
Abstract
Introduction
Sleep is an important part of maintaining human health. Good sleep quality not only promotes mental health but also relieves fatigue, helps the body focus, improves reaction and judgment, and reduces the risk of adverse events such as traffic accidents and medical errors.1,2 In contrast, chronic insomnia can adversely affect the body's immune 3 and cognitive functions, 4 and even cause anxiety and depression, 5 having serious consequences.
During the COVID-19 pandemic, the increase in cases placed a huge burden on the healthcare system, and a large number of medical staff worked on the frontlines of the fight against the pandemic and played a crucial role in its control. However, the quality of sleep of medical staff is neglected by many. Numerous factors affect the quality of human sleep, especially as medical staff were often required to work long and intense hours in isolation wards during the pandemic and were subjected to tremendous pressure regarding the care for those afflicted and the uncertainty regarding disease control. 6 Additionally, medical staff were some the most vulnerable people during the COVID-19 outbreak, and their mental health symptoms are often more severe than those of the general population.7,8 Their working longer hours and increased night shifts are risk factors for developing depression and anxiety. 9 In addition, the number of infections and deaths among healthcare workers owing to COVID-19 was constantly reported in the news media, which may have led to ostracism of healthcare workers due to the misconception that they carry the virus and a decrease in contact with relatives and friends due to the fear of infection or infection of others. This could have led to a lack of social support for healthcare workers, thereby affecting their self-efficacy, sleep quality, and anxiety levels. 10 Thus, the outbreak of COVID-19 created serious psychological distress for medical professionals and improving sleep quality may have a positive impact on daily mood 11 ; daytime mood has a counterproductive effect on sleep quality. A strong correlation exists between mental health and sleep quality, which then likely contributes to insomnia in medical staff. 12 Therefore, it is reasonable to assume that factors such as length of job and work shift will have a direct impact on the sleep quality of frontline medical workers assisted in Shanghai in Fujian Province.
Exploring the sleep quality of medical staff during COVID-19 is not a new area of study; for example, studies have been conducted by foreign scholars showing that medical staff have significantly more sleep problems than other occupational groups, which are associated with increased time and labor intensity, 13 but few researchers have applied machine learning (ML) for sleep quality prediction; to some extent, scientific guidance for improving the sleep quality of medical staff is lacking. Machine learning is a continuum of computer science and statistics integration that has been used with some success in some medical specialties. 14 Machine learning techniques have been used to predict the sleep quality of different populations such as university students and medical staff during the COVID-19 pandemic,15,16 but, to the best of our knowledge, no study has explored the factors affecting the sleep quality of frontline medical staff from multiple perspectives and developed models for prediction, especially in Shanghai as the economic, financial, trade, and shipping center of China, characterized by a large flow of people and a high number of COVID-19 infections, which has placed more pressure on frontline medical staff.
The aim of this study was to analyze the factors influencing the sleep quality of medical staff in Shanghai, China, from a multidimensional perspective. On this basis, we established a method based on logistic regression (LR), artificial neural network (ANN), random forest (RF), gradient boosted tree (GBT), naive Bayes (NB), and decision tree (DT) to predict the sleep quality of frontline medical staff in Fujian Province, China. We compared the performance of the different models. Our study provides a scientific reference for improving the sleep quality of these frontline medical staff.
Methods
Data sources
From 25 June 2022 to 14 July 2022, a retrospective, cross-sectional survey was conducted with 1326 medical workers in Fujian Province to understand the sleep quality of frontline medical workers in Shanghai during the COVID-19 pandemic. After the Chinese questionnaire was completed, a literature search, clinical expert discussion, and validation were conducted; finally, the online questionnaire tool called “Sleep Medicine Research Management Platform” was used to create the online questionnaire.
The survey requested basic information such as age, sex, education, job title, years of work, and marital status; factors influencing sleep quality; and the Pittsburgh Sleep Quality Index (PSQI) questionnaire. The PSQI questionnaire is a self-reported instrument applied to assess the respondent's sleep quality in the past month, which consists of 18 self-assessment entries in seven domains including subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping pills, and daytime dysfunction. Each component is scored on a scale of 0–3, and the overall score ranges from 0–21, with higher scores indicating poorer sleep quality. Previous studies have confirmed that taking a PSQI score of 7 as a reference threshold for classification of sleep quality is more suitable for Chinese population.17,18 Since the subjects of this study were Chinese, we defined PSQI < 7 as good sleep quality, while poor sleep quality was defined as PSQI > 7 (Details are represented in the Supplementary File 1).
The study inclusion criteria were (1) administrators, nurses, clinicians, and other (medical technology, pharmacy, and testing) personnel who participated in frontline medical work against COVID-19; (2) those working on the clinical frontline for ≥1 week; (3) those located in cities throughout Fujian Province; and (4) those who completed the questionnaire within 10 min.
The exclusion criteria included (1) nonworking medical staff; (2) nonmedical staff from various cities in Fujian Province; (3) questionnaire filling time too short (<100 s) or too long (>10 mins); and (4) questionnaire whose answers were obviously abnormal.
Based on the aforementioned inclusion and exclusion criteria, we eliminated missing and outlier values, resulting in a total of 1326 valid questionnaires included, as illustrated in Figure 1.

The flowchart of this study data sources.
Statistical analysis
Descriptive analysis was performed for all variables. Quantitative data with a normal distribution are expressed as mean ± standard deviation (x ± s), α = 0.05. Frequency and percentage were used for count data, whereas “sex” and “involvement in public health emergencies” were analyzed with two independent samples t-tests, and others were analyzed with one-way ANOVA. To explore the effect of life changes on frontline medical staff's sleep-related factors and the incidence of sleep quality, univariate and multivariate logistic analyses were conducted. Multiple comparisons using ANOVA and the Bonferroni method were used for multiple comparisons to explore the differences among frontline medical staff in Fujian Province during the Shanghai COVID-19 period, compared with univariate analysis at p < 0.05 and multivariate analysis at p < 0.05 considered statistically significant. All statistical data were analyzed using SPSS 26.0 and R version 4.2.3.
Development and validation of prediction models
Logistic regression is a multiple regression method used for analyzing the relationship between binary results or classification results and multiple influencing factors. One major advantage of LR over other similar methods (e.g., probability regression) is that the exponential LR slope coefficient (eb) can be easily interpreted as the odds ratio (OR). The OR is the degree of change in the odds of a particular outcome by 1 unit in the independent variable or reference category. 19 Artificial neural network is a statistical method that simulates complex neural connections and mimics the learning dynamics of the human brain. These two methods play important roles in clinical decision making, and their goal is not biological reality but to provide effective models for nonlinear regression or classification. 20 An ANN model can be trained to identify complex functional relationships between covariates and response variables. Artificial neural networks outperform linear models in several clinical areas. As such, ANN is becoming a powerful algorithm for predicting medical diagnoses.21,22 Naive Bayes is a simple probabilistic classification method based on Bayes’ theorem, and the models are trained on a training dataset. Naive Bayes is a simple model, capable of handling noisy data and learning from small datasets, 23 and can be used to retrieve detailed information related to each observed object to analyze the performance of the system based on accurate outcome predictions.24,25 Gradient boosted tree is an iterative DT algorithm that can flexibly handle various types of data, including continuous and discrete values; additionally, with relatively little tuning time, the prediction accuracy can be relatively high. However, GBT has not yet become a mainstream tool for medical imaging due to its computational cost. 26 Random forest is a typical supervised learning algorithm based on DTs and has long been a widely popular approach in medical image analysis. 27 Random forest involves a set of DTs during training and outputs patterns of classes predicted by individual trees 28 using majority voting of the trees to predict outcomes and minimize training error. 29 Decision tree is a predictive model in ML, providing an intuitive use of probabilistic analysis as a graphical method. Its main purpose is to learn from observation and logic. Rule-based prediction systems represent and classify events. 30
In summary, the six decision algorithms have their own emphasis and advantages and disadvantages on predicting the correlation between independent and dependent variables. Therefore, further comparison of these six models can be explored to find a prediction model that is more suitable for the purpose of this study. We utilized grid search to search the hyperparameter space efficiently. This allowed us to find the optimal combination of hyperparameters for each model.
A total of six models were developed using LR, ANN, NB, GBT, RF, and DT. The samples were grouped using a cutoff point of 7 for PSQI scores, with scores ≥7 defined as poor-quality sleep and scores ≤7 defined as high-quality sleep. All models were trained to predict the sleep quality of medical staff during COVID-19 in Shanghai using the variables found to significantly affect sleep quality. Regarding feature selection for the six predictive models, we chose variables that were statistically significant based on single-factor and multi-factor logistic analyses (p < 0.05). We conducted data splitting using a random split method with an 8:2 ratio. The included data were divided into a training test set (n = 1061, 80%) and an independent validation set (n = 265, 20%). Stratified sampling was performed based on the results of the sleep quality assessment. To avoid over-fitting and improve the model, we used a 10-fold cross-validation in the training-test set. This method involves dividing the dataset into 10 approximately equal parts, using nine parts for training and one part for validation in each iteration, repeated 10 times with different validation sets each time.
The area under the curve (AUC), the area under the precision-recall curve (AUPR), and the calibration curve of the six models in the training set. The higher AUC and AUPR value closer to 1 indicates better performance. In addition, we calculated performance metrics including AUC, accuracy, sensitivity, specificity, precision, F1 score, and kappa. All models were performed using R version 4.2.3. Finally, the calibration curve was analyzed to assess the agreement by the slope, intercept, and Brier score of the calibration curve.
Results
Demographic characteristics of participants
This study was conducted on 2024 medical staff in Fujian Province supporting Shanghai, and a total of 1326 valid questionnaires were collected, accounting for 65.96% of the medical staff in Fujian Province supporting Shanghai at this time. Table 1 shows the descriptive statistics of the sample, including age, sex, place of residence, marital status, and education level. Most of the medical staff involved in Shanghai aid were women (75.8%); mainly from Fuzhou, Xiamen, and other regions; most of them were married; their education was at the bachelor degree level and above; and the numbers of those above and below 35 years of age were similar.
Demographic characteristics of survey participant (N = 1326).

Sleep quality of frontline medical staff in Fujian province during COVID-19 in Shanghai
Comparison of sleep quality scores of medical staff in different support positions
The results of the statistical analysis showed that the mean PSQI score of the participants was 11.354 ± 4.051. Of the 1326 participants included in the sample, 254 frontline medical staff had high sleep quality and 1072 had poor sleep quality, with a sleep disorder detection rate of 80.8% (n = 1072).
Among the seven dimensions of the PSQI, we found no statistical significance in the use of time to fall asleep, sleep duration, or use of hypnotic medications (p = 0.804, 0.184, and 0.136, respectively). The medical staff supporting the fever clinic had the lowest scores for sleep disturbance (1.402 ± 0.792), daytime dysfunction (1.566 ± 1.029), and total PSQI score (10.665 ± 4.249), which indicated that this group of medical staff encountered the fewest barriers to sleep and the experienced the highest functional activity during the day. In contrast, the medical staff responsible for nucleic acid specimen testing had the highest scores for subjective sleep quality (1.984 ± 0.833), sleep disturbance (1.961 ± 0.853), and daytime functional impairment (2.058 ± 0.908), which indicated that they had the worst sleep quality, encountered the most barriers to falling asleep, which had the most impact on their functional activities during the day. The overall PSQI score showed that the medical staff supporting the fever clinic had a better overall quality of sleep (10.665 ± 4.249), whereas the medical staff responsible for nucleic acid specimen testing had the worst overall quality of sleep (12.708 ± 3.892). However, the overall sleep quality of medical staff was poor regardless of support position (Table 2).
Comparison of sleep quality scores of medical staff in different support positions (

Compared with designated hospital general ward.
Comparison of sleep quality scores of medical staff with different titles
Here, statistically significant differences were found for sleep quality, time to sleep, use of hypnotic drugs, and daytime dysfunction. The medical staff who did not have a title had the lowest scores in all categories; whereas the medical staff at the senior level had the highest scores in most categories. The total PSQI score of the former (9.410 ± 4.778) and the latter (13.094 ± 4.631) indicated that the medical staff who did not have a title had the best sleep quality, whereas those at the senior level had the worst relative sleep (Table 3).
Comparison of sleep quality scores of medical staff with different professional job titles (
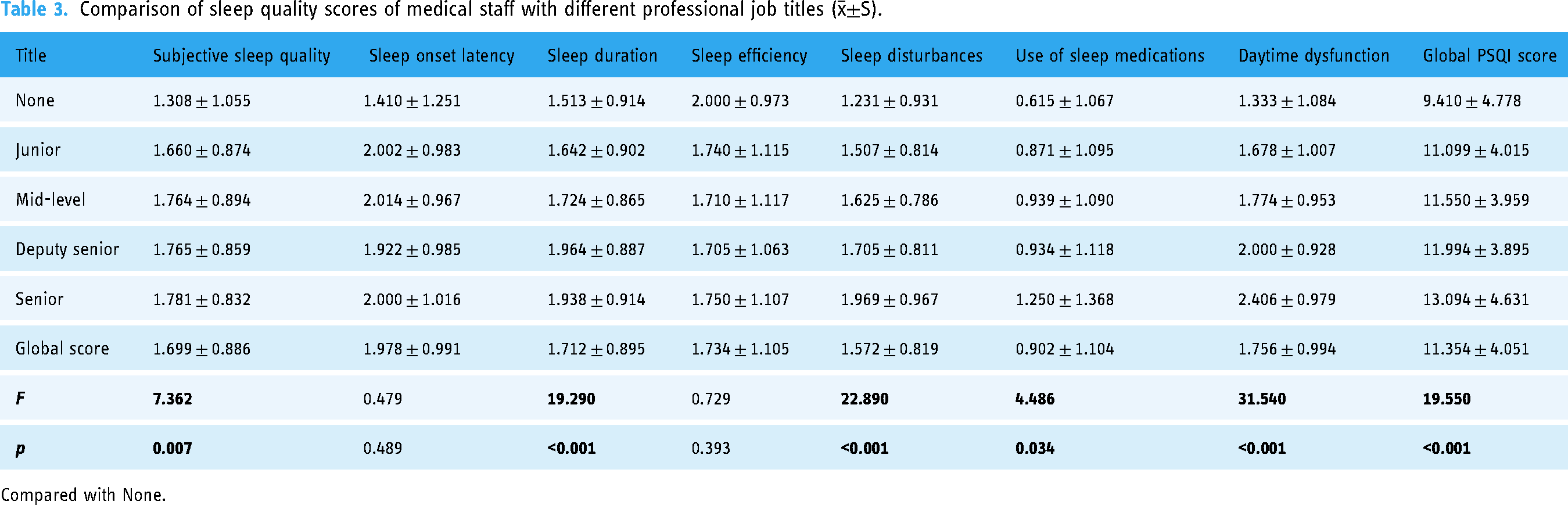
Compared with None.
Comparison of sleep quality scores among medical staff with and without medical assistance history
Medical staff who had a history of providing medical assistance showed statistically significant differences compared with those without in all five categories of the PSQI, except for time to sleep and sleep efficiency. Medical staff who were involved in the treatment of public health emergencies had higher sleep quality than those who did not; therefore, the latter used hypnotic medications at a higher rate than the former (Table 4).
Comparison of the detection rate of seven sleep problems in this study for those with and without a history of providing medical assistance [n (%)].

Each PSQI component score > 1 point indicates a sleep problem.
Analysis of factors affecting sleep quality of medical staff
We used one-way analysis of the factors influencing the sleep quality of medical staff. The results of the chi-square test showed that their sleep quality of medical staff during the aid period in Fujian Province in 2022 was associated with the following 12 variables: education, weight change, type of work, job title, working hours, medical aid history, support position, working shifts, daily working hours in contaminated areas, drinking tea during assistance, smoking during assistance, and underlying diseases.
Multivariate unconditional LR analysis was performed to determine the predictors of sleep quality among the medical staff during COVID-19 Shanghai. The PSQI score was selected as the dependent variable. The 12 variables that were statistically significant for univariate analysis were included as independent variables in multifactorial unconditional LR analysis. The results showed that six variables were associated with sleep quality, namely, weight change, type of work, professional title, work shift, tea consumption during assistance, and underlying illness. Lighter weight, day shifts, working >8 h per day, and drinking tea >1–2 times per week were considered factors influencing poor sleep quality. The details are shown in Table 5.
Analysis of factors affecting sleep quality (number) among medical staff in this study.
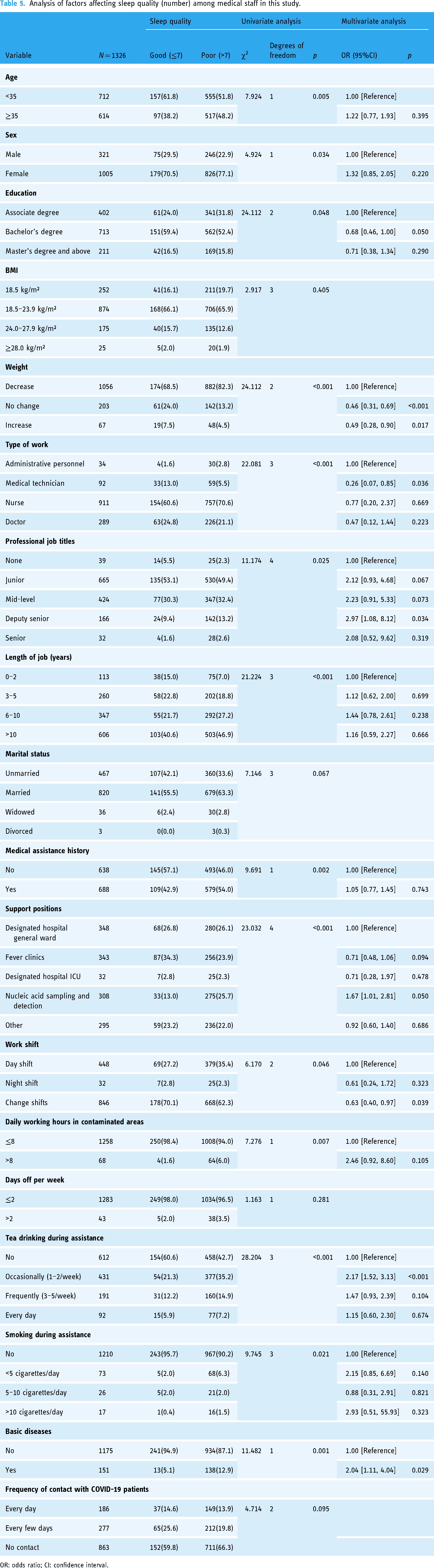
OR: odds ratio; CI: confidence interval.
Performance of prediction model
As previously described, the prediction model used to screen frontline medical staff for poor sleep quality had six input parameters. After adequate training, the six models were applied to the validation set. The metrics of all models are shown in Table 6. The hyperparameters of the optimal ANN model were: training cycles = 200, learning rate = 0.01, and Momentum = 0.9. The hyperparameters of the remaining five models are detailed in Supplementary file 2. The generated models all performed well, with AUCs of 0.663, 0.716, 0.656, 0.636, 0.523, and 0.642 for LR, ANN, NB, GBT, RF, and DT, respectively. The ANN model had AUC, AUPRC, accuracy, sensitivity, specificity, precision, F1 score, and kappa values of 71.6%, 69.7%, 68.7%, 66.7%, 69.2%, 34.0%, 45.0%, and 26.2%, respectively. The sensitivity of the NB model was high.
Performance metrics of six models.
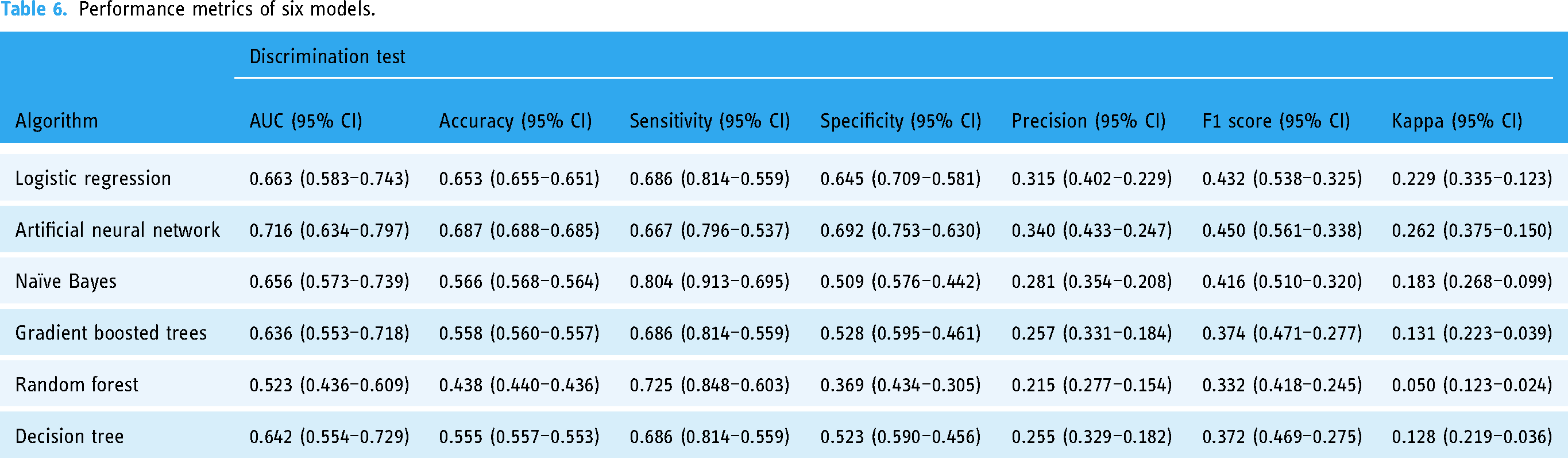
Figure 2 depicts a schematic of the ANN model. Figure 3 shows the receiver operating characteristic (ROC) curves of the six models applied to the validation set. Figure 4 show the precision-recall (PR) curves for the six models applied to the validation set, respectively. The calibration curves (Figure 5) show that the predictions agreed well with the observations, with the LR, ANN, NB, GBT, RF, and DT models achieving Brier scores of 0.153, 0.132, 0.177, 0.220, 0.160, and 0.143, respectively.

Schematic representation of ANN model.
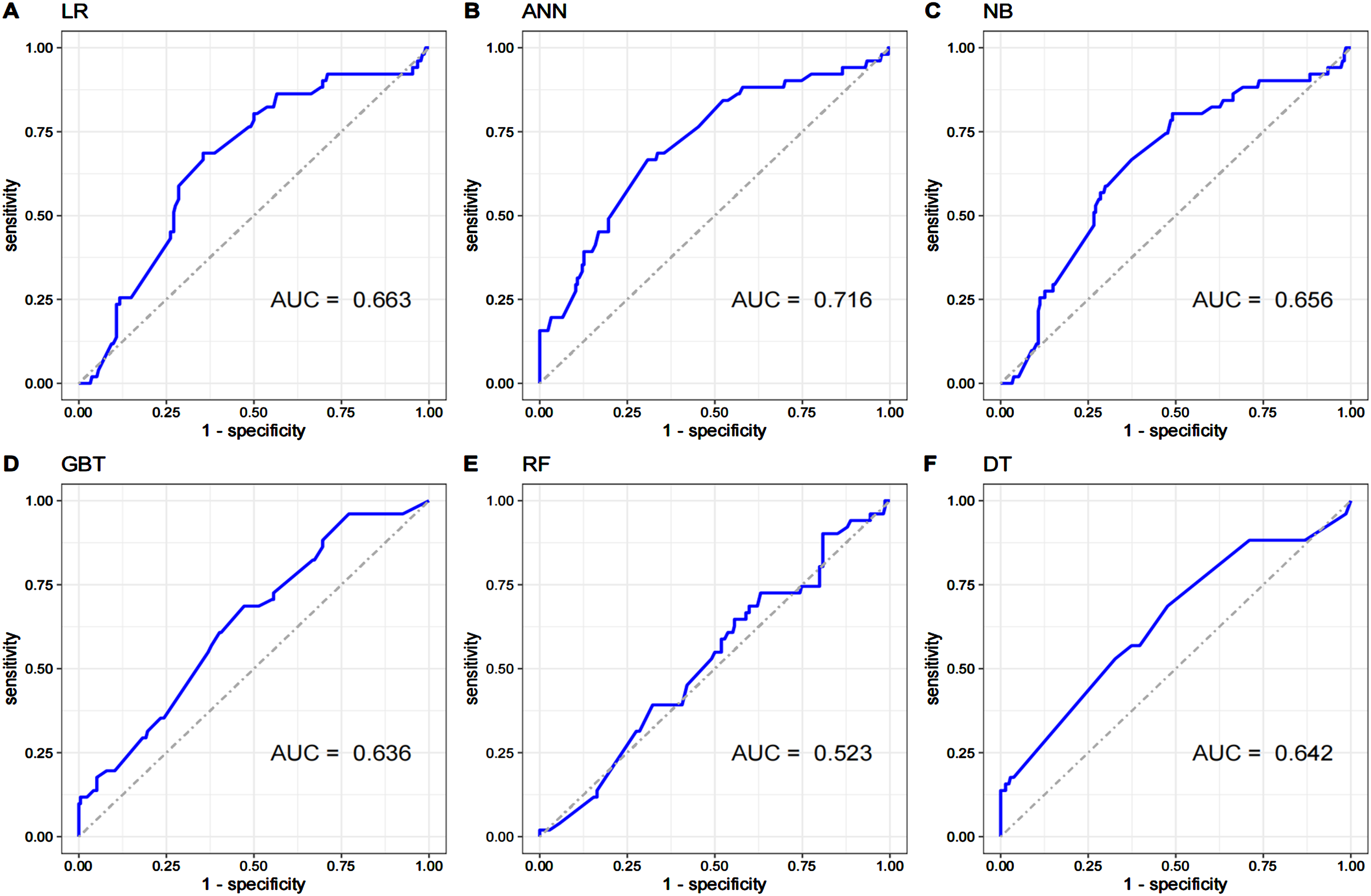
The ROC curves of six developed models.
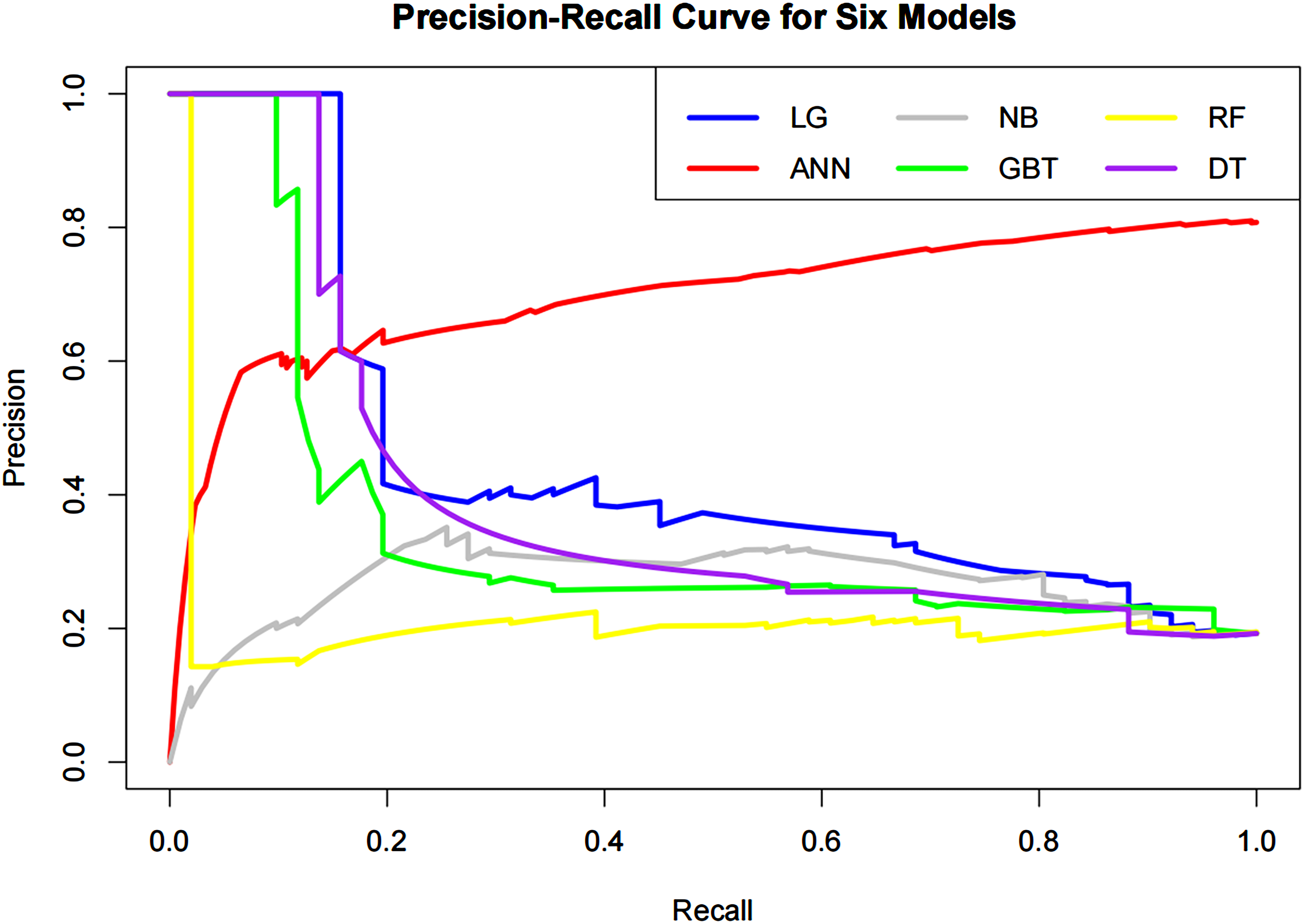
Precision-Recall curve of the six models developed.

Calibration curve and brier score of six developed models.
Discussion
Key findings
Our findings showed that more than 80% of the frontline medical staff had poor sleep quality. Many previous studies have found elevated rates of COVID-19-related sleep quality issues in the general population, with one study noting a 13.6% prevalence of COVID-19-related insomnia. 31 In another Chinese study of nearly 12,000 adolescents and young adults, the prevalence of insomnia symptoms was 23.2%. 32 This suggests that the impact of the public health emergency owing to the COVID-19 outbreak on the sleep quality of frontline health workers was stronger than on other populations. The possible reasons for this are as follows: During the rapid rise of confirmed cases in Shanghai, healthcare workers were on the frontline, in direct contact with positive patients, and were tasked difficult treatment and care, heavy work pressure, and higher risk of infection. Additionally, medical staff supporting nucleic acid sampling and testing was exposed to higher risk of infection. As were the senior medical staff who were not only responsible for coordinating care but also interacting more with critical patients; they also had more responsibilities. In addition, according to the results of a previous survey on the sleep quality of medical staff in Wuhan, the incidence of sleep problems was higher there among medical staff from other cities. 33
In this study, we compared the sleep quality scores of medical staff in different support positions and with different job titles and found the most significant variability in daytime dysfunction scores (p < 0.001). The worst mean sleep quality was found in those involved in nucleic acid sampling and testing and senior title medical staff. We speculate that the reason for the variability in daytime dysfunction may be the differences in the work environment and working hours. Additionally, long hours of intensive work, exposure to high levels of stress, and irregular work schedules, combined with being at the peak of a pandemic, exposed frontline health care workers to particularly demanding conditions that often deteriorated their mental health, likely contributing to the onset of poor sleep quality.34–36 Physical activity and sleep are highly correlated health behaviors. Our physical activity during the day (waking hours) affects the quality of our sleep, and vice versa. A 2015 study recommended “restoration of daytime functioning” as one of the basic outcome indicators for optimal treatment of insomnia, and improving daytime dysfunction is important to improve the sleep quality of medical staff. 37 To confirm whether sleep problems were associated with this history of medical care provision, we also compared detection rates and found that medical staff who had previously participated in public health emergencies had higher sleep quality than those who had not, suggesting that first-time involvement in medical assistance was an important reason for the occurrence of sleep problems. In addition, predictive models are gradually being applied to assess sleep quality. For example, Chen et al. developed the Sleep Quality Rapid Classification Scale to screen and group those with poor sleep quality using four main variables, including sleep quality, hypnotic drug use, sleep onset time, and lack of enthusiasm. 38 However, Chen et al.'s scale was designed specifically for older adults, and research tools applicable to medical professionals are still lacking.
Logistic regression, ANN, RF, GBT, NB, and DT are common modeling tools in biomedicine, and we developed and validated sleep quality prediction models using these tools with six readily available variables: senior associate title, tea consumption, and underlying illness, which are risk factors for poor sleep quality factors; and nurses, work shift, and weight gain, which are protective factors for sleep quality. The results were broadly similar to those of another study reporting that flexible-shift nurses obtained better outcomes in terms of sleep duration than day-shift and night-shift nurses. 39 Additionally, persistent insomnia is significantly associated with higher blood pressure variability, 40 and the theophylline in tea promotes attention wakefulness by inhibiting adenosine A1 receptors in the basal forebrain and inhibited sleep. 41 In addition, Yang et al. studied 463 young adult women aged 23 years, where PSQI >5 was found to be associated with a higher mean BMI. 42 The findings also pointed to an inverse relationship between sleep duration and BMI 43 and that sleep quality can affect BMI by altering metabolic parameters such as reduced glucose tolerance, 44 distorted oxygen-producing hormone levels, 45 and increased sympathetic nervous system activity. 46 These findings could help with the development of strategies to aid medical professionals to better adapt to high-intensity work.
Our results also show the strong predictive power of our fitted models, with ANN being the most effective, having AUC, accuracy, sensitivity, specificity, precision, F1 score, and kappa values of 71.6%, 68.7%, 66.7%, 69.2%, 34.0%, 45.0%, and 26.2%, respectively. In addition, it obtained a Brier score of 0.132. The calibration curve showed good agreement between prediction and observation.
Compared with the PR curve, we prefer to apply the ROC curve to evaluate the performance of the model. Previous studies have shown that these two curves should be selected with a consideration of prevalence and clinical scenarios. When the prevalence was less than 20%, especially less than 5%, the PR curve could be adopted. 47 However, the incidence rate of poor sleep quality in our study was about 75%, the ROC curve may be more applicable than the PR curve. And our results prove that our model is valid (AUC = 0.716, AUPR = 0.697, F1 = 0.450). In this study, the results of the prediction model are divided into good sleep quality and poor sleep quality. Poor sleep quality tends to cause fatigue, daytime dysfunction, and slow reaction, so it is more meaningful to implement early screening for the medical staff. The model we developed can be used as an effective preliminary screening tool.
In addition, compared with some predictive models from previous studies predicting sleep problems, as selecting the prediction OSA model with six features predicting AHI cutoff value of 30/h, the sensitivity and specificity of 70.26% and 70.30%, respectively. 48 The ANN model developed in this study has a similar specificity and sensitivity. In terms of the specificity, in the prediction models developed in 2020 and 2022, the specificity was 59% and 57%, respectively,21,49 lower than that in ANN model we developed. Because the specificity of the ANN model was higher than its sensitivity, the model we built has a strong ability to correctly identify high-quality sleep (true negative rate); in other words, the positive results in the prediction model with high specificity help us diagnosis sleep quality. The prediction model rarely produced positive results for frontline medical staff with normal sleep quality, where the presence of a positive result indicates a high probability of poor sleep quality.
The ANN model can enhance awareness of risk factors among frontline medical staff in Fujian Province and provide guidance to health authorities on supporting these workers. Specifically, healthcare professionals can utilize the model to predict their own sleep quality in similar scenarios, thus ensuring better sleep hygiene by mitigating identified high-risk factors. For instance, our predictive model highlights tea consumption during shifts as a significant predictor; adjusting tea intake could potentially improve sleep quality among frontline medical personnel. Furthermore, health authorities should implement strategies to safeguard healthcare workers’ sleep based on these predictions. In response to identified predictors, we propose six targeted recommendations: (1) Deploy additional personnel in roles where sleep quality is compromised, such as administrative duties. Subdivide tasks among medical staff to allow for more rest time, improve working conditions, and provide sleep hygiene guidance. (2) Medical staff facing high-pressure environments due to complex patient cases should benefit from multidisciplinary care approaches to alleviate individual workload. (3) Daytime responsibilities like nucleic acid testing could benefit from volunteer support organized by health departments to reduce medical staff workload. (4) Dietary adjustments should be implemented for medical staff by offering a variety of nutritious meal options to help them maintain adequate nutrition and achieve a healthy body weight. (5) Provide daily guidance during shifts to minimize tea consumption among medical staff and encourage regular rest and relaxation. (6) Modify the workload of medical staff dealing with routine cases by decreasing physical demands and increasing administrative tasks.
Additionally, we found that the RF model performed poorly on the validation set of the generated model (AUC value of 0.52), which is consistent with our prediction results because, in the questionnaire design, we artificially divided medical staff into multiple categories, and attributes with higher value divisions would more strongly impacted the RF algorithm. Therefore, the RF output of attribute weights on such data was not credible. Therefore, the ANN model is a promising tool for predicting the sleep quality of medical staff in Shanghai and can provide strong scientific guidance regarding the management of the sleep quality of frontline medical staff during the pandemic. As being a senior associate was determinants of poor sleep quality, future studies should focus on prospectively investigating the relationship between these roles and sleep quality, incorporating the results of long-term follow-up of study subjects into future studies to explore the impact after the pandemic in Shanghai.
Advantages and limitations
One of the strengths of this study is its representativeness. Our study population included 1326 frontline medical staff, covering over 80% of the frontline medical staff in Fujian Province who provided assistance in Shanghai between April and June 2022; moreover, the platform on which we released the questionnaire passed a rigorous system upgrade to ensure system accessibility, stability, data compatibility, and security, which makes our findings more reliable and representative and suitable for used as a reference for similar subsequent studies. New variables affecting sleep quality were innovatively proposed. Our results are the first to suggest some of the factors that influence sleep quality, such as job title, job type, and support position, which are likely to have important implications for health management and clinical practice. In addition, we build a prediction model based on ML algorithms, with good consistency between prediction and observation, which is consistent with the current healthcare situation, and can provide important and timely support for epidemic control. However, our study also has some limitations. First, this was a cross-sectional study, so the causal relationships between the variables are unknown.
Although we could analyze the associations between variables in this study, further research is needed to determine the causal relationships between sleep quality and various variables. These variables may also interact with each other. Second, the survey was a largely web-based self-report, which is subject to recall bias, subjective feeling interference, and personal expectation bias, resulting in the selection of individual options that do not reflect reality. Third, although our ML modeling appears to have strong predictive power, the results depend on the data used in development and validation, and external datasets for validation were lacking. If possible, external validation on frontline medical staff from Fujian Province in Shanghai would lead to a more trained predictive model. Fourth, this study adopted stratified sampling when studying the effects of different titles on the sleep situation of medical staff, which may lead to data imbalance in certain circumstances, so a standardized random sampling method is needed to minimize confounding factors. Finally, it is important to note that while the PSQI is a validated instrument for assessing sleep quality, the other questionnaires utilized in this study have not undergone formal validation. This lack of validation may impact the reliability and generalizability of the findings. Furthermore, although we conducted a preliminary assessment of these questionnaires, a comprehensive pilot test was not performed. Therefore, the potential for measurement errors and biases in the responses cannot be completely ruled out. Future research should focus on validating these instruments within the specific population of frontline medical staff to enhance the robustness of the findings.
Conclusions
Sufficient evidence in this study suggested that the sleep quality of frontline medical staff in Fujian Province in Shanghai was severely affected by the pandemic, with approximately 80.8% of medical staff reporting poor sleep quality. A total of six variables were found to be associated with sleep quality, including weight change, type of work, professional title, work shifts, tea drinking during assistance, and underlying illness. Improving the sleep quality of medical staff is important for maintaining a stable and healthy health care workforce, and the findings of this study will help policymakers focus on key populations and implement targeted measures to improve the overall sleep quality of medical staff. Among the models we developed and validated, the ANN model performed the best, and the application of ML technology enabled the prediction of sleep quality of medical staff involved in medical assistance work through several key variables that can be easily obtained, providing strong data and tools to support appropriate prevention and intervention strategies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241287363 - Supplemental material for Artificial neural network–based model for sleep quality prediction for frontline medical staff during major medical assistance
Supplemental material, sj-docx-1-dhj-10.1177_20552076241287363 for Artificial neural network–based model for sleep quality prediction for frontline medical staff during major medical assistance by Qingquan Chen, Zeshun Chen, Xi Zhu, Jiajing Zhuang, Ling Yao, Huaxian Zheng, Jiaxin Li, Tian Xia, Jiayi Lin, Jiewei Huang, Yifu Zeng, Chunmei Fan, Jimin Fan, Duanhong Song and Yixiang Zhang in DIGITAL HEALTH
Footnotes
Contributorship
Conceptualization, Chunmei Fan, Duanhong Song, and Yixiang Zhang; methodology, Yixiang Zhang and Duanhong Song; writing—original draft preparation, Zeshun Chen and Xi Zhu; writing—review and editing, Qingquan Chen and Jiajing Zhuang; validation, Qingquan Chen, Huaxian Zheng, and Jiaxin Li; formal analysis, Ling Yao, Tian Xia and Jiayi Lin; data curation, Jiewei Huang, Yifu Zeng, and Jimin Fan. All authors have read and agreed to the published version of the manuscript.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fujian Provincial Health and Family Planning Commission, China, Natural Science Foundation of Fujian Province, China, Quanzhou Science and Technology Project, China, (grant number 2021GG01010048, 2022J01792, 2021C061R).
Ethics approval and consent to participate
Ethical review in the data collection procedure was obtained from the Medical Ethics Committee of the Second Affiliated Hospital of Fujian Medical University, Sleep Medicine Key Laboratory of University in Fujian, and the Sleep Disorder Medicine Center of the Second Affiliated Hospital of Fujian Medical University (IRB No. 2021–309). The participants were informed of the purpose and confidentiality means of this anonymous research and were free to withdraw from the survey at any time without any reason. Responses to the questionnaire were considered as informed consent. Additionally, the PSQI questionnaire is publicly available and not restricted to specific groups or institutions. The use of the PSQI typically does not involve the collection of personal privacy or sensitive information, which means that special authorization is not required.
Informed consent
Informed consent was obtained from all subjects involved in the study.
Guarantor
YZ.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.