
Abstract
Introduction
An electronic medical record (EMR) can enhance the quality of care and patient outcomes. Ethiopia started the implementation of EMR in 2013. However, its adoption among healthcare providers has been low. Thus, this study explored the barriers and facilitators of EMR adoption among healthcare providers in Addis Ababa, Ethiopia.
Methods
A descriptive-phenomenological approach was used. Data were collected from one hospital and three health centers from 5–13 June, 2023, that implemented the EMR. A total of 25 EMR users (physicians, health officers, pharmacists, nurses, laboratory technologists, radiology technicians) were included in the key informant interviews. The interviews were audio-recorded, transcribed verbatim, translated to English, and exported to OpenCode 4.03 software for analysis. Thematic analysis was applied to analyze, summarize, and present the data.
Results
Healthcare providers reported barriers operating at three levels: individual, technological, and organizational. Individual barriers included lack of digital literacy, technical knowledge, skill; motivation; and favorable attitude. Technological barriers included lack of infrastructure including computers, networks, and reliable power supply; and software-related challenges such as system downtime, lack of interoperability, comprehensiveness, and decision support systems; and system security and privacy concerns. Organizational barriers included poor quality of training, lack of follow-up, supervision and technical support; poor leadership commitment; lack of incentives and motivation; and staff turnover and workload. Perceived benefits of the system, such as ease of access to quality data, improved quality of care and work efficiency; availability of onsite technical support; presence of information technology supplies; and feedback from supervisors, were identified as facilitators of EMR adoption.
Conclusion
The study identified different barriers and facilitators to the adoption of the EMR. The health system should prioritize strategies to address technological, individual, and organizational factors influencing the successful adoption of the EMR to support the delivery of quality care and improve patient outcomes.
Introduction
Digital technologies can enhance healthcare delivery and address the challenges faced by health professionals. There is widespread implementation of the electronic medical records (EMR) system in healthcare settings. EMR is set to replace the current widely used paper-based medical recording. 1
EMR helps collect, store, and display information and helps automate medication and laboratory exam ordering processes, ensuring standardized, readable, and complete orders. It may include a decision support system (DSS) that provides up-to-date medical knowledge, reminders, or other actions that aid healthcare providers in decision-making at service delivery points. EMR may also improve communication among healthcare providers. 2
EMR enhances the efficiency of the healthcare system, promotes patient safety, and improves patient outcomes and healthcare quality by enhancing healthcare providers’ adherence to guidelines and allowing real-time access to patient health records.3, 4 Recent studies show an association between EMR use and improvements in health outcomes, including mortality and morbidity. The reported improvement was due to a reduction in medical errors, easier access to clinical DSSs, improved communication between healthcare providers, and enhanced information management.5–7 It is also reported to improve healthcare productivity and efficiency. 8 When properly implemented, EMR has the potential to reduce medical costs associated with medical errors, adverse drug events (ADEs), and inefficiency.9, 10
Implementation of EMR is a slow and complex process. Successful adoption requires consideration of a range of technological, individual, and organizational factors.11, 12 Studies identified various factors influencing the successful adoption of the EMR system: design or technical concerns including hardware, software, system problems (e.g., slow system speed, unplanned downtime); user-friendliness or usability13–18; access to internet connectivity, computers, and electric power12, 17–19; privacy and security issues12, 18–22; cost (high startup and ongoing maintenance cost), time, workload, and productivity12, 19, 22, 23; interoperability 17 ; training, technical support, knowledge, and familiarity with EMR17, 19,24–26; and willingness, resistance to change, and attitude of healthcare professionals.12, 18, 19, 25, 27
Ethiopia started the implementation of EMR in 2013. Despite efforts to encourage the adoption and use of EMR, the pace of adoption and use has been inconsistent and suboptimal across providers and health facilities. A systematic review and meta-analyses done in Ethiopia also revealed that only half (51.85%) of the healthcare professionals are ready to use EMR. 28 This study explored the barriers and facilitators of EMR adoption among healthcare providers.
Methods and materials
Study design, setting, and period
The study used a descriptive phenomenological approach to explore the barriers against and facilitators of EMR adoption. The study was conducted at selected EMR-implementing health facilities in Addis Ababa, Ethiopia. Accordingly, Tirunesh Beijing General Hospital (TBGH) and three health centers, namely: Kazanchis, Saris, and Ferensay health centers were included. These health facilities implemented the Bahmni EMR. Data were collected from June 5–13, 2023.
Study population and eligibility criteria
Physicians, health officers, pharmacists, nurses, laboratory technologists, and radiology technicians participated in the study. Healthcare providers aged 18 years or older who consented to participate in the study and used EMR for at least six months were included. Health professionals who were not available during the data collection period were excluded from the study.
Sample size and sampling method
A total of 25 key informant interviews (KIIs) were conducted among healthcare providers working in the selected health facilities. The healthcare providers were selected through a purposive sampling technique considering their level of EMR experience and profession. Accordingly, five physicians, five pharmacists, five nurses, five laboratory technologists, three radiology technicians, and two health officers were included. The interviews were conducted until a point of data saturation was reached, which was achieved after 25 KIIs.
Data collection tools and method
A KII guide was developed, pretested, and used to explore the lived experience of EMR users. The English version of the guide was translated into the local language (i.e., Amharic) for data collection. Before data collection, the KII guide was pretested, and based on the input from the pretest, revisions were made to the guide. Data collection was carried by three trained medical doctors (two females and one male), all experienced in qualitative data collection and familiar with EMR implementation in Ethiopia. The data collectors received a two-day training along with a simulation. Relationship was not established with the study participants prior to the start of the study. The study participants were informed about the interviewer, the study objectives, and informed consent was taken before initiating the data collection process. The data were collected at their workplace using face-to-face interviews and were conducted in an environment that ensured privacy. Probing questions were used to explore the barriers and facilitators in detail. The interviews were audio-recorded, and supplemental notes were taken. The KIIs were conducted until data saturation was reached, which was achieved with the 25 KIIs. The interview lasted 45 min on average.
Data analysis
The data were transcribed verbatim in Amharic, the interview language, and then translated into English. To ensure consistency, the translated data were cross-checked with the audio file. The data were exported to OpenCode 4.03 software for analysis. Line-by-line coding was done by four experienced coders, and thematic analysis were used to analyze, summarize, and present the data. Themes were identified until saturation was achieved. In addition, representative quotations were included to provide context for the themes.
Data quality assurance and management
Credibility was ensured through probing, the use of experienced data collectors who were familiar with the implementation of EMR, training of data collectors, in-depth methodological description, and ensuring the adequacy of the data (saturation). The research team carefully read the information obtained from individual interviews and field notes. All information provided by the participants was fully presented. Participant validation was also made by returning the transcripts to participants to check for accuracy and resonance with their experiences, and their feedback was considered. To ensure transferability, a detailed and complete description of the data and context was provided.
Ethical approval and consent to participate
This study was approved by the Ethical Review Committee of the Addis Ababa City Administration Health Bureau (Approval number AAH/8448/227, dated January 23, 2023). Permission was granted by the heads of the health facilities before data collection. Written informed consent was obtained from key informants after explaining the study objectives and data confidentiality issues before the study. Identification data, such as names, were not collected to ensure the anonymity of the information. The transcripts of each respondent were given unique codes to maintain the confidentiality of the information relating to each participant. The KII recordings and transcripts were stored on a password-protected computer to ensure confidentiality of the information.
Result
Socio-demographic characteristics
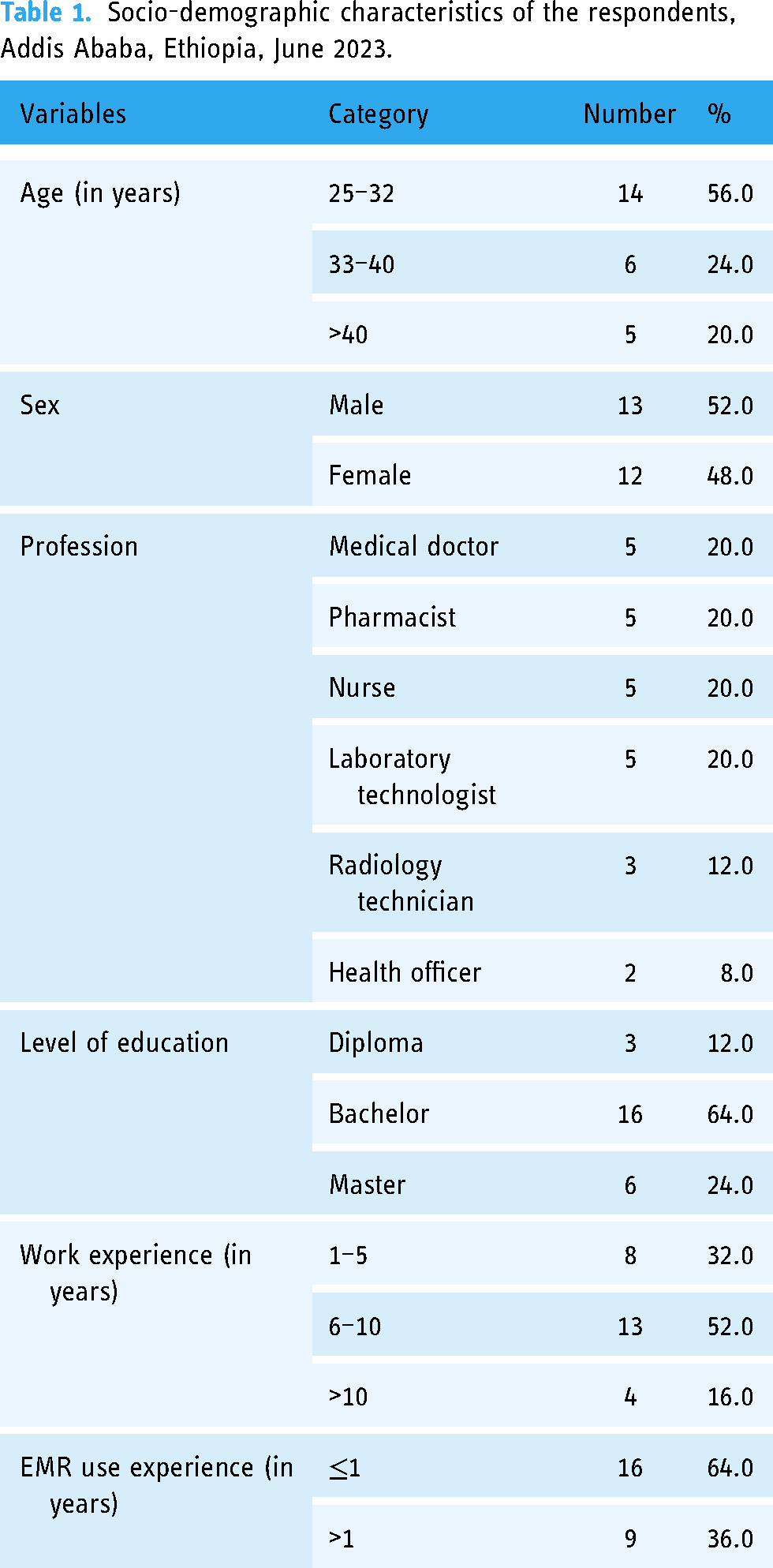
A total of 25 KIIs were conducted with EMR users, including physicians, health officers, pharmacists, nurses, laboratory technologists, and radiology technicians. The mean (±SD) age of the participants was 33.8 (±6.08) years. More than half of the participants (52.0%) were male. The majority (64.0%) held a bachelor degree. The mean (± SD) duration of professional and EMR use experience of the participants was 1.24 (±0.53) years and 7.16 (±4.02) years, respectively (Table 1).
Socio-demographic characteristics of the respondents, Addis Ababa, Ethiopia, June 2023.
Barriers and facilitators of EMR adoption
During the analysis, three themes and four subthemes emerged that explain the barriers to EMR adoption, while four themes emerged that describe the facilitators of EMR adoption (Table 2).
Major themes, themes, and subthemes.

Barriers against EMR adoption
This study identified various barriers against EMR adoption operating at different levels. Three major themes emerged during the data analysis explaining the barriers against the adoption of EMR by health service providers: individual, technological, and organizational barriers. Individual barriers included lack of digital literacy, technical knowledge, skill; motivation; and favorable attitude. Technological barriers included lack of infrastructure including computers, networks, and reliable power supply; and software-related challenges such as system downtime, lack of interoperability, comprehensiveness, and DSSs; and system security and privacy concerns. Organizational barriers included poor quality of training, lack of follow-up, supervision, and technical support; poor leadership commitment; lack of incentives and motivation; and staff turnover and workload.
Individual level barriers
Individual-level barriers such as poor digital literacy, lack of knowledge and skill about EMR, resistance to change, and lack of motivation and commitment were identified as barriers to EMR adoption.
Digital literacy
Digital literacy encompasses the skills and knowledge necessary to effectively use digital technologies, including computers and software applications. Healthcare providers need to have these skills to navigate various sections of a digital system. This also includes basic computer skills, such as proficient typing, to capture patient medical information, notes, and prescriptions. However, a significant number of healthcare providers in Ethiopia lack basic computer skills due to lack of access or adequate training. Most respondents mentioned that this general lack of computer skills has hampered the adoption of EMR. The main problem I see, both as a country and as an institution, is that health professionals don’t have adequate computer skills. There are people with 20 years of experience who have no clue about it. Due to this, it takes us longer to record patient data on the system. So we usually record on the system after serving the patients, we don’t do it alongside treatment since we don’t have adequate skill to do it simultaneously. (Nurse from Tirunesh Beijing General Hospital). Basic computer skills are mandatory for effectively using EMR. Most health professionals lack these skills. I believe that incorporating basic computer skills training during the introduction of EMR would have significantly eased the transition process. (Physician from Ferensay Health Center)
EMR knowledge and skill
The EMR is a complex system that requires adequate training and post-training follow-up to equip healthcare providers with the necessary knowledge and skills to effectively use the system. Lack of technical knowledge and skills to use EMR was reported as a barrier to the adoption of EMR by most of the respondents. During the implementation phase, more comprehensive training should have been given. We currently have a skill gap to use the system. I strongly believe that additional training is still required. (Nurse from Saris Health Center) The most significant weakness I have observed so far is the lack of training. Some individuals continue to make errors in filling out essential details such as age, name, and address in the EMR. The absence of proper training has hindered our ability to work in a more coordinated and synchronized manner. (Physician from Tirunesh Beijing General Hospital) My knowledge and skills about digital tools are limited because we are not trained at the university level. It would be beneficial to incorporate EMR into the university's training curriculum by allocating dedicated credit hours. (Laboratory technologist from Kazanchis Health Center)
The system is a bit complicated compared to the previous system. My knowledge and skills are also poor since I didn’t receive proper training. Due to this, it is taking us more time to record. It is better to simplify the system for easy navigation and use. There should also be a dedicated technical support team to quickly address questions from the users’ side. (Health Officer from Saris Health Center)
But what I am worried about is that since the implementation of EMR, we have decreased our face-to-face contact with the patient. We do not give more time to the patient; rather, we spend our time on desktops. This is because of poor knowledge and skill. (Physician from Tirunesh Beijing General Hospital)
A significant number of individuals lack EMR knowledge, and it has become frustrating to use the system because of its complexity. This is slowing our work and potentially impacting workflow efficiency. (Physician from Ferensay Health Center)
Motivation
Motivation drives behavior change, influences others, and ensures that adoption efforts are sustained over the long term. Due to a lack of necessary knowledge, skills, and infrastructure, some healthcare providers are not motivated to use the EMR for patient care. Staff are becoming demotivated to use the system. The lack of motivation comes from power interruptions and inadequate computers. Sometimes one has to wait a long time to get a computer. (Physician from Tirunesh Beijing General Hospital) The poor infrastructure in our facility is discouraging. People at the top are not committed to providing us with the necessary infrastructure. Ideally, EMR is expected to reduce the time it takes to provide service, but in reality, because of poor infrastructure, we are not seeing that effect. (Physician from Saris Health Center)
User attitude
Resistance to adopt new behaviors was reported as a barrier to EMR adoption. A few of the respondents mentioned that healthcare professionals are not willing to use the system because they are doubtful about its benefits. They also believe that using EMR is time-consuming and burdensome compared to paper-based records. There are health professionals who perceive that using the system is a burden rather than a benefit. At least awareness creation about the advantages and disadvantages of digital technologies is important. (Physician from Kazanchis Health Center) There was a challenge at the beginning because there were employees who were resistant to accepting the system. (Nurse from Saris Health Center)
Technological barriers
Healthcare providers included in this study reported various technological barriers hindering the adoption of EMR. These barriers included lack of infrastructure, including computers, networking, and power supply, and software-related challenges such as system downtime, lack of interoperability, user friendliness and comprehensiveness of the EMR, and security and privacy concerns.
Lack of infrastructure
Robust infrastructure, such as computers, networking, and power supply, is needed for a proper transition from paper-based records to EMR in healthcare. It ensures consistent use of the system, supporting the delivery of high-quality patient care. It also provides a foundation for secure and efficient exchange of patient information that enables data-driven decision-making. However, shortage and low processing capacity of computers, networking problems, and frequent power interruptions hindered the adoption of EMR.
Computers. Consistent use of EMR requires computers in sufficient quantity and quality. Most healthcare providers reported that the number of computers available at health facilities is limited, hindering the widespread adoption of EMR. The storage and processing capacity of the available computers was inadequate. This slowed the performance of the system during patient care, compromising the quality of care and patient outcomes. The staff are motivated to use EMR. What is hindering the use of EMR is a problem with infrastructure. The available computers are inadequate and have poor storage capacity. It takes longer to open and work on the EMR system. (Nurse from Tirunesh Beijing General Hospital) The computers we have here are slow and are also old. They [health facility administration] should replace the old ones with better-capacity computers. (Laboratory technologist from Saris Health Center) Unavailability of sufficient computers during the introduction of EMR posed a significant challenge. Ideally, all necessary supplies should have been made available from the start to ensure a smooth transition from the paper record to EMR. (Physician from Tirunesh Beijing General Hospital) Due to the shortage of computers, some departments in the health facilities are not integrated. This forced health providers to switch between paper-based records and the EMR, hindering continuous use of the system for service delivery. It also increased healthcare providers’ workload and constrained their time for patient counseling, compromising the quality of service. The system by itself is good but now since we are working both on paper and on the system it has somehow increased the workload. It is taking our time and we are not counseling our patients properly. However, I believe that we are in a transition period and everything will be corrected in the future. (Pharmacist from Ferensay Health Center)
It would be beneficial if we could access the system on phones or tablets. This would increase flexibility and allow us to access patient information and input data more conveniently, especially in situations where desktop computers or laptops are not readily available. (Physician from Ferensay Health Center)
Networking. Storing, accessing, and sharing patient information requires a connected workstation. However, most EMR users reported that the local area network installation in the health facilities was reported to have been problematic, resulting in significant delays in the transmission of patient information from one department to another during service delivery. Sometimes the medication we prescribe using the system can’t be delivered to the pharmacy. The same is true for laboratory test orders. The test request usually failed to reach the laboratory department on time. These problems are delaying the service we deliver to our patients. (Physician from Tirunesh Beijing General Hospital)
Power supply. Continuous use of EMR requires an uninterrupted power supply to allow continuity of patient care. In most health facilities, the electric power could blackout unpredictably and sometimes be out for hours with no alternative power source. This hinders the continuous use of EMR for patient care. This also causes service interruptions as it takes longer to restart the system and resume activities. The main barrier we are facing is frequent interruption of power. We can’t predict it. It happens at any time. Since we are working fully paperless, system and service interruption occurs when the power is interrupted. (Nurse from Ferensay Health Center) Before the implementation of EMR, shortages of paper and other print materials were the major challenges. However, after EMR, new challenges have arisen. Infrastructure, especially power outages, is a big obstacle we have now. We have a generator, but it takes time until the system restarts. (Physician from Kazanchis Health Center)
During electric power outages, health facilities rely on generators as a backup power source. However, one EMR user reported that sometimes due to a shortage of fuel, generators could not provide an alternative power supply. One time the light went out and no fuel was available at the time. We faced a lot of challenges during that time. Even if fuel was available, it took time until the generator worked and the system restarted. Patients don’t usually believe us when we tell them to wait for a while until the system is fully functional. (Nurse Ferensay Health Center)
The frequent power interruption also caused the system and hardware to fail or restart, resulting in the loss of patient data, delaying health service, and causing dissatisfaction and disappointment among patients. …during a power outage, the service we provide is delayed until the generator is activated and the system restarts. (Physician from Kazanchis Health Center) …the power interrupts frequently. We even faced system failure due to frequent power interruptions. Sometimes, you may not get the data that you have entered after the system restarts. (Physician from Tirunesh Beijing General Hospital) Infrastructure plays a crucial role in the utilization of the EMR system. For instance, the power interruption causes patient dissatisfaction due to delays in service until the generator is activated. (Nurse from Ferensay Health Center)
Software-related barriers
Software includes the programs, applications, and algorithms that enable data processing, analysis, and decision-making. It is also important in ensuring the security and privacy of patient data. Healthcare providers reported one or more of the following software-related barriers hindering EMR adoption: system downtime and complexity, lack of interoperability, comprehensiveness and user-friendliness of the system, and data security and privacy concerns.
System downtime. Frequent downtime, delays, or system freezes were reported as major impediments to adoption by most of the respondents. Such challenges delay activity processing time and cause discomfort among users, delaying its adoption. It also causes service interruptions, affecting the quality of care and patient outcomes. Sometimes we face difficulty logging into the system, and it takes longer to change the page from one patient to another. There are times when the system becomes slow, and sometimes it totally stops working for hours or even all day. If it stops working, we go back to the paper to continue providing service to the patients. (Physician from Tirunesh Beijing General Hospital) Technical issues, such as system downtime or slow performance, are also a challenge. Addressing these technical issues promptly and providing comprehensive training helps staff develop trust and confidence in the system. (Laboratory Technologist from Saris Health Center)
The system usually gets interrupted; there can be a problem on the server, and in such cases, working on paper is the only solution we have as a backup. Which means we’re moving backward. There is also a shortage of trained IT personnel to respond quickly. (Physician from Tirunesh Beijing General Hospital)
User-friendliness. EMR design and development requires an understanding of needs and contexts to enhance the usability of the system by healthcare providers. Some respondents mentioned that the EMR software is not user-friendly. This implies the need to engage end users in the design and development process and collect feedback for continuous system improvement. The EMR system is not user-friendly and complex. It is becoming a burden and hindering our ability to provide quality patient care. Additionally, we commented that it would be beneficial for the system to have a drop-down option for some data instead of manual entry. This can ease our burden and save our time. (Laboratory Technologist from Tirunesh Beijing General Hospital) First, it is better to study well about how we used to work using paper, then health care workers should be involved in the development of the system. It is crucial to listen to the feedback of healthcare workers. (Laboratory Technologist from Saris Health Center)
Standard operating procedures are not integrated into the EMR system yet for some of the procedures. So, I face difficulty when using it. I believe that integrating these procedures into the EMR would enhance efficiency and overall workflow. (Laboratory technologist from Tirunesh General Hospital)
Interoperability. Reporting requires systems to seamlessly exchange information with each other. The lack of interoperability between EMR and DHIS2 was reported as a major impediment to adoption by most of the respondents. This forced users to generate reports manually, making their work cumbersome and time-consuming. There are some issues that need solutions. EMR is not integrated with DHIS2. So, when we want to send a report to the higher officials, we copy the data from EMR to the tally sheet and then enter it into DHIS2 for reporting. Using both the EMR system and paper is a burden to us. (Physician from Tirunesh Beijing General Hospital, Addis Ababa)
Comprehensiveness. Some respondents mentioned that the EMR software did not meet their specific needs. The system lacks standard laboratory tests, units of measurement (SI units), and biological reference values for some tests. There is also a lack of frequent content updates. This hinders EMR adoption, as it requires resorting to the paper-based record system. The system lacks SI units and biological reference ranges for the tests we do. The other is that there is no functionality for revising your test results. The system should enable healthcare professionals to allow test revision, indicate the reason for revision, time and date stamp, and put a signature. (Laboratory technologist from Tirunesh Beijing General Hospital) …the area that needs some adjustment is the investigation format, which I have discussed with IT technicians. There are some missing investigation types, and we have discussed this. We hope they will update it soon. (Physician from Kazanchis Health Center)
Lack of space to provide feedback or discussion for radiological findings and enter laboratory test results done at diagnostic centers outside the health facility was reported as a challenge to EMR adoption by some respondents. There is a problem with the radiology section. It has no space to write comments, and radiologists use paper to write the comments, conclusions, and recommendations. (Radiology Technician from Tirunesh Beijing General Hospital) The system is not well developed yet and it still needs to be upgraded. For example, X-rays and ultrasounds aren’t available in our facility but we send it to another facility. After receiving the results, we are unable to upload it to the system. If it was done in our facility, it would have been easier. But radiology or ultrasound results from outside of the institution can’t be uploaded. (Physician from Saris Health Center)
DSSs such as alerts and prompts improve patient safety, enhance clinical decision-making, increase efficiency, and facilitate compliance with standard treatment guidelines and patient care requirements. Respondents expected the system to include prompts or alerts. However, some respondents in some facilities reported that this expectation was not met. This compromises engagement with the system, reducing its benefits and hindering its adoption. The system is incomplete. Our EMR lacks prompts or alerts to enhance clinical decision-making. There are no time stamps for both test entry and completion (time in and time out) that would provide a comprehensive overview of the testing process and aid in efficient patient care coordination. (Laboratory technologist from Tirunesh Beijing General Hospital)
Data security and privacy. Some respondents perceive that EMR is not reliable for storing patients’ information, as unauthorized access to patient data could be possible. They also believe that storing patients’ information in EMR poses a risk of malicious attack, compromising the security and privacy of patient information. The concern I have with the system is patient data security and privacy issues. Anyone can access recorded data on the system. There may also be a virus attack. The system may also be damaged by a virus, and we may lose the data. This is not an issue with the paper-based record. (Physician from Kazanchis Health Center, Addis Ababa) Patient data security is a major threat. The system doesn't have a backup system. So, we may lose everything if damage occurs. So, the authorities should provide a means to ensure data security and privacy. (Health Officer for Saris Health Center)
Organizational level barriers
A supportive organizational culture can promote continuous use of EMR by providing the necessary resources and ongoing support for users. However, organizational-related barriers such as inadequate training, lack of technical support and post-implementation follow-ups such as supervision and mentorship, staff turnover and workload, lack of support from colleagues, and poor leadership commitment were reported to have challenged the smooth implementation of EMR.
Training
Proper and consistent EMR training for end users is required to effectively use the system during service delivery. However, most EMR users reported the training provided was inadequate to equip them with the required level of knowledge and skill to effectively use the system. Short duration of the training, lack of follow-up and on-site support, and a lack of tailored support to the different professional categories were reported as major impediments. Initially, we were given on-the-job training. I can’t say we were given adequate training. They just gave us a half-day orientation, and I do not believe that it is enough. We learned to know more about the system after we started working on it. (Pharmacist from Ferensay Health Center) The training I received on EMR was insufficient. I was only provided with a training session lasting 25 to 30 minutes, which is inadequate. We need additional training to effectively navigate and make use of EMR. (Nurse from Saris Health Center) I joined the hospital after EMR was implemented. But what I heard from other colleagues is that the training was not adequate. It was also given to all professionals in the same way, without considering their knowledge and skill levels. I usually hear them complaining that even those who are here to help are not well-trained. (Physician from Tirunesh Beijing General Hospital) There was no training. Initially, 3 people took training, and after the implementation of EMR, those people showed us how to use the system. Otherwise, there was no well-organized training, including time for practice. (Physician from Kazanchis Health Center)
Post-implementation support, including on-the-job training, mentorship, and supervision, can help EMR users overcome challenges, develop new skills, and build confidence, ensuring consistent use. However, user training was not sufficiently maintained after implementation. The post-training follow-ups given in the form of supervision and mentorship were also inadequate to ensure consistent use of EMR for service delivery. One-time training is not enough. Giving training a few times a year is a must. For example, there are new staff and new graduates, they basically don't even know how to use computers. Regular training and follow-up is a must. (Pharmacist from Ferensay Health Center) The training we received at first was not sufficient. So we didn’t perform well at first. We need further support. When we request further support, they consider it as if we didn’t want to work using the system. (Pharmacist Tirunesh Beijing General Hospital) It would have been better if orientation was given to all staff about EMR and its benefits. Continuous training and support should have been given. If these were done, our work would have been easier. (Physician from Tirunesh Beijing General Hospital) The best way to encourage healthcare workers is by raising awareness about the benefits of EMR and offering ongoing training. I haven’t seen any kind of training since I started working here. I recommend conducting training sessions at least every quarter to keep us updated. (Physician from Ferensay Health Center)
I don’t think the training we received was adequate. In addition, only half of the staff were trained. So, we need at least a module so that it can be used as a guide when using the system. (Nurse from Ferensay Health Center)
Technical support
Continuous use of the system requires the availability of onsite technical support. In some health facilities, a shortage of well-trained IT technicians who can provide timely maintenance and troubleshooting services was mentioned as a barrier to EMR adoption. There is a shortage of IT personnel with in-depth knowledge. One of the major barriers we face when using EMR is technical issues like system delays. This is precisely why we need IT personnel to help address these technical challenges, ensure system stability, and provide support during such interruptions. (Physician from Ferensay Health Center) In our setting, while there is technical support, I don’t believe it's enough. Having dedicated IT personnel available to quickly address EMR-related issues is needed. It will encourage us to use the system. (Health officer from Saris Health Center) Having only one person responsible for technical support, who likely has other duties as well, does create challenges in accessing timely assistance, particularly during duty hours. This gap in technical support is impacting the smooth functioning of the EMR system. (Physician from Tirunesh Beijing General Hospital)
Staff turnover
Staff attrition and the inability to get a suitable replacement on time is hindering the adoption of EMR at health facilities. Some of the study participants reported that high turnover of trained staff challenged the smooth implementation of EMR at their facilities. I want to highlight the shortage of human resources and the significance of training. A shortage of trained personnel is affecting our operations; addressing this and providing comprehensive training could greatly enhance our effective use of EMR. (Nurse Saris Health Center) We received training. But the high staff turnover is affecting us. It is difficult to get trained. (Laboratory Technologist from Kazanchis Health Center)
Workload due to high patient flow affects your use of EMR. There is a shortage of human resources; most of the time, for example, during an emergency, it gets out of control, and we can’t use the system in such cases. (Nurse from Saris Health Center)
Workload
Coupled with the shortage of trained staff, capturing patient medical information on paper and in the system at the same time is believed to have been both time-consuming and burdensome. This may cause resistance among healthcare providers due to the burden of data collection, further affecting EMR adoption. I would rather say I didn’t get any benefits from the system in this department. Since we are using both the manual and digital system we still face challenges to deliver the quality service. I personally think it has increased our workload and is also time consuming. (Pharmacist from Tirunesh Beijing General Hospital) The fact that it has not yet become fully paperless is causing another burden to us. We also use prescription on paper. Service payment and community based health insurance are also registered on paper. (Pharmacist from Ferensay Health Center)
Attitude
Unfavorable attitudes and the resistance of colleagues to use EMR were reported as hindrances to its adoption by few respondents. This may create a non-conducive work environment and frustration and demotivation among healthcare providers, further delaying the adoption process. …some staff are negligent and reluctant to try new things. This negatively influences you not to use the system. (Pharmacist from Tirunesh Beijing General Hospital) It's important to work on their mentality before implementation. It's hard to force anyone to use the system if they have a negative attitude about it. There should be strict supervision that will track our progress as well. (Nurse from Ferensay Health Center)
Incentives
Users need to be motivated and engaged in the EMR adoption process to ensure successful implementation of the system. However, some EMR users reported a lack of incentives and a supportive work environment as barriers to adoption. Staff have a positive attitude towards EMR; they have positive feedback about it. However, I have not seen incentives being given to encourage the use of EMR. (Radiology Technician from Tirunesh Beijing General Hospital) There is no motivating factor in the facility. Giving incentives to those who do well and addressing concerns can motivate others to accept the system. (Health Officer from Saris Health Center)
Using champions as a role model can enhance the adoption and use of EMR in healthcare settings. Their motivation, expertise, and leadership help overcome barriers and drive adoption. Some respondents mentioned that such practices have not been implemented in the health facility where they work. There is no platform for sharing successful experiences. Encouraging those who have successfully integrated EMR into their workflows to share their insights can inspire others to adopt the system. (Laboratory technologist for Kazanchis Health Center) Promoting the long-term benefits of EMR is crucial. Supervisors and leaders should share their experiences and provide regular support to encourage and motivate others to use it. (Physician from Tirunesh Beijing General Hospital)
Leadership commitment
Leadership commitment helps establish a conducive environment for a smooth EMR adoption among healthcare providers by providing necessary resources, technical support, and guidance. The lack of commitment to provide necessary infrastructure and resources, including budget, was mentioned as a major impediment to EMR adoption by most of the respondents. Commitment issues from the health facility administration side are also a challenge. They have to divert the money that used to be spent on paper to the system. They have to invest in some important infrastructure. They also have to advocate for the benefit of using EMR. (Pharmacist from Tirunesh Beijing General Hospital) The other thing is that those in administrative positions don’t know the benefits of the system well. They are not initiating others to use the system. I am saying this because if those in higher positions know the system very well, it can be easier to motivate others to use it. (Pharmacist from Tirunesh Beijing General Hospital)
Lack of commitment from higher officials is the other obstacle. Higher officials and leaders are not committed to seeing the benefits and making the system mandatory in all departments. They should be responsive to our questions and not consider us as if we hated the system. (Laboratory Technologist from Saris Health Center)
EMR use has not been made mandatory in all departments of a health facility due to a lack of integration and the necessary infrastructure, such as computers. There is also a lack of standardized guidelines that guide the proper transition from paper-based records to EMR. As a result, healthcare providers are switching between paper-based record and EMR, hindering progress toward a paperless initiative. The lack of well-facilitated setup is a challenge. The policy should focus on equipping health workers with the required skills and make sure that the setup of health facilities is convenient and the minimum standards are met for the implementation of EMR. There is also no standardized guideline to guide the implementation of EMR. (Laboratory Technologist from Saris Health Center)
Facilitators of EMR adoption
This study also explored the facilitators of EMR adoption. Perceived benefits of EMR, the presence of IT supplies and onsite technical support, and supervisory feedback were identified as major facilitators of EMR adoption.
Perceived benefit of EMR
Effective implementation of EMR ensures easy access to quality data for clinical decision-making, improves quality of care, and enhances work efficiency. One or more of these benefits were reported as facilitators for the adoption of EMR.
Data quality and accessibility
EMR cannot only provide easier access to patient medical information but also to improve the quality and reliability of the information. Most EMR users reported that the system facilitated real-time availability and remote access to patient information for clinical decisions. This improvement in access to quality data was reported as a facilitator of EMR adoption. It generates accurate data and increases data quality. You can also access the information you need easily from the system. This is motivating. It encourages you to use the system. (Physician from Saris Health Center) The implementation of EMR has significantly decreased the occurrence of human errors, contributing to more accurate and reliable patient information. (Laboratory Technologist from Tirunesh Beijing General Hospital)
First of all, it has significantly reduced our workload. It also avoided the loss of patient cards due to damage over time. Moreover, the risk of losing patient data has notably decreased since implementing EMR. We can now easily access patient data when we need it, especially during follow-up and readmission. (Nurse from Saris Health Center)
Quality of care
In addition to improved access to quality data, most healthcare providers reported that EMR also leads to better quality of care by reducing patient waiting time and facilitating interdepartmental communication. This ensures the timeliness of care and improves patient satisfaction and outcomes. The quality of service has significantly improved because EMR reduced patients’ waiting time and enhanced patient experience by minimizing inconvenience. Furthermore, it has facilitated communication with other departments such as the emergency room, radiology, and pharmacy. This is really encouraging. (Physician from Tirunesh Beijing General Hospital) The implementation of EMR has significantly reduced the time patients spend waiting to get services. It is also easier to exchange information between different departments. (Physician from Ferensay Health Center)
EMR enhances communication among healthcare providers. It also stimulates networking and care coordination by actively seeking input from experts, potentially improving the quality of care. EMR is now integrated with pharmacy, and this integration has facilitated our work. We can directly communicate with the pharmacy to order medication. (Physician from Kazanchis Health Center, Addis Ababa) The system made our communication with our patients and other providers easier. I can easily communicate with my patients and other providers serving in other sections. (Physician from Tirunesh Beijing General Hospital) …additionally, EMR allows better coordination among healthcare teams, minimizing errors and ensuring comprehensive patient care. (Laboratory Technologist from Kazanchis Health Center)
They also reported that EMR offers faster turnaround times for laboratory and radiological test results, improved traceability of test results, and avoided the risk of results being lost, improving service quality and patient outcomes. EMR is highly beneficial for both us (service providers) and patients. It takes less time to receive lab requests and send the results. So, it reduced waiting time and enhanced patient experience by minimizing inconvenience. (Laboratory Technologist from Kazanchis Health Center) Previously, there were instances where patients’ results were lost or interchanged. The system avoided such problems. (Laboratory technologist from Tirunesh Beijing General Hospital)
Work efficiency
The implementation of EMR in health facilities streamlined activities such as patient history recording and retrieval, appointment scheduling, billing, and documentation, saving significant time and energy for healthcare providers. This was mentioned as a facilitator of EMR adoption by most of the respondents. Using EMR facilitates our activities and also saves time in the process. It helps you simplify a lot of processes. The system helps us easily identify the patient's history, including the total payment expected from the patient. It can also help in saving time and resources and improving performances. (Physician from Tirunesh Beijing General Hospital)
The benefit we get from the system is encouraging. It reduces costs, like the cost of printing paper. (Physician from Kazanchis Health Center)
The workload before and after EMR is incomparable. Before EMR, we had a lot to do, like fill out a logbook. But after EMR, we are not expected to do this. It has modernized our work process. Now we can do our tasks easily and in a short time. (Radiology technician from Tirunesh Beijing General Hospital)
EMR decreased our workload and also saved time. Tasks like recording test results, and patient details, and sharing information required multiple steps. With EMR, these processes have become very easy. Most tasks that previously demanded more of our time are now done easily. This allowed us to focus more on conducting accurate tests and providing quality services. (Laboratory Technologist from Tirunesh Beijing General Hospital)
IT supplies
The availability of adequate IT supplies, such as computers, accessories, and internet connections, is critical for the effective implementation of EMR in health facilities. Although in short supply, the availability of computers and internet connectivity is facilitating EMR adoption by healthcare providers. The availability of computers, connectivity, and nearby technical support, despite the limitations in quantity, is highly encouraging. Having these resources at hand enables us to effectively utilize EMR and address any technical issues promptly. (Physician from Tirunesh Beijing General Hospital) The MOH and other organizations supported us by providing additional supplies, like computers. This facilitated our use of the system, and we are planning to expand to other departments in the facility. (Physician from Saris Health Center)
Technical support
Onsite technical support facilitates EMR adoption by providing training to the users, troubleshooting, customization, and ongoing maintenance support during and after implementation. Few respondents mentioned that the availability of onsite technical support at a health facility facilitated the implementation and adoption of EMR. “We have technical support in place, including readily available EMR implementation personnel to assist during challenges. Their support, especially during the transition period, was extensive and facilitated the implementation of the system. (Laboratory Technologist from Tirunesh Beijing General Hospital) In our setting, we have a trained person who gives us technical support. His expertise in assisting with any EMR-related issues is encouraging. This support ensures that any obstacles we encounter while using EMR can be promptly addressed. (Laboratory Technologist from Kazanchis Health Center)
Support from supervisors
Feedback from supervisors can create a more supportive, caring, and positive work environment by promoting regular communication, problem-solving, accountability, and teamwork. It also helps develop professional skills and creates a feeling of support. Some respondents mentioned that, despite the challenges, the feedback from their supervisors encouraged them to continue using EMR. Our facility actively communicates the benefits of EMR continuously. Supervisors continuously encourage us by telling us how EMR can enhance patient care and improve collaboration among healthcare professionals. Their support motivates us to use the system. (Health Officer from Saris Health Center) We communicate with each other about the system, even with our supervisors and higher officials. They also try their best to solve problems as quickly as possible and encourage us to use the system. The interaction we have, starting at the administrative level, is very good. As a result, there is an encouraging working environment. (Nurse from Ferensay Health Center) “The management and quality teams often motivate the staff and make sure that all are utilizing the EMR effectively. There is also a committee that checks the implementation of the system.” They try their best to solve the challenges. (Pharmacist from Tirunesh Beijing General Hospital)
Discussion
This study explored barriers and facilitators of EMR adoption among healthcare providers in Ethiopia. EMR users reported various barriers operating at different levels: technological, individual, and organizational. They also reported some facilitators of EMR adoption at health facilities.
Digital health literacy plays a crucial role in effectively utilizing digital health technologies. This study identified a lack of knowledge and skills in handling EMR, coupled with inadequate computer skills, as impediments to EMR adoption. Studies conducted in different countries also reported a lack of necessary knowledge and skills to use EMR as a major hindrance to adoption.11, 29–39 Digital literacy and technical knowledge and skills to use EMR are closely linked to the acceptance, use, and satisfaction of healthcare providers.29, 30, 38, 40 Healthcare providers are also hesitant to adopt EMR because they are doubtful about its reliability in protecting patient data. 11 Thus, comprehensive training should be provided to healthcare providers to build their technical capability, confidence, and trust in adopting EMR.
Shortage and limited processing capacity of computers, poor networking, and frequent power interruptions were identified as major infrastructural impediments as health facilities are not adequately equipped with the necessary infrastructure to meet EMR needs. This hindered the widespread adoption of EMR. Similar findings were reported in studies from both developed and developing countries.11, 30, 41 Implementing EMR requires a robust infrastructure, such as computers, networking cables, and reliable power sources. Prioritizing and investing in infrastructure is crucial to ensure a successful transition from paper-based records to EMR in healthcare settings, ultimately enhancing the quality of care and patient outcomes.42, 43
System downtime, delays, or freezes were reported as hindrances to EMR adoption. Studies conducted in Ethiopia, Nigeria, Japan, and America also reported system delays and unexpected downtime as impediments to adoption.31, 32, 44, 45 These issues can lead to service disruption, compromise data security, and patient safety, and introduce medical errors, impacting the quality of care patients receive. In addition, the unreliability of the system may cause frustration among healthcare providers, eroding their trust in using EMR for service delivery. Healthcare organizations should devise strategies to improve the reliability of EMR and implement suitable backup and recovery mechanisms to ensure swift restoration of patient data in cases of loss or corruption.
The lack of interoperability between EMR systems and DHIS2 was identified as a barrier to adoption, causing health workers to revert to paper-based reporting. Networking problems also impeded the smooth exchange of information and collaboration among healthcare providers. Our study findings align with studies conducted in developed and developing countries.29, 40, 46–51 In addition, the lack of comprehensiveness and the complexity of EMRs have posed further challenges for healthcare providers. Studies also revealed that healthcare providers are resistant to adopting technology that doesn't serve their specific needs. Complexity of screens, options and navigational aids was also reported as an impediment.33, 42, 52–54 A collaborative effort involving authorities, healthcare organizations, and system developers is essential to enhance the interoperability, customizability, and usability of EMR, and to establish a connected and efficient healthcare ecosystem.
Implementing digital technologies in healthcare requires careful planning and ongoing support. The lack of adequate training and post-implementation follow-up were major hindrances to EMR adoption reported in this study. Several studies have demonstrated a lack of training and technical support as obstacles to EMR implementation.11, 45, 50 This compromises healthcare providers’ confidence, resulting in frustration and a loss of interest in using EMR for patient care. Healthcare organizations should ensure that comprehensive training and ongoing support are provided to facilitate the effective implementation of EMR and fully leverage its benefits.
Workload, unfavorable attitudes, resistance from colleagues, and a lack of incentives were all hindrances to EMR adoption reported in this study. Leaders’ lack of commitment to establish robust infrastructure and provide necessary resources also hindered the adoption of EMR by healthcare providers. Studies reported that a positive work environment, coupled with incentives, is crucial for motivating healthcare providers to shift from paper-based records to EMR.34, 40, 55–57 More attention should be given to establishing a supportive work environment, including incentives to expedite the adoption of EMR. Leaders also need to be targeted in leadership training to help them guide the EMR and other digital health technologies implementation and adoption.
Perceived benefits of EMR over paper-record systems, such as easy access to quality data and improvements in quality of care and work efficiency, facilitated the adoption of EMR in this study. The availability of infrastructure, including hardware, and onsite technical support were additional facilitators for using the system. These findings are not peculiar to our study. Studies revealed that a higher perceived usefulness of the EMR system increases the end user's willingness to use the system. Improvements in communication or reporting, work efficiency, care processes, and data accessibility were identified as drivers of EMR uptake among healthcare providers.45, 46, 48, 49, 58–60 This underscores healthcare professionals’ recognition of the advantages that EMR offers in terms of patient care, efficiency, and overall practice management.
Strengths and limitations of the study
The qualitative nature of the study allowed a detailed exploration of barriers and facilitators of EMR adoption. The study also provided compelling evidence as it is based on users’ lived experiences of EMR use. However, the study was limited to Addis Ababa city only and may not reflect the situation in other parts of the country. Therefore, generalizing the findings to a larger population should be made with caution.
Conclusion
Healthcare providers reported various barriers operating at different levels: individual, technological, and organizational barriers. Individual barriers: lack of computer literacy, EMR knowledge and skill; lack of motivation; and unfavorable attitude. Technological barriers: lack of infrastructure, including computers, networking, and reliable power supply; software-related challenges such as system downtime, lack of interoperability, comprehensiveness, and DSSs; and data security and privacy concerns. Organizational barriers: poor quality of training, follow-up, and supervision; lack of technical support; poor leadership commitment; lack of incentives and motivation; and staff turnover and workload. Perceived benefits of the system, such as easy access to quality data for clinical decisions, improved quality of care and work efficiency; availability of onsite technical support; presence of information technology supplies; and feedback from supervisors, were identified as facilitators. Therefore, the health system should prioritize strategies to address technological, individual, and organizational factors influencing the successful adoption of the EMR to support the delivery of quality care and improve patient outcomes. In addition, further studies should be conducted to understand the benefits of EMR and its effect on service quality and patient outcomes.
Footnotes
Acknowledgments
We thank the United States Agency for International Development (USAID) for funding this study. We are also grateful to staff at the health facilities for their cooperation during data collection, and to all respondents for their willingness to participate in the study.
Author contributions
T.B., L.G, and T.B. were involved in conception and design of the study, data collection, analysis and interpretation, writing the article, and manuscript preparation. H.W., J.M., B.A., B.S., L.A., N.W., S.M., and B.D. assisted in data analysis and interpretation, and helped write and review the manuscript. All authors have given final approval of the version to be published, have agreed on the journal for submission, and accept responsibility for all aspects of the work.
Accessibility of data and materials
Data supporting the findings in this research article are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approval and ethical clearance was obtained from the Ethical Review Committee of the Addis Ababa City Administration Health Bureau (Approval number AAH/8448/227).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the United States Agency for International Development (USAID).
Informed consent
Written informed consent was obtained from key informants after explaining the study objectives and data confidentiality issues before the study.