
Abstract
Background
Nigeria faces significant challenges in providing access to and utilisation of professional mental health treatments. Digital health systems play an essential role in healthcare across diverse settings. This study aimed to determine the perceptions, attitudes and use of digital health platforms in mental health promotion among University of Ibadan students in Nigeria.
Method
This study was a cross-sectional survey, and 400 respondents from the University of Ibadan, Nigeria, were selected using a multistage sampling procedure. The data were obtained using a semi-structured self-administered questionnaire. The data were analysed using SPSS version 25 via descriptive and inferential statistics, such as chi-square tests and multiple linear regression at the 5% significance level.
Result
The respondents were 24.2 ± 4.8 years. Most respondents (99.8%) had access to at least one mobile phone. The majority (83.2%) were unaware of any digital health platform for mental health promotion. Despite the lack of awareness, most respondents (47%) positively perceived the usefulness of digital health platforms for mental health promotion. Most (74.2%) had favourable attitudes toward using digital health platforms for mental health promotion. Most (88.3%) reported never using any mental health promotion applications, and 11.7% reported using at least one application. In the mental health assessment, 46.5% reported mild–severe mental disorders. There was a significant association between students’ awareness and use of these platforms (r = 25.429; p < 0.001).
Conclusion
These findings revealed low awareness of mental health promotion digital platforms, but the respondents had positive perceptions, attitudes and good behavioural intentions.
Keywords
Introduction
Mental health is a fundamental human right and a requirement for the development of all nations. 1 People are better equipped to establish connections, function effectively in society, cope with life's challenges, and ultimately thrive when they have strong mental health. According to the World Health Organization, 25% of the population will experience some mental illness at some stage in their lives, or an estimated 450 million people worldwide will suffer from mental disorders. 2 Despite the magnitude of the challenge, the global landscape of mental health care reveals that only around 10% of people who require attention or treatment for mental health issues receive it. 3
Nigeria faces many challenges in dealing with mental health issues, including limited access to mental health services, low allocation of funds and a significant percentage of young people dealing with mental health problems. As a country with over 200 million people, the disparity between its population size and the allocation of resources towards mental health is concerning. According to the World Health Organization, the government expenditure on mental health accounts for 4.1% of the total government health expenditure. 4 An estimated 70% of the roughly 50 million Nigerians facing mental health challenges fall below the age of 30. 5 In a newspaper content analysis study, from January 2010 to December 2019, there were approximately 350 suicide reports. Among these suicide reports, the percentage of students was 33.6%, and 50% of these cases were below the age of 35 years.6,7
Despite the high prevalence of mental health issues among young Nigerians, less than 15% of them receive and utilise professional mental healthcare services. 8 Several factors influence the use of mental health services, as evidenced by research conducted among undergraduate students. 9 One of the main limiting factors to accessing mental health help, among other factors, is that the cost of these services is reportedly high. The concern that their mental health issues would not be kept confidential, coupled with the stigma surrounding mental health, was another factor. The mental health status of a person has now become an additional intersection, further driving inequalities in health. 10
Digital platforms have already shown promising potential for mental health promotion, especially among young people. For example, social media is a potentially effective way of contacting many people quickly. 11 In particular, young adults have high rates of access to, use of and interest in technology, including smartphones and social media. 12 There used to be a high level of technology utilisation among those residing in higher income countries. However, there has been a shift in recent years, with these technologies becoming progressively more accessible and cost-effective to people in low- and middle-income countries. Digital platforms for mental health promotion are designed to address issues such as helping students schedule conflicts arising from academic demands and social commitments. It also helps with young people's reluctance to seek professional help and their developmental need for autonomy and independence. 13
Given the popularity of digital technology among young people, digital mental health services present a promising avenue to bridge this treatment gap in low-resource settings and underserved communities. 14 Research has shown that digital mental health services can enhance the efficiency, accessibility, acceptability and effectiveness of mental health services for young people. 15 However, the acceptability and usability of these interventions are influenced by their design, scepticism and differences in cultural and social norms.16,17 Health-tech solutions like digital mental health services are constantly being developed to improve health outcomes but they are often underused or abandoned, leading to inefficiencies and higher care costs. 18 This could be due to several reasons including a lack of user-centred characteristics, evaluation process, awareness or user perception.17,19 Investigating whether young people are aware of and willing to use digital health options in promoting their mental health is one of the first steps to developing user-centred solutions. These will be solutions tailored to the needs of young people that can supplement traditional mental health services. This could guide the development of future digital mental health services, policies and health interventions for underserved communities. The findings can help fill the gap in knowledge about young people's perception, attitude and use of digital mental health promotion platforms, with an ultimate goal of improving their mental health and holistic well-being and reduce the burden of mental health globally.
This study assessed the acceptability and usability of digital health platforms (DHP) for mental health promotion, using the Technology Acceptance Model (TAM). TAM is derived from the theory of reasoned action and theory of planned behaviour, which is meant to ‘trace the causal links from beliefs, through attitude and intention to actual behaviour’. 20 It posits that users are more likely to adopt a technology if they perceive it beneficial. TAM is founded on two constructs: perceived usefulness (PU), the belief that using the technology will enhance performance and perceived ease of use (PEOU), which is the belief that using the technology will be simple and straightforward. PEOU positively impacts PU, meaning easier-to-use technology is perceived as more practical. 21
When users find these platforms useful and easy to navigate, they develop positive attitudes toward using them, viewing them as valuable tools for their mental health. This positive attitude, in turn, influences their intention to engage with the platforms. Those who have a favourable attitude are more likely to express a strong intention to use the platforms regularly. The interconnected nature of the TAM highlights the symbiotic relationship between PU and attitude toward using, as well as between perceived ease of use and attitude toward using. These connections emphasise that users’ attitude are shaped by their perceptions of usefulness and ease of use, ultimately influencing their willingness to adopt the technology. 22
Aim of the study
This study investigated the awareness, perceptions, attitudes and use of digital health platforms (DHP) for mental health promotion among university students in Nigeria.
Specific objectives
The specific objectives are to
Determine the level of awareness among students regarding the availability of digital mental health platforms (DMHPs). Determine the perceptions of students regarding the effectiveness, benefits and use of digital platforms for mental health promotion. Assess students’ attitudes towards the use of DHP for mental health promotion. Determine the level of digital platform utilisation for promoting mental health among students. To examine the relationship between the TAM constructs (external variables, perception, attitude and behavioural intention) and the actual use of DHP.
Research questions
Are students aware of DHP designed to promote their mental health?
What are students’ perceptions regarding the use of DHP for mental health promotion?
What are students’ attitudes towards the use of DHP for mental health promotion?
What is the level of utilisation of DHP for promoting mental health among students?
What is the relationship between the constructs of the TAM—external variables, perception, attitude and behavioural intention—and the actual use of DHP?
Research hypotheses
The following hypotheses were tested.
Methodology
Study design
A cross-sectional study design was used for this study.
Study setting
The study was conducted between November 2023 and April 2024 at the University of Ibadan located in the south-western geopolitical zone in Nigeria, with data collection occuring from December 2023 to January 2024. The University of Ibadan is not only one of the oldest degree-awarding institutions in Nigeria but also holds the distinction of being the first university in the country. Established in 1948 as an external college of the University of London, the University of Ibadan has since become a prestigious institution of higher learning in Nigeria.
The study population included undergraduate (first to sixth year) and postgraduate students (master's students only). The study recruitment and data collection process lasted for 2 months (December 2023–January 2024). This study was conducted among undergraduate and postgraduate (master's) students, with the majority (384 out of 400) falling within the 15–34 age range, reflecting the study's focus on young people.
Eligibility criteria
Inclusion: Undergraduate and postgraduate students of the University of Ibadan who were in the selected faculties and willing to participate.
Exclusion: Distance-learning/part-time time students, including students who were indisposed.
Sampling technique
The students were selected from eight faculties at the University of Ibadan, covering both on-campus and off-campus residents. The sample size was determined via Cochran's formula for sample size, assuming a prevalence of 50%.23,24 A multistage sampling technique with a four-stage sampling procedure was adopted to select the 422 study respondents (Figure 1). 24

Multistage sampling for respondent recruitment.
Proportion sampling calculation

Sample size calculation
The sample size for this study was estimated using Cochran's formula for calculating sample size.23,24


A total of 406 students participated in the study but only 400 were eligible for analysis due to incomplete data.
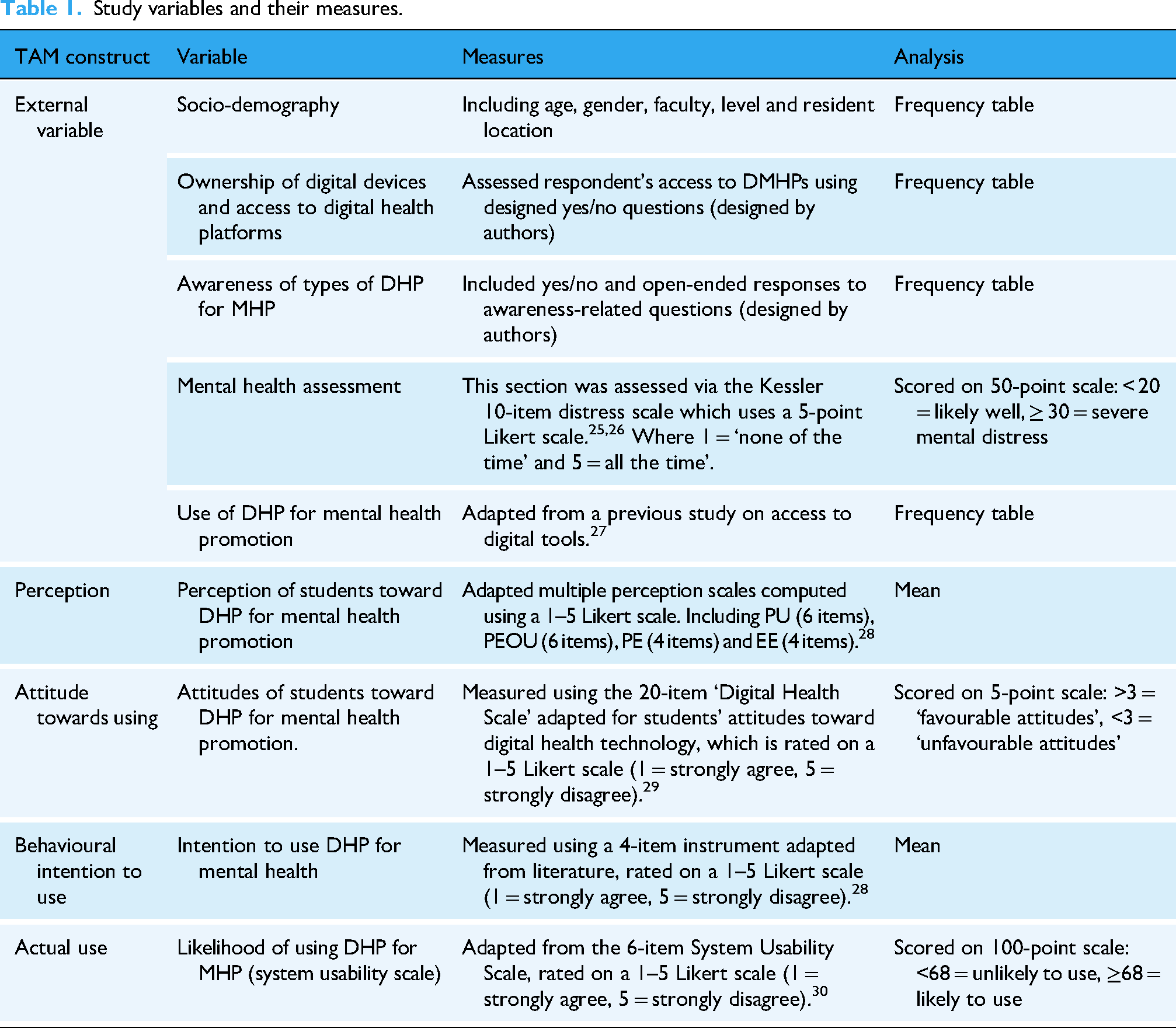
Study variables and their measures
The following variables were used based on the construct in the TAM. A section in the questionnaire represented each construct in the model to assess the relationship between the constructs.
Validity and reliability
To ensure the validity of the instrument, the authors reviewed relevant literature to develop it. Content validity was established by incorporating standard measures to design some parts of the study instrument including perception, attitude and mental health assessment (Table 1). Additionally, some sections, such as awareness and device ownership, were designed by the authors to address study-specific questions. Face validity was assessed through a pre-test conducted on 10% of the study population from a representative institution. Based on feedback from the pre-test, the instrument was revised and adjusted to improve clarity and relevance. Reliability assessment and reliability coefficient calculation were performed on the pre-test questionnaire to determine the instrument's reliability (Table 2).
Study variables and their measures.
Reliability statistics.

Data quality management
Quantitative data collection method was used for this study. A digital data collection tool was used for data collection at the start of the study. This process was done by contacting departmental class representatives to distribute links to students in their class through group chats. However, the response rate was low, and the remaining data were collected via self-administered questionnaires. Data collection was standardised across participants using a validated questionnaire, minimising the risk of information bias. The paper-collected data was meticulously entered into Kobo Toolbox and exported to IBM/SPSS (version 25) statistical software for cleaning and analysis.
All data were well documented for analysis, and the copies of the completed instruments were stored in a password-protected laptop, with only the authors having access to it. All data obtained from respondents is confidential and will remain confidential. A coding guide was developed after data collection to facilitate subsequent analysis. Data cleaning, recording and coding were conducted.
Data analysis
The data was entered and cleaned thoroughly by checking frequency distributions. There were no outliers recorded. All data were cross-checked during data collection. Out of 422 questionnaires, 16 were excluded. Data from 406 were collected, and 400 questionnaires qualified for entry and analysis. Data were analysed using descriptive statistics such as mean, median, mode, and inferential statistics such as chi-square and t-test. Chi-square tests were used to assess the significant relationship between categorical variables, with no adjustment made for the sampling strategy. No subgroup analyses or tests for interactions were performed. The level of statistical significance was set at a p-value <0.05. A multiple linear regression analysis was conducted to examine the effects of each factor on the likelihood of using a mental health platform based on the TAM construct. Tables and figures were used to ensure clear data presentation.
Results
Socio-demographic characteristics
Most respondents were between 15 and 50 years; the mean age was 24.25 ± 4.8 years. Most respondents (84.5%) were Christians, and 85.0% were from the Yoruba ethnic group. Most respondents (16.3%) who consented to the study were from the faculty of Clinical Sciences. There were more (63.8%) undergraduate students. Most respondents (60.5%) received allowances equal to or less than 30,000 Naira ($21). Over half of the respondents (64.2%) stayed in campus halls (Table 3).
Socio-demographic characteristics of the respondents (N = 400).

Ownership of digital devices and access to DHP
Almost all the respondents had access to a smartphone (99.8%) and owned a laptop (74.5%), whereas only a few owned a tablet (11%). The majority of the respondents also had access to the Internet (99.2%) (Figure 2).
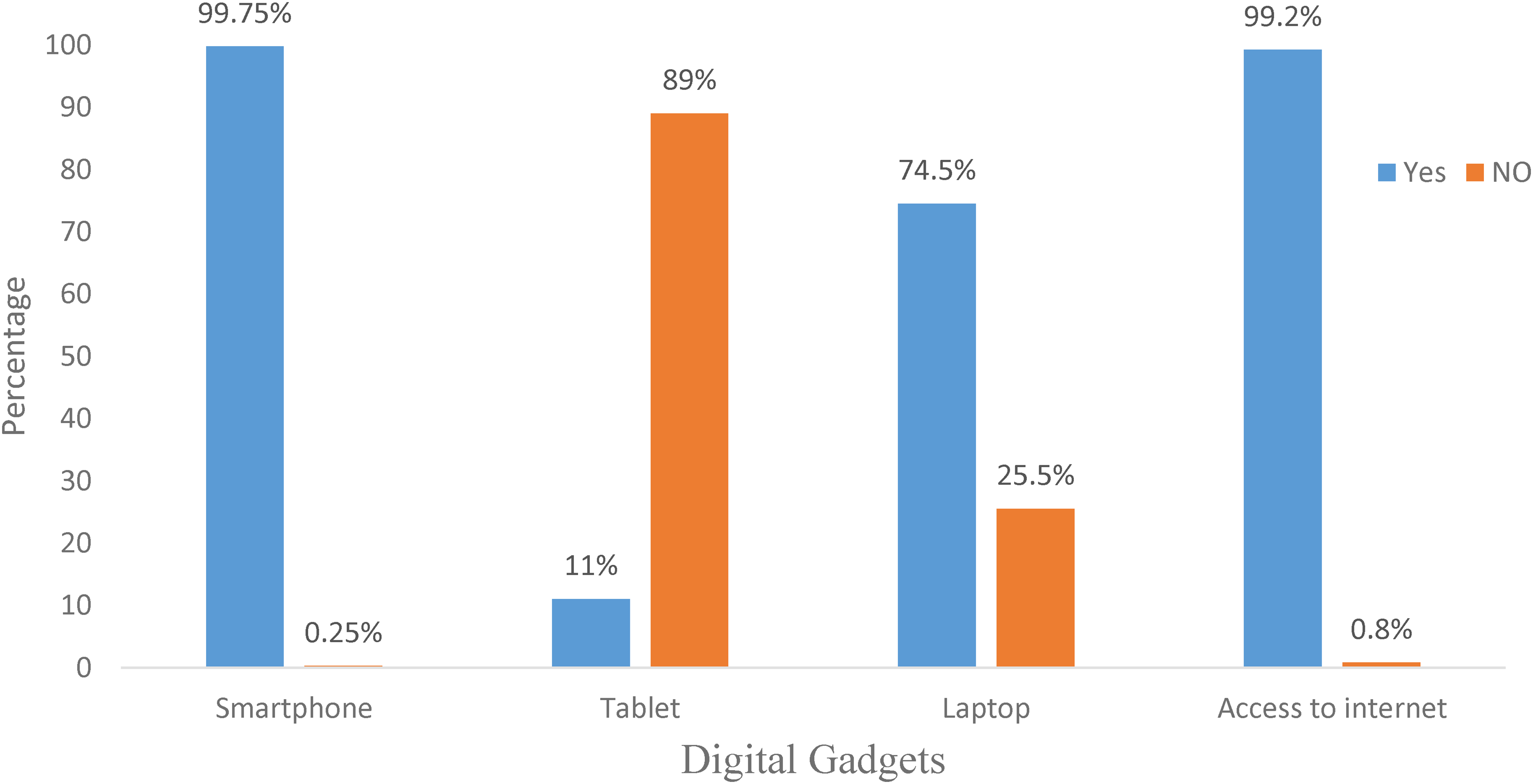
Ownership of digital devices and access to digital health platforms.
Awareness of types of DHP for mental health promotion
Most respondents (83.2%) were unaware of any digital health platform for mental health promotion. Among those who were aware of any digital health platform for mental health promotion, most respondents used digital mental health apps or social media apps (84.8%). Among those who were aware, most respondents (61.1%) heard it through the Internet (Supplementary Table 1).
Perception of students toward DHP for mental health promotion
The mean scores for PU (3.6846), perceived ease of use (3.7596), and performance expectancy (3.6731) were high. The mean score of effort expectancy, on the other hand, was below average (2.8650). Most respondents had positive perceptions of usefulness, ease of use and performance expectancy but negative effort expectancy (Table 4).
Mean scores for the perception scale.

Attitudes of students toward DHP for mental health promotion
The majority of respondents had a favourable attitude toward the use of digital platforms for mental health promotion (Figure 3). Over half of the respondents (51.7%) believed technology could enhance mental healthcare. Concerning the use of smartphones for blood tests, more than one-third of the respondents (38.5%) agreed that they would use smartphones for this purpose. A notable proportion of respondents (26%) strongly disagreed with preferring to search the Internet for help rather than consulting a mental health specialist or doctor. Approximately one-third of the respondents (32.4%) either disagreed or strongly disagreed with the statement, ‘I would never look for mental health information on the Internet if I were going through mental health challenges’ (Supplementary Table 2).

Attitudes of students toward DHP for mental health promotion.
Likelihood of using DHP for mental health promotion
The possibility of platform usage was low, with less than a quarter of respondents (19.2%) likely to use DHP to promote their mental health. Most respondents (51%) expressed their disinterest in using mental health platforms frequently.
There is no association between students’ attitude towards DHP for promoting mental health and their likelihood of using digital mental health platforms.
Fisher's exact test showed that there was a significant association between respondents’ attitudes towards DHP for promoting mental health and their digital health platform usability, (X² = 23.815, p < 0.001). The null hypothesis was rejected (Table 5).
Association between students’ attitudes towards DMHPs and their likelihood of using DMHPs (N = 400).

Fisher's exact test was used for variables with frequencies less than 5.
*Level of significance set at <0.05.
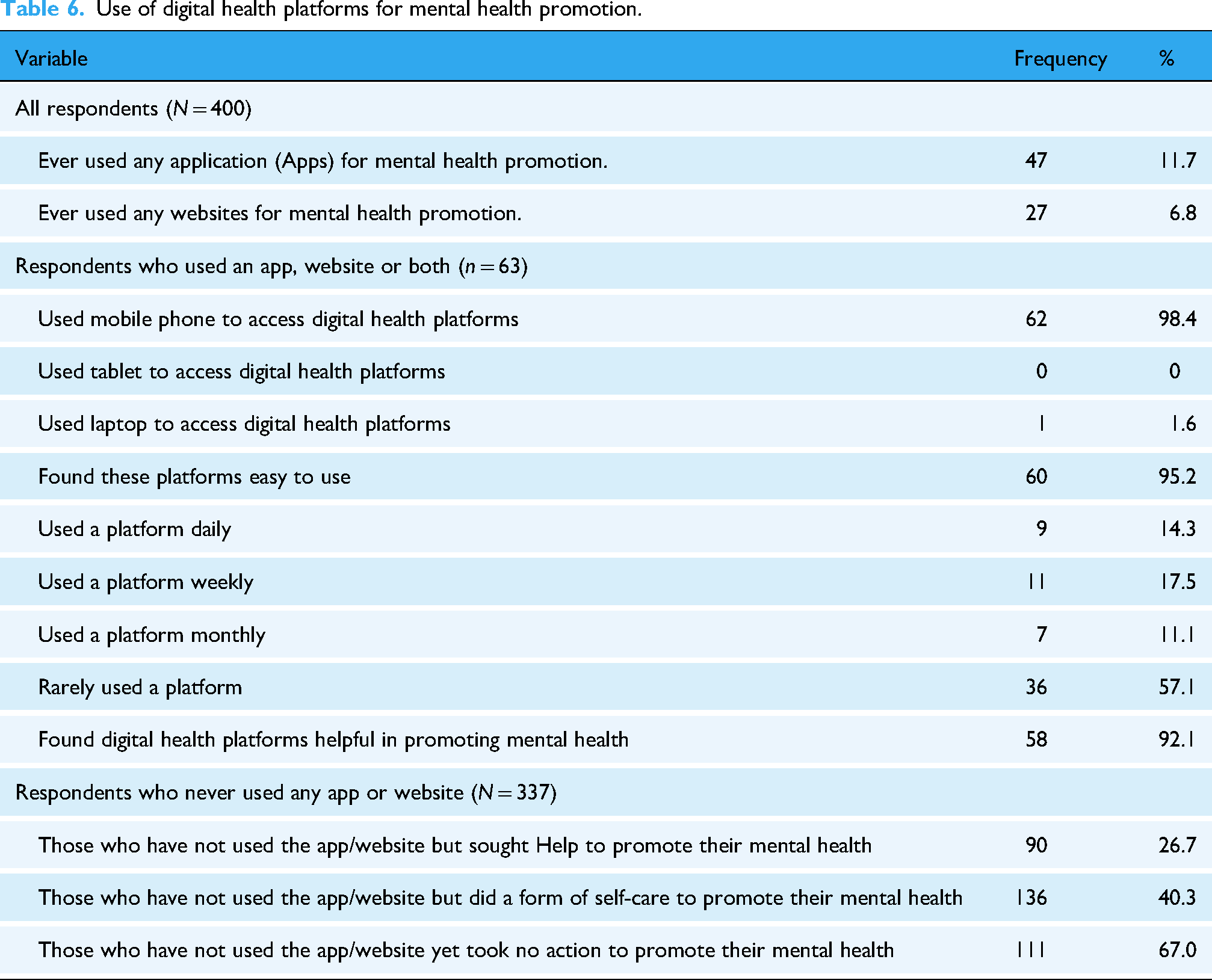
Use of DHP for mental health promotion
Table 6 shows that the majority of the respondents (88.3%) reported that they had never used any application (apps) for mental health promotion. Most respondents (93.2%) also reported not using any website for mental health promotion. Among those who utilised apps, social media (62.3%) was the most frequently mentioned, and other apps included the Apple Health Kit (5.7%) and Google (3.8%). Concerning website usage for mental health promotion, only 6.8% of the participants had engaged with such resources. Among the users, the Mentally Aware Nigeria Initiative (MANI) was the most commonly used website, mentioned by 22.2% of the respondents. Other notable resources included mental health foundations, such as the Asido Foundation (14.8%) and the Stop Mental Illness Foundation (7.4%). In comparison, 22.2% of the participants could not recall the specific names of the websites they had used. Those who have not used an app/website to promote their mental health mentioned several things they do in the form of seeking help or self-care (More results in Supplementary Table 3 and Supplementary Figure 1).
Use of digital health platforms for mental health promotion.
There is no association between Student's awareness of DHP for promoting mental health and their use of the platforms.
The chi-square test was used to test the association between respondents’ awareness and their use of DHP to promote their mental health and it revealed a significant association for apps (X² = 25.429, p < 0.001) and websites (X² = 59.700, p < 0.001) (Table 7). The null hypothesis was rejected.
Association between students’ awareness of digital health platforms for promoting mental health and their use of the platform (N = 400).

Level of significance at <0.05.
Intention to use DHP for mental health promotion
The respondents had a high intention to use DHP for mental health promotion. A significant portion (35%) agreed they intended to use a digital mental health platform. Most respondents (40%) also agreed that they intend to explore the availability of a suitable mental health app or website.
Mental health assessment
A significant proportion of respondents reported experiencing fatigue during the last 30 days. When asked about how often they feel tired for no good reason. A more substantial percentage of respondents said some of the time (31.5%), others reported having felt this way most of the time (13.8%), and a few respondents said all the time (3.8%). Additionally, more than a quarter of the respondents (28.4%) reported that they felt nervous some of the time, others felt nervous most of the time (11%), and a small percentage felt nervous all of the time (3%) in the last 30 days of the study Overall, the mental health assessment of the respondents showed that about 12.5% had severe mental health disorders. The details of these results can be found in Figure 4.

Mental health assessment.
Multiple linear regression
There is no relationship between the TAM construct (external variables, perception, attitude and behavioural intention) and the actual use of DHP for mental health promotion.
Regression indicates the directional linear relationship between two or more variables. The coefficient of determination (R²) expresses how well the regression line reflects the relationship between the independent and dependent variables (Table 8). The dependent variable is system usability; the predictors are PU, perceived ease of use, attitude and intention to use.
Multiple linear regression model.

Predictors: (constant), Perceived usefulness, perceived ease of use, attitude, intention to use.
Dependent variable: actual use (likelihood to use).
The results show that the linear model is statistically substantial t [F(6, 393) = 70.629, p < 0.001]. This indicates that the model has explanatory power, and the relationship between the variables is unlikely to have occurred by chance (Table 9).
ANOVA.

Dependent Variable: Actual Use (Likelihood to use).
Predictors: (Constant), Resident location, Perceived usefulness, perceived ease of use, attitude, intention to use.
Additionally, the influence of each factor within the model was analysed. It was found that mental well-being (t = 2.328, p = 0.020), PU (t = 4.287, p = <0.001), attitude (t = 12.218, p < 0.001), and intention to use (t = 5.966, p = <0.001) all had a significant influence on actual use/likelihood to use of digital health platform for mental health promotion. While perceived ease of use (t = −1.408, p = 0.160) and resident location (t = −0.261, p = 0.794) did not have a significant influence on actual use/likelihood to use (Table 10).
Multiple linear regression coefficients.
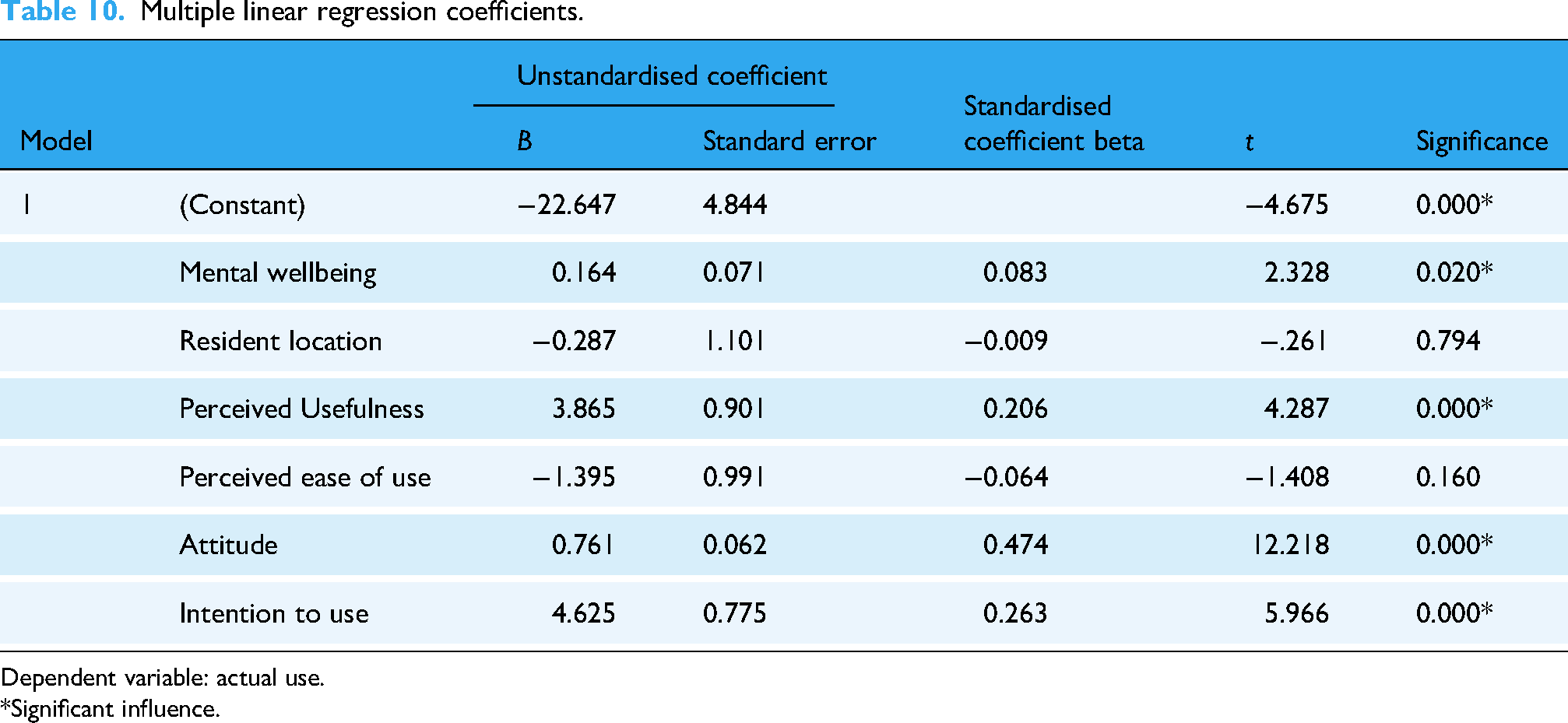
Dependent variable: actual use.
*Significant influence.
Discussion
Based on the aim of the study which was to determine the perception, attitude and use of digital health platform for mental health promotion. The study showed a positive perception and favourable attitude towards digital platforms for promoting mental health, but the use of this platform was very low despite the respondents having access to digital devices.
The demographic profile of the respondents in this study aligns with findings from previous research on technology use and digital health adoption among young adults and university students in different contexts. The concentration of respondents was young people, which mirrors similar studies conducted elsewhere. For instance, one study found a similar age distribution among their respondents, emphasising the relevance of DHP among younger populations. 12 There were also more undergraduate students among the respondents, as noted in our study, which is consistent with the findings of studies among Bangladesh and South African students.31,32
The overrepresentation of respondents from the clinical science faculty in this study resonates with the findings of a prior study that explored digital health use and opinions among university students. 27 This pattern suggests that students within specific academic disciplines may exhibit varying levels of interest or familiarity with digital health technologies. 27 The demographic characteristics of the respondents in this study closely align with previous research findings, emphasising the importance of considering age, academic discipline, and educational level in understanding the perceptions, attitudes and utilisation of DHP for mental health promotion among university students.
Nigerian students’ high ownership and use of mobile phones, particularly smartphones with Internet access, is consistent with contemporary trends in digital technology adoption. Nearly all participants reported having a mobile phone and access to the Internet, highlighting the ubiquitous nature of this technology within the study population. Moreover, a considerable proportion of the students also reported ownership of laptops but only a few owned tablets. This pattern of device ownership aligns with findings from prior research, such as the study on technology use and interest in digital apps for mental health promotion and lifestyle intervention among young adults, which similarly observed widespread smartphone ownership and comparatively lower rates of tablet ownership among participants. 12
The common use of smartphones among young people shows the potential utility of platforms for accessing mental health promotion resources. Given the portability and connectivity afforded by smartphones, they serve as accessible and convenient tools for engaging with digital health apps, resources, and interventions. Furthermore, the ownership of laptops among respondents suggests the availability of additional digital platforms that may complement smartphone-based interventions or facilitate broader access to digital health resources. The relatively lower ownership of tablets among respondents may reflect differences in device preferences or usage patterns within the study population. Despite the high ownership of digital devices like smartphones and laptops, with a high percentage of students having access to the Internet, their awareness of digital mental health platforms was very low. A study in India on awareness of mental health applications among smartphone users also reported a low level of awareness among Indian students regarding mental health platforms, but their awareness was still two times higher than Nigerian students. 33
In this study, most of the students who reported they were aware of digital mental health platforms were aware of social media platforms that promote mental health. Only very few students were aware of applications and websites specifically designed with mental health promotion features and principles, This aligns with research on mental health in Nigeria which reported that there exists a significant lack of awareness regarding digital platforms for mental health promotion and many NGOs that operate mental health programmes primarily utilise digital platforms such as Twitter, Facebook, WhatsApp, Emails and Hotline calls. 5
The low level of awareness did not influence the perception and attitude of students towards the use of DHP for mental health promotion. This study revealed that the students had positive perceptions and were favourable towards DMHP. In this study, close to half of the respondents acknowledged the usefulness of DHP in promoting their mental health. These findings are consistent with prior research, particularly a study conducted among Bangladeshi students, which highlighted the perceived value of smartphone apps for mindfulness exercises in enhancing mental well-being. 32 Participants in that study regarded these apps as essential tools for overcoming barriers to seeking professional help, providing a convenient and accessible avenue for practising mindfulness. 32 Additionally, participants appreciated the user-friendly interface and informal support provided by these apps, making mindfulness practices more accessible. 32
The favourable attitude recorded in this study explains the potential for these technologies to play a crucial role in addressing mental health concerns within this demographic. This result was also influenced by their positive perception (PU and ease of use) which is similar to a study that explored students’ perspectives on mindfulness-based stress reduction exercises via smartphone app in Bangladesh. 34 This finding aligns with previous research conducted among undergraduate students in Nigeria, where a considerably high percentage of the respondents demonstrated a positive attitude towards mental health services. 9 The high percentage of students indicating a willingness to seek professional help suggests a growing recognition of the importance of addressing mental health challenges among university students. Similarly, research conducted among students in Bangladesh revealed a strong attitude towards utilising DHP for mental health promotion. 32
On the use of DMHPs for mental health promotion, a study that investigated the factors influencing the adoption of mental health applications identified ‘Calm,’ ‘Headspace,’ ‘Woebot’ and ‘BetterHelp’ among the popular applications utilised by participants. 28 These applications/websites were also mentioned by some of the respondents in this study (Supplementary Table 3). The respondents that were using digital mental health platforms said they used platforms such as Blueroom Care, BetterHelp and Nguvu Health, but most of them rely on social media as a mental health promoting platform. These applications offer a range of features and services aimed at promoting mental well-being, including mindfulness meditation, guided therapy sessions and access to licensed therapists. The prevalence of these applications among respondents underscores their PU and ease of use in addressing mental health concerns and promoting emotional well-being. Factors such as user-friendly interfaces, accessibility and effectiveness in delivering evidence-based interventions may contribute to their popularity among individuals seeking support for mental health challenges.
This study also assessed the mental health status of participants. The result showed that only a few of the respondents might have severe mental health issues, using the Kessler distress scale. This study reported that more than half of the respondents were likely to be well and only a few but still a concerning percentage might have moderate mental issues and severe mental issues. This is similar to research in South Africa among undergraduate and postgraduate students. 31 This study reported that most of the respondents had excellent and good mental health status but a concerning percentage also had fair and poor mental health status.
Multiple regression was also conducted based on the conceptual framework. This aimed to investigate the relationship between system usability and other predictors, including PU, perceived ease of use, attitude, intention to use and other factors such as mental well-being and resident location. The model's explanatory power was confirmed by a statistically significant F-statistic [F(6, 393) = 70.629, p < 0.001], indicating that the relationship between the predictors and system usability is unlikely to have occurred by chance. The findings highlight that attitude, intention to use, PU and mental well-being were significant factors influencing the use or likelihood of using DHP for mental health promotion. Notably, attitude (t = 12.218, p < 0.001) emerged as the most influential predictor, suggesting that users’ perceptions and beliefs about the platform are essential in determining whether they will engage with it. This aligns with previous literature, consistently showing positive attitudes towards technology predict adoption and continued use.21,35
The findings from our study and previous research suggest a growing acceptance and recognition of the value of DHP in promoting mental well-being among university students, not only in Nigeria but also in other contexts such as Bangladesh and South Africa.31,32 Factors such as social influence, ease of use and PU of digital health play a critical role in driving this acceptance. Importantly, leveraging DHP can help bridge gaps in access to mental health care and provide much-needed support to students who may otherwise face barriers in seeking traditional forms of assistance. 31
This study has revealed low awareness and an even lower level of use of DHP for mental health promotion. Developers of DMHS seldom engage with underserved communities during the design process or offer guidance on using the technology.36,37 Therefore, they might lack understanding of the unique challenges faced by underserved populations, such as language barriers, cultural differences and varying levels of digital and health literacy. 38 This gap can lead to designs that do not cater to these groups’ specific requirements. Their lack of inclusion can be due to resource constraints or assumptions of homogeneity. Excluding users from the design process of digital mental health platforms can result in poor usability, diminished trust and low engagement. 39 This worsens their mental health state as these groups are not as financially free or have unlimited access to traditional mental health services. A study reported that user involvement contributed to shaping specific DMHS for young people. 40 This highlights the urgent need for a more inclusive and participatory approach to the development of digital mental health services.
Limitation of study
The study was conducted in a single national institution in Nigeria, so the findings cannot be generalised to all students in the country. However, as a national institution that admits students from all parts of Nigeria, the results can be generalised to students in other national universities. The participants represent various ethnic groups and geopolitical zones, making the findings reflective of a broader academic context beyond the study location. However, private and state-owned institutions may have different perspectives. Further studies could compare the perspective of young people across different zones in the country. Other study design methods like longitudinal studies, qualitative studies or randomised control trials (RCTs) can also be employed to evaluate the effectiveness and usefulness of specific digital mental health interventions in promoting young people's mental health. These methods could compare different intervention strategies, such as workshops, targeted campaigns, training programmes and peer support initiatives, to determine which approaches are most effective in increasing platform uptake and improving student mental health outcomes. By using mixed methods, future studies could generate robust evidence to inform the development and implementation of effective interventions to promote mental health among young people through DHP.
Conclusion
Mental health is an essential aspect of health and can be promoted through easily accessible means like digital platforms. Digital services have demonstrated significant potential in promoting mental health, particularly among young people, and bridging the treatment gap in underserved communities. Despite the benefits of digital mental health technology, the awareness of young people and their use of digital mental health platforms is low. Nonetheless, young people are willing to explore these digital interventions and promote their mental health. Health technology developers should involve young people from diverse backgrounds, especially those in underrepresented communities, in the design of digital mental health services to improve awareness and use of these platforms among these groups. An evaluation framework can also be designed to ensure that developed digital mental health services are satisfactory and acceptable to the people they are designed for.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251331841 - Supplemental material for Perception, attitude and use of digital health platforms for mental health promotion among students in a national university in the south-western part of Nigeria: A cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251331841 for Perception, attitude and use of digital health platforms for mental health promotion among students in a national university in the south-western part of Nigeria: A cross-sectional study by Racheal Oluwabukunmi Ogundipe, Oyenike Elizabeth Omotosho and Yetunde Olufisayo John-Akinola in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076251331841 - Supplemental material for Perception, attitude and use of digital health platforms for mental health promotion among students in a national university in the south-western part of Nigeria: A cross-sectional study
Supplemental material, sj-doc-2-dhj-10.1177_20552076251331841 for Perception, attitude and use of digital health platforms for mental health promotion among students in a national university in the south-western part of Nigeria: A cross-sectional study by Racheal Oluwabukunmi Ogundipe, Oyenike Elizabeth Omotosho and Yetunde Olufisayo John-Akinola in DIGITAL HEALTH
Footnotes
Acknowledgements
We acknowledge all the students who participated in the study. We are grateful to the ethical committee who provided approval for the study.
Ethical considerations
Ethical approval was sought from the University of Ibadan/University College Hospital Research Ethics Committee before data collection (UI/EC/23/0657). Consent was sought from participants using written informed consent forms before participating in the study. Research participants were fully informed about the nature of the study, its benefits, and its objectives. The research ensured that participation was entirely voluntary. The participants were assured of the safety and confidentiality of their information. All ethical principles, including beneficence, respect for the person, non-maleficence, justice, informed consent and voluntary participation, were strictly adhered to during the study.Participants were informed of their right to withdraw their consent at any point during the study. All the data obtained from the respondents will remain confidential even after the research. All data were well documented for analysis, and completed instruments were securely stored.
Author contributions/CRediT
ROO and YOJA conceptualised the study and designed the study instrument. ROO collected and analysed the data, interpreted the results and developed the first draft of the manuscript. YOJA supervisedthe research by revewing critically, providing feedback, editing at appropriate levels and guiding the direction/focus of the study. OEO reviewed the manuscript and made notable additions. ROO, YOJA, and OEO gave the manuscript final approval.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was self-funded.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.