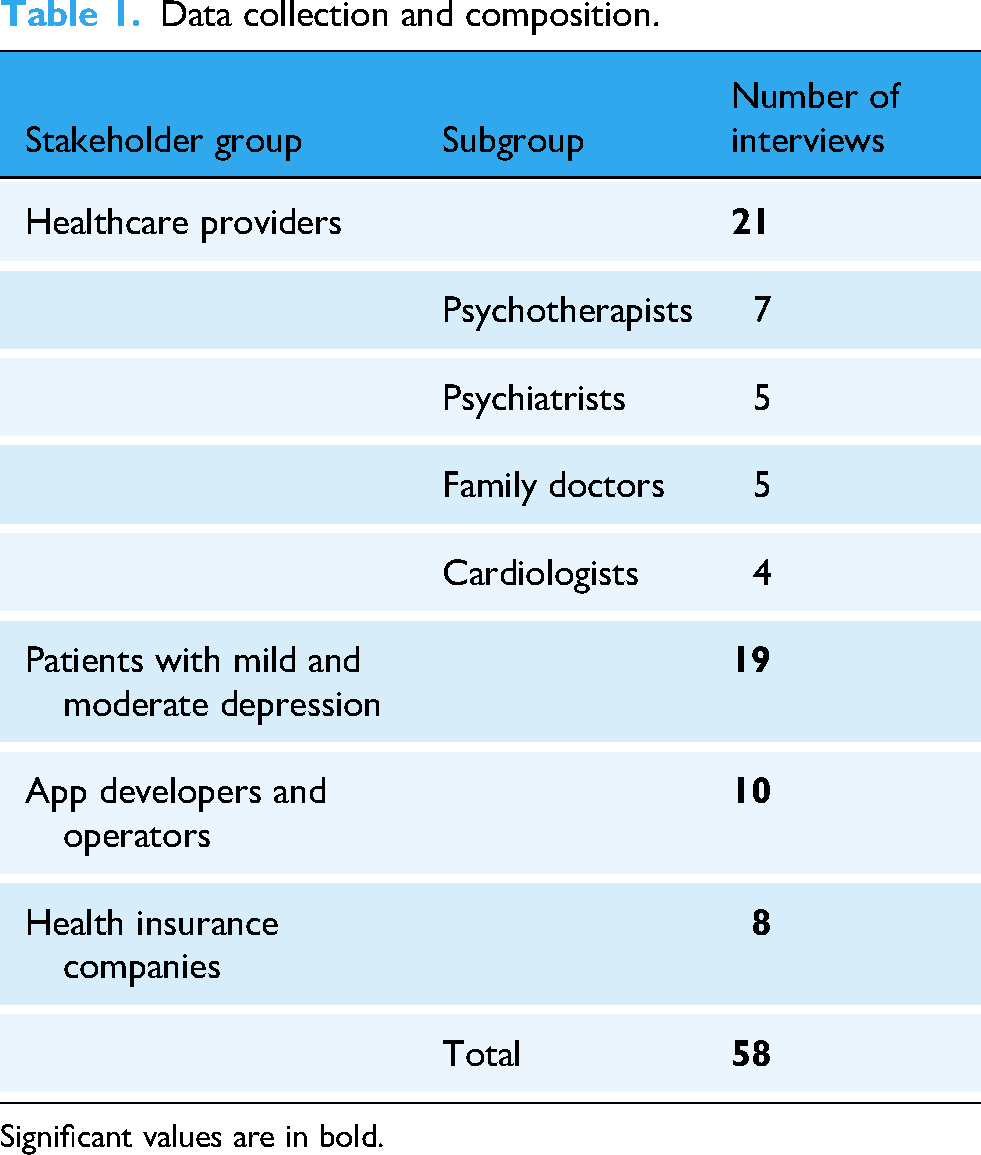
Significant values are in bold.
Interviews lasted around 30 to 120 minutes. The author's team conducted them in German or English and fully transcribed them afterward. Our transcripts serve as primary data for the construction of the DPs. We analyzed the transcripts with MAXQDA 2022 and made use of an iterative descriptive coding process, as suggested by Myers, 36 to identify MRs (“patterns”) and DPs (“characteristics within those patterns”) from the data. Descriptive coding has been used several times in related contexts, for example, DSR-specific contexts. 37 Initially, we used the question blocks from our interview guidelines as the first orientation to reduce the complexity of the transcripts and the content. Then, with this descriptive coding procedure, we ran a structured analysis within those question blocks regarding the qualitative data's most important design factors, characteristics, and possibly other important conditions. For example, we found several text passages through descriptive coding that were concerned with the “content and structure” of the depression app. Within this “content and structure” MR, we found arguments regarding “gamification” elements as potential DP. We used the identified coding examples from this DP “gamification” as inspiration to formulate a description of the DP “gamification” within the MR “content and structure” according to the logic of Gregor et al. 24 for the formulation of DPs. We structured our DPs according to the components of the aim of the DP, the context, the mechanism, and the rationale behind the respective DP. 24 Also, we took a closer look at the DPs that the different stakeholder groups named.
After identifying the first set of MRs and DPs, we initiated the evaluation stage, as suggested by Peffers et al. 30 of our research. We evaluated our initial MRs and DPs in light of several evaluation criteria based on existing seminal literature on DSR artifacts and DPs evaluation.31,32,38,39,40,41 As a result, we oriented our evaluation interviews to important criteria like accessibility, importance, and insightfulness, as well as guidance and usefulness. As we identified researchers and practitioners as the main stakeholder groups for our findings derived, we invited individuals from those. We ensured these were not included in the first data collection phase to avoid response biases. As a result, we were able to conduct four evaluation situations. MRs and DPs were sent in advance for the preparation of the interviews. They lasted around 45 minutes, were held online and in German, and conducted in June and July 2023. We wrote extensive interview protocols that serve as primary information for a potential evaluation and revision of our MRs and DPs. We refined our MRs and DPs according to the collected statements derived. Interview guidelines, the coding scheme with anchor examples, and evaluation questions can be found in the appendix of this article.
Results
We identified seven distinct MRs

Meta-requirements and design principles for depression apps.
Content and structure
Based on
“I would find that important because I always say that it's not appendicitis, and the symptoms and the people are so different. I would find that important that you could pick out something that affects you or where you need support. […] I don't have a lack of drive or anything, and you have to shape that very individually [in the depression app], I think.”
This can be achieved by individualization, that is, selecting therapeutic modules according to a therapist's recommendation
“I could imagine, if I use it [in my therapy], that I would always pick up on how the patient uses it and whether they use it. So, I would already accompany [the application] and not simply separate it, so to speak.”
Lastly, to create a more enjoyable user experience, incorporating gamification features, for example, providing a mascot or virtual companion, is helpful and should be considered by app operators
Simplification
A central aspect emphasized by all interviewees is illustrated in
“Interviewer: Okay. And now, […] what difficulties do you see in the independent use of such a depression app if a therapist doesn't accompany it?
Patient 4: My technical know-how [I: yeah]. In any case, the technical know-how, the fear, if I download it now and do something wrong, press somewhere that my data is freely available. And often, I find these incredibly long explanations about apps are so cumbersome that I leave it there.”
Our interviews brought several statements regarding appropriate user interfaces for depression apps. We received numerous potential design aspects from developers and patients to achieve an appealing user interface. Here, developers put effort into subtle colors and illustrations, while patients emphasized easy-to-read fonts. Especially the last has been identified as crucial for the success of depression apps.
44
While the examples are diverse among the stakeholder groups, subtle colors are important for patients and developers. As a result, we formulate the following DP5 regarding appropriate use interfaces: an appealing user interface that supports effortless use should be designed by, that is, using subtle colors, easy-to-read fonts, and illustrations
Supportive resources
This simultaneously provides a partial aspect to ensure supportive resources like mouse-over functions and has some aspects of simplicity
“So, for me personally, now not so important. […] not because I'm not a social person, not a person who doesn't like to talk to people, but when I talk to other people, I wouldn't want to talk about the depression app [through it].”
As a result, allowing the user to connect with other affected individuals to promote social interaction and encourage each other
Reassurance
A lack of drive and poor motivation are characteristic symptoms of depression sufferers. Patients typically experience difficulty establishing continuous use of treatment programs. Interventions in depression treatment should be designed to reassure the user
“One idea would also be to see we know quite a lot about the psychopathological profile of the users, that we don't just say we're going to make one solution for everyone, but that we also personalize it a bit. The people where we notice, ok, they have good self-regulation abilities, they get fewer reminders, because they [the remainders] are just annoying anyway, and the people who have difficulties, they get a little bit more and maybe also get a little bit of cheerleading from the app and a little bit more positive reinforcement and praise and ‘Hey, great, you've done a course!.’”
To sum up, we identify that, in addition to implementing social interactions in, for example, forums, receiving direct feedback and praise when using the app, for example, upon reaching a milestone, also provides increased motivation for the user
Security and privacy protection
Generally, security and privacy protection are very important while using health data. Still, the processing of sensitive health data, in particular, is an aspect that is a key issue for all interview partners
“Yes, so of course, it's an important topic, especially in depression. I can also think of a negative example: A hacker attack on a Finnish depression online therapy. The hackers blackmailed the patients who used the online therapy with personal data. So, data security and data protection are one thing. You do everything you can, but a professional can always get at the data somehow. Another thing is, of course, if you leave a door open, for example, or have old software and it is therefore no longer secure, then it's your fault.”
This is not surprising since data protection and security issues have been extensively studied as crucial for the success of mental health apps
51
and depression apps in particular.10,52 We formulate the following DP: To establish the user's trust in the app provided, the user must be made aware of the measures that have been taken to protect their health data
Quality
Furthermore, ensuring quality is essential for a reliable product, that is, a successful depression app
To summarize the fulfillment of all-important quality requirements, widely recognized certifications should be supplied as a quality criterion, showing the user that the product was developed according to recognized standards
“I think the most important thing is that we have carried out studies on our program, there are currently three studies on the depression program, and they are investigating how effective the programs are, and I think this is the only way to go out confidently and say “we know that our program works”.”
Framework conditions
There is a need for framework conditions that must be considered within the overall development process to make depression apps attractive to potential users and enhance their dissemination
“And the second point, which I also signaled a bit of disappointment about earlier, is that something like pay-for-use would also be possible for digital applications. Saying, no, I don't pay for downloading the app, but I pay for using the app, and if the thing has ten lessons, then the payment amount also breaks down into ten partial payments, each of which is called up when working on these ten lessons in the app. This would all be possible, would not involve a large administrative procedure, would be more in line with the uses and applications of the apps, and would also resolve a few stomach-aches on the subject of remuneration and costs.”
The cost aspect is also relevant on the side of the practitioners. The additional time and effort they spend to get used to new treatment methods must be adequately compensated
Multistakeholder-specific considerations
As shown, different DPs were mentioned by the various stakeholders. Table 2 shows an overview of the DPs and their articulation by our interviewed stakeholder groups. DPs identified are sorted according to their mentions.
Design principles sorted according to the mentions per stakeholder group.

D: developers; DP: design principle; HCP: healthcare professionals; HI: health insurances; P: patients.
Significant values are in bold.
Some observations can be made from this multistakeholder perspective and overview: The developers name most DPs (15), followed by patients (12), health insurances (11), and healthcare providers (10) out of our total number of 16 DPs. It can be assumed that developers have several ideas and imaginations on what seems crucial for designing depression apps. Healthcare providers, in contrast, follow the opinions of the majority and are included in DPs that are named by at least three or four stakeholder groups.
We identified congruent assessments among all stakeholder groups of several design factors: there is agreement that individualization (DP2), all DPs regarding simplicity (DP4, DP5, and DP6), crisis interventions and management (DP7), and data security (DP10) must be considered as crucial. It can be assumed that those DPs show high importance and must be considered in any way within the overall development process of apps for depression.
DPs that are named by three of four stakeholder groups (DP1, DP11, DP12, DP14, DP15, and DP16) are diverse in their composition of stakeholder groups. However, we observed here a centered inclusion of opinions by healthcare providers. Furthermore, only developers and patients, not health insurance companies and service providers, attach importance to gamification (DP3) and praise and feedback (DP9).
Two DPs were named by only one stakeholder group: these are DP8 “Interaction,” which was named exclusively by the patients, and DP13 “Certification,” which was named exclusively by developers. It should be noted that because a DP is named by one stakeholder group only, this does not necessarily mean it is unimportant for other groups. It can be assumed that different stakeholder groups understand design aspects under different terms or cannot formalize them if not explicitly asked. 56 For example, it became apparent that patients understand certification in terms of the quality of the app for depression. Consequentially, their statements, in this case, are connected to the overall (medical) quality of the contents provided by the app. While developers, healthcare providers, or health insurance companies do not place particular emphasis on the ability of patients to interact with each other through the app, this aspect may be a critical feature for patients to use. However, these single-stakeholder opinions highlight the need to consider a multistakeholder perspective in developing depression apps to receive a holistic overview of the phenomenon.
To sum up, each DP mentioned in Table 2, even if it is mentioned by all stakeholder groups or only one, can impact the acceptance and success of the app and, thus, the overall implementation process. The service portfolio of the depression apps heavily depends on the interests, that is, business model, of the developers, and healthcare providers that mainly want to offer appropriate services to patients and healthcare professionals. This issue of potential criticalities between those DPs was further explored through our conducted evaluation phase in this research.
Discussions
We evaluated our MRs and DPs that we identified before with four individuals. In total, three researchers, in the following denominated as evaluation partners 1 to 3 (EP1 to EP3) and one practitioner (EP4), were interviewed and asked their opinions about our research output. EP1 is a postdoctoral researcher in the e-health and m-health sector. EP2 and EP3 are research assistants at two German universities concerned about medical management, technologies, and m-health apps. All three scientists have a strong fit for the research topic and have published several peer-reviewed conference and journal articles concerned with m-health and/or depression apps. EP4 is a psychotherapist with a strong connection to the health insurance sector in Germany. Also, EP4 is closely connected to the app developer industry in the medical sector and apps for depression in particular. Statements regarding different evaluation criteria follow the procedural logic of Iivari et al. 32 for reusability of DPs, namely accessibility, importance, novelty and insightfulness, actability and guidance, and effectiveness and the evaluation criteria by Prat et al., 31 namely ease of use, consistency, or completeness. In the appendix, we present our evaluation questions for all criteria mentioned.
The presented MRs and DPs have been evaluated as accessible, especially by EP1 and EP3, meaning they are expressed in an understandable language. They recommend a change in the denomination of MR7 “framework conditions” that could be renamed to “access factors.” Also, a merge of MR5 to MR7 could be realized since security aspects play, according to EP1 and EP2, a subordinate role within the overall development process since they are often a pre-requisite within the depression app development and sometimes led by regulatory aspects, as in Germany. EP4 underlined this statement. In addition, a relabeling to “data security“ is considered for MR5 by EP2. As a result, the first pre-requisite (“accessibility”) for the reusability of DPs is fulfilled.31,32
We then revisited the importance of the listed MRs and DPs regarding their completeness, especially regarding our data's multistakeholder perspective. Here, respondents liked the good overview of the opinions of the different stakeholder groups about important design factors and characteristics of depression apps. This comparison has been evaluated as insightful and novel (EP1, EP2, and EP3).
Scientists argued that the DPs could guide (“provide guidance and actability”, according to Iivari et al. 32 ) a process for the development and dissemination of a depression app. However, EP1 argues that a holistic view of all DPs could also guide a starting process as a checklist for founding new businesses offering mental healthcare through apps. Following the DPs does not necessarily mean the developed depression app will be automatically successful. This fact is underlined by EP4, who argues that certification is one of the most crucial aspects of the design of depression apps. If the certification is not trustworthy to the user, other aspects play a subordinate role in the usage.
As noted by Iivari et al., 32 effectiveness or usefulness 31 is sometimes difficult to measure as one of the main indicators for the reusability of DPs. Consequently, we asked our evaluation partners about the potential usefulness of our results and findings. They find the comprehensive overview of the phenomenon, that is, design aspects of depression apps and their importance for specific stakeholder groups (EP1, EP3, and EP4) useful. From a practitioner's perspective, seeing which aspects are named and identified as most important is useful. Practitioners will be motivated to assess and order the DPs for their individual depression app development process (EP2 and EP4). Figure 2 represents the iterated MRs and DPs that became apparent through our evaluation phase.

Iterated meta-requirement and design principles for depression apps.
As the evaluation shows, our MRs and iterated DPs are important and can be useful for practitioners and academics. Focusing on the problem-centered approach by Peffers et al., 30 our theoretical contribution is a solution for a real-world problem in medicine to develop and offer depression apps that are appealing and cost-efficient for providers and intended users. Targeted app development requires indication-specific consideration and the inclusion of all stakeholders because focusing only on the patient gives a limited view of the care situation. The pre-requisite of successful mobile app development in medicine, that is, depression app development, is the integration of software developers and medical professionals. 14 The involvement of other stakeholder groups in the design of those apps has so far been limited, but it is critical to tailor the health app to the characteristics and needs of the end-user. 10 Also, healthcare professionals’ perspective regarding the app's content and development influences the application's acceptance. 15 In addition, health insurance companies form the interface between healthcare recipients, providers, and insurers and thus influence the adoption of m-health. 15 The question is which specific design factors and aspects can increase the acceptance of health apps from the perspective of stakeholders involved in the overall lifecycle of depression apps. With our multistakeholder perspective and examination, we aid this involvement.
In line with Gregor's logic, 33 we contribute with a theoretical contribution of the “design and action” type. Consequently, our DPs expand the current view on scattered design aspects and characteristics of depression apps that must be conserved within a development process. We contribute to the literature on the successful design and important characteristics of depression apps by providing clear recommendations. Also, our DPs overcame the development process challenges and the motivations in the introduction section. With our holistic multistakeholder perspective, established through extensive qualitative data collection among four stakeholder groups, we examined the differences and similarities of important design aspects between different stakeholders. DPs can be interpreted as nascent design theories since they can provide generalizable insights into other classes of mental health apps. 57 Two of our evaluation partners (EP2 and EP3) also confirmed this finding. Both interview partners in our evaluation stage reveal that the identified DPs could also be transferred to an extent to another e-health and m-health context. They stated that the DPs could also be transferred to international markets, even if the primary data was collected primarily in a German context. Contrarily, EP3 missed a DP regarding the obligation of providing an advertising-free depression app, which must be considered in several countries, like Germany.
Contributions for practitioners are intuitive and were explicitly mentioned by all our evaluation interview partners: as described, with our DPs, we want to guide an overall development process of depression apps. Responsible stakeholders like IT project managers can use our carefully derived DPs for their development projects to save time and effort in reducing development costs and the complexity of the overall development process.26,27 In addition, as indicated by EP1, our DPs can guide a grounding process of development companies that want to specialize their offerings within the healthcare sector or in the depression domain in particular. As a result, our findings can help practitioners overcome challenges like the high complexity of the overall process connected to implementing and disseminating digital health solutions. 58 As marked by our interview partners for evaluation (EP1 and EP4), developers and investors in depression apps must be clear about their own prioritization of the presented DPs. Regarding our RQ, we can claim that we identified the most important DPs, based on the statements of our interview partners.
However, successful depression app development in terms of, for example, development costs can be influenced by many other factors, like the composition of the development team,, 59 and implicit importance by the developers (as also mentioned by EP4) that may not be reflected through our DPs.
As indicated before, EP3 missed a DP regarding the obligation of providing an advertising-free depression app, which must be considered in several countries, like Germany. While the DPs derived provide a holistic overview, some of them, like data security (DP10) or remuneration (DP16), are influenced by country-specific regulations. The study was conducted in Germany with mostly German-based participants, and reflects potential specifics for Germany or the European Union. It should be noted that the study's findings should be reflected in the corresponding regulations. For example, areas like the United States or China, in which different regulations apply, could have different views on some DPs.
Also, as seen, the DPs derived holistic views and opinions on the topic of relevant design aspects. They do not precise a concrete development process and may be difficult to apply in real-world settings. We have some advice here: the DPs could be complemented by practitioners with forward/backward chaining models 28 to first structure them into a sequential behavior and visualize them in a processual manner. Also, the usage of the Persuasive Systems Design Framework 60 and persuasive systems principles, like reductions or self-monitoring, could be valuable for practitioners to first cluster the DPs derived to special interests in the light of the corresponding business model that the developer wants to achieve. Especially the last has been successfully adapted in the mental health context. 61 This outlined complementation could lead to further complexity reduction for the start of the development process of a depression app. In addition, incorporating the DPs into practitioners’ environments process models in the (mobile) software development domain, for example, agile processes 62 can help. In any case, the usage and adaptation of the DPs derived are influenced by a set of various internal and external factors that should be considered.
Limitations, further research directions, and concluding remarks
Our research has limitations that open the potential for further research. First, our presented DPs have been evaluated generally according to established evaluation criteria, but have to be tested in real-world setups. This research does not aim to develop a depression app based on the MRs and DPs derived. We received the first statements regarding the ordering and wording of our DPs and MRs. However, our evaluation here mainly focuses on the interview partners’ subjective opinions.
In addition, we did not interview noncare-providing researchers who develop depression diagnoses with advanced technologies like machine learning pipelines. In the past, several researchers have articulated the importance and usefulness of advanced technologies for depression diagnosis and interventions.63,64 While those technological possibilities were not explicitly mentioned in our material, including this stakeholder group in future research, like interview studies, could enhance a more unified view of important design aspects and technological backbones for depression apps.
Practitioners should use the DPs derived in real-world contexts and test the usefulness of these problem-solving artifacts in more detail. It is also valuable to weigh the importance of the DPs mentioned here or quantify them in terms of money and time resources saved. This procedure would lead to more quantitative insights into the usefulness of specific DPs. At the same time, iterative evaluation is an imminent step toward more appropriate DPs in DSR.30,65 This can be a fruitful avenue for further research.
Also, our DPs derived could be quantitatively measured and verified with surveys that collect the opinions of patients who suffer from mild or moderate depression. Research like this could examine the importance of the design factors derived in terms of importance and prioritization from a user's perspective. With this promising sequential mixed-method design and triangulation procedure 66 DPs and MRs derived can be iterated for a wider and better understanding of the phenomenon.
Our DPs are designed for depression apps and have a narrow design perspective. However, some MRs could be used to develop and construct other e-health and m-health solutions with or without focusing on mental disorders. 57 It could be valuable to investigate the generalizability of our findings to other domains, that is, to apps designed in an anxiety context. Here, interviews and subsequent instantiations, according to the DSR paradigm, could be an interesting first step.
The current research analyzes a set of crucial MRs and DPs for depression apps. We developed the DPs with qualitative data collected from interviews with 58 stakeholders to carve out design aspects and elements that must be considered when developing depression apps successfully in terms of tailored app functionalities and framework conditions. DPs were discussed and evaluated with scientists and practitioners, showing the importance and usefulness of our results. Our research can ignite a structured discussion among scientists and practitioners about the importance of design aspects of depression apps and the overall development process from planning to dissemination. The set of examined and evaluated DPs can lead to well-accepted and high-quality depression apps for patients who suffer from mild or moderate depression and, in the end, to quicker recovery.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251336276 - Supplemental material for Success by design: A holistic analysis of design principles for depression apps
Supplemental material, sj-docx-1-dhj-10.1177_20552076251336276 for Success by design: A holistic analysis of design principles for depression apps by Oliver Werth, Irene Jankowski, Nina S Müller, Fenja Schulte, Paula Warnemünde-Jagau, Michael H Breitner, Annika Herr and Kai G Kahl in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors would like to thank all the individuals who participated in this study.
Ethical considerations
The study was approved by the Ethics Committee of the Hannover Medical School under number 10017_BO_S_2021.
Consent to participate
All probands gave informed written consent before study entry.
Author contributorship/CRediT
OW, NSM, and IJ contributed to conceptualization; OW to methodology; OW, NSM, IJ, PW-J, and FS to investigation, visualization, and validation; OW, NSM, IJ, PW-J, FS, MHB, AH, and KK to writing—original draft; and OW, NSM, IJ, PW-J, FS, MHB, AH, and KGK to writing—review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Culture of the State of Lower Saxony (grant number ZN3751).
Conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KGK received speaker honoraria by EliLilly, Servier, TAKEDA, Idorsia, Dr Schwabe, Janssen (J&J).
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.