
Abstract
Persons with autism spectrum disorder (ASD) and/or intellectual disability (ID) have difficulties in planning, organising and coping with change, which impedes the learning of daily living skills (DLSs), social participation and self-management across different environmental settings. Assistive technologies (ATs) is a broad term encompassing devices and services designed to support individuals with disabilities, and if used in a self-controlled manner, they may contribute inclusion in all domains of participation. This comprehensive literature review aims to critically assess and unify existing research that investigates the use of assistive technology within the practical domain for individuals with ASD and/or ID. The 18 relevant studies included in this review highlighted the benefits of AT for social participation and independence in daily activities of individuals with ASD and/or ID. Professionals working with this target group should be knowledgeable of the speedy progress of AT products and the potential of persons with ASD and/or ID to use mainstream devices to meet their individual needs. This awareness provides an opportunity to advocate for the universal benefits of AT for everyone. Technologies such as virtual reality, mobile applications and interactive software have been shown to improve DLSs, communication and social interaction. These tools offer engaging, user-friendly platforms that address the specific needs of these individuals, enhancing their learning and independence.
Introduction
Initial problematisation
People with autism spectrum disorder (ASD) and those with intellectual disabilities (IDs) both face challenges in social participation.1–4 Studies indicate that this population has fewer social participation opportunities than typical developing peers. 5 In this context, the literature refers to participation in various aspects of daily life (e.g., education,6–9 social activities, spending time with family, friends10–12 and recreational activities11,13,14) and in several stages of life (childhood, adolescence and adulthood). This is in line with the barriers faced by individuals with ASD and ID due to the impairments associated with their diagnosis. According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 15 both ASD and ID are classified as neurodevelopmental disorders, meaning that the disorders typically manifest early in development and are characterised by developmental impairments leading to limitations in personal, social, academic or occupational functioning. Specifically, the ID-diagnosis includes deficits in intellectual and adaptive functioning in conceptual, social and practical domains. Without ongoing support, the adaptive deficits limit functioning in one or more activities of daily life, such as communication, social participation and independent living, across multiple environments (home, school, work, and community). Regarding the ASD-diagnosis, the DSM-5 refers to persistent deficits in both social communication and social interaction and restricted repetitive behaviours. Symptoms cause clinically significant impairment in social, occupational or other important areas of functioning. 15 Adaptive skills are typically below those for measured IQ, which applies to persons with ASD with and without ID. 16 Difficulties in planning, organising and coping with change negatively impact academic achievement, even for students with above-average intelligence. In adulthood, individuals with ASD face difficulties in independent living and gainful employment. 15
Common for ID and ASD is the impairment in individual adaptive functioning. Complying with a social-ecological view on disability, the level of functioning results from a dynamic interaction between a person's health conditions, personal factors and environmental factors. 17 Disability is not considered a characteristic of the individual but a problem of alignment between the person with functional limitations and abilities on the one hand and society on the other hand. 18 This way, the impact of the environment can be stimulating (enabling environment) or constraining (disabling environment), which may influence a person's full and effective participation in society on an equal basis with others. 19 Consequently, the emphasis shifts from a disorder or impairment in functioning to a need for support to perform activities and participate in society. 20 One of the enhancement strategies to address this need for support is the use of technology to strengthen cognitive, social and practical skills.17,21 This comprehensive literature review aims to assess and unify existing research that investigates the use of AT within the practical domain for individuals with ASD and/or ID.
The knowledge gained will benefit the development of methodologies for AT applications to accommodate and facilitate practical skills. Emphasis is placed on user-centred design principles, ensuring that the technologies are tailored to meet the unique needs of individuals with ASD and ID. It highlights the integration of various disciplines such as psychology, computer science and engineering in developing assistive technologies. The review identifies a lack of standardised metrics for evaluating the effectiveness of ATs for ASD and ID. It proposes a framework for consistent assessment, facilitating comparative studies and evidence-based practice, and the need for cost-effective solutions that are widely accessible, particularly in low-resource settings.
The review also addresses some existing gaps in the research – notable deficiency in longitudinal studies that assess the long-term impact of ATs; the gap in training and support for caregivers and professionals using these technologies; and the need for better integration of ATs within existing educational and therapeutic frameworks – and discusses strategies for seamless incorporation, ensuring that these tools complement and enhance the traditional approaches.22–24
This review makes significant contributions by thoroughly analysing current ATs for ASD and ID, highlighting novel advancements and addressing critical gaps in the research. Its comprehensive and interdisciplinary approach, coupled with practical recommendations, paves the way for future innovation and improved outcomes for individuals with ASD and ID. This knowledge will be beneficial in the development of targeted tools that accommodate the individuals’ needs for support in promoting practical skills.
Definition of the key concepts
Following the review aim, the four key concepts in relation to persons with ID and/or ASD are defined: (a) social participation, (b) adaptive functioning in the practical domain, (c) AT and (d) empowerment.
Social participation
Social participation refers to the involvement of individuals in activities and interactions within their community or society. It encompasses various forms of engagement, collaboration and contribution to a community’s social, cultural, political or economic aspects. Social participation is a crucial aspect of a person’s wellbeing and plays a significant role in building and sustaining a healthy, vibrant society. Participating in a diverse range of activities and experiences across life domains is central to the lives of all people, including people with ASD and ID.25,26
The World Health Organization (WHO) 18 defines participation as ‘involvement in a life situation, influenced by the environment’, which corresponds to the social model of disability. However, this definition focuses on the objective condition and does not adequately capture the subjective experience of involvement with others in society. Therefore, in research, the concept of social participation is frequently used. Notwithstanding the above, there is no single definition of social participation. Piškur et al. 27 identified three ways in which authors refer to social participation as a distinct entity: (a) as consumer participation (involvement in decision-making to increase wellbeing), (b) social activity (involvement in activities that provide interaction with others) and (c) levels of involvement in society (continuum from relatively passive to very active). Within the scope of this literature review, the term social participation is used as defined in the Quality of Life conceptual and measurement model, a widely used model in research with persons with ASD and ID as well.2,28–30 Social participation, besides independence and wellbeing, is one of the three higher-order factors that constitute this Quality of Life concept. Each factor reflects multiple domains. Social participation is related to the following three domains: (a) interpersonal relations (social networks, friendships, social activities, interactions and relationships), (b) social inclusion (community integration/participation, community roles and supports) and (c) rights (human – respect, dignity, equality, legal access and due process). 28 This description is largely consistent with the interpretation of social participation 27 as a social activity because of its focus on interpersonal relationships and social inclusion.
Adaptive functioning in the practical domain
Adaptive functioning refers to an individual’s ability to carry out everyday tasks necessary for self-sufficiency and independence. It refers to the person’s ability to meet community standards of personal independence and social responsibility compared to individuals of similar age and socio-cultural background. 15 It is often assessed across various domains, including the practical skills or DLSs domain. For individuals with ASD and ID, adaptive functioning in the practical domain can be particularly challenging. To meet the demands of their environments, each person must learn a set of conceptual, social and practical skills. As environments change (e.g., in place, in time), people must learn new skills to continue to meet the environmental demands. 31 Examples of conceptual skills are literacy, concepts of numbers, money and time. Social skills may include interpersonal skills, social responsibility, self-esteem and social problem-solving. Practical skills involve learning and self-management across life settings, including skills such as personal care (e.g., hygiene, eating, dressing and household tasks), job responsibilities, money management, recreation, self-management of behaviour and school and work task organisation.15,31–33 Thus, in both ASD and ID, a person-centred and individualised approach to adaptive functioning in the practical domain is crucial.
Assistive technology
AT refers to devices, tools, software or equipment designed to enhance the independence, functional capabilities and quality of life of individuals with disabilities. These technologies are intended to help people overcome limitations related to physical, cognitive, sensory or communication impairments. The WHO defines AT as ‘assistive products and related systems and services developed for people to maintain or improve functioning and thereby promote well-being’ 34 (e.g., wheelchairs, prosthetic devices, hearing aids, communication boards). 35 AT is an overarching term for products and related services used by persons with disabilities to enable and enhance their inclusion in all domains of participation. AT can be used by people of all ages, with all types of disabilities and all kinds of limitations in activities, for short or long periods. 36 AT can contribute to promoting access to education, employment, justice, health and wellbeing, as well as broader cross-cutting values of promoting social inclusion and participation, independence and autonomy, as well as leading a dignified and meaningful life. 37
In recent decades, besides specially developed products for people with disabilities, there has been an emerging trend on developing mainstream products accessible to a broader audience, including people with disabilities.35,36 There is an increasing focus on developing products according to the principles of Universal Design, Design for All, and Inclusive Design.38–40 Among other things, techniques mainly used in ATs are being integrated into mainstream technologies (e.g., text-to-speech, speech-to-text, augmentative and alternative communication, navigation support apps and eye-gaze technology).36,37 As such, mainstream technologies offer features that allow them to function as assistive products (e.g., smartphones, computers).35,41 An assistive product can consequently be described as any product, either specially designed and produced or generally available, whose primary purpose is to maintain or improve an individual's functioning and independence and thereby promote their wellbeing. 36 The field of AT continues to evolve, incorporating advancements in electronics, robotics and artificial intelligence to create innovative solutions that enhance accessibility and inclusion for individuals with disabilities. This technological evolution runs parallel to the paradigm shift from the medical model to the social-ecological model. While ATs have historically been developed to address the deficits of people with disabilities, there is a tendency to use ATs, and universally designed technologies in general, to support people to be active members of society.42,43 Currently, there is an emerging trend of using participatory methods in AT development and research.44,45 However, from a disability studies perspective, it is argued that research on AT is still mostly technical or therapeutic in nature and that the importance of AT deserves even more attention from social science disciplines. 42
Empowerment
It refers to the process of enabling individuals or communities gain control over their lives, make informed decisions, and take action to improve their wellbeing. It involves fostering a sense of self-efficacy, confidence and autonomy. Empowerment can manifest in various aspects of life, including personal, social, economic and political domains. The term empowerment originated in the last century and was a central theme of civil rights associations, striving to give all people a voice, including marginalised groups.46,47 Over time, the concept of empowerment has been explored in depth in multiple contexts and ecological levels: individual, organisational and community.48–50 Empowerment can be seen as an open-ended construct that can vary by context or person, have a different meaning for each person and evolve over time. 50 Definitions of empowerment differ depending on the level or context in which the term is used. A common element in the definitions across time is that empowerment is a process. According to Zimmerman and Warschausky, 51 empowerment can be defined as ‘processes and efforts that support people to gain control and influence of issues that concern them as well as to participate in decisions that affect their lives’. More recently, Haddad and Toney-Butler 52 defined empowerment as ‘the interpersonal process of providing the proper tools, resources, and environment to build, develop, and increase the ability and effectiveness of others to set and reach individual goals’. The WHO 53 defines empowerment as ‘the process by which people gain control over the factors and decisions that shape their lives. It is the process by which they increase their assets and attributes and build capacities to gain access, partners, networks, and/or a voice to gain control’.
Concerning the quality of life concept mentioned earlier in this introduction, empowerment is, besides skill development and involvement, one of the quality of life-related principles at the individual system level. Examples of enhancement strategies are decision-making, choice-making, risk-taking, goal-setting, self-advocacy and self-management. 17
Empowerment is a dynamic and multifaceted concept that recognises the importance of addressing various factors contributing to individuals’ ability to shape their lives. It plays a crucial role in fostering resilience, promoting social justice and building strong, vibrant communities.
Specific objectives and research questions
The specific objectives of the present review were (a) to systematically scrutinise and evaluate research studies delving into the applicability of ATs concerning adaptive behaviour within the practical domain for individuals with ASD and ID; (b) to gauge the influence of AT on the empowerment of individuals with ASD and ID, with a specific emphasis on its potential to promote self-management, independence and self-determination in daily activities and (c) to investigate the association between the utilisation of AT and the augmentation of social participation for individuals with ASD and ID. This encompasses its applicability and role in communication, community engagement and access to educational and vocational opportunities.
This analysis of the literature aims to answer the following three research questions: (a) What is the applicability of AT in facilitating behavioural adaptations related to practical skills in individuals with ASD and ID? (b) How does AT empower individuals with ASD and ID, enabling them to attain greater independence and make informed choices that contribute to their overall well-being? And (c) Does the incorporation of AT lead to improvements in social interactions, communication and participation within educational and occupational environments for individuals with ASD and ID?
Methods
We performed a methodological examination adhering to the PRISMA guidelines 54 (see PRISMA checklist, Supplementary File 1), encompassing peer-reviewed journal articles and full-text conference papers published in English from 2011 to 2021. Subsequent subsections explain the individual components of our approach in detail. The review was registered with PROSPERO (CRD42022350242). Briefly, we devised two sets of eligibility criteria, each applied at distinct stages of the review process. We employed a comprehensive approach for information retrieval, probing databases across various disciplines and adapting the search string for each database. The selection process encompassed nearly 3000 papers. The 18 studies selected for this review were reviewed for quality and analysed using thematic synthesis and variables selected to address the formulated research questions.
Eligibility criteria
The eligibility criteria set 1 was established to include any study that (a) evaluated the effectiveness of interventions using AT, either alone or in combination with other tools; (b) involved individuals who had been diagnosed with autism and/or with ID and directly used the AT being investigated; (c) had applied empirical research designs, which could be quantitative, qualitative or mixed-methods, in any type of setting and (d) the outcomes measured were the effect of the AT investigated on any learning skill (e.g., reading, dressing) and, in turn, on the empowerment and social participation of people with autism people and/or with ID. The definitions provided in the introduction were considered to assess empowerment and social participation. Both primary and secondary outcomes on empowerment and social participation were deemed appropriate for a study to be included in our systematic review. Any study that did not meet these criteria was excluded.
Once the target skills of the studies were manually identified and classified according to the three domains described in the introduction (i.e., conceptual, social and practical) and the articles focusing on practical skills, which are the focus of our work, were selected, the eligibility criteria set 2 was established to exclude (a) AT-mediated intervention studies that included people with ASD and/or with ID who also had a comorbid sensory-motor (e.g., visual, auditory or motor) disorder; (b) AT-mediated intervention studies aimed at parents, professionals, employers, etc., instead of individuals with ASD or people with ID; (c) surveys or interviews on individuals with ASD and/or with ID's perspectives with no direct interaction with AT; (d) studies on the development of AT for therapists to evaluate children's behaviour and (e) studies on the use of ATs to empower family members or professionals working with individuals with ASD and/ or with ID, and not to them directly.
Information sources
Our systematic search was designed to thoroughly gather relevant studies from the following scientific databases: Web of Science, ACM Digital Library, IEEE Xplore, Scopus, EBSCO, APA PsycInfo, PubMed, Embase, ASSIA, Medline (Pubmed), CINAHL Complete, Education Resources Information Center (ERIC), Google Scholar and Allied and Complementary Medicine Database (AMED). The selection of these databases was made to encompass a wide range of disciplines, including technology, education, psychology, medicine and allied health, among others. Google Scholar and AMED were used to capture grey literature and complementary sources, ensuring a comprehensive approach to information retrieval. 55
Search strategy
Our search strategy aimed to identify relevant studies by employing a systematic combination of keywords and controlled vocabulary terms. The Boolean operator “AND” was used to combine three concepts, and the Boolean operator “OR” was used to connect search terms within each concept. The search strategy included the following concepts and terms:
Concept 1. Intellectual Disability and autism-related terms: (“Intellectual* Disab*” OR “Intellectual* Impair*” OR “Intellectual* Retard*” OR “Intellectual* Handicap*” OR “Intellectual* Defici*” OR “Mental* Disab*” OR “Mental* Impair*” OR “Mental* Retard*” OR “Mental* Handicap*” OR “Mental* Defici*” OR “Learning Disabilit*” OR “Developmental Disorder” OR Autis* OR “Autism Spectrum Disorder” OR “Autism Spectrum Condition” OR “Asperger* Syndrome” OR “Pervasive Developmental Disorder”) AND Concept 2. Assistive Technologies related terms: (Technolog* OR Digital OR “Internet of Things” OR Computer OR “Electronic device” OR “Speech Generating Device” OR Wearable OR Smartphone OR iPhone OR Smartwatch OR iWatch OR “Mobile phone” OR Tablet OR iPad OR iPod OR Robot OR “Virtual Reality” OR “Augmented Reality” OR “Eye tracking” OR “Smart Glasses” OR “Artificial Intelligence” OR “Global Positioning System”) AND Concept 3. Empowerment and Inclusion: (empowerment OR inclusion)
Concepts 1 and 2 had to appear in the title, the abstract or the keywords, and Concept 3 could appear in any section of the article. The search string was adapted for each database to ensure compatibility with their specific requirements, ensuring a comprehensive retrieval of relevant literature.
Selection process
The flowchart in Figure 1 illustrates the selection process used for the final sample. The identification phase was conducted by implementing the search strategy to locate and retrieve data from the information sources. The results obtained through the 14 databases used (n = 2909) were transferred to Rayyan (https://www.rayyan.ai), an artificial intelligence tool to collaboratively work on systematic reviews, which facilitated the process of removing duplicates (n = 1350). During the first part of the screening phase, the eligibility criteria set 1 were applied focusing exclusively on titles and abstracts. Then, 197 full-text papers were retrieved and assessed for eligibility according to the same set of criteria. As a result, 96 papers were excluded. The remaining 101 papers were then classified according to the three domains described in the introduction section: 72 papers focused on conceptual and/or social skills, and 29 papers focused on abilities, which included at least one practical skill. Given that this paper focused on practical skills, as described in the introduction, the corresponding 29 full-text papers were reassessed with the eligibility criteria set 2. After excluding 11 papers for not meeting these criteria, 18 studies were finally included in our systematic review.

The selection process following the PRISMA 2020 updated guideline for reporting systematic reviews. 54
Data retrieval
The 18 selected papers were thoroughly examined, and data were extracted for the following variables: (a) author(s) name(s) of the article, (b) year in which the article was published, (c) journal or conference title in which the article was published, (d) characteristics of the participants included in the study (i.e., number, sex, age and diagnoses), (e) technology used (i.e., hardware (HW), software (SW) and its availability for the public), (f) which specific practical skill was targeted in the study, (g) research design applied, (h) characteristics of the intervention (i.e., length and intensity of the sessions, who implemented the study sessions and the setting in which the intervention took place and the country in which the intervention was implemented) and (i) the results obtained in the study about the effect of the intervention on both the practical skill(s) targeted and the social inclusion and/or empowerment of the participants included. These variables were selected to respond to the formulated research questions and allow us to discuss the matter reviewed thoroughly.
Quality assessment of the studies
All studies that met the eligibility criteria were reviewed for quality using the Critical Appraisal Skills Program (CASP) (see Tables 1 and 2). To ensure objectivity in the quality review, CASP reviews were first carried out individually, independently of each other, by three co-authors (ZP, KF and TØ). Then, each other's reviews were compared and discussed until a consensus was reached (ZP, KF and TØ). CASP assessment ranges from 0 to 10 for studies with qualitative design and for other designs from 0 to 12. Studies with 10 and 12 points are considered being of high quality. Studies with a quality assessment below 10 points were excluded to ensure validity and reliability. Meanwhile, none was excluded after the CASP assessment.
CASP assessment of included studies with qualitative design.

Note. CASP Checklist (Yes = 1; Can't tell = X; No = 0).
CASP examination of pilot and intervention and feasibility studies.
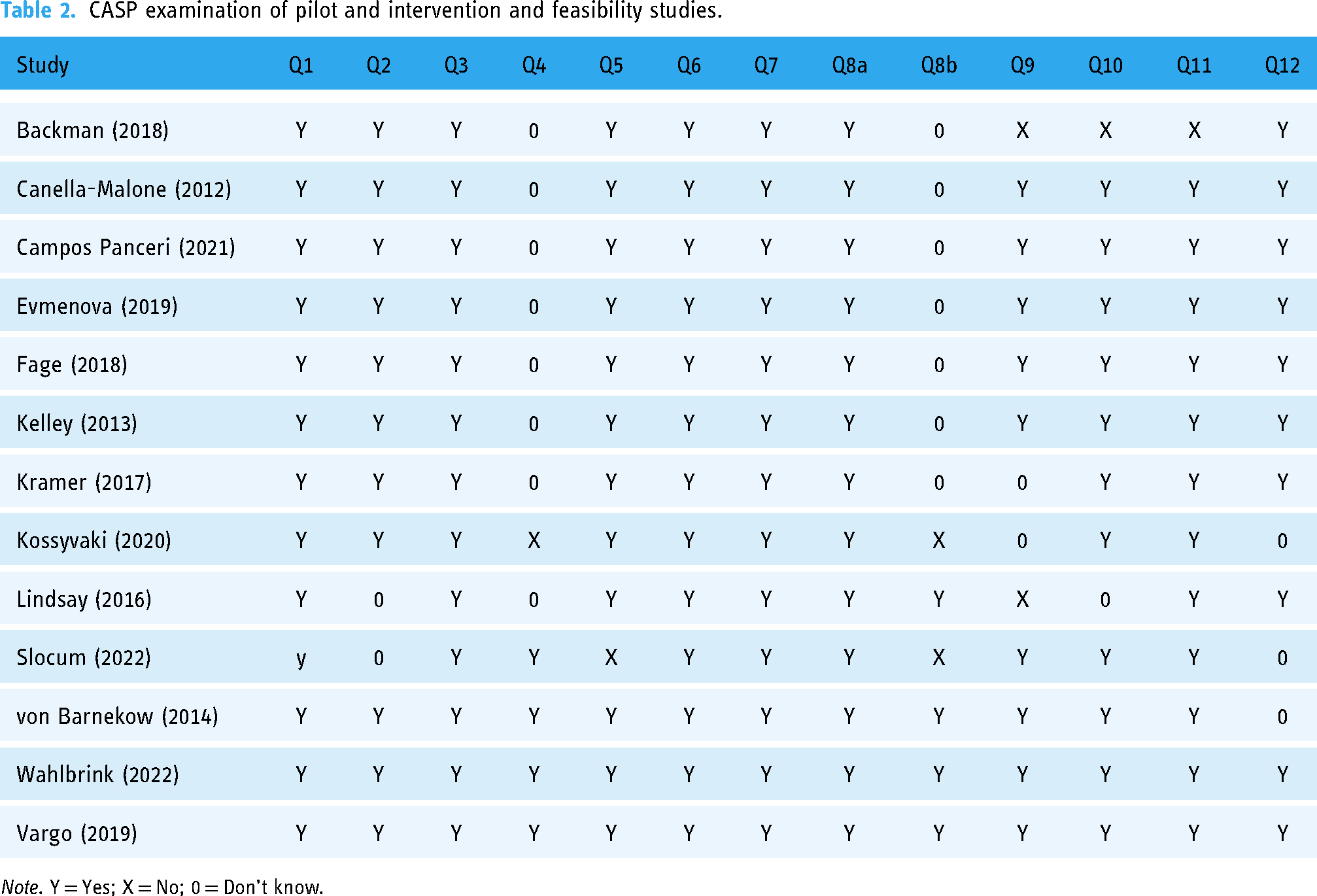
Note. Y = Yes; X = No; 0 = Don’t know.
Data synthesis and analyses
To synthesise and analyse the data, studies were subdivided by the type of technology used and practical skill assessed. The narrative summary was used to discuss the experience of AT use for persons with ASD and/or with IDs in the practical domain. Thematic synthesis, as outlined by Thomas and Harden, 56 was employed for data analysis. This included extracting primary themes and subthemes from the studies included in the analysis. The focus of the discussions was limited to AT, specifically related to the practical domain.
Results
Study characteristics
Study characteristics are summarised in Table 3. The research described in the articles was conducted in different countries and continents. Seven studies were carried out in the United States (#1, 2, 5, 6, 11, 13 and17), two in France (#12 and16), and two in Great Britain (#15 and 18). One each was carried out in Norway (#3), Saudi Arabia (#4), Australia (#7), Canada (#8), Spain (#9), Brazil (#10) and Sweden (#14). Such international diversity reflects a global interest in understanding and implementing ATs for individuals with ASD and IDs in the analysed period.
Characteristics of participants, design, independent variables and assistive technologies in included studies.

*Tier A = Digital Health Technologies that do not demonstrate measurable patient outcomes but provides services to the health and social care professionals; Tier B = Digital Health Technologies that provide information, resources or activities to the public, patients or health care professionals about a condition or general health and lifestyle; Tier C = Interventions to facilitate preventive behaviour change, self-management, treatment active monitoring, calculations that impact treatment, diagnose conditions. 75
No specific and global methodological trend emerged from the analysed papers. On the contrary, significant variation was observed in terms of research design. In the context of studies with small research samples, case studies dominated. In contrast, in the case of larger research samples, the research often had the character of an experiment with an intervention. However, it was rarely an experiment controlled by a control group. Moreover, many projects concluded the effects based on qualitative data, e.g., interview based. There were also mixed approaches in which the effects were diagnosed based on qualitative and quantitative data. Focus groups (with relatively small research samples) were also organised in several cases. It should be emphasised that there has yet to be a study with an identical methodology or any study in which previous procedures were replicated. Moreover, 22% were marked as a pilot study, i.e., one in which the sample needs to be bigger or there are no differentiated measurements and control conditions. All these studies are, therefore, complicated to compare and it is even more challenging to build convergent knowledge from them. Consequently, it is impossible to point out the statistics here (in the methodological area of analysis). Combining these observations with the differences in age and disability of the participants, we can see that there is a great need to standardise procedures and emphasise on the publication of the definitive outcomes, presenting both the results of the pilot and the final research, with a detailed description of the participants and much larger groups representing the tested developmental disorder.
Setting and participants
The final research samples varied greatly in size. The average sample size was 17 people, but the standard deviation was as high as 16. In two studies, N was only 3. The largest N (two studies) was 48 (originally N = 50, but two participants were not included in the final analysis). The samples exhibited diversity also in terms of gender. For instance, some studies focused on males exclusively,57–61,69,71–73 while others included a mix of males and females.63–66,68,70 The age range was also diverse, ranging from children to adults, covering a broad spectrum of developmental stages. Most (nearly half) of the studies focused on teenagers, with an average age of 15, and the fewest studies focused exclusively on adults (only one study: 18–26 years) or only on children (two studies: 4–9 and 5–7 years). The second most common sample structure was a mix of teenagers and young adults (e.g., 14–22 or 16–25). There was also a structure, such as a mix of children and teenagers (e.g., 6–13 years old). The youngest participants were 4-year-olds, and the oldest were 26-year-olds. In two studies, it was impossible to determine the participants’ age.
Most studies (39%) focused on people with ID. About 22% referred to individuals with ASD. Other papers included participants with diverse conditions, showing a comprehensive approach to intellectual disabilities. To be precise, 28% referred to ASD and ID, 6% (one study) to ASD and Down syndrome, 66 and another one to ASD, ID and Down syndrome. 61 Only some studies (less than one-fourth) specified (or considered in analyses) the severity, such as mild or moderate ID, which is an essential problem because including different severity levels and conditions contributes to a richer understanding of how ATs can cater to various needs. 1
Settings ranged from public schools (Studies #1, 9, 11, 12, 15, 16, 17 and 18), university campuses (#2 and 7), sheltered workplaces (#3), home environments (#5 and 13), health care centres (#8 and14) and community locations (e.g., Starbucks) (#4, 6 and 10). The choice of diverse study locations ensured contextual relevance and practical insights into the implementation of ATs.
Major findings
Upon examining the outcomes of this review, the Evidence Standards Framework for Digital Health Technologies was adopted. 75 As shown in Table 4, it is evident that no Tier A studies were found in our review. Most identified studies were categorised as Tier B (n = 14), while the remaining were classified as Tier C (n = 4). This allows us to categorise AT solutions into levels and summarise their types. Tire B primarily focuses on solutions based on computers, smartphones and tablet computers. However, there may be instances where alternative hardware solutions, such as earbuds or socially assistive robots, are also included. For example, Kossyvaki and Curran 71 implemented special hardware with six switches which provide auditory (i.e., sounds and music) and visual cues (i.e., multicoloured lights), demonstrating positive outcomes of engagement levels and social communication skills of 5–7 years old children with autism and ID at school (#15). Four studies (#3, 4, 6 and 13) used smartphones and phone applications to improve communication in the community and foster social inclusion by increasing independence in using public transportation. Wass and Safari 59 concluded that photovoice facilitated the understanding of the individual and contextual experiences of participants with ID and that they could make decisions according to their preferences. Alanazi 60 presented results of the focus group demonstrating strong support for using the Careem and Uber apps to enhance the confidence of persons with ID in navigating various locations. Additionally, this study's findings suggested that these apps are gaining popularity among individuals with ID as they progress in the learning process on how to use them. Wahlbrink et al. 62 reported that using the Apple iPhone 6s equipped with the List Recorder application demonstrated improved interpersonal DLSs and effectively used the mobile device as a prompting system for three participants with ASD. The observed generalisation of effects indicates that the participants’ behaviours continued to show improvement even after the intervention. Kramer et al. 69 reported that individuals with ID, serving as both peer mentors and mentees, can effectively engage in structured mentoring relationships through phone calls and video chats.
Summary of the interventions, results, and impact on inclusion and wellbeing.

Computer- or tablet-based applications were implemented in four studies (#1, 5, 7 and 16). According to Vargo and Brown, technology-enhanced Good Behaviour Games (GBGs), namely ClassDoJo GBG, led to reductions in disruptive behaviours in high school students with ASD. 57 Slocum and Ault demonstrated that the use of video modelling (VM) in combination with the system of least prompts (SLPs) was effective in teaching three individually selected behaviours to three individuals with ID and ASD for participation in a faith community. 61 iPads were used to support researchers with ID to improve their research skills and contribute to their social lives. Fage et al. showed that the ‘School+’ applications empowered individuals with ASD, enabling them to enhance their socio-cognitive functioning. 72 Two studies (#8 and 10) implemented robotic technologies. Lindsay and Hounsell examined the development of an adapted robotics program, suggesting positive effects on social interactions, communication and participation within educational environments. 64 Panceri et al. introduced a socially assistive robot with integrated serious games, emphasising encouraging results in child–robot interactions and social engagement. 66 Both studies involved young children (age 4–13 years) with ASD, Down syndrome and other IDs.
One study used gamified vocational training simulation (#9) to demonstrate positive outcomes, as users recognised real-life scenarios and attempted to apply what they had learnt. 65
The study of Evmenova et al. (#11) presented stakeholders’ feedback, including young adults (18–27 years) with ASD and ID, on the technology prototype (application for the smartwatch) usability to facilitate learning and self-regulated behaviours in academic inclusive postsecondary education (IPSE). 67
Tier C studies (#12, 14, 17 and 18) primarily addressed software solutions (phone apps, video chat and mobile applications). All studies discussed the improvement of social and life skills of persons with ASD and ID. Three out of four studies aimed to promote the use of assistive technologies in education settings. A study by Fage et al. assessed the impact of a tablet-based application on social interactions and socio-adaptive behaviours, suggesting positive effects in the mainstream classroom for children with ASD and ID. 68 Also, parents reported high usability, indicating that the applications were well-received in daily life environments. Cannella-Malone et al. directly addressed the incorporation of AT (video prompting with an iPod Touch) leading to improvements in skill acquisition (sweeping and table washing), with implications for communication and participation in individuals with moderate to profound ID. 73 Smartphone technology fosters the development of social and life skills and independence of children with ASD and thus promotes their inclusion in mainstream settings. 74 The study by Backman et al. was implemented by the Internet Habilitation Unit, Habilitation & Health at the municipality council in Stockholm (Sweden), demonstrating that internet-delivered coach-guided psychoeducational intervention, Spectrum Computerized PsychoEducation (SCOPE), was feasible to increase knowledge of ASD and themselves. 70
Next is the summary of study outcomes related to each research question from the data extracted.
Ten studies demonstrated the applicability of AT to benefit behaviour adaptations related to practical skill outcomes in individuals with ASD and ID. Three studies (#2, 3 and 4) aimed to improve independent use of transportation and travel to novel locations. The study outcomes indicated positive results across interventions. For example, 15- to 30-min intervention sessions four to five times a week, implementing video iPod training, improved independent travel skills for young adults with ID. 58 Furthermore, the practical skills needed for independent travel were demonstrated in two qualitative studies implementing photovoice 59 and smartphone apps, such as Uber and Careeem, 60 for young adults with moderate to severe ID. ATs have been shown to contribute to behavioural adaptations across different environments (schools, public sites, faith communities and homes). For example, in Vargo and Brown, the daily use (40 min of math session) of technology-enhanced GBGs was shown to lead to reductions in disruptive behaviours in high school students with ASD. 57 von Barnekow et al. demonstrated the applicability of 3D-gamified simulations as vocational training tools for adolescents with ID to learn practical skills related to hostel cleaning. 65 In Fage et al., a technology-based system (CS+) for children with ASD significantly increased socio-adaptive behaviours in both classroom and verbal communication, while improvements among children with ID were only established during non-verbal classroom routines. 72 VM on iPad combined with SLPs effectively taught three individually selected behaviours to individuals with ID and ASD for participation at home and in faith communities in the United States. 61 Similarly, in home environments, phone or video chat technology (e.g., Skype) was effectively used for structured mentoring relationships through electronic communication for individuals with ID serving as both peer mentors and mentees. 69 An Apple iPhone equipped with the List Recorder application demonstrated improvement in interpersonal DLSs and effectively used the mobile device as a prompting system for individuals with ASD in public places (e.g., Dunkin Donuts, Starbucks). 62
Transportation and navigation were among the most notable domains where using AT was particularly beneficial. Specifically, three studies highlighted that AT, mainly through picture prompts on iPod, 58 photovoice 59 and using the Careem and Uber apps, can increase travel independence in individuals with ID to enable participation in activities outside the home. In addition, other studies showed that AT may enable people with ID and ASD to be independently involved in activities across different environments, for example, in church 61 and educational settings.65,72 Also, AT can empower individuals with ID enabling them to serve as peer mentors. 69 Regardless of the domain where AT was used, enhancing the empowerment of individuals with ID and ASD appeared to be closely linked to respecting their needs and desires, thus strengthening their capacity for independent decision-making, providing opportunities for them to take responsibility over their lives and fostering their active social participation.
Fifteen studies showed that AT can improve the social interactions of individuals with ID and ASD, contributing to the development of their communication skills with friends, colleagues at work locations and community members (e.g., at faith community), and enhance their social life.57,60–62,64–74 For example, the use of robotic programs enhanced the ability to understand and participate in scientific activities 64 and therapy sessions 66 promoting social interactions. AT can be used to improve the ability to learn new life skills, for example, sweeping and table washing following video prompting in individuals with severe and profound ID, 73 cooking, attending the dentist, using public transport by using mobile phones in school-age children with ASD, 74 purchasing meals following recorded audio messages on mobile phone 62 and performing occupational skills by using 3D gamified simulations. 65 The research evidence demonstrated beneficial effects in decreasing social isolation among individuals with ID and ASD.60,61,67,68
Discussion
This comprehensive literature review aimed to assess and unify existing research that investigates the use of AT within the practical domain for individuals with ASD and/or with ID. The analysis of the literature led to answering the three predetermined research questions. Despite the limited number of publications, evidence could be demonstrated through various studies for each research question. This systematic review included 18 studies addressing the use of AT contributing to social participation and community engagement of individuals with ASD and/or with ID.
Overall, empirical evidence indicates that interventions employing AT are potentially beneficial in enhancing engagement levels in the educational processes (e.g., reduction of disruptive behaviours, improvement of socio-cognitive functioning), improving social communication skills (e.g., joint attention, social interaction), increased independence in using public services (e.g., public or commercial transportation, shopping and church), learning vocational skills (e.g., cleaning services) and fostering social inclusion.
The complexity of the practical domain has resulted in the application of various research designs across the selected studies. The criteria for evidence of effective practices have been established to guide researchers in following the quality indicators for selected research designs. 76 Only four of the selected studies met all the quality indicators and can be defined as high-quality research designs.
This literature review broadly used the term ‘assistive technology’. Both technologies designed specifically for the target group and mainstream technologies were included. This reflects the growing trend towards universal design, where mainstream products become accessible to a broader audience, including people with disabilities.35,36 Most of the studies used mainstream smartphones, computers or tablet computers. A few studies included alternative hardware solutions such as earbuds, 62 switches with visual and auditory cues 71 or socially assistive robots.64,66 In terms of software, both commercial and bespoke software were used (e.g., iMovie, 61 Classroom Schedule+ 72 ). Mainstream software was also used to develop specific applications (e.g., PowerPoint 58 ). This review echoes previous reviews demonstrating a noticeable transition in the nature of AT over the past decade, replacing handheld computers with portable electronic devices like iPods, iPads and smartphone applications.77,78 The shift towards more advanced technology is evident throughout the studies in this review. For instance, video prompts are provided on iPods and iPads, and navigation instructions are provided on smartphone apps. The trend of using portable electronic devices as ATs has contributed to removing social boundaries between mainstream technology and AT, as many individuals without disabilities use smartphones daily. 79 Moreover, when individuals with ASD and/or ID perceive AT positively rather than as a tool to mitigate disability-related challenges, it can promote social participation and a sense of belonging in the community. 80 Overall, the variety of target behaviours and skills to which AT was used throughout the reviewed studies illustrates the strong potential that these technologies can play in supporting individuals with ASD and/or ID across different settings and life situations.
As the first research question focused on studies that aimed to strengthen the adaptive skills of people with ASD and/or ID in the practical domain,15,31 results are described as outcomes on DLSs across different environments (e.g., independent travel, 58 vocational training, 65 interpersonal DLSs 61 ). Applications were also used as a prompting system for learning and self-management across life settings.61,73 This ties in with the second research question concerning the impact of AT on empowering individuals with ASD and/or ID. The included studies showed that AT could be seen as a tool to build, develop and increase the ability of people with ASD and/or ID to set and reach individual goals (e.g., independent involvement in multiple environments). 79
With 15 out of 18 studies showing that AT can improve social interactions in people with ASD and/or ID (e.g., contribution to communication skills in several environments 71 and participation in social life 62 ), the third research question was also positively addressed. This is significant given that people with ASD and/or ID often face challenges in social participation.1,4,5 Not least because social participation can be seen as a crucial aspect of a person's well-being. These studies collectively underscore the diverse ways in which AT positively impacts social participation, communication and inclusion within educational, occupational and different community environments.
This review provides practitioners and policymakers with numerous recommendations on how to maximise the benefits of AT for persons with ASD and/or ID. First, educators, therapists, trainers and assistant personnel should learn to use AT in various social environments and settings as part of their professional development. For example, integrating AT in implementing individual education plans can be essential to support inclusive education practices. 81 Second, partnerships between special schools, social care institutions or NGOs and information technology companies should be encouraged to generate user-friendly and cost-effective solutions that address the needs of people with ASD and/or ID.
Finally, it is vital to design and implement national and international policies requiring the incorporation of AT in public services and educational institutions, for example, free Wi-Fi access, accessible and user-friendly infrastructure (e.g., ticket machines for public transportation). Furthermore, improving public space infrastructure to facilitate AT use is important, such as establishing Wi-Fi in public locations and ensuring that public service systems are compatible with various AT devices.82,83
Limitations
Despite the positive results, some critical comments on the limitations of this review should be made. First, the wide variation in study designs and the number of participants involved made it difficult to compare studies and build convergent knowledge. Moreover, one-fifth of the studies were pilot studies, demonstrating only preliminary results. The second limitation of the reviewed studies is that six of the 18 studies did not mention whether or not the software was commercially or publicly available. Four other studies definitively used a prototype. Third, there was the heterogeneity of the participants across the reviewed studies. In addition to the difference in the age range, there was also a difference in the participants’ adaptive functioning levels. Since an individual's level of adaptive functioning is the result of the person's health status, personal factors and environmental factors,17,18 this varies for each individual. Although some studies specified the severity of ID (e.g., mild or moderate ID), there was little to no consistency in the way the adaptive functioning of the participants was described. A more accurate characterisation of the participants would provide more insights into the use of AT in relation to the various support needs of the target group.
Finally, this review consists only of studies published in the English language. Thus, some relevant studies published in other languages might be overlooked. These limitations highlight the need for ongoing research, personalised approaches and better access to resources to optimise the use of AT for skill development in this population.
Relevance of studies
Despite the limitations, the reviewed studies are replicable in different vocational, educational or community settings. While many studies evaluating the applicability of AT were in the development phase, the simple research designs enabled teachers, vocational skill trainers or other professionals to obtain pre- and post-intervention data across various environments. Most of the interventions implied a limited number of tasks or steps, simplifying the data collection process. Overall, the review outcomes are promising: most of the AT solutions used in studies led to positive outcomes in facilitating the independence of people with ASD and/or ID in performing relevant daily activities and increasing their independence.
Recommendations for future research
This systematic review has identified important directions for future research and potential ways in which ATs should be considered and can be integrated to enable individuals with ASD and/ or ID to accomplish practical tasks of daily life, enhancing their social participation. Additionally, this review highlighted challenges encountered in prior research, providing valuable feedback for prospective investigations. Future research should implement interventions that consider the affordances of the applied ATs, conduct comprehensive evaluations of research designs and incorporate one or more components related to the technology quality indicator. Emphasis should be placed on the exploration of mainstream technologies and service models offering features that allow their use as assistive products to enhance the social inclusion and participation of individuals with ASD and/or ID. It is important to be meticulous about technological advances and harness their potential for empowering individuals with ASD and/or ID. On the other hand, previous studies have also proved that specifically designed applications for people with disabilities inspire the universal design of products that most people can use. Therefore, future interventions should include target groups and service models identified and explored in previous feasibility or pilot studies described in this review. It is recommended that people with ID and/or ASD, as experts by experience, should be even more directly involved in the research and development of (assistive) technologies. To this end, participatory development and research methods are appropriate.
Conclusions
In conclusion, this systematic review highlighted the benefits of AT for social participation and independence in the daily activities of individuals with ASD and/or ID. Professionals working with this target group should be knowledgeable of the speedy progress of AT products and the potential of persons with ASD and/or ID to use mainstream devices to meet their individual needs. In turn, this provides an opportunity to advocate for the universal advantages of ATs for all.
This systematic review on the use of AT to promote practical skills in individuals with ASD and/ or ID reveals promising outcomes. Technologies such as virtual reality, mobile applications, and interactive software have been shown to improve DLSs, communication and social interaction. These tools offer engaging, user-friendly platforms that cater to the specific needs of these individuals, enhancing their learning and independence. The review highlights the importance of integrating technology into educational and therapeutic practices to support skill development in this population. Also, this review addresses researchers from underrepresented communities, particularly those with direct experience with persons having intellectual challenges or psychosocial disabilities. This overview extends to voices of disability rights activists or leaders of grassroots initiatives whose contributions are vital for fostering an inclusive discourse.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241281260 - Supplemental material for The use of assistive technology to promote practical skills in persons with autism spectrum disorder and intellectual disabilities: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076241281260 for The use of assistive technology to promote practical skills in persons with autism spectrum disorder and intellectual disabilities: A systematic review by Aija Klavina, Patricia Pérez-Fuster, Jo Daems, Cecilie Nørby Lyhne, Eglantina Dervishi, Zada Pajalic, Tone Øderud, Kristin S Fuglerud, Silvana Markovska-Simoska, Tomasz Przybyla, Michal Klichowski, Gregor Stiglic, Egija Laganovska, Soraia M Alarcão, Alan H Tkaczyk and Carla Sousa in DIGITAL HEALTH
Footnotes
Acknowledgments
This article or publication is based upon the work from the COST Action a-STEP: advancing Social Inclusion through Technology and EmPowerment–CA19104 (https://www.a-step-action.eu), supported by COST (European Cooperation in Science and Technology; ![]() ).
).
Contributorship
PPF, AHT, and CS designed the review, performed literature searches and documented the search results. ED, JD, GS, SMS, TP, MK, CNL and EL screened articles, extracted and analysed the data. The risk of bias was verified independently by ZP, TØ, SMA and KSF. AK drafted the manuscript with input from all authors. All authors contributed to the study conceptualisation, scientific discussions and manuscript review, and all have accepted the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical Approval
This paper is a systematic review that does not need approval from the ethics committee or institutional review board.
Funding
Guarantor
AK.
Informed Consent
Informed consent was not required as no personal data were processed in the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.