
Abstract
Aims
To determine the acceptability and identify potential concerns and barriers of using a hypothetical smartphone application (app) for home monitoring (HM) of visual function among patients with diabetes.
Methods
Quantitative, cross-sectional study using a self-administered questionnaire. Patients diagnosed with diabetes aged between 20 and 70 years were included. The research was conducted across five regions in Saudi Arabia. The questions were adapted from a validated, published questionnaire and translated into Arabic. It focused on socio-demographic factors and barriers which associated with the acceptance of the hypothetical visual function HM app, using descriptive statistics.
Results
A total of 240 patients with diabetes participated in this study. About half of the participants (40.4%) ranged between 40 and 59 years; 42.5% were male, and most of the participants (93.8%) lived within 2 h of their healthcare facility. The rejection to the use of a hypothetical HM app was associated with increased age (p = 0.025), lower education level (p = 0.023), urbanicity (p = 0.011), residing closer to health centres (p = 0.021), and never experiencing telehealth services previously (p = 0.025). Logistic regression revealed that accepting a hybrid clinic approach was more likely to be acceptable by younger patients (20–39 years: OR, 5.01; 95% CI, 1.82–13.82; p < 0.001; and 40–59 years: OR, 2.28; 95% CI, 0.084–5.00; p = 0.48), as well as patients who attended primary healthcare or specialised governmental clinics (p = 0.038 and p = 0.019, respectively).
Conclusion
Factors that altered patients’ acceptance of the hypothetical app included their age, educational level, urbanicity, traveling distance, and telehealth experience. Therefore, careful consideration of acceptability and barriers is essential before implementing such an intervention.
Introduction
Diabetes is a leading cause of sight loss internationally due to the development of diabetic retinopathy (DR) and/or diabetic macular oedema (DMO). The International Diabetes Federation reported that the prevalence of adults with diabetes worldwide is 537 million adults (age range, 20–79 years). 1 According to the Global Burden of Disease Study (2021), DR is now the fifth leading cause of blindness in adults aged 50 years and older. 2 The global prevalence of retinal complications among individuals with diabetes is 22.27% for DR, 6.17% for vision-threatening DR, and 4.07% for clinically significant macular oedema. 3
Studies indicate that diabetes disproportionately affects adult populations in countries such as the Middle East and North Africa (MENA) region. In this region, the prevalence of diabetes was 9.3% in 2021, and it is expected that the number of people with diabetes will rise to 11.3% by the year 2050. 4 In addition, the MENA population with visual impairment due to DR was estimated to be approximately 3.2 million by the year 2020. 5
Though the urbanised cities in Saudi Arabia have considerable healthcare services focused on diabetes, there has been a significant rise in the prevalence of diabetes by about 25.4% compared with rural areas.6,7 Further evaluation of the prevalence of DR in the Saudi National Diabetes Registry data showed an overall percentage of 19.7% due to the absence of fully structured screening programmes 7 and the shortage of healthcare infrastructure in rural areas.
Patients with diabetes require a regular comprehensive eye examination as DMO is considered a major cause of significant visual impairment. Therefore, carrying out a routine DR screening in primary eye care clinics according to established guidelines is important,8,9 as it enhances the ability to monitor the progression of retinopathy or instigate urgent referral if undertaken by well-trained specialists. 10 This can be delivered in most tertiary hospitals. However, tracking those patients regularly and effectively is challenging from the service delivery perspective.11,12 In addition, the high examination costs in the private sector and the difficulty reaching clinics from rural communities lead to patients dropping out of follow-up. This can lead to delayed or diminished outcomes and an increased risk of sight loss.
Thus, telehealth might offer a solution in primary care as several studies have shown its potential to reduce the burden on an already strained health system and solve delays in delivering healthcare services to patients with chronic diseases such as cardiovascular disease and diabetes. 13 In addition, it can provide a regular screening and monitoring examination for DR. 14
Before the COVID-19 pandemic, Alshammari et al. (2019) reported that 70% of 781 general beneficiaries in Saudi Arabia were satisfied and interested in using telehealth even with limited experience and knowledge about the app. 15
In addition, telehealth services have been developed with diverse implementation methods across several hospital departments in Saudi Arabia which were extensively adopted during the COVID-19 pandemic. About 19 digital applications (apps) or platforms were launched to provide healthcare services, education, and telecommunication.16,17 Government records have revealed that more than two million users had a general medical consultation during the pandemic, indicating the popularity of remote health services.18,19
Recently, various digital apps have been developed to measure visual function at home, such as DigiVis, 20 Smart Optometry, 21 and Peek Acuity. 22 Other digital apps apply gamification to increase the frequency of visual function measurements, such as Odysight 23 and OKKO health. 24
The roll out of digital health interventions requires an appreciation of local culture and traditions is essential to increase uptake. Factors such as patient's age, education level, economic situation, willingness to travel to clinics, and the costs associated with such a journey likely have a massive impact on the usability outcomes. Understanding these factors and other possible barriers to uptake will enable us to consider whether hypothetical home monitoring (HM) app is acceptable in this context. Therefore, this study aimed to assess the acceptability of a visual function HM app after the COVID-19 outbreak in Saudi Arabia.
Methodology
Study design and setting
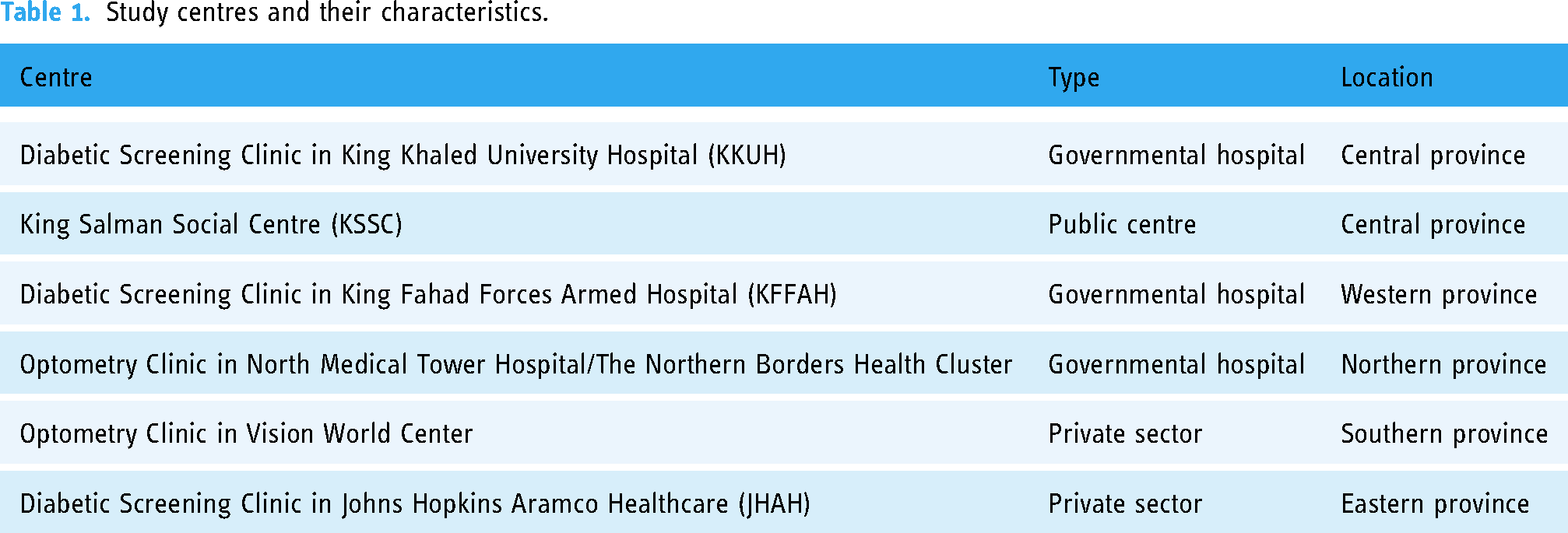
This is a quantitative, analytical, cross-sectional study using a self-administered questionnaire under the supervision of optometrists. This study was approved by the research ethics committee under the deanship of scientific research at King Saud University (E-22-6647) and adheres to the Declaration of Helsinki; additional approvals were obtained from the collaborating institutions. Written consent was obtained from all participants. The study was undertaken from August 2022 to October 2023. The research was conducted in six centres in Saudi Arabia (see Table 1 for centre characteristics).
Study centres and their characteristics.
The sample size was calculated using the G*Power online tool 25 with a confidence interval (CI) of 95%, a margin of error of 5%, and a critical Z (−1.64). Based on prior knowledge of estimates about the prevalence of diabetes in Saudi Arabia, 26 a population proportion of 20% was applied, leading to a calculated target sample size of 172.
Study participants and data collection procedures
Patients were recruited according to the information held within the hospitals/institutions in their medical records. Patients were aged between 20–70 years old, were diagnosed with either Type 1 or Type 2 diabetes, and were of Arabic ethnicity. Any patient below 20 years of age or with any evidence of cognitive decline was excluded. Their clinic presentation was mainly for a routine eye examination or screening due to a referral from another department. All cases were non-urgently referred after having a fundus examination test with either optical coherence tomography (OCT) or direct ophthalmoscope. The questionnaire was provided on a tablet directly after the examination or as a hyperlink to be sent to the patients through their WhatsApp or email to receive their responses within the examination day. The questionnaire was adapted from a validated questionnaire titled (Assessment of Patient Preferences for Telehealth in Post-COVID-19 Pandemic Health Care). 27 Further modifications were made regarding the average population size across cities and average total income. Additional questions focusing on visual performance and mobile phone proficiency were added. All questions were translated into Arabic to ensure accessibility for participants. The complete questionnaire in both English and Arabic is provided in Supplemental material. Each centre was provided with a target for sample responses ranging between n = 30–60 depending on each region's population distribution. A consecutive sampling strategy was employed.
The first section of the questionnaire contains 17 questions about patient socio-demographic characteristics, such as age, education level, total income, location to the nearest primary eye care clinic, and visual function status. Other questions included barriers to implementation, such as traveling time, whether technical assistance is required when using a mobile telephone, whether an escort was needed for attending visits, and the gender of the care provider. The responses to these questions were either numerical or short descriptive multiple-choice answers. Two ‘yes/no’ questions sought to determine whether the patients used telehealth options during the COVID-19 pandemic. Additional evaluation of a patient's acceptance of the visual function HM app was recorded in multiple-choice questions with further free-text short answer fields to enable them to insert their perspectives towards the selected option.
The second section contains five questions that gather information on the patient's preference for the following comparisons. Firstly, the respondents were asked about their baseline preference for an in-person or an HM app for a nonemergency ocular condition that could be handled either way. Then, the scope of the question was narrowed by specifying an HM app option. For those who preferred in-person, a second question was posed, offering the preferred modality for an out-of-pocket cost of 370 SR (98 USD) or an HM app. The fees were selected based on the average consultation fees in some private sector centres in Saudi Arabia. 28 For the respondents who expressed a preference for an app, we posed a second question: offering an in-person consultation for an out-of-pocket cost of 370 SR or the app for half of the consultation fees. Participants were asked about their willingness to download an HM app on their smartphone to track their visual status on a scale from 1 to 5, where 5 indicates the most willingness and 1 indicates firm refusal. Finally, participants were asked to evaluate the extent of their preference for an app rather than visiting a consultant, especially after the COVID-19 pandemic.
Piloting phase
Two senior researchers (K.S.A and A.A.A) reviewed each question in the questionnaire to ensure the clarity of the contents. Then, a pilot phase was performed by distributing the questionnaire to three optometrists from different regions to assist with the clarity of the text and determine the time required to complete the questionnaire until no further modifications were requested.
Statistical analysis
Statistical analysis was performed using SPSS version 28 (IBM Corp., Armonk, NY, USA). Data from closed-ended questions were converted to numerical data and entered into SPSS. Outcomes from descriptive statistics were presented as frequencies and percentages for categorical variables. We used the chi-square test for bivariate comparisons of in-person or HM app, age range, educational level, total incomes, and other barriers. Adjusted multinomial logistic regression was implemented across demographics and applied to identify preferences after the COVID-19 pandemic using demographic variables with less than 1% missing data. The odds ratio (OR) with a CI of 95% and a p-value less than (0.05) was applied to be considered statistically significant.
Results
Patients’ demographics
A total of 240 subjects agreed to participate in this study: Central Province (n = 62), Eastern Province (n = 65), Western Province (n = 30), Northern Province (n = 41), and Southern Province (n = 42). One participant was excluded for not having Arabic ethnicity and not completing the questionnaire, leaving (n = 239) available for analysis. The centre's location, type, and participant demographic responses are summarised in Table 2. Of the participants, 40.4% were in the average range between 40 and 59 years old, and nearly 36% of the participants either had a minimum degree of high school or a bachelor's degree. About half of the participants (47.9%) had a monthly income range between 10,000 SR and 19,000 SR, and 58.3% of participants resided in a city with more than one million residents. Most participants (93.8%; n = 225) were required to travel for 2 h to reach their healthcare appointment, while 60% of the participants could travel without the need for assistance or escort.
Patients’ demographics (n = 239).

GS: governmental sector; PS: private sector; PC: public centre; HS: high school; Dip: diploma; BSc: bachelor (undergraduate degree); PG: postgraduate degree. b Overall percentage (I don't mind + Partially + As much as possible)
Nearly 40% (n = 98) of the subjects attended primary eye care for regular follow-up visits, and 47% (n = 113) attended for a routine eye examination. Meanwhile, 19.6% (n = 47) reported that they had been diagnosed specifically with DR. Over half of the patients required reading glasses due to refractive error or presbyopia, 54.6% (n = 131). A smaller proportion (6.7%) believed that they needed glasses but were not currently using them. Of the respondents, 27.9% reported normal vision as they did not need any correction, and 9.6% were unsure about their need for glasses. Of the participants, 8.5% reported that they were visually impaired, while the vast majority (81.7%) indicated they were not. Additionally, 2.1% reported they were borderline for visual impairment, and 6.3% were unsure. However, more than half of them used their mobile phone independently.
Despite only 9.6% (n = 23) having previous experience with telehealth services, there was an overall acceptance of 67.1%, representing 48.8% who did not mind trying. Few subjects (10.4%) accepted using the app partially, and 7.9% of participants were happy to use the app as much as possible. In addition, 43.8% were very willing to download an app for visual function assessment, whereas nearly 20% showed ‘average’ and ‘very unwilling’ to download the app.
Most participants (40.8%) preferred in-person care after the COVID-19 pandemic; 33.3% were willing to use the app occasionally, and only 16.3% would be willing to use it as much as possible.
How do patient demographics impact the acceptability of the visual function HM app?
Regardless of the financial consequences, there was a significant trend towards in-person examinations due to age, education level, urbanicity, travel distance, and patients who never used telehealth before, as shown in Figure 1.

The impact of the most demographic factors that affect the acceptability of the visual function HM app.
There was a significant hesitation in using an HM app in older patients (p = 0.025). Explicitly, 54.1% of older patients (>60 years) preferred an in-person visit. The highest proportion of patients in our sample was aged between 40 and 59 years; most of them preferred an in-person visit (37.4%), while 33.3% preferred HM app occasionally, and 17.2% preferred as much as possible. In comparison, few participants had no preference for either option (12.1%). On the other hand, among younger patients between 20 and 39 years old, most of them (47.3%) preferred the app occasionally or as much as possible (20%).
Patients with lower educational levels preferred in-person visits compared with those with higher academic levels. Specifically, 47.6% of high school graduates and 48.9% of diploma graduates preferred physical visits (p = 0.023).
Furthermore, the results indicated that the most influential barriers to patients’ preferences were urbanicity (p = 0.011) and travelling distance (p = 0.021) compared with the other barriers addressed in this questionnaire. Consequently, 54.7% of patients who lived in central cities and 42.2% who resided more than 2 h from their nearest healthcare centre tended to prefer physical visits. However, patients who lived less than 2 h away showed the highest willingness to use the app as much as possible (80%), and patients who lived 3 to 5 h away showed the highest willingness to use HM app occasionally (75%).
Ultimately, among the few patients who experienced previous telehealth services, 52.2% of them preferred to use HM app occasionally. Others preferred using it as much as possible or had no preference 17.4% (p = 0.025) (Table 3).
The preference for using HM app after COVID-19.

HS: high school, Dip: diploma, BSc: bachelor (undergraduate degree), PG: postgraduate degree.
How does cost impact acceptance of HM app?
Whether cost contributed to their preference for a nonurgent eye examination is described in Table 4. Out of 124 patients who preferred an in-person appointment for a nonurgent condition, 71.6% still insisted on this preference despite the extra cost of paying for a private clinic; in this scenario, only 14.7% switched to preferring HM app. In contrast, out of 31 patients who preferred HM app, 20% switched to a governmental or private sector clinic to be seen in-person if the app was going to cost half of the physical consultation. However, 63% were still keen to manage remotely despite the additional cost of using an HM app. Patients who preferred either option of care services or those who were uncertain which visit modality they preferred were not questioned on the impact of cost (Table 4).
Visit modality preference for an unurgent eye examination.

Subsection questions for the first option.
Subsection questions for the second option.
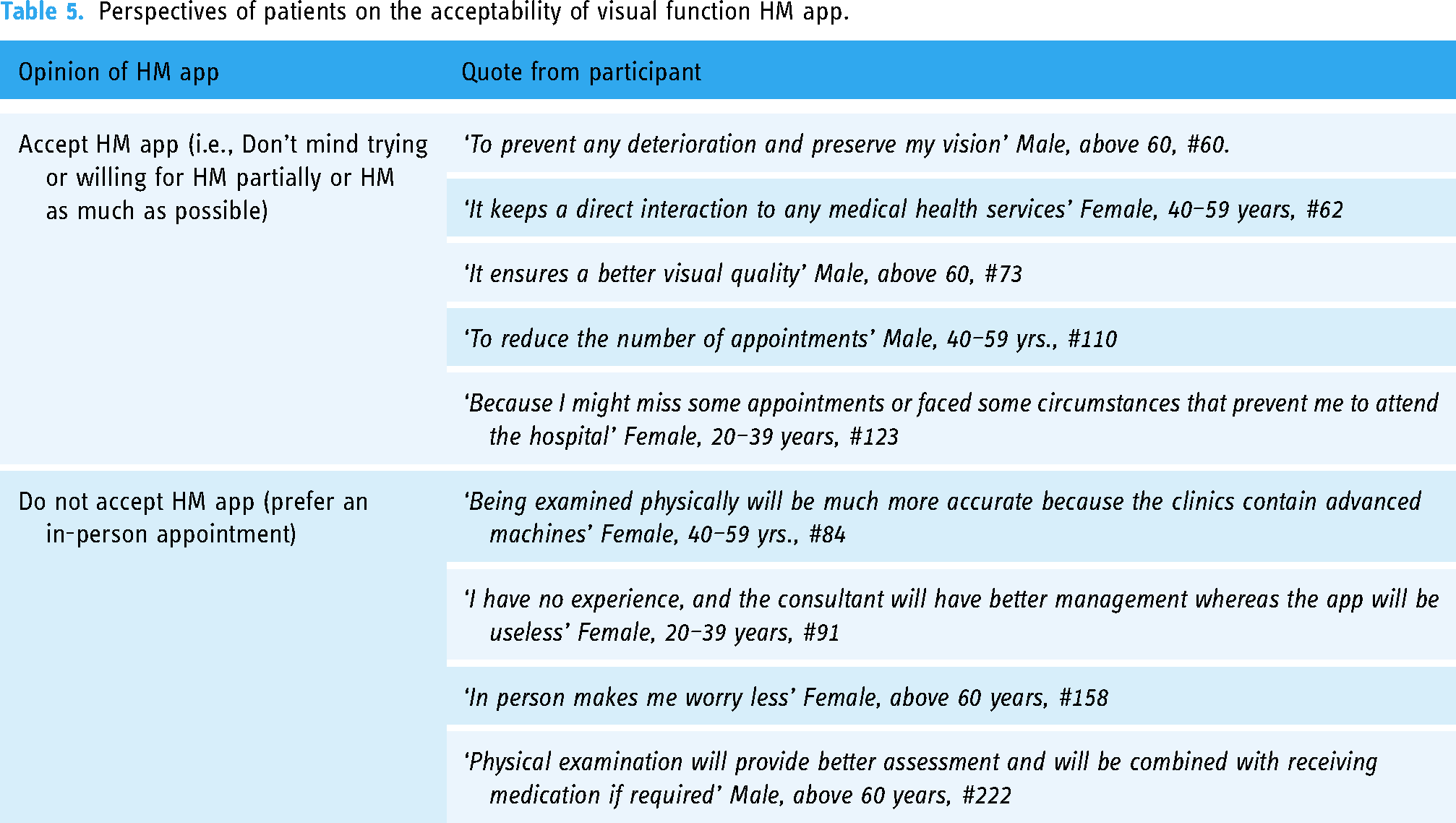
Further perspectives gained from free-text short answers
To provide further perspective from responses of participants, (n = 54) short answers were categorised into two sections based on whether they were willing to accept an HM app or not. The quotes of their words were translated and summarised in Table 5.
Perspectives of patients on the acceptability of visual function HM app.
Combinations of factors associated with patients’ preferences towards visual function HM app
An adjusted multinomial logistic regression was applied to find which factors were associated with HM app usage preferences. The OR and CI of the adjusted predictors are found in Table 6. Females (OR, 0.453; 95% CI, 0.21–0.92; p = 0.029), younger patients (20–39 years: OR, 5.01; 95% CI, 1.82–13.82; p < 0.001; and 40–59 years: OR, 2.28; 95% CI, 0.084–5.00; p = 0.48), and patients with diploma certificates (OR: 0.13; 95% CI, 0.03–0.60; p = 0.007) were more likely to accept usage of an HM app. Patients with a total income below 30,000 SR (8000 USD) were more likely to consider using HM app occasionally. Both collinearity and the potential interaction effect between education and income were evaluated. Collinearity did not appear to be an issue, as all Variance Inflation Factor values were well below the commonly accepted threshold of 5. Furthermore, patients who regularly visited primary care clinics or specialised governmental clinics were strongly associated with the preference of using HM app occasionally (p = 0.038 vs p = 0.019). Patients with no previous experience with telehealth services were also more likely to accept using an HM app occasionally (p = 0.01) (Table 6).
Predictors of preference for HM app after COVID-19.

Multinomial logistic regression (in person) was indicated as a reference. b HS: high school, Dip: Diploma, BSc: bachelor (undergraduate) degree; PG: Postgraduate degree. * p-value <0.05
Discussion
This study explored the acceptance of a hypothetical HM app for assessing visual function remotely in patients with diabetes in Saudi Arabia. The study found that the reluctance to use a HM app was associated with increased age, lower levels of education, urbanicity, short traveling distance to healthcare facilities, and those who had never experienced telehealth services. Surprisingly, the consideration of cost did not play a significant role. The study also showed that females, younger patients, and those who regularly attended primary eye clinics or specialised governmental clinics for routine eye examinations and who never used telehealth services were more likely to accept a hybrid clinic.
The potential for acceptance
In this study, there was generally a positive response to the prospect of using an HM app. The overall satisfaction with telehealth services in Saudi Arabia was studied by Eddine et al. (2021). The study found that half of the patients were satisfied with the virtual clinic within the ambulatory care centre in Saudi Arabia during the pandemic. 29 Dawood et al. (2022) indicated a similar level of satisfaction (76.36%) using (Sehhaty) app provided by the Saudi government to provide general consultations remotely during the pandemic. 30
Further studies showed a strong acceptability and feasibility of adopting HM devices. For instance, a recent study evaluated the acceptance and feasibility of using a visual field HM device and home tonometer for glaucoma patients. Interesting acceptability has been indicated in all patients with glaucoma using the iCare HOME tonometer and Virtual Field (VF) devices at home multiple times daily for a week. The study was combined with a semi-structured interview. The thematic analysis emphasised the benefits of using VF as many patients believed that HM devices could reduce the traumatic experience due to glaucoma and the anxiety expression for visual loss, and it would also encourage independence by allowing more control when they use the device. 31 Differences in the level of satisfaction could be due to differences in literacy rates, economic status, network coverage, and logistical restrictions on implementing new technologies. However, the overall positive satisfaction with telehealth services provided in Saudi Arabia may imply the potential of accepting to track visual function for patients with diabetes with stable conditions. Consequently, it could reduce the load of the routine eye screening setting and promote early intervention.
Barriers to accepting visual function HM app
This study showed that age, educational level, and previous telehealth experience were the most common mitigations perceived by our participants. Addressing these barriers before implementation may improve the acceptance of an HM app.
Age and educational level
This study had limited participants with a previous diagnosis of DR or visual impairment (VI), and we could not find any significant correlation between visual performance, level of impairment, independence, and confidence in handling a mobile phone, as most of the patients with diabetes who attended the diabetic screening clinics were in a stable condition. However, it was evident that those over 60 years of age and those with less than a diploma level of education were very reluctant to use an HM app. Our results were similar to Thirunavukkarasu et al. findings (2021), which indicated a reduction in the satisfaction rate of patients >40 years old who used telehealth features and those with less than undergraduate certificates. They also showed diversity across different specialised clinics. They reported the lowest percentage of telehealth consultations in ophthalmology clinics compared with all other clinical specialities, which could be correlated with inadequate competency due to visual and hearing difficulties in older patients. 32 In our multinomial regression model, we predicted that younger patients (<60 years) were more likely to accept HM app occasionally. The demographic of the participants who accepted an HM app in our study were older (40–59) compared with the subjects in the study by Thirunavukkarasu et al., who were predominantly under 40 years of age. In our study, younger patients showed higher acceptance of the hybrid model compared with the older group. Differences in the level of acceptance among participants’ age groups could be related to inclusion criteria, patients’ medical conditions, the department involved, or differences between healthcare technologies.
Several studies have also highlighted factors that could increase acceptance of telemedicine and HM devices in patients with common ocular diseases. For instance, Liu et al. (2022) investigated a health information technology (HIT) acceptance model in patients with hypertension and diabetes. Perceived visual function (PVF) was tested on a tablet every 8 weeks up to 24 weeks, and they reported that it indirectly influenced behavioural intention (BI), which changed their acceptance over a longer period. This could be associated with the limitation of visual perceptions among older people and make monitoring patients with patient-focused HIT systems very challenging. 33 Furthermore, the MONARCH study implemented three tests (paper-based KeepSight Journal, the MyVisionTrack®, and the MultiBit App) for age-related macular degeneration (AMD) patients and evaluated their acceptability and adherence to weekly HM. The study highlighted that feasibility could be improved if the apps were quick and easy to use for older participants. 34
Previous experience with healthcare technology
The present study showed that more than half of the participants (56.3%) were using their mobiles independently and 21.3% of participants required assistance for some technical issues. However, the acceptance of adopting an HM app was mainly influenced by previous experiences with telehealth services in our patients. Few subjects (9.6%) used telehealth features provided in our study; half of those patients preferred to use an HM app occasionally. The acceptability of HM in the MONARCH study was also influenced by a patient's understanding of its purpose. Unfamiliarity in digital technology use was found to be due to the lack of initial training and ongoing support. Both of which were considered essential to the successful implementation of telehealth monitoring. 34
Another modality of HM app in glaucoma has been investigated and provided great diagnostic power when using a tablet-based visual field test compared with in-clinical testing. However, the biggest barriers that affected the uptake and compliance of this technology were the lack of motivation and technical experience to perform the test without assistance, which could also be related to health deterioration. 35 This study showed that less than half of the participants (43.8%) were very willing to use visual function HM app. It has also been predicted that participants who have never experienced telehealth options were more likely to accept an HM app occasionally, and this might reflect their willingness to involve digital technology in healthcare services for older people and their awareness of the advantages of similar apps in early intervention. A similar modality of telemedicine's advantages and disadvantages has been conducted among physicians in Taif. The study showed that almost a third of physicians believed that telemedicine increased the effectiveness of therapeutic intervention due to the enhancement of the care quality. 36
Accepting HM app and its impact on travel distance and cost
In general, most patients with diabetes who participated in our study were persistent in preferring a physical examination regardless of the incurred costs, which may reflect their priority of saving their sight. Few studies have evaluated the impact of the cost on patients’ acceptance of adopting HM apps. Peek et al. (2014) showed that the most crucial aspect concerning telemedicine services in the pre-implementation stage was the high cost, especially for older people. A recent systematic review showed that cost was the most concerning aspect of using technology (p < 0.05). 37
On the other hand, the present study depicted that patients who attended primary eye care and governmental hospitals could accept hybrid. The economic benefits of telemedicine in DR have been addressed in previous studies.38,39 The cost-effectiveness of DR screening programmes using telemedicine was reviewed and highlighted ultimate cost-saving benefits for the patients in terms of increasing their independence and reducing the need to travel to the nearest hospital. 40 This finding might emphasise the utility of implementing similar apps in our communities and reduce the economic burden of diabetes. It would enhance the role of health services in screening patients with DR, aligning with the Vision 2030 goal of fostering a healthy society with fulfilling lives in Saudi Arabia. 41
Limitations
Our sample size exceeded the targeted number, providing a better dataset than initially planned. However, limitations were related to the potential of selection bias in terms of subjects who were willing to take part in the survey to adopt new healthcare services than those who refused to take part. In addition, this study relied on self-report and had no accompanying clinical information to verify diagnoses. While this survey provided insight into patient intentions, real-world longitudinal tracking usage of an HM app would be a more accurate means of assessing feasibility.
Conclusion
While an HM app may offer efficiency for health service delivery and patient convenience, this study demonstrated that careful consideration of acceptability and barriers to uptake are essential before implementation. In this population, there is considerable hesitation in accepting HM of visual function via an app related to older individuals, low educational level, urbanicity, and those living close to healthcare services. Therefore, considerable mitigation may be required to achieve successful implementation. Those wishing to implement such a device must address the barriers highlighted by this study and develop better features within the app, increasing patients’ engagement, especially for old adults. Despite the challenges, smartphone app could be transformative in healthcare delivery in addressing the lack of equipment and skilled specialists in rural areas.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241290405 - Supplemental material for ‘Assessing patients’ perception of the potential utility of visual function home monitoring app among patients with diabetes in Saudi Arabia’
Supplemental material, sj-docx-1-dhj-10.1177_20552076241290405 for ‘Assessing patients’ perception of the potential utility of visual function home monitoring app among patients with diabetes in Saudi Arabia’ by Hanan Khalid Mofty, Marwan A Abouammoh, Hala A Al-Muqbil, Khaled S AL-Zahrani, Talhah M AL-Ghasham, Abdullah A Assiri, Ahmad T AL-Mnaizel, Hayat S Mushcab, Kholoud A Bokhary and Ruth E Hogg in DIGITAL HEALTH
Footnotes
Acknowledgements
The study is sponsored by the External Joint Supervision Programme (EJSP) at King Saud University. It was designed in collaboration with the Saudi Society of Optometry (SSO). The first author would like to acknowledge all clusters, governmental hospitals, private centres, and social centres mentioned for their collaboration in collecting the data. Diabetic Screening Clinic in King Khaled University Hospital (KKUH), King Salman Social Centre (KSSC), Diabetic Screening Clinic in King Fahad Forces Armed Hospital (KFFAH), Optometry Clinic in North Medical Tower Hospital/The Northern Borders Health Cluster, Vision World Center, and Diabetic Screening Clinic in Johns Hopkins Aramco Healthcare (JHAH).
Contributorship
HKM and REH conceptualised and designed the study. HKM investigated, analysed, and wrote the initial draft of the manuscript. KSA and AAA were involved in the pilot phase of the methodology. HAA, KSA, TMA, AAA, ATA, and HSM were involved in data collection. MAA, KAB, and REH reviewed and edited the manuscript and approved the final version. All co-authors have reviewed the manuscript and approved it for submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the research ethics committee under the deanship of scientific research at King Saud University (E-22-6647) and adheres to the Declaration of Helsinki; additional approvals were obtained from the collaborating institutions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is part of the PhD project. The scholarship of the first author is financially funded by External Jount Supervision programme (EJSP) at King Saud University, Riyadh, Saudi Arabia.
Guarantor
HKM and REH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.