
Abstract
Objective
Australia is committed to establishing a digitally enabled healthcare system that fosters innovation, strengthens data capabilities, and establishes a foundation for future digital health reform. This study provides a comprehensive overview of digital health implementation research in Australia, employing scientometric analysis and data visualization. We assess the existing knowledge base, identify key research areas and frontier trends, and explore their implications for healthcare delivery in rural and remote settings.
Methods
A systematic search of the Web of Science Core Collection database was conducted for relevant documents up to December 31, 2023. Analysis of annual growth patterns, journals, institutional and authorship contributions, reference co-citation patterns, and keyword co-occurrence was conducted using scientometrics to create outputs in the form of graphs and tables. Evolutionary analyses were undertaken to delineate the current knowledge base, predominant research themes, and frontier trends in the field.
Results
A total of 196 documents related to digital health implementation in Australia were identified, demonstrating sustained growth since 2019. The evolution of the field is characterized by four distinct phases, with a pronounced focus on telehealth, particularly in the context of the COVID-19 pandemic. ‘Remote health’ emerged as a significant area of contemporary interest.
Conclusions
This scientometric study contributes to our understanding of digital health implementation research in Australia. Despite a considerable body of research, there remains a relative paucity of studies focused on implementation in underserved rural and remote areas which arguably stand to benefit the most from digital health advancements. Continued research in this field is crucial to ensure equitable access to the benefits offered by digital health innovations.
Introduction
Digital health innovations are increasingly integrated across the healthcare landscape, offering substantial value in enhancing care, optimizing healthcare delivery, and improving overall health outcomes. 1 These innovations encompass a diverse array of technologies, including electronic health and medical records, 2 artificial intelligence (AI) and big data, 3 telehealth and virtual care, 4 mobile health (mHealth) applications, 5 and wearable devices. 6 The value of these technologies lies in their potential to streamline healthcare processes, increase efficiency, and empower consumers to actively engage in their own care. 7 When effectively implemented, the benefits of digital health innovations are likely to be most pronounced in underserved rural, regional, and remote areas, where access to healthcare remains limited.
In Australia, the government has committed A$951.2 million over 4 years to enhance digital health. 8 This funding aims to modernize the healthcare system and improve interoperability, introduce new digital health services, and advance data capabilities, while laying the groundwork for future digital health reforms. Additional investment will facilitate the implementation of various initiatives designed to promote the adoption of digital healthcare modalities, which gained prominence during the COVID-19 pandemic. This includes upgrading the national electronic health record system (My Health Record) and establishing the Australian Digital Health Agency to lead efforts in supporting the uptake and integration of technology, including the adoption of standards to improve interoperability of information transfer within the health system.
For digital health reforms to be effective, they must be tailored to the Australian healthcare system, enhancing the integration of health services and improving continuity of care for recipients. This underscores the importance of systemic and systematic implementation and evaluation of digital health, which presents several challenges. 9 Barriers such as interoperability, data privacy concerns, and resistance to change among healthcare professionals can obstruct the seamless integration of these technologies into existing health systems. 10 Achieving widespread adoption also requires addressing issues related to the digital divide, ensuring that all individuals, regardless of socioeconomic status, have equitable access to and benefit from digital health innovations.11–14 Overcoming these barriers necessitates collaborative efforts from policymakers, healthcare providers, technology developers, and other stakeholders to establish a supportive ecosystem for digital health. Despite these challenges, there are substantial opportunities to advance healthcare through the judicious implementation and support of digital health innovations. For instance, the integration of AI and machine learning algorithms can enhance diagnostic accuracy and treatment planning. 15 Remote patient monitoring and telehealth services offer the potential to extend healthcare access to underserved populations, particularly in remote or rural areas. Furthermore, digital health tools can facilitate preventive care and early intervention, ultimately reducing healthcare costs and improving overall population health. 16
Implementing digital health requires a dynamic and adaptive approach. The interaction between technology, end-users, healthcare teams, and settings inherently fluctuates and can experience significant variation over time. 17 It is also important to recognize that digital health technologies support broader healthcare needs, such as appointment scheduling, which are as crucial as the innovations themselves. Consequently, understanding the digital health implementation research landscape is essential for digital health users, providers, and health systems.18,19 As highlighted in a review by Hassan Mumtaz et.al., 20 ‘to address the challenges of digital health implementation, it is important to prioritize ethical research addressing issues of user consent and addressing socioeconomic disparities in access and effectiveness’(p. 1). This awareness is critical for anticipating future developments, preparing for new challenges, and strategically positioning health care systems for ongoing technological advancements. For instance, familiarity with digital health implementation research enables healthcare leaders, policymakers, and practitioners to make informed decisions about adopting and integrating digital health technologies, 21 informs strategies for optimizing health care delivery, 22 and provides evidence-based practices and guidelines. 23 These insights are crucial for ensuring that the integration of digital technologies into healthcare is grounded in research, thereby enhancing the reliability and effectiveness of implementation. Additional benefits include improved resource allocation and investment in technologies, 24 quality improvement initiatives and customized solutions to meet consumer needs, well-informed policies that foster innovation, address ethical considerations, and create an environment conducive to the successful integration of digital technologies in healthcare, 25 and strategies designed to reduce disparities and improve healthcare access for all. 26 Insights from research can guide the selection and implementation of digital health solutions that align with healthcare objectives.
In scholarly research, bibliometrics and scientometric analysis play pivotal roles in evaluating the impact and significance of scientific contributions. 27 Bibliometrics involves the quantitative analysis of publication patterns, citation counts, and collaboration networks, offering valuable insights into the scholarly landscape. Conversely, scientometric analysis explores the broader scientific community by examining patterns of research productivity, interdisciplinary connections, and the evolution of scientific disciplines over time. These methodologies can provide researchers with powerful tools to visually assess the influence and growth of scientific knowledge. As demonstrated by the work of Cronin and Meho, 28 bibliometrics and scientometrics significantly enhance our understanding of scholarly communication and the dynamics of scientific progress.
Currently, no studies offer a comprehensive overview of digital health implementation research in Australia or globally using bibliometric or scientometric analyses. While some studies have explored the broader aspects of digital health,29,30 or focused on specific technologies such as mHealth, 31 eHealth, 32 telehealth, 33 AI, 34 and digital medicine,35,36 or addressed particular health conditions, 37 these analyses have predominantly adopted a global perspective. This study aims to fill this gap by providing a detailed examination of digital health implementation research outputs in Australia through quantitative analysis and data visualization techniques. It analyses collaborative networks across journals, countries, institutions, and authors, using co-citation analysis, keyword co-occurrence examination, citation bursts, and clustering pattern identification.
This approach reveals hidden patterns, emerging trends, and collaboration networks that might not be apparent from conventional literature reviews. Through scientometric analysis, the study provides an objective insight into research hotspots and frontier trends in digital health implementation within the Australian context. This contribution is vital for advancing our understanding of the unique challenges and opportunities in digital health within Australia and for shaping future research and policy efforts.
Methods
Data source
A bibliometric and scientometric analysis was conducted using data retrieved from the Web of Sciences Core Collection (WoSCC), an extended version of the Science Citation Index. The WoSCC citation database encompasses the Science Citation Index, Social Science Citation Index, and Arts and Humanities Citation Index as its core components. This database includes over 9000 globally recognized and influential academic journals, and the documents within it are highly authoritative within the academic community.
Search strategy
To capture research articles addressing digital health implementation in Australia, a set of criteria was established encompassing the three key concepts of (#1) digital health, (#2) implementation, and (#3) Australia. Table 1 provides a summary of these key concepts and corresponding search terms, while Supplementary File 1 presents specific search strings employed. The query command (#1 AND #2) was used to retrieve articles focused on the implementation of digital health, and the inclusion of (#3) ensured that the articles related specifically to the Australian context.
Key concepts and search terms.

Recognizing that digital health encompasses a broad range of technologies used to deliver healthcare services or to collect and share an individual's health information, 38 and in the absence of a universally accepted definition, we adopt the Queensland Health definition, which describes digital health as ‘the use of technology and innovation to deliver and enable healthcare services’. Additionally, we refer to Fatehi et al.'s definition to articulate the technological components of digital health. 39
Document titles and abstracts were screened based on the inclusion and exclusion criteria outlined in Table 2. These were selected to ensure a focused and relevant analysis of digital health implementation research in Australia. The inclusion criteria targeted original research articles available in English, published from inception to 31 December 2023, and conducted in Australia, specifically those that describe or evaluate the implementation of digital health innovations. This approach ensured the study was based on empirical evidence from the Australian context, capturing real-world applications and outcomes relevant to the nation's healthcare system. In contrast, the exclusion criteria eliminated reviews, protocols, case studies, or descriptions of broad digital health technologies, as well as conceptual, descriptive, or guideline articles that do not provide new empirical data or specific insights into digital health implementation. Articles were excluded if they were conducted outside Australia, not published in English, or lacked an explicit description or evaluation of digital health implementation. For example, exploratory articles that detailed stakeholders’ perceptions of broad digital health topics or assessed readiness for digital health were excluded. Together, these criteria ensured the study remained focused on identifying research hotspots and frontier trends in digital health implementation in Australia, based on high-quality, original research findings.
Inclusion and exclusion criteria.

Implementation refers to the use of strategies to adopt and integrate evidence-based interventions and change practice within specific settings (i.e., putting the innovation into practice (application), policy and/or action).
Digital health innovation refers broadly to the use of a technology intended to prevent, diagnose, or treat medical conditions, promote health, or provide rehabilitation, organize the delivery of healthcare access, transparency, or personalization. In the realm of prevention science/health, digital health innovations are designed to improve the healthcare system for providers and consumers alike and may include telehealth, electronic health records, electronic prescriptions, healthcare identifiers, electronic referrals, electronic medication charts, and access to trusted data.
To minimize potential bias due to ongoing database modifications, the retrieval and export of documents were completed on a single day, 4 January 2024. After full-text screening, the final dataset comprised 196 documents (see Figure 1).

PRISMA flow chart of the literature search strategy.
Data analysis and visualization
Records identified in WoSCC were exported into Microsoft Excel (Redmond, WA, United States) for the analysis and illustration of publication and citation metrics. Full records and cited references were exported in plain text format for scientometric analysis and data visualization.
VOSviewer (version 1.6.17) 40 was employed to construct and visualize network graphs of journals, countries, institutions, authors, and keywords. Full counting was applied, with nodes representing the journals, institutions, or authors. The size of each node represents the number of published documents, and the connections between nodes reflect the strength of their relationships. Clustering analysis was performed to identify sub-clusters of collaboration within the overall literature structure. 41 CiteSpace (version 6.2.R6) 42 was utilized to identify frontier trends in the research. Document co-citation and co-occurring keywords analyses, along with cluster analysis, were used to highlight the research specialities within clusters. The parameters for this investigation were set with a time-slicing range from 1999 to 2023 (2 years per slice), look back years = −1, link retaining factor = −1, top N% = 10.0%, top N = 50, and g-index = 25. Default settings for text processing and links were retained.
Results
Trend analysis of scientific production
The trend analysis of scientific output provides valuable insights into the evolution of digital health implementation research in Australia. As illustrated in Figure 2, a total of 196 documents were published between 1999 and 2023. The initial output was minimal, with only six publications prior to 2010. However, there was a notable increase in the number of publications from 2010 to 2017, followed by a slight decline in 2018. Since 2018, there has been a consistent upward trend in publication rates, with an average annual growth rate of 43%, leading to a doubling of output approximately every 2–2.5 years. This sustained growth is indicative of a heightened research focus and investment in digital health, likely influenced by technological advancements, the impact of the COVID-19 pandemic, and strategic policy shifts towards digital healthcare reform in Australia.

Annual trends in publications and citations from inception to 31 December 2023.
Analysis of journals
The 196 documents are distributed across 96 journals, reflecting the multidisciplinary nature of digital health research. Figure 3 visualizes journals with three or more publications, and Table 3 summarizes the top five journals, which collectively account for 32.3% of the publications. This concentration of research in select journals highlights key platforms that are central to the discourse on digital health. The prominence of journals such as the Journal of Telemedicine and Telecare and the Journal of Medical Internet Research suggests a focused interest in telehealth and internet-based health solutions.

Visualization of the journal network. The colour of the node represents the change in the number of published documents over time.
The top five journals publishing research on digital health implementation in Australia.

Excluding self-citation.
Analysis of countries and institutional networks
The publications stem from 19 countries/regions and 299 institutions. Table 4 presents the top five countries and institutions with the highest productivity. This concentration suggests a strong research capacity and the potential for extensive collaborative efforts. Figure 4 reveals that research institutions are clustered regionally, indicating that collaborations are often geographically concentrated. This clustering underscores the role of localized research hubs and highlights opportunities for expanding collaborative networks to include institutions from other regions.

Network visualization of institutions. Colours represent institutional collaboration networks.
The top five countries and institutions publishing digital health implementation research in Australia.

The top 10 authors producing articles on digital health implementation in Australia.

Analysis of author networks
The analysis of author works, presented in Figure 5, identifies 1150 authors, with 126 core authors significantly contributing to the research output. This indicates that while digital health implementation research is expanding, it remains concentrated among a relatively small group of researchers. The presence of a core group of authors (Table 5) suggests an emerging but still developing field, where additional researchers may find opportunities to contribute and broaden the scope of investigation.
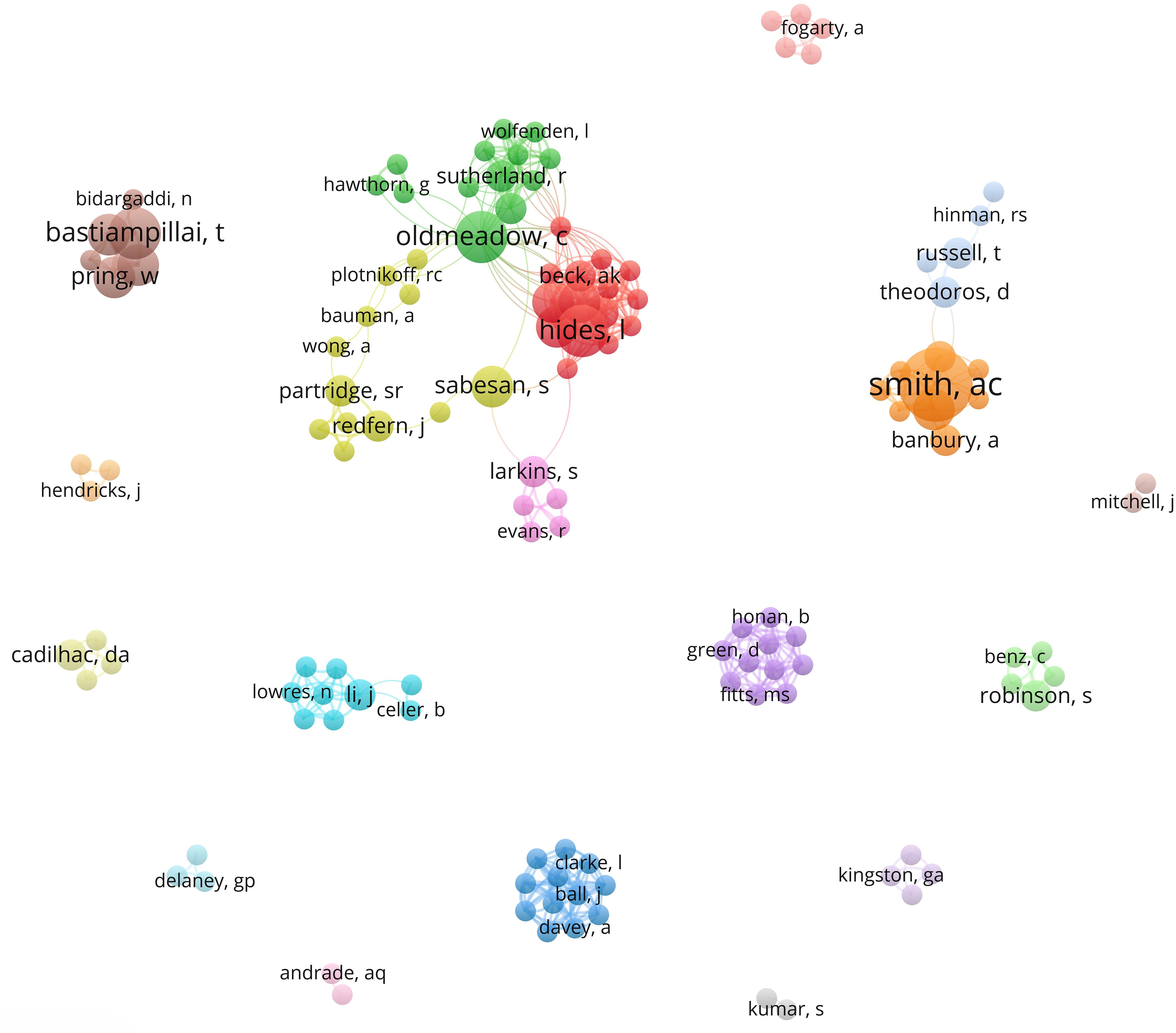
Network visualization of author cooperation. Colours represent author collaboration networks.
Analysis of documents
A crucial aspect of constructing the knowledge structure involves identifying highly cited articles and key research areas. Figure 6 presents the top 10 cited documents, highlighting those with the strongest citation bursts. Notably, the article titled ‘Cost savings from a telemedicine model of care in Northern Queensland, Australia’ 43 has the longest citation burst spanning from 2015 to 2018. Published in 2013, this study presents an economic analysis of a telemedicine model for cancer care (teleoncology) in Northern Queensland, Australia.

Through document co-citation analysis, nine research clusters were identified and visually represented over time in Figure 7. The overall structural properties of the cluster network reveal dense intra-cluster connections and limited intra-cluster links. This fragmentation indicates a need for interdisciplinary approaches to connect disparate research areas and develop cohesive digital health strategies. Clusters are ranked by the number of documents, with ‘rural population’ (#0) being the largest cluster and ‘telerehabilitation’ (#11) being the smallest. The focus on specific clusters, such as ‘rural population’ and ‘telerehabilitation’, highlights critical research areas but also points to gaps in integrating these findings into broader frameworks.
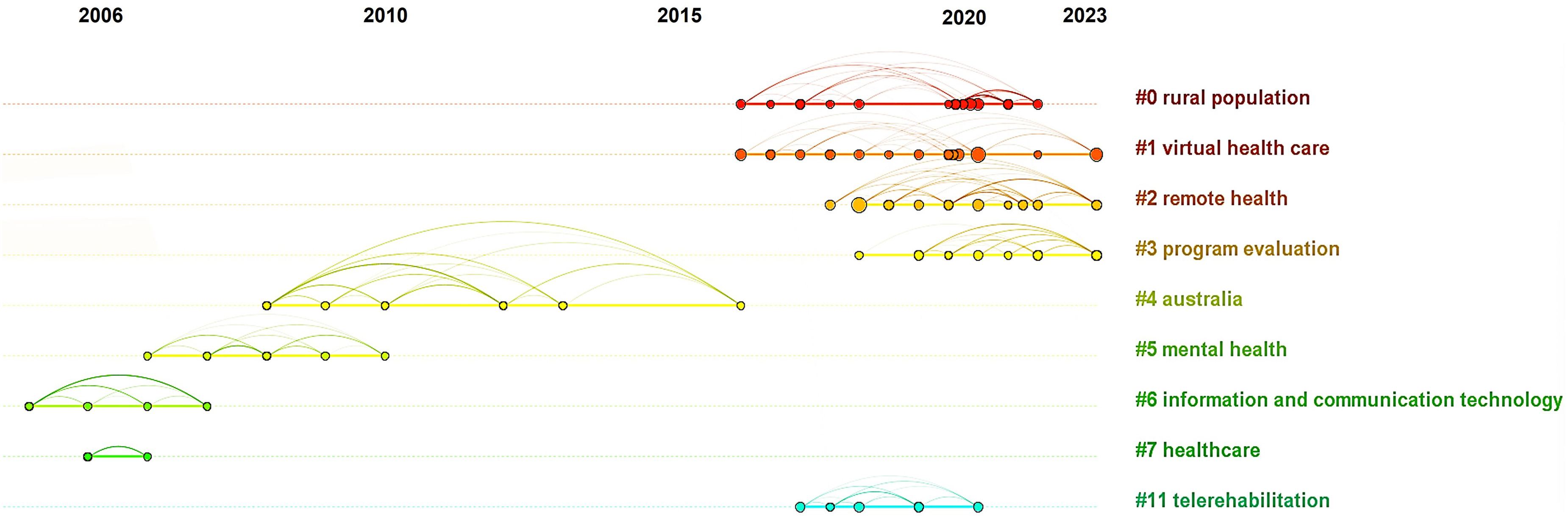
Timeline visualization of document co-citation clustering (modularity Q score = 0.9021 and silhouette score = 0.9511).
Analysis of keywords
Keywords capture the central concepts of a document, and co-occurring keywords highlight research hotspots. In this study, 57 high-frequency keywords (with more than five co-occurrences), excluding the terms ‘digital health’, ‘implementation’ and ‘Australia’, were identified. The size of each node corresponds to the frequency of the keyword, and the lines between nodes represent keyword co-occurrence.
Analysis of the keyword co-occurrence map (Figure 8(a)), reveals that the high-frequency keywords are ‘telehealth’ (97), ‘telemedicine’ (68), ‘covid-19’ (28), and ‘care’ (26). The high frequency of these keywords reflects their prominence in current research. The clustering density function, illustrated in Figure 8(b), shows a gradient from cold to warm tones, indicating an increase in clustering density and research focus over time. These trends indicate a shift towards incorporating digital health solutions into primary care and responding to public health challenges, such as the COVID-19 pandemic.

Keyword co-occurrence (a) network map; (b) clustering density map; (c) cluster analysis.
Cluster analysis resulted in 10 research clusters (Figure 8(c) and Supplementary File 2). The largest cluster (#0) is ‘healthcare’ with 32 keywords related to the quality of innovations across various health settings and domains (e.g., reliability, validity, feasibility, quality, and efficacy). Cluster two (#1), ‘models of care’, includes 31 keywords associated with telemedicine, prevalence, health outcomes, meta-analysis, apps, and evaluation across different healthcare domains such as eye health, cancer care, and clinical supervision. This suggests a comprehensive assessment of telemedicine applications from prevalence and outcomes to meta-analysis and app-based models of care. The third cluster (#2), ‘implementation science’, comprises 28 keywords focusing on disease management, medication adherence, promotion of physical activity, public health strategies, and validation and impact of digital health support systems. The fourth largest cluster (#3), with 21 items, is ‘early intervention’, addressing digital tools for mental health, managing depression, anxiety disorders, and cognitive behavioural therapy.
The remaining six clusters cover themes of healthcare accessibility and management in rural or remote areas (#4 ‘telehealth’), leveraging technology and patient engagement strategies to enhance healthcare education, access, and management (#5 ‘personal health information’), the intersection of mental health care, technology, and decision-making support (#6 ‘prevention’), adherence strategies, program management, and evidence-based approaches to improving health outcomes (#7 ‘management’), primary care and community-based health care, (#8 ‘primary care’), and healthcare delivery in remote or underserved areas with a particular emphasis on emergency medical services (#9 ‘remote health’).
Figure 9 displays the top 10 keywords with the most significant citation bursts. The line represents the time intervals, with the red lines indicating periods during which the keyword bursts occurred. The most recent keywords with citation bursts, occurring in 2021, include primary care, mobile phone, COVID-19 pandemic, consultations, barriers, health services, internet, and experiences, with bursts extending through to 2023.

The top 10 keyword terms with the most citation bursts, where the blue line represents the time interval, and the red line represents the time during which the keyword bursts were discovered.
Discussion
This analysis of digital health implementation research in Australia reveals prominent thematic clusters, and highlights influential publications, prolific authors, and collaborative networks. Additionally, we identify significant research hotspots and frontier areas for future investigation, including implementation science, early intervention, personal health information, and remote health. These insights offer valuable guidance for researchers, policymakers, and healthcare practitioners, facilitating their engagement with, and contributions to the advancement of the field. Ultimately, these findings support efforts to enhance the quality, efficiency, and accessibility of healthcare services.
Knowledge base
The study highlights three key attributes of digital health implementation research in Australia. First, the significant increase in the volume and investment in digital health implementation research has been observed since 2018. This trend is marked by a substantial rise in annual publications, which have been doubling approximately every 2–2.5 years, with a sustained increase since 2019. While this upward trajectory was already in progress, the COVID-19 pandemic accelerated this shift by necessitating the rapid adoption of digital health solutions in place of traditional face-to-face care. This acceleration was further supported by notable advancements in supportive policy measures. Second, a considerable proportion of research and influence is concentrated in five institutions that lead in publication output, accounting for 56.8% of the total contributions. This concentration reflects the institutions’ organizational prominence and suggests extensive collaborative relationships that drive digital health initiatives. These leading institutions are notably represented in three of the five research clusters identified (see Figure 4), while the remaining two clusters are geographically concentrated in Western Australia and South Australia.
Third, an analysis of the author cooperation network reveals a robust collaborative network involving 1150 authors. This network highlights the collective efforts within the field, indicating potential for ongoing expansion and collaboration among core authors.
In constructing the knowledge base of the research, identifying highly impactful articles and pivotal research areas is essential. Among the ten documents with the highest citation bursts (see Figure 6), nine have citation increases since 2021, reflecting their recent prominence in the scientific community. Notably, most of these articles focus on telehealth, particularly its implementation and impact during the COVID-19 pandemic. These results provide valuable insights from the various perspectives, including global implications, user experiences in Australia, mental health services, and telehealth usage. Together, these articles contribute to a comprehensive understanding of telehealth, potentially guiding future initiatives and policy decisions aimed at enhancing the overall effectiveness and integration of telehealth services.
Further, document co-citation and cluster analysis have delineated nine distinct research clusters (Figure 7), including ‘virtual healthcare’, ‘remote health’, and ‘program evaluation’ as recent trends in the research. Research within ‘virtual healthcare’, is notably contextualized by the COVID-19 pandemic, offering critical insights that inform our understanding, development, and strategic implementation of telehealth services in diverse healthcare settings. Studies in ‘remote health’, focus on improving accessibility, quality, and outcomes in remote and underserved areas, highlighting the potential benefits of digital health initiatives in optimizing access. Articles in ‘program evaluation’ address the feasibility, acceptability, and sustainability of telehealth programs, particularly during the COVID-19 pandemic and within allied health services. This research provides valuable information for evaluating the scalability and effectiveness of telehealth programs, incorporating qualitative insights into consumer experiences to enhance the evaluation process.
Research hotspots
The analysis of research keywords reveals significant shifts in focus over time. First, recent years have witnessed a prominent shift in research focus, with clusters such as ‘implementation science’, ‘early intervention’, ‘personal health information’, and ‘remote health’ being increasingly prominent. Notable, in 2023, keywords such as ‘emergency medicine’, ‘remote health’, and ‘communication’, emerged with the highest frequency and centrality all within cluster #9. Figure 10 illustrates the evolution of research keywords, revealing four distinct time periods.
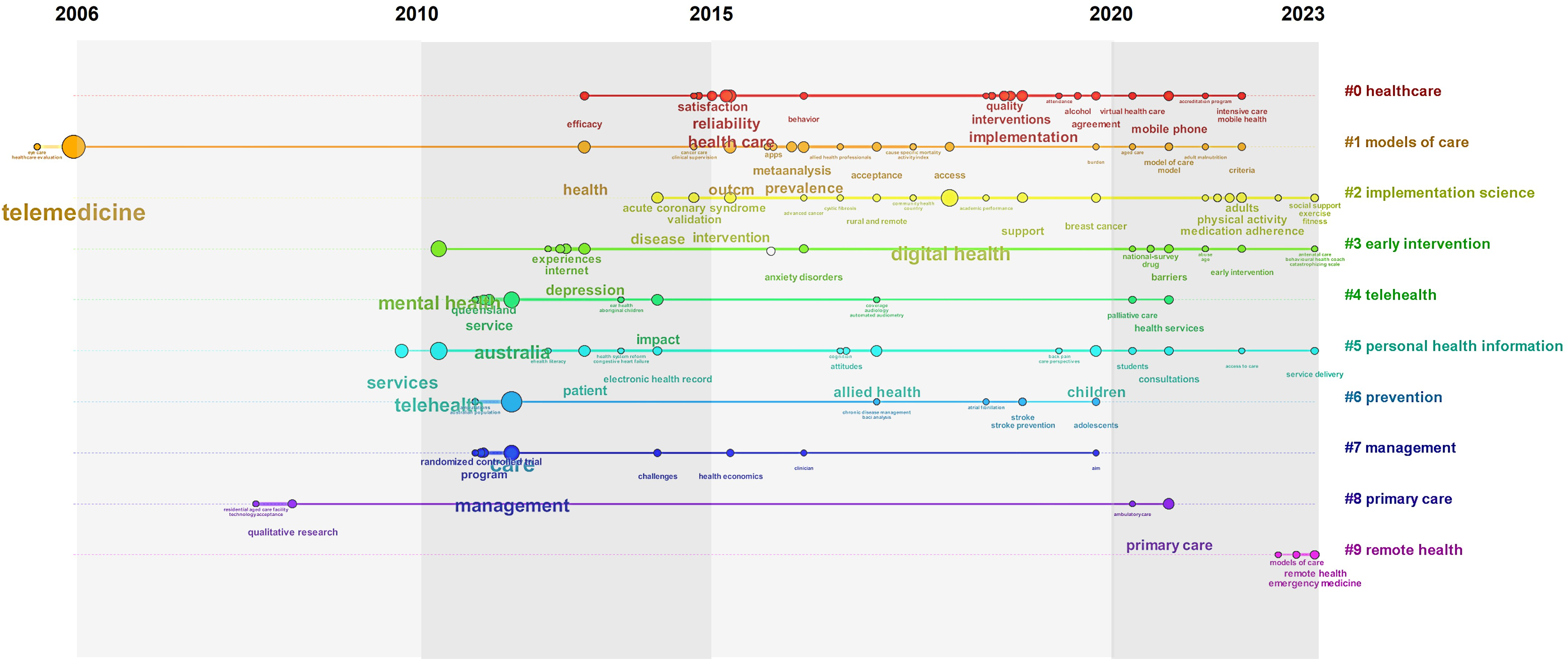
Timeline view of keyword clustering analysis. Each node indicates when the keyword appears for the first time in large numbers.
During the first period (2006–2010), the prominent keywords included ‘telemedicine’, ‘qualitative research’, ‘technology acceptance’, and ‘healthcare evaluation’. These keywords primarily appear in cluster #1 (models of care) and #8 (primary care), which define the initial stages of digital health implementation research. The focus during this period was on qualitative aspects, including user acceptance and the unique digital health needs within various healthcare settings. These early studies provided foundational insights into the diverse applications and challenges of digital health, addressing both emergency and chronic care settings, and including dynamics within residential aged care and hospital wards.
In the second period (2011–2015), the research concentrated on innovative responses to mental health emergencies, particularly in rural and remote regions. The implementation of telehealth services in New South Wales exemplified the commitment to providing accessible mental health support. 53 This period also highlighted barriers to telemedicine uptake and the challenges faced in broader integration within the Australian healthcare system.54,55 Specific clinical applications, such as enhancing tuberculosis treatment through home videophones 56 and reducing patient transfers in mental health through videoconferencing, 57 underscored the potential of technology to improve treatment efficacy and accessibility, especially in remote areas. The standardization of clinical practice management and electronic documentation systems further demonstrated systematic approaches to improved care. 58 Evaluation and impact studies of telehealth initiatives became prominent, including research on the acceptability of online mental health resources in rural Australia, clinician perceptions, and the effectiveness of digital platforms. 59 Collaborative efforts and quality improvements were evident in initiatives such as the National eHealth Record System 60 and the Victorian Stroke Telemedicine Project, highlighting the transformative potential of telehealth in stroke management. 54
The third period (2016–2020) focused on the uptake, prevalence and impact of digital health, telehealth, and eHealth initiatives across diverse healthcare domains. Research during this time explored the efficacy of mHealth, from lifestyle programs for weight management 12 to the development and validation of mobile applications.61,62 Chronic disease management emerged as a significant theme, with studies investigating telehealth applications in screening, monitoring, and treating conditions such as diabetic retinopathy, 63 cancer, 64 and viral hepatitis.65,66 Themes of health literacy and equity were addressed through the co-design of eHealth innovations for rural populations, telehealth in remote and rural areas, 67 and feasibility and acceptability studies in various contexts, including support for burns victims 68 and intensive care units. 69 The integration of telemedicine into specialized care services, such as stroke consultations and mental health support, 70 highlighted the evolving landscape of digital healthcare. Beyond clinical applications, the research delved into the intersection of technology and behavioural health, addressing issues like anxiety disorders and smoking cessation through digital health. 71 The quality of care remained a recurring focus, with studies evaluating the impact of telehealth on hospital readmission rates 72 and cost-effectiveness. 73 The integration of digital tools for disease management, patient-reported outcome measures, along with the adoption of telehealth during the COVID-19 pandemic, contributed to a comprehensive understanding of the evolving digital health landscape.
In the fourth period (2021–2023), research covered a broad spectrum of digital health applications and its impact on healthcare delivery in Australia. Studies explored the development, implementation, and evaluation of telehealth programs for specific health conditions, such as the SWAP IT trial 74 and the TeleClinical Care model, 75 which investigated mHealth-based innovations for dietary habits and remote clinical care. Specialized telehealth initiatives, including TeleDermatology adaptations 76 and Teleaudiology service, 77 demonstrated the adaptability of telehealth in addressing dermatological and audiological concerns. The research also examined the implementation and optimization of telehealth services during critical situations, with studies such as COVID-care telehealth during the pandemic, and virtual health care for community management of patients with COVID-19. These projects assessed the feasibility, acceptability, and outcomes of rapid telehealth deployment. Additionally, the impact of telehealth on specific populations, including those with chronic conditions, mental health, and cancer survivors, was explored, providing valuable insights into consumer experiences, clinical outcomes, and acceptability across diverse healthcare domains. The emphasis on evaluating the cost-effectiveness of telehealth programs contributed to the broader discussion on the economic viability and sustainability of digital health services. Collectively, these research themes highlight the versatility, impact, and challenges associated with integrating digital health into various healthcare settings in Australia.
Frontier trends
Insights into emerging research areas within digital health implementation can be deduced from a comprehensive analysis of existing studies. Figure 10 presents a timeline map of research clusters, revealing the evolution of research themes in this field. The earliest focus is on ‘models of care’, while more recent trends include ‘implementation science’, ‘early intervention’, ‘personal health information’, and ‘remote health’. Notably, ‘remote health’ has emerged as a prominent and frontier trend, appearing only in the recent years as a significant research hotspot.
The focus on remote health suggests an increasing emphasis on extending healthcare delivery and monitoring beyond traditional settings. The growing interest in telehealth, remote patient monitoring, and virtual care models as strategies to improve access to healthcare for rural and remote residents is expected to drive future research in this area. In Australia, with its vast and geographical expanse and dispersed population, optimizing remote health delivery through digital tools – such as telemedicine, remote monitoring, and mHealth applications – is particularly crucial.
Considering the low population densities and workforce shortages prevalent across rural and remote Australia, improving connectivity, system interoperability, and digital readiness and literacy among both healthcare consumers and providers is vital. These factors are essential to optimizing the effectiveness and sustainability of digitally enabled models of care, which aim to enhance healthcare delivery and equitable outcomes to rural and remote areas. Leveraging the remote capabilities of digital health is fundamental to bridging these gaps and ensuring equitable healthcare access for all Australians. This is particularly pertinent for managing chronic conditions, such as chronic kidney disease, where regular monitoring and timely intervention are critical. Additionally, remote health facilitates access to medical or allied health expertise, diagnostics, and ongoing or rehabilitative care in regions with limited traditional healthcare infrastructure. 78
Other examples of this approach include telemedicine-supported breast screening and assessment services for women in regional Australia, 79 mHealth application for remote dental screening to aid caries diagnosis, 80 and remote surveillance monitoring for vascular patients. 81 The expansion of research in this area, is poised to enhance access to medical expertise, reduce geographical barriers, and reach individuals in remote or underserved regions.
Effective implementation strategies and targeted upskilling will be essential for the adoption of patient self-monitoring technologies and telehealth components. These elements will be key outcomes of remote health research, enabling continuous monitoring of health metrics and facilitating proactive management of chronic diseases. Optimizing remote care models will require the development of user-friendly digital healthcare delivery platforms, advanced video conferencing technologies, personalized virtual care plans, and education programmes to improve digital literacy among both consumers and providers. In alignment with current national health priorities and policies in Australia, government initiatives, funding opportunities, and healthcare reform efforts will shape the future direction of digital health research, within an increasing emphasis on remote health.
Strengths and limitations
This study demonstrates rigorous methodological standards, using advanced software to visually represent citation patterns and bibliometric trends. One of the study's major strengths is its focus on the country level, which provides valuable insights into the current landscape of digital health implementation research in Australia. However, it is important to recognize that specific outcomes may differ based on the focus and objectives of individual research studies. Additionally, as this is the first study of its kind in the field, no direct comparisons can be made to previous research. The study's reliance on scientometric analysis presents several limitations that must be acknowledged. Firstly, the analysis is constrained by its focus on published literature indexed in bibliometric databases, thereby excluding grey literature such as policy reports, digital strategies, and unpublished research, which could provide a more broad view of the field. Additionally, the quality and completeness of citation and publication data can impact the accuracy and reliability of the findings. While analysis offers valuable quantitative insights, qualitative aspects of the research such as theoretical contributions and contextual factors are outside of the scope of work. Lastly, the reliance on citation metrics as a measure of research impact can be problematic, as citations can be influenced by various factors that do not necessarily align with the quality or significance of the research.
Implications
Policymakers
The study highlights a notable increase in digital health implementation research in Australia. Policymakers should leverage this momentum by prioritizing investments in digital health infrastructure and enacting supportive policies that expedite the adoption of digital health solutions. Given the concentration of research within specific institutions and regions, there is potential to strengthen collaborative networks and partnerships. Such efforts could enhance the effective implementation of digital health innovations and address healthcare access disparities, particularly in remote and underserved areas.
Policymakers should also focus on developing frameworks that facilitate the integration of digital health tools into existing healthcare systems. This includes addressing infrastructure challenges and improving digital literacy. For example, the Australian Health Practitioner Regulation Agency has developed guidelines for telehealth consultations, 82 ensuring that health practitioners are well-trained and qualified to deliver safe and effective remote care. Such guidelines exemplify the kind of support needed to optimize the integration of digital health technologies.
Healthcare practitioners
Practitioners could proactively adopt telehealth and remote monitoring technologies, particularly to enhance care for patients in rural and remote areas. Ongoing professional development is crucial for staying updated on advancements in digital health, and sharing best practices can aid in the effective implementation of these solutions. Active involvement in the evaluation and optimization of initiatives ensures that digital tools are effectively integrated into patient care and contribute to improved health outcomes.
Researchers
The study highlights several key implications for researchers. Identifying specific research clusters and gaps, particularly regarding digital health implementation in rural settings, emphasizes the need for comprehensive studies in these areas. Researchers should address these gaps to deepen the understanding of digital health challenges and opportunities. The fragmented nature of current research suggests a need for interdisciplinary approaches. Researchers should strive to integrate findings across various domains of digital health, including telemedicine, remote care, and implementation science, to develop more holistic solutions. Moreover, the identification of core research teams and institutional networks underscores the potential for expanded collaborations. Researchers should engage in collaborative projects and contribute to larger networks to leverage collective expertise and resources. The focus on remote health further indicates the necessity for research that translates findings into practical applications, providing actionable insights and recommendations for improving digital health implementation and addressing real-world challenges.
Conclusion
This study provides a comprehensive overview of digital health implementation research in Australia from 1999 to 2023, highlighting key findings and providing a roadmap for future research. It reveals a growing focus on digital health solutions, particularly for addressing the needs of remote health. However, challenges such as connectivity issues, interoperability, and digital literacy must be overcome to fully realize the potential of these technologies, especially in rural areas. The Productivity Commission's report underscores that better integration of digital technology could save over $5 billion annually and ease pressures on the healthcare system. 83 Future research should address digital health gaps in rural and remote health, adopt interdisciplinary approaches to integrate findings across various digital health domains, foster increased collaboration among research teams, and focus on translating research into practical applications to provide actionable insights for improving digital health implementation. This study serves as a foundational guide for advancing research, investment, and policy-making for digital health in Australia.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241297729 - Supplemental material for Digital health implementation in Australia: A scientometric review of the research
Supplemental material, sj-docx-1-dhj-10.1177_20552076241297729 for Digital health implementation in Australia: A scientometric review of the research by Michelle A. Krahe, Sarah L. Larkins and Nico Adams in DIGITAL HEALTH
Footnotes
Acknowledgements
Not applicable.
Contributorship
MK conceptualized the study, curated the data, conducted the formal analysis and visualization of data. MK prepared the original draft and SL and NA reviewed and edited the manuscript. All authors approved the final version of the manuscript.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
There are no human participants in this article and informed consent is not required.
Funding
This work was completed under the Northern Australian Regional Digital Health Collaborative (NARDHC), who are supported by the Australian Government Department of Education.
Guarantor
MK is the guarantor for this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.