
Abstract
Background
Mobile health is being increasingly considered as a strategy to deliver healthcare to people with chronic diseases. This stands particularly true for cancer management where treatment is being progressively administered at home, requiring more involvement, education, and changes in behavior from patients. This article aims to identify the main axes of intervention for behavioral change of mHealth in cancer management and its relative impacts, as well as identify recent evidence on user preferences for optimal engagement in mHealth-based behavioral change strategies.
Methodological Approach
A literature search was carried out in the Databases PubMed and Cochrane during the period October–December 2023. The search retrieved 505 initial entries narrowed down to 21 articles included in this commentary.
Results
Evidence is available on Mobile apps for cancer management being used to successfully promote behavioral changes in the areas of treatment adherence, symptoms self-management, communication with healthcare professionals, and holistic well-being in cancer patients. These are activities traditionally relevant in healthcare management interventions and contribute to further developing the relevance of the field of Digital Health in healthcare management.
Relevance to Clinical Practice
The article contributes to a practical understanding of how Mobile interventions are being applied to promote higher self-care, a better emotional status, lesser adverse impacts, and, ultimately, increased survival rates for cancer patients. Several cancer patients’ preferences were identified for the promotion of user engagement related to app design, available features, interoperability, and app creation process, as well as advanced healthcare management intervention. Preferences were found to be different for adolescents and young adult cancer patients when compared to other cohort groups.
Keywords
Introduction
Mobile technologies are a ubiquitous aspect of contemporary life, and, according to the World Health Organization (WHO)1,2 mobile health has the possibility to radically reorganize the way healthcare is delivered around the world. Mobile health (from now on mHealth) can be defined as all medical and public health practices supported by mobile and wireless devices or applications.1,3 As examples of mHealth we can mention: apps, SMS messaging, wearable, social media, and remote sensing. 4 mHealth is a ramification of digital health, which encompasses the different usages of information and communication technologies as tools to promote health and manage disease: telemedicine, artificial intelligence, and mobile applications for health. 5 There are many opportunities inherent to delivering healthcare via mobile applications; first and foremost because the access to mobile technology is widespread—it is estimated that 2.5 billion people in the world possess a mobile phone 6 and relatively inexpensive. 5 Chronic diseases such as diabetes, cancers, and hypertension are considered epidemic worldwide causing a substantial burden of disease and decreased life expectancy. Given that the majority of chronic patients are also mobile application users, mHealth is being increasingly considered as a strategy to augment the realm of action of healthcare services and improve the quality of life in people with chronic diseases.5,7 Traditionally, during the active disease phase, as well as in the follow-up stages, cancer patients were intensively reliant on traditional healthcare services for treatment, symptom management, health literacy, and communication with healthcare professionals. 7 In the last decade, mobile health has proven to be a valid complement to traditional healthcare services for cancer patients, given that treatment is being progressively administered at home, requiring more involvement, education, and changes in behavior from patients. Given that mobile health is widely accessible and allows for remote monitoring, it creates a unique possibility for cancer patients to actively participate in disease self-management, granting patient's empowerment and behavioral change5,8–10 describe behavioral change interventions via mobile health as all interventions destined to improve education, incentivize desirable behaviors related to treatment and non-treatment aspects, and create environmental restructuring in the interaction with healthcare professionals. This literature review aims at identifying the main axes of intervention for behavioral change of mHealth in cancer management and relative impacts, as well as user preferences for optimal engagement in mHealth-based behavioral change strategies.
Methodological approach
Although this is not a systematic literature review, we still feel the need to identify how we selected the articles for this commentary.
In order to develop this narrative review, a literature search was carried out on PubMed and Cochrane databases. The search strategy was applied by using the keywords “digital health” AND “mobile health” AND “mobile applications” AND “behavioural change” AND “cancer management” AND “neoplasms management“. Results were selected from the Databases PubMed and Cochrane as published during the period January/2018 to December 2023.
The inclusion criteria defined for the study were the following:
- Articles published in peer-reviewed Journals; - Full-text in English available; - Published from January 2018. - Secondary studies; - Publications not specifically related to cancer management; - Related to digital interventions that were not apps/mobile-based; - Focusing on survivors, rather than patients in active disease management; - Not focused on behavioral change.
We excluded from the final pool of selected articles:
The search yielded initially 505 results that were narrowed down to 21 articles after the triage process that involved the removal of duplicates and the assessment of the relevance of articles first by title/abstract, and then by full-text (see Figure 1).
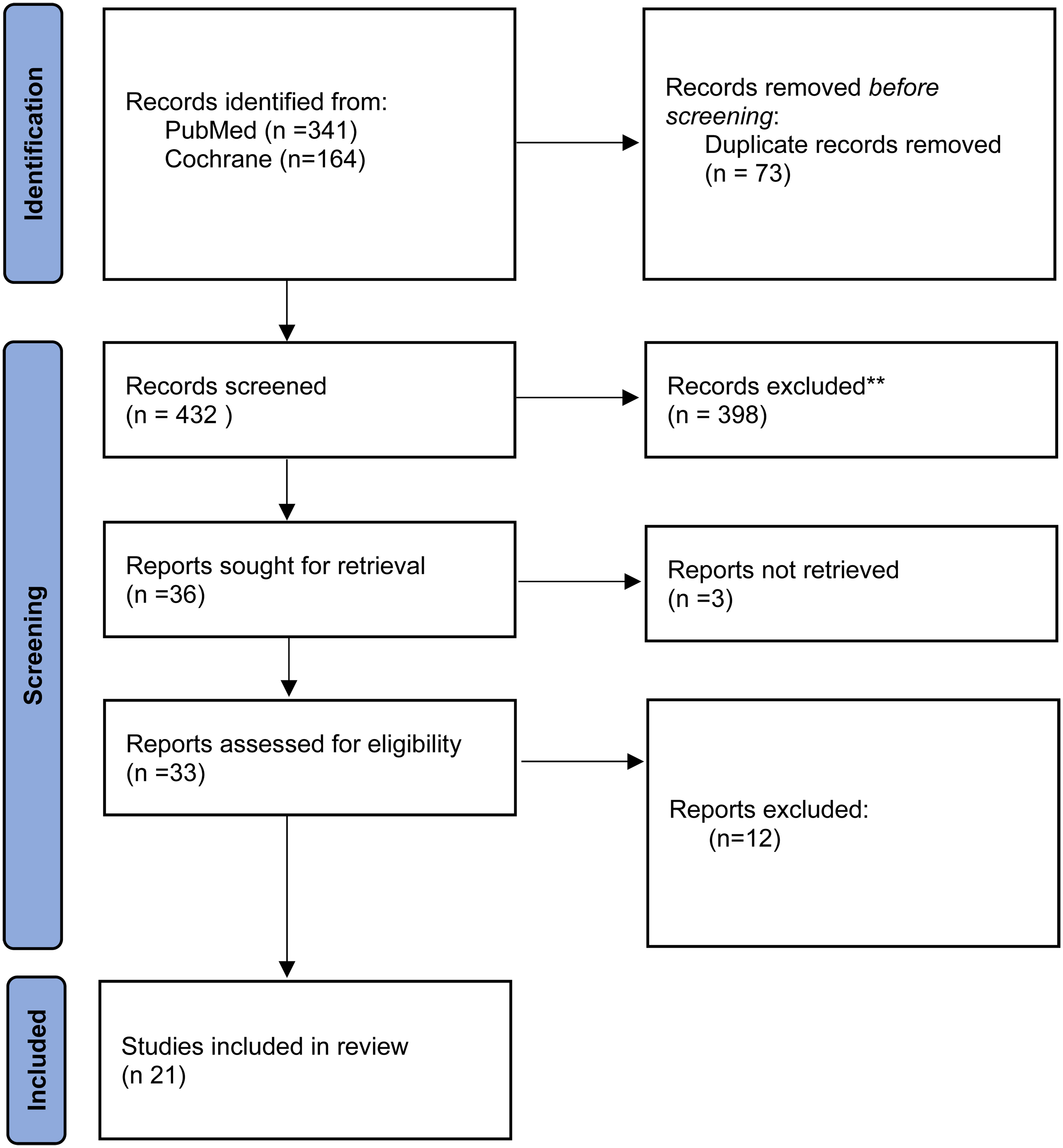
Literature search flow diagram.
Axes of intervention for behavioral change
Four axes of behavioral change pursued via mHealth were encountered in the reviewed studies and inductively defined by the analysis of the international authors developing the review: mobile-based interventions aimed at increasing treatment adherence in cancer patients, improving the self-management of symptoms, bettering the communication and registering of patient-reported outcomes and target holistic wellbeing.
Increased treatment adherence
Within the reviewed articles, mHealth was been found to be a valid potential ally in increasing treatment adherence in cancer patients, specifically, for what concerns the adherence to oral anticancer medication. As discussed in relevant literature11,12 the growing utilization of oral anticancer medication, generally managed by patients autonomously and remotely from healthcare professionals, has brought about challenges related to correct treatment adherence. This poses a great risk as suboptimal adherence increases the risk of relapse and mortality.5,13,14 As discussed in a 2020 study 13 the WHO had, already in 2001, flagged the need for strategies directed at supporting and augmenting treatment and medication adherence, mobile health representing an extremely valid candidate due to its reduced need for resources and increased accessibility.11,12 WHO reiterated most of these needs in 2011. 15
The most important type of app-based behavioral intervention identified by cancer patients within the observed studies touched upon the use of reminders and memory supports to track taken and missed therapeutic doses.11,16 Some participants in a 2021 study reported feeling more empowered in treatment management, and most likely to form medication-taking habits 16 although in a previous 2018 study for some of the patients such kind of intervention was deemed less important than educational interventions. 11 A 2020 randomized trial 17 did not find significant differences in adherence within the study group receiving app-based treatment support, versus standard care support. However, the same study did identify gains associated with mobile app intervention in the subgroups that reported elevated anxiety. 17 Also, it was observed that a greater engagement with the app was associated, within the intervention group, with fewer visits to the emergency department leading to hospitalization.
There is a population for which mobile health has been discussed in the literature as representing a specific opportunity in terms of treatment adherence, that of adolescents and young adults (AYAs). AYAs have been found to have reduced adherence and survival outcomes when compared to younger or older age groups, the so-called “AYA gap.”14,16 At the same time AYAs have been found to be particularly likely to use apps 16 and have been observed to yearn to share experiences about the disease to alleviate emotional suffering. 14
Symptoms’ self-management
Mobile technology offers the possibility to manage symptoms via the app-based logging of patient-reported outcomes as well as gain educational material about their diagnosis. As discussed above, as cancer patients are treated also on an outpatient basis, some extent of self-management of symptoms is needed as patients may have to deal with adverse symptoms, such as nausea and fatigue, without the support of clinical professionals. 8 Symptoms’ management in cancer patients typically leads to social isolation and anxiety, being the incapacity to manage or understand symptoms a predictor for greater emergency visits. 18 Mobile technology supports self-care by allowing them to track symptoms in a daily manner, being supported in the identification of expected versus alarming symptoms, increasing the ability for self-care8,19 as well as survival rates. 18 This was deemed very valuable, especially the first time a symptom appeared. 8 Patient-based symptom monitoring has been associated with decreases in pain and mental distress, and increases in survival rates, quality of life, and patient satisfaction8,15,20 At the same time, it has led to a decrease in healthcare utilization and unplanned emergency visits and hospital admissions. 20 Nevertheless, a study carried out in 2020 research 12 did not find relevant differences in symptom burden within the study group receiving app-based support to treatment when compared to the control group receiving standard care support.
Communication with healthcare professionals
Mobile technology offers the possibility to manage symptoms via the app-based logging and transmission of patient-reported outcomes to clinical professionals. According to relevant literature, 8 the possibility to report and promptly transmit symptoms to healthcare professionals created a channel for continuous communication, providing a sensation of participation and supervision with fostered reassurance. At the same time, remote symptom communication was perceived as convenient, given that it was done on the patient's own timeline. Symptoms can be communicated via Mobile health as soon as experienced, and, although they might not be answered by professionals immediately, the timeliness guarantees that the patient will not forget to communicate as it may happen if they have to wait for the next visit. 10 This in turn was found to incentivize reporting. 21 The studies reviewed support the view that remote symptom monitoring and communication increases patient communication, responsibility, involvement, satisfaction, and results.18,22 It also may lead to an increase in value-based healthcare, as patients are being supported in outcomes that are subjectively important to patients. 10 On the other hand, the patients approached in another study 22 reported a negative impact, expressing that symptom reporting had them seldom too preoccupied with their symptoms, and reminded constantly of their diseases. Another negative aspect pointed out was the longing for the human interaction and the level of detail offered by a presential communication. 22
Holistic wellbeing
One very important aspect of non-treatment-related cancer management is the possibility of mobile technology in promoting health and delivering interventions in aspects such as nutrition, physical activity, sleep, and anxiety. 11 Mobile health has proven to be a sound compound to offer education material related not only to the diagnosis but to aspects of holistic well-being via measures as simple as a “tip of the day”. Nutrition-wise, cancer patients often experience nausea, taste changes, or dry mouth as a treatment side effect. These symptoms adversely impact nutritional intake, which can lead to a sub-optimal nutritional status. 23 Mobile health interventions can target nutritional behavioral change by focusing on appropriate caloric intake and healthy eating. Concerning nutrition, 23 evidence warns on the need to only use evidence-based, clinically formulated apps warning that the majority of public apps available on Apple App Store and Google Play was less than optimal, and in some cases even potentially harmful furnishing misleading information. Physical activity is also considered a fertile domain for app-based behavioral change for cancer patients. As pointed out by other study, 17 traditionally the recommendation for cancer patients was to rest, but more recent evidence has shown that sedentary behavior is related with adverse treatment and recovery outcomes. On the same line, another study 24 argues that physical activity is the most determinant lifestyle factor linked to survival in breast cancer patients, whilst another study 25 suggests that the number of steps taken each day is a reliable parameter for predicting hospital discharge in gastric cancer patients’ post-operation. Technology-based trackers or wearables allow for self-monitoring, encouraging the attainment of physical activity milestones, as it is the case for step-counting. 25 Still according to the same study, 25 these methods are highly reliable, as they do not overcount or undercount steps, making so that physical activity becomes both an objective and a measurable performance indicator. Stress levels and mental distress are typically high in cancer patients—being experienced in roughly half of the cases—due to the diagnosis itself, but also the adverse impacts of treatment. 26 When compared to physical health, mental health is often disregarded, although its reduction has significant impacts in terms of reduction of quality of life and even adherence to treatment. 26 mHealth-based behavioral changes promoting self-monitoring, meditation, muscle relaxation, emotional control training, and cognitive behavioral therapy can help reduce stress levels. 26
Engagement and perception concerning app-based behavioral interventions
As discussed in relevant literature8,11 patients’ engagement in app-based behavioral interventions is influenced by a panoply of factors, starting with demographics (age, education, employment, income, and marital status), users’ competencies, experience with mobile devices and technology, to aspects inherent to the mobile application itself, such as design and usability, all the way up to contextual factors such as availability of technologies and internet connection. According to available evidence, 26 cancer patients may be more interested and adherent to mHealth given their realm of treatment and their self-care necessities, as “engagement is linked with distress and need.” 26 This view is backed by additional evidence 8 which observed that mHealth utilization was referred to as being more relevant at the beginning of the cancer journey when symptoms and treatment management was an unknown pathway for the patient. As the disease journey progressed, and respondents were found to gain experience in the different aspects of cancer management, the mobile support was deemed less relevant, and a need for a deeper and more personalized healthcare pathway emerged.
In the evidence generated by another study 11 70% of patients with access to mobile technologies were interested in downloading an app for cancer management, this number increasing to 100% in the adolescents and young adults cohort of another study. 16 In one other study, 17 almost the entirety of app users were likely to recommend the utilization of the mHealth intervention.
User preferences
Unsurprisingly, the preferences of users of apps destined for behavioral change are concerned mainly with app design, available features, and interoperability. As with other mobile technologies, it was deemed of utmost importance that apps be simple, intuitive, and graphic.11,21 An excess of scientific terminology was deemed negatively, making the navigation less accessible. Customizable apps and apps using multimedia content were preferred in terms of user engagement.11,13,17 In terms of customization, calendar views, alarm sounds, time settings, and the possibility to add notes or instructions were all found to be preferred features. 13 Apps able to interface with clinical appointments, clinical health records, and prescriptions were favored over less interfaceable apps.16,21 The possibility to use the app on different devices and, if needed offline was also deemed of primordial importance.6,13 For treatment adherence users, the use of images, and in specific images providing generic and brand names, was deemed as valuable as observed in evidence11,16 that seldom medication reminders were considered as sufficient features for a medication adherence app. On the same note, another study 8 pointed out that users would like symptom management apps to also include aspects of holistic wellness, related, for instance, to nutrition or emotional well-being. Of the breast cancer patients studied, 8 whose app objective was mainly to communicate with clinical professionals, demonstrated interest in being able to flag if a telephonic follow-up was needed or not. Additional evidence suggests that educational features concerning diagnosis and treatment plan were always deemed relevant namely in a study 15 in which participants referred that the mobile information center would be the first feature of the app to be explored, being the preference for content searchable content by symptom. It was deemed transversally fundamental for the mHealth tools to be designed in a collaborative manner, taking into account the preferences of current and prospective users 27 together with the input of evidence-based and clinical professionals.15,23 One interesting finding concerning AYAs was the consideration, in one study 4 that AYAs are not interested in cancer-management social media features, which is unexpected given the cohort's high interest in the engagement of social networks. This lack of interest is justified by the authors in terms of the potential stigma associated with the oncology condition. According to such findings patient and parent's app versions’ need by require specific age-appropriate adjustments. 4
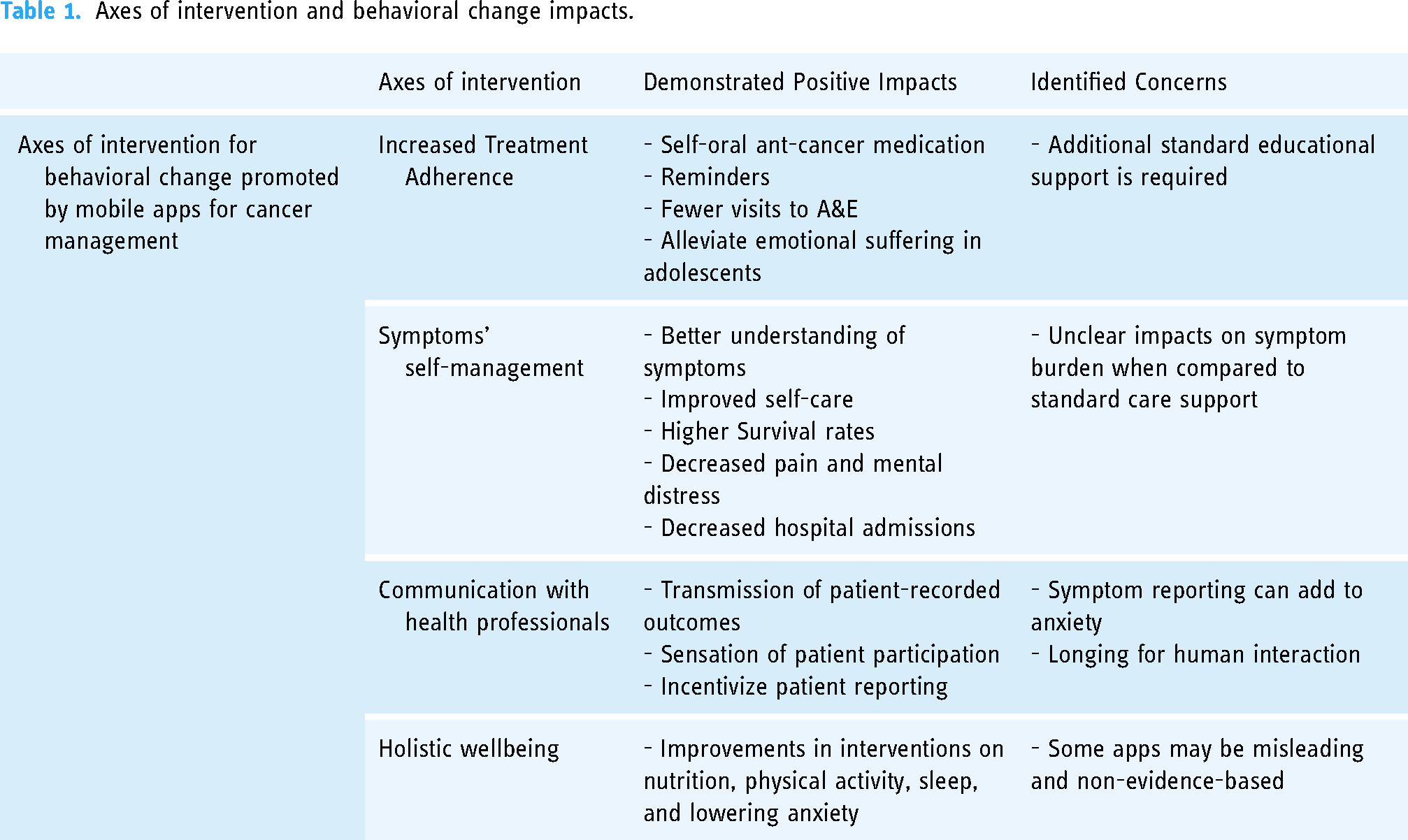
Table 1 summarizes the axes of behavioral change impacts as described in the literature retrieved. Results from the literature search are presented in Table 2, which is the map of the literature identified.
Axes of intervention and behavioral change impacts.
Mapping the results of the review.

Discussion
To develop this commentary and narrative review, the authors considered available evidence and the related international debate on healthcare management perspectives33–37,38 and the related application of digital health applications in all its dimensions.2,37,39 This was followed by the focused research for this commentary in which the authors screened 505 articles, finally selecting 21 articles containing qualitative information used to better understand the behavioral change of cancer management via mHealth. In specific, it aimed at identifying the main axes of intervention for behavioral change of mHealth in cancer management and relative impacts, as well as user preferences for optimal engagement. Behavioral apps for cancer management were been found to be useful in increasing treatment adherence in the general population and were indicated as particularly beneficial in bettering the adhesion chances of the adolescents and young adults age group. Furthermore, they were found to positively impact symptom self-management in oncological patients, especially for what concerns the management of first-time symptoms, leading to a reduction in emergency care visits. They were found to allow for an increase in patients’ communication with healthcare professionals incentivizing symptom reporting and stirring an increase in value-based healthcare. Finally, cancer management via mHealth was found to provide services in terms of holistic well-being: nutrition, physical activity, and emotional support and overall promote healthy behaviors. Engagement was found to be high, especially in the first phase of the cancer journey, and user preferences depicted the key importance of customization, good user experience design (better if collaboratively designed), and interoperability with other devices.
Among the pool of articles selected from peer-reviewed high-quality Journals, only a small proportion of the articles were found to explore in detail the potential for behavioral apps to impact the areas of wellness, holistic health, and health education, being the focus of other articles largely set on treatment adherence and symptoms self-management and patient-reported outcomes, which is coherent with the existing body of literature on patient-reported outcome measures (PROMs) and mHealth. Furthermore, very few studies focused on specific population cohorts, based, for instance, on educational background, gender, or ethnicity, making it difficult to pinpoint the differences originating in the participants’ different social determinants of health.
Conclusions
Available evidence suggests that the four axes of behavioral change identified in this article are actively pursued via mHealth applications and the evidence encountered in the reviewed studies suggests their potential to develop mobile-based healthcare management interventions aimed at: (a) treatment adherence; (b) self-management of symptoms; (c) communication with health professionals and registering of patient-reported outcomes; (d) target holistic wellbeing.
From the analysis performed, notwithstanding the limited number of articles found, and the small pool of participants of each study, it appears that mHealth behavioral interventions do promise a great potential for cancer patients in terms of empowerment, quality of life, survival rates, and reduction of healthcare costs due to unnecessary morbidity or emergency visits.
On further research necessary, our analysis of available evidence suggests that it is of utmost importance that further, larger-scale studies, such as large-scale randomized controlled trials, be carried out on the subject, preferably segmenting participants based on demographic aspects as well as specific cancer disease trajectories. This is a gap in research identified.
Concerning the relevance to clinical practice, this article identified evidence of how Mobile interventions were found to give origin to higher self-care, a better emotional status, lesser adverse impacts, and, ultimately, increased survival rates for cancer patients. Several preferences were identified for the promotion of user engagement related to app design, available features, interoperability, and app creation process, as well as advanced nursing intervention. Preferences were found to be different for adolescents and young adult cancer patients when compared to other cohort groups.
Thus, this article generates some practical recommendations for healthcare providers and patients, namely (1) healthcare organizations caring for cancer patients should adopt and offer mHealth options to their patients; (2) cancer patients should be targeted for education efforts on using mHealth options during their chronic disease management process; (3) mHealth solutions developers should revise and adopt their apps to cancer patients preferences identified in this article as demonstrated by available evidence.
Limitations of the review
The authors have undertaken the search base for this article in two major high-quality scientific databases for healthcare: Pubmed and Cochrane. Other databases may have other articles on this topic. The search for published evidence on the topic focused on evidence from January 2018. Previous studies may be available but were not considered.
Footnotes
Author’s note
All authors gave their final approval of this version to be published and agreed to be accountable for all aspects of the work.
Contributorship
WL and PM conceptualized the article and the research, and supervision and revised the draft manuscript. MM undertook the methodology, DLW, and BdS Data Curation. THNg undertook a formal analysis and edited a revised version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent statement
The literature review did not require patient consent.
Guarantor
NA