
Abstract
Background
Sleep complaints are a major concern for the aging population. Insomnia affects quality of life, and is associated with unfavorable geriatric outcomes. Digital technologies offer promising perspectives to assess and support various health conditions, including for the older adults. Among them, the KANOPEE app, a smartphone-based virtual autonomous conversational agent, has been validated in general adult population for insomnia assessment and behavioral interventions. This research primarily aimed to assess the acceptability of the KANOPEE application for evaluating insomnia in older adults. The secondary objective aimed to identify the determinants influencing the acceptability of the app.
Methods
This cross-sectional study included geriatric department inpatients aged 70 or older, undergoing a standardized interview with the app, addressing sleep complaints. Acceptability was assessed using the Acceptability E-Scale (AES) and ECA Trust Questionnaire (ETQ). Sociodemographic and geriatric data were collected for multivariate linear regression analysis to assess determinants of acceptability scores.
Results
Fifty inpatients were included (mean age: 85.8 years, men: 48%), 40% declaring a novice level of familiarity with technology. Insomnia Severity Index mean score was of 8.2, with significant clinical insomnia for 12%. The KANOPEE app showed good acceptability on AES and ETQ scales (respectively 22/30 and 18/24). Familiarity with technology increased credibility in the app (β = 1.5, CI [0.1, 2.9]). Acceptability increased with multimorbidity score (β = 1.5, CI [0.1, 2.2]), and decreased with hearing impairment (β = 1.5, CI [−10.6, −2.8]). Higher depression score decreased trust in the app (β = −0.7, CI [−0.9, −0.4).
Conclusion
This preliminary investigation confirms that older adults can use autonomous virtual agent based applications to quantify their sleep complaints. Understanding and tailoring the unique needs of older users are paramount for successful digital interventions. Further research is needed to confirm these preliminary findings and assess the broader impact of digital apps in a larger sample.
Background
Sleep complaints are particularly prevalent among older adults. Leading the charge, insomnia complaints are a significant concern, exhibiting a higher prevalence compared to the general population, with estimates indicating that between 12% and 20% of older adults experience insomnia.1,2 Insomnia complaints may result from physiological changes of circadian rhythm with the ageing process, bad sleeping habits, or clinically validated insomnia. Frequent misdiagnosis or underdiagnosis of sleep disorders poses a substantial challenge, making effective sleep assessment a major public health concern in the context of ageing populations. Such mismanagement can lead to inappropriate and potentially harmful prescriptions of hypnotic drugs. Clinical insomnia adversely affects individuals’ quality of life on a daily basis, and is associated with an increased risk of somatic diseases and psychological disorders, such as anxiety or depression.3,4 For older adults, insomnia also leads to a greater risk of cognitive impairment, falls, and polypharmacy, and thus contributes to frailty. 5 Insomnia complaints diagnosis and treatment is therefore essential in older adult care.
The digital transformation of modern societies offers numerous opportunities, including for the ageing population. Older adults have become regular users of digital technologies, for applications such as communication, functional and health outcomes, or healthcare access. 6 However, a particular attention must be paid when developing such technologies, to ensure their usability, accessibility, and inclusivity, thereby ensuring that older adults can genuinely benefit from them. 7 Meeting these challenges, digital technologies offer a new perspective for geriatric care. In the mental health area, a recent systematic review has shown that cognitive-behavioral therapy for insomnia, based on internet interventions, significantly improved quality and quantity of sleep duration for older adults. 8 Although based on studies of heterogeneous quality, this review highlights the role of Information and Communication Technologies in managing sleep complaints. Recently, numerous digital interventions have been developed, either relying on internet questionnaires, or more sophisticated evaluations, with self-reported questionnaires based on a smartphone app, actimetric automeasures, or conversational agents. To our knowledge, none of these interventions has been genuinely evaluated among other adults, for insomnia complaints screening, nor for sleep improvement. 9
The KANOPEE app, developed by the SANPSY team in Bordeaux, is a smartphone-based application that features a virtual conversational agent called “Louise.” This app has been evaluated in terms of acceptability in general adult population for insomnia complaints or mood disorders screening. 10 In addition, it provides a daily follow-up through a sleep diary, and gives users personalized recommendations grounded in behavioral interventions, which include sleep hygiene practices, sleep scheduling, stimulus control, and physical activity). The effectiveness of the KANOPEE interventions has also been demonstrated on sleep complaints and duration among general adults population. 11
As KANOPEE is a digital widely accessible application, it may provide a valuable screening tool for sleep disorders among older adults. Furthermore, based on its behavioral interventions, it may fit better for older adults than classical psychotropic drugs, whose adverse effects may occur in this frequently polymedicated population. Yet, its acceptability and efficacy have not been formally evaluated in this population. Therefore, it is essential to conduct such evaluations to endorse its application for sleep assessments, to facilitate further modifications to tailor KANOPEE for older users, and to determine its effectiveness in identifying insomnia issues and enhancing sleep quality.
This preliminary study main objective was to evaluate the acceptability of a first virtual interview with the KANOPEE app for insomnia assessment in geriatric inpatients settings. The secondary objective consisted of identifying the sociodemographic and geriatric determinants of the application's acceptability.
Materials and methods
Study design and population
This study followed a cross-sectional design, and was conducted across four acute care and rehabilitation facilities within the gerontology department of Bordeaux University Hospital, from February to October 2022. The study population consisted of patients who met the following criteria: (1) inpatients aged 70 or older, (2) providing informed consent, (3) scoring above 20 on the Mini-Mental Score Examination (MMSE). Exclusion criteria included patients with (1) significant sensory impairments (such as hear loss or blindness), (2) severe dyspraxia or motor deficits, (3) moderate to severe major neurocognitive disorder as classified by the Diagnostic and Statistical Manual of Mental disorders, 5th revision, 12 which would hinder their ability to effectively utilize the KANOPEE application.
Study procedure
During the study period, patients who were screened and met the inclusion criteria received both oral and written information regarding the study. Included patients were invited in a digital tablet interview facilitated by “Louise,” the KANOPEE virtual agent, under the supervision of the investigator (Figure 1). Initially, patients were asked to provide their written consent through the application. Subsequently, they were requested to supply various sociodemographic data, including age, gender, educational background, and socioprofessional category. Then, “Louise” engaged the patients in a standardized interview aimed at addressing sleep complaints, based on the Insomnia Severity Index (categorized as <8: no insomnia, 8–14: subthreshold insomnia, 15–21: clinical moderate insomnia, and >21: clinical severe insomnia). 13 Additionally, feelings of fatigue and mood disorders were evaluated with the Fatigue Scale Severity and the Patient Health Questionnaire (PHQ-9), using standard scales thresholds.14,15 Patients interacted with the app by responding to a multiplechoice questionnaire directly on the touchscreen. The main investigator provided feedback of this interview when requested, in collaboration with the patient's physician.

Illustrative references of KANOPEE application.
Outcome variables
Upon completion of the virtual interview, included patients were asked about their user experience, in order to meet the objectives of this study. The acceptability of KANOPEE app was evaluated using two French-translated validated scales: the Acceptability E-Scale (AES) tool, which comprises two subscales (AES-Usability and AES-Satisfaction), and the ECA Trust Questionnaire (ETQ), also relying on two subscales (ETQ-Benevolence and ETQ-Usability).10,16 These Likert-scales rate from 1 (very unsatisfied) to 5 (very satisfied) for the AES, and from 1 (not at all) to 4 (totally agree) for the ETQ (see Supplemental Figure S1).
Supplementary data collection
The main investigator assessed whether patients required clarifications regarding the digital device, as well as their habits and familiarity with technology use (novice, intermediate, advanced). Additional geriatric data were also anonymously extracted from patients’ medical records to address our secondary explanatory objective. This included the MMSE for cognitive impairment, 17 a functional evaluation of activities of daily living (ADL), 18 the presence of mild to moderate sensory impairments (hearing and/or visual), the Charlson multimorbidity score, 19 and the count of medications taken daily.
Statistical analysis
Varying recommendations regarding pilot studies sample sizes can be found in literature, usually suggesting a minimum of 30 subjects. 20 To perform our explanatory secondary analysis, based on regression models, we aimed for a power of 80% with a 5% alpha risk, which necessitated an estimated sample size of between 50 and 70 patients. 21 For practical considerations, 50 participants were included.
Given that the primary analysis was descriptive, we summarized AES and ETQ scores using their means and standard derivation, and graphical representations. Other qualitative variables were reported in terms of counts and frequencies. To meet our secondary objective, β coefficients from multivariate linear regression analysis were estimated for the variables of interest, at 5% alpha risk. The assumptions of the regression model were rigorously tested. Adjustment hypothesis in modeling were based on geriatric experts advice and a thorough review of the literature.
The KANOPEE application complies with current legislative standards regarding data protection. The French national data protection authority (CNIL) approved the study protocol.
Results
Population inclusion and characteristics
Fifty patients hospitalized in the department of clinical gerontology were included in the study, 64% (n = 32) from the rehabilitation facilities, and 36% (n = 18) from acute geriatric care wards (Figure 2). The mean age was 85.8 years (standard derivation, i.e. SD = 5.9) (Table 1). Overall, 48% (n = 24) of the included patients were male, and 30% (n = 15) had a higher education than secondary school. Hospital referral was mostly motivated for falls (50, n = 25), infectious disease (16%, n = 8), or neurological strokes (10%, n = 5). For geriatric standardized data at baseline, mean ADL score was 4.6 (SD = 1.6), MMSE was 24.9 (SD = 2.6), and the mean Charlson multimorbidity score was 7.1 (SD = 2.3), mostly represented by heart and neurological conditions (respectively 84 and 48% of patients). This leaded to polypharmacy for more than a quarter of study population (n = 38), with 64% of inpatients being prescribed at least one psychotropic drug (n = 32). In terms of sensory impairment, 40% (n = 20) of included patients declared no hear or vision impairment, 4% (n = 2) had hearing impairment with hearing aids, 34% (n = 17) a vision impairment with vision aids, and 24% had both (n = 12).

Flow chart of included inpatients from gerontology department, University Hospital of Bordeaux, 2022.
Characteristics of study population (n = 50) in the gerontology department, University Hospital of Bordeaux, 2022.

Sd: standard derivation; ADL: activities of daily living; MMSE: mini-mental state examination; ISI: Insomnia Severity Index; PHQ-9: Patient Health Questionnaire-9 questions; FSS: Fatigue Severity Scale.
Before hospitalization, 40% of participants reported a novice level of familiarity with technology, with smartphone devices being the most frequently utilized (88%, n = 44). Three patients (6%) sought technical assistance before using the digital tablet. Once the interview started, the majority of the patients involved did not require any support or clarification from the investigator to operate the application.
KANOPEE assessments
From the KANOPEE application, the virtual agent assessed a clinical insomnia complaint for 12% of interviewed patients (n = 6), and a subthreshold insomnia for 44% (n = 22). A significant fatigue complaint was shown for 54% (n = 27), and a depressive disorder mild to moderate for 40% (n = 20).
Acceptability of KANOPEE application
Mean score for AES acceptability was 22/30 (SD = 4.8), with a distribution deported on highest scores (Figure 3 and Supplemental Table S1). Same distribution was observed for ETQ trust scale, with a mean score of 18/24 (SD = 2.5). Usability and overall satisfaction subscales were reported good, with more than half of patients being satisfied or very satisfied by the interview with the virtual agent (Figure 4). The majority considered KANOPEE virtual agent to be benevolent with them, and about two thirds agreed or totally agreed when asked about its credibility.

Distribution of global acceptability (AES scale) and trust score (ETQ scale) for KANOPEE application among inpatients from gerontology department, University Hospital of Bordeaux, 2022.
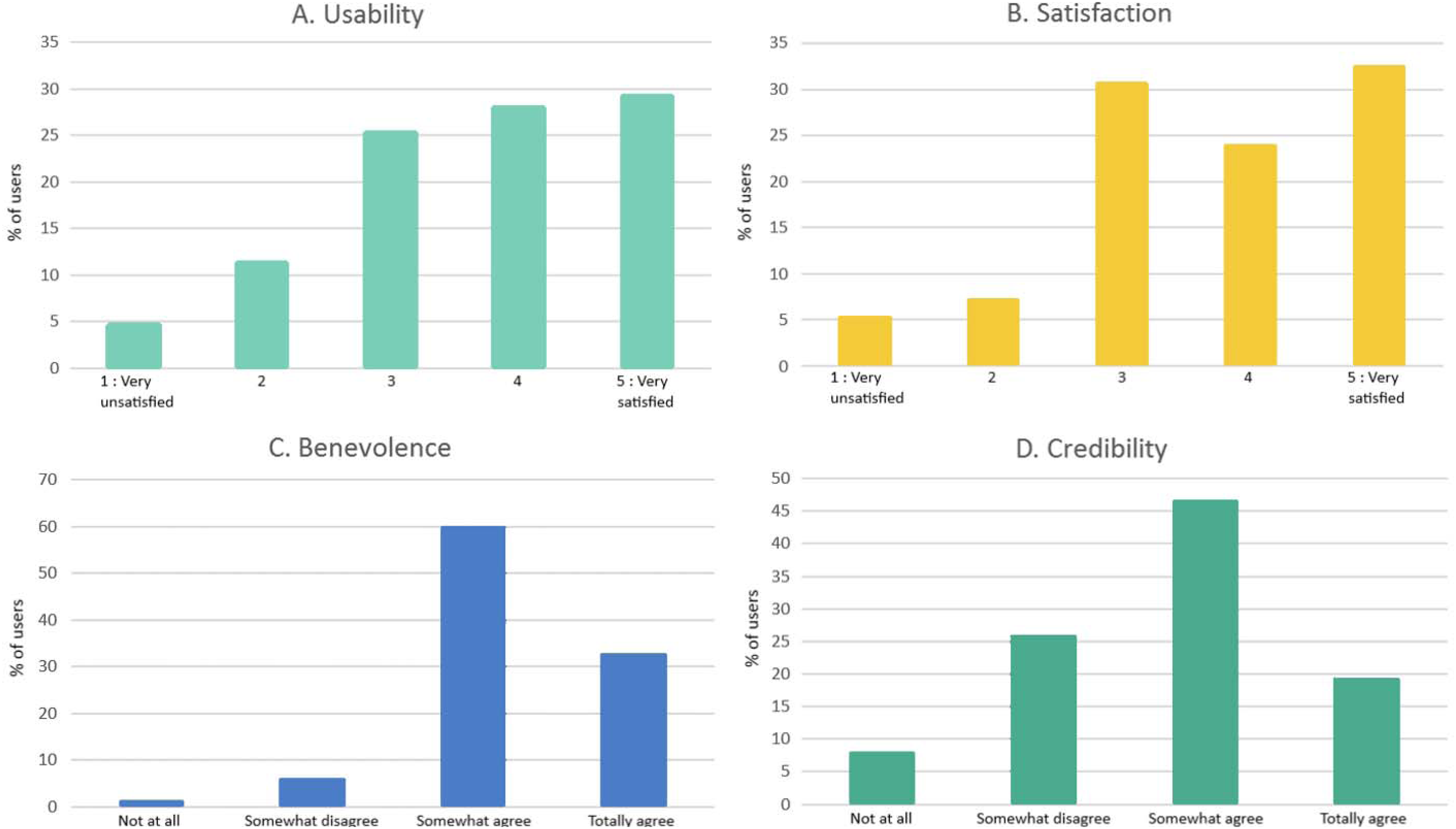
Perception of acceptability (subscales A + B: usability, satisfaction) and trust (subscales C + D: benevolence, credibility) for KANOPEE application among inpatients from gerontology department, University Hospital of Bordeaux, 2022.
Determinants of acceptability of KANOPEE application
In evaluating the acceptability of KANOPEE within the study population, no significant association was found on uni- or multivariate analysis between AES score and sociodemographic determinants (Table 2). Older age was not significantly associated with lower acceptability (β = −0.5, CI [−1.9, 0.9], p = .46). No other significant association was found for AES subscales (see Supplemental Tables S2 to S6). Among geriatric factors, the Charlson score was significantly correlated with higher acceptability of KANOPEE, after adjustment. Specifically, for each two-points increase in the Charlon score, the estimated β was 1.5 (CI [0.1, 2.2], p = .04). Inpatients with hearing impairment had a significantly lowered AES score, decreased by an average of 10 points after adjustment, compared to inpatients without sensory impairment (β = 10.6, CI [−18.4, −2.8], p = .04). These results were consistent in AES subscales analysis.
Determinants of AES and ETQ scores among characteristics of study population (n = 50). Multiple linear regression. Gerontology department, Bordeaux University hospital, 2022.
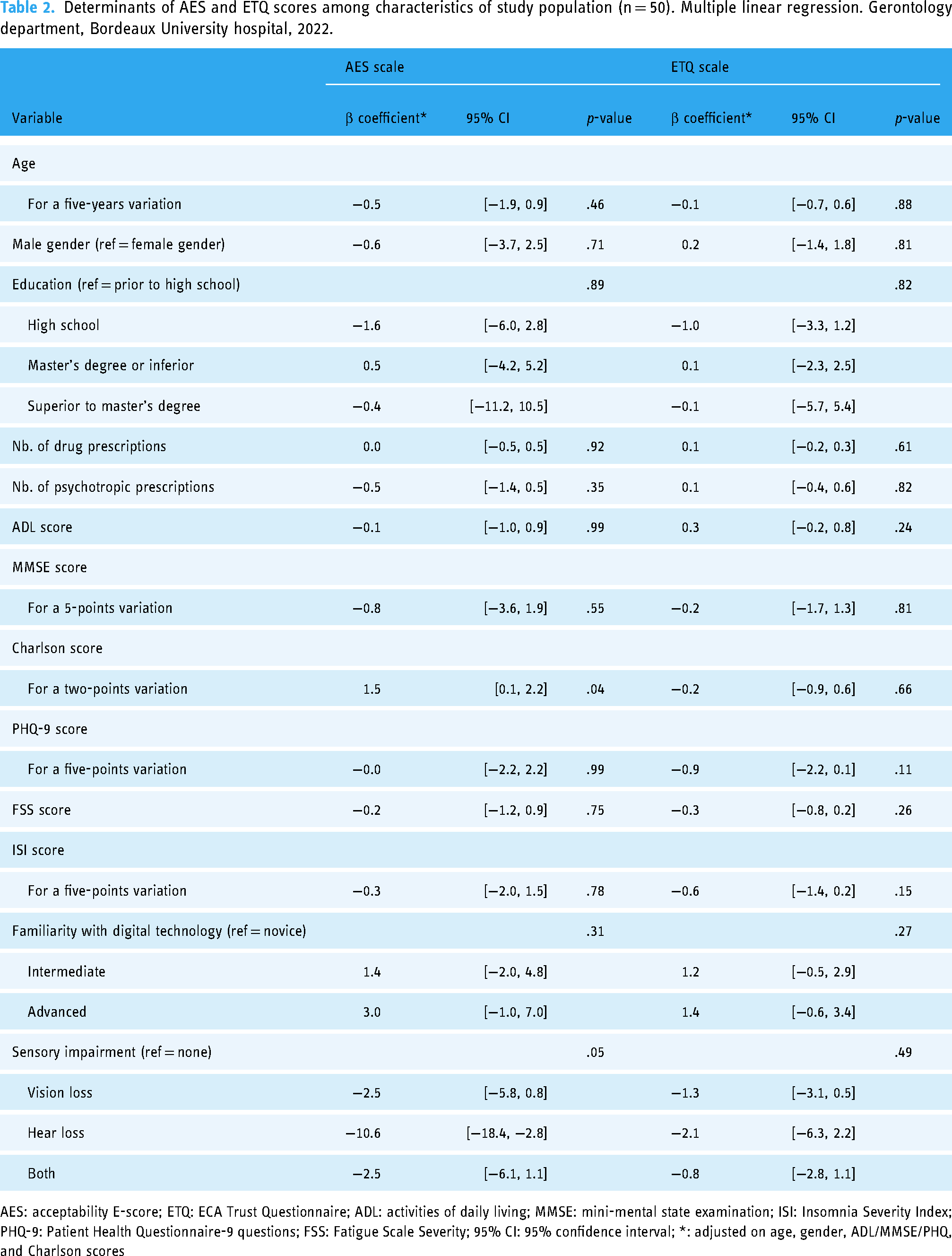
AES: acceptability E-score; ETQ: ECA Trust Questionnaire; ADL: activities of daily living; MMSE: mini-mental state examination; ISI: Insomnia Severity Index; PHQ-9: Patient Health Questionnaire-9 questions; FSS: Fatigue Scale Severity; 95% CI: 95% confidence interval; *: adjusted on age, gender, ADL/MMSE/PHQ, and Charlson scores
Considering the trust in “Louise,” the KANOPEE virtual agent, no significant association was found between ETQ scores and collected variables of interest. Although nonsignificant, ETQ-Credibility subscale tended to decrease when PHQ-9 depression score increased (β = −0.7, CI [−0.9, −0.4], p = .08). Similar effect was shown on ETQ-Benevolence subscale. Finally, although nonsignificant, credibility score of “Louise” remained higher for inpatients reporting advanced familiarity with digital technology, compared to novice inpatients (β = 1.5, CI [0.1, 2.9], p = .09). No other significant associations were detected in the models that were estimated.
Discussion
This study sheds new light on the use of digital technology for health in older patients hospitalized in geriatric wards, and brings original perspectives on insomnia evaluation and treatment in this population. This study highlights two main results, i.e. good acceptability of the KANOPEE app, and encouraging trust in its virtual agent, “Louise.” Hypothesizing that geriatric population's digital habits and use may differ from general adult's, our secondary analysis allowed a better understanding of the acceptability determinants, in order to tailor such app to this population.
Acceptability for KANOPEE app showed satisfactory results in our study, with a majority of older adults being satisfied or very satisfied on the Usability and Satisfaction subscales. The trust in “Louise,” the virtual agent, relying on Benevolence and Credibility subscales, also showed promising results. The distribution of these scores remained similar to those obtained in general adult population,10,11,22 although this comparison can be tempered by differences shown in Satisfaction and Credibility subscales distribution. Indeed, user satisfaction remained slightly lower comparing to general adults, and a higher proportion of patients disagreed with the credibility of “Louise” (25% against less than 20%), with more equivocal results for this subscale. The study population, being acute and rehabilitation older inpatients may partially explain these differences. The credibility of a virtual agent may be underestimated or less appreciated in hospital settings, where empathic professional caregivers and psychologists are available to provide the necessary support, as opposed to a virtual agent. Nevertheless, the potential target population of KANOPEE app is the general older adult population, for a domestic use, in order to assess sleep complaints. Therefore, these results remain encouraging, as acceptability and trust observed in our sample probably underestimates acceptability in the targeted population of older adults. However, population-related differences may also intervene in these different perceptions of technology, highlighted by our secondary objective.
Several factors were evaluated as potential determinants of acceptability and trust of KANOPEE app. Older age, gender, and education level were not associated with differences in users’ experiences. These results remain consistent with previous validation studies of KANOPEE app in general population, 10 and with recent systematic reviews on acceptance of digital technologies among older adults. 23 Familiarity with technology and digital habits seemed to improve the users’ experience, with reported higher credibility scores. This result, consistent with literature, highlights how digital literacy is a key determinant when considering and maintaining digital technologies, especially for older adults.6,7 Such digital background should be explored prior to recommend the use of KANOPEE app, and novice users may benefit from explanations and assistance of natural or health caregivers.
Among clinical determinants, acceptability, on both Usability and Satisfaction subscales, remained significantly higher for patients with increased Charlson multimorbidity scores after adjusting on sociodemographic and geriatric factors. Main prehospitalization comorbidities were cardiovascular and neurological conditions, clinical situations usually associated with polymedication and sleep disorders. 24 As a result, this nonpharmacological app may be particularly welcomed and by these patients, with a good usefulness perception of the app. On the contrary, a trend was observed for patients with higher depression scores according to PHQ-9 scale, with a reported lower credibility and benevolence experienced. One may hypothesized that such patients would rather benefit from a human interaction when a comorbid psychological trouble exists. This assertion aligns with existing literature that explores various theoretical frameworks of older adults digital engagement.6,23 Among the potential obstacles to digital engagement, depressive disorders may hinder motivation, perceived utility, and the capacity to adapt to new technologies. These findings warrant further investigation through studies with larger sample sizes to enhance statistical robustness. However, considering the frequent association between sleep and mood disorders, a specific attention should be paid on the digital engagement of this population, suggesting that digital interventions should be integrated into a comprehensive multidimensional approach that also incorporates human support and care.
Finally, our study provided pragmatic results in order to tailor KANOPEE app for older adults. Given that acceptability was notably lower among patients with hearing impairments, it is essential to consider such sensory challenges to enhance the user experience for these individuals. Recommendations include utilizing the app in quieter settings and encouraging the use of hearing aids or earphones. Furthermore, an enhanced version of the KANOPEE app, specifically designed for older adults, could be advantageous. Potential enhancements may rely on improved synchronization between the virtual agent's speech and lip movements, the inclusion of subtitles, and the option for users to request “Louise” to repeat interview questions.
For other determinants of AES and ETQ scores, no statistically significant or clinically relevant association was found. Further research is necessary to specify uncertain or negative results, and explore other clinical factors, based on a larger and more representative sample of older adults. Such research should also evaluate the determinants of long-term digital engagement in KANOPEE, especially in completing sleep diary on the app, for a complete sleep assessment. As digital engagement of older adults is multidimensional, the quantitative-based approach with acceptability scales could be enhanced with a mixed-methods approach and qualitative methodology assessments on acceptability of KANOPEE and its determinants. Depending on such exploratory and confirmatory studies, the efficacy on sleep duration and sleep quality of KANOPEE app and its behavioral intervention should be assessed.
This study has some limitations to acknowledge. This study was based among a clinical population in acute care or rehabilitation and might be not representative of the general older population. However, the acceptability is likely to be better in other condition and it is very encouraging to be able to use digital therapeutics even in hospitalization. Secondly, we were not able to test the acceptability of all application content which extends over 17 days. Further study should reassess acceptability at different times and adherence over the total period. Third, an experiment in ecological conditions is necessary to confirm that the research setting and the medical environment did not promote greater acceptability.
Conclusion
To conclude, these preliminary results confirm that older adults can use autonomous virtual agent-based applications to quantify their sleep and mental complaints. This research advocates for the use of this nonpharmaceutical and easily accessible application, which appears to be well-received and trusted among this population. Additionally, it contributes novel insights into the factors influencing digital engagement, in order to tailor such interventions to older adults. Further research is needed to confirm these preliminary findings and assess the broader impact of digital apps like KANOPEE on sleep complaints assessment and support, in a larger and more representative sample of older adults.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241293935 - Supplemental material for Assessing the acceptability of a sleep-targeted digital intervention among geriatric inpatients: A preliminary study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241293935 for Assessing the acceptability of a sleep-targeted digital intervention among geriatric inpatients: A preliminary study by Alex Chanteclair, Marion Lartigau, Nathalie Salles, Julien Coelho, Florian Pécune, Pierre Philip and Clément Champeville in DIGITAL HEALTH
Supplemental Material
sj-DOCX-2-dhj-10.1177_20552076241293935 - Supplemental material for Assessing the acceptability of a sleep-targeted digital intervention among geriatric inpatients: A preliminary study
Supplemental material, sj-DOCX-2-dhj-10.1177_20552076241293935 for Assessing the acceptability of a sleep-targeted digital intervention among geriatric inpatients: A preliminary study by Alex Chanteclair, Marion Lartigau, Nathalie Salles, Julien Coelho, Florian Pécune, Pierre Philip and Clément Champeville in DIGITAL HEALTH
Footnotes
Contributorship statement
All authors have approved the manuscript and participated sufficiently in the work. Marion Lartigau, Clément Champeville, Pierre Philip, and Nathalie Salles made a substantial contribution to the concept and design of the work. Clément Champeville and Marion Lartigau contributed to the collection and the analysis of the data. Statistical analysis were led by Alex Chanteclair, Florian Pécune. Alex Chanteclair, Marion Lartigau, Clément Champeville, Pierre Philip, Florian Pécune, and Nathalie Salles contributed substantially to the interpretation of the data. Alex Chanteclair drafted the article. All of the authors have critically revised the manuscript for important intellectual content.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This research being noninterventional, written consent was provided for each included patient. Data protection requirements of French Data Protection Council (CNIL) were followed.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data protection requirements of French Data Protection Council (CNIL) were followed under the Grant No. CHUBX2020GSP0102 for KANOPEE evaluations.
Guarantor
AC.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.