
Abstract
Introduction
Cataract remains a prevalent cause of visual impairment among the elderly, significantly increasing the risk of falls due to compromised visual function. Cataract removal surgery has been established as a means to enhance visual acuity and balance control. The advent of novel technologies, such as accelerometers integrated into smartphones, provides an opportunity to assess static balance control. We compared static balance measurements obtained from accelerometer built-in smartphones before and after cataract removal surgery.
Methods
Our sample comprised 29 individuals diagnosed with bilateral cataracts scheduled for cataract removal surgery. We evaluated participants’ visual acuity and recorded their body oscillations using the smartphone's embedded accelerometer during static balance maintenance, both with eyes open and closed, before and after surgery. We compared quantitative parameters of static balance evaluation at both time points.
Results
A significant improvement in visual acuity following cataract removal surgery was observed. Moreover, under open-eye conditions, all quantitative parameters of static balance evaluation exhibited significant improvement, with only one parameter showing improvement under closed-eye conditions.
Conclusion
Inertial sensors integrated into smartphones serve as practical tools for monitoring changes in static balance control resulting from cataracts, as well as for evaluating balance recovery after lens extraction surgery.
Introduction
Cataracts constitute a global public health concern that significantly affects the quality of life, particularly for those aged 50 and above. 1 The standard treatment for cataracts involves surgical removal of the affected lens, which typically yields a positive prognosis for visual recovery and improved quality of life. 2
Several studies have examined the impact of cataracts on balance control in older adults and have demonstrated a decline in balance control that can be improved with cataract surgery.3,4 Force platforms considered the gold standard for balance evaluation are expensive and may not be readily accessible, particularly in impoverished and developing countries. Therefore, there is a need for alternative approaches that offer better cost-effectiveness than force platforms and high accuracy for balance assessment in diverse settings.
In recent years, inertial sensors have emerged as a cost-effective alternative for evaluating static balance control across various populations and health conditions and they have demonstrated validity when compared to gold-standard methods for assessing balance control, such as force platforms. 5
The objective of this study is to compare balance control before and after cataract removal using the built-in accelerometer in smartphones. We hypothesize that the smartphone's integrated accelerometer will effectively detect the expected improvement in balance control following cataract surgery.
Methods
Ethical considerations
The present study was designed as a pre–post study to investigate balance changes after cataract removal. The present investigation adhered to the Declaration of Helsinki of 1964 and all procedures were approved by the Ethical Committee for Research with Humans of the Federal University of Pará (report no. 5.264.473). Informed written consent was obtained from all participants.
Participants
The study sample of patients with cataracts comprised 29 participants ranging in age from 55 to 75 years old, including 23 females and six males, all of whom had been diagnosed with cataracts and were referred for cataract surgery by an ophthalmologist. All participants had no clinical history of neurological or other degenerative diseases, and no other ocular diseases were reported. A sample of participants without a diagnosis of cataracts was used as a control group (n = 26).
Experimental and clinical procedures
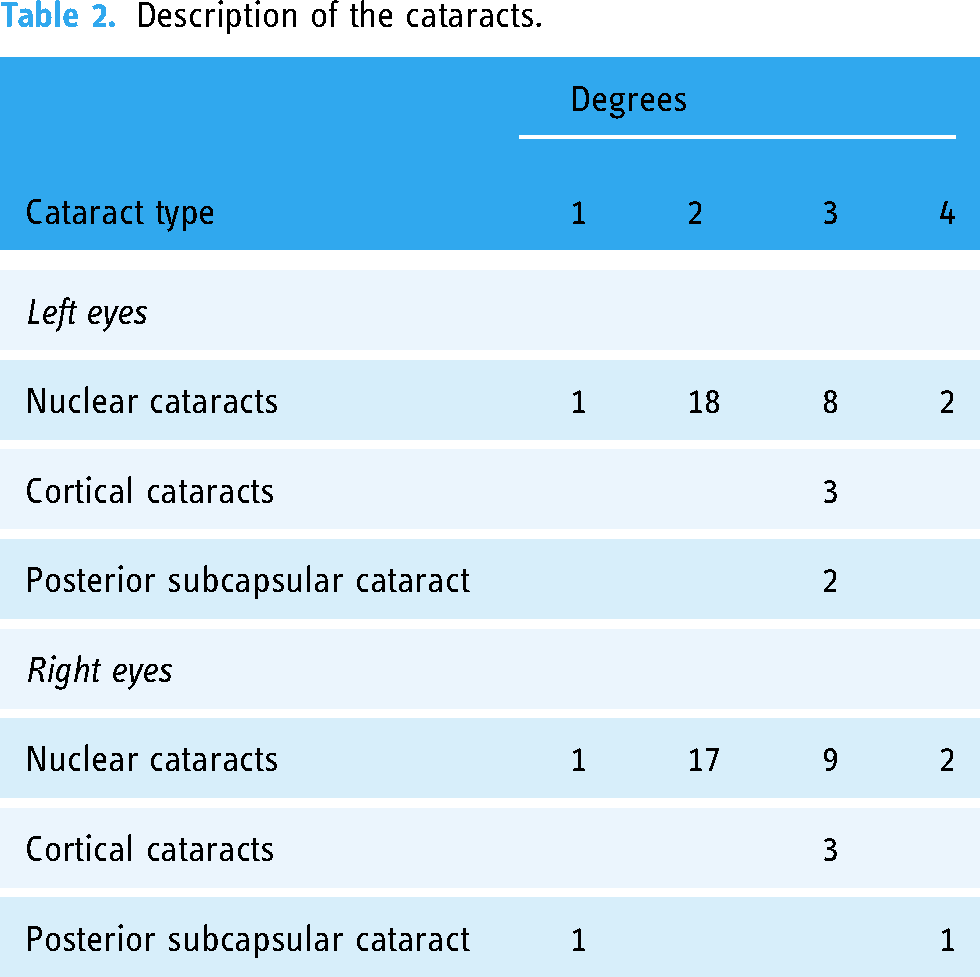
All participants underwent phacoemulsification cataract extraction with intraocular lens implantation in both eyes using a one-week interval between surgeries. The procedures were conducted at least one week before the first eye surgery and one month after the second eye surgery. The Lens Opacities Classification System III (LOCS III) was used by an expert ophthalmologist to evaluate cataract development by grading the slit-lamp and retro illumination of the cataract. 6 The LOCS III grading included six degrees of severity for nuclear, cortical, and posterior subcapsular cataracts. Visual acuity was assessed using the standard Early Treatment Diabetic Retinopathy Study chart (Xenonio, São Paulo, Brazil). All participants had no history of neurological or degenerative diseases, as well as no other ocular diseases.
Balance control procedures
A Samsung Galaxy A10S smartphone device (Samsung, Seoul, South Korea) was utilized to obtain the inertial measurements of body sway during a quiet standing position. A custom-made Android Studio application (Momentum Science), which has been validated for several protocols, including static balance control, 5 was used to record readings from the built-in triaxial accelerometer (LMS6DSL model, amplitude resolution: 16 bits, range: ±8 g) of the smartphone at an acquisition rate of 50 Hz. The smartphone was secured using double-sided tape to the lower lumbar spine region, between vertebrae L3 and L5. The recording comprised two attempts with eyes open and two attempts with eyes closed, each lasting for 60 s. It is indicated that after 30 s recording, 7 there is a trend of stabilization in the stabilometric parameters, and we consider that in 60 s of recording this trend is greater than in shorter recordings. We instructed the patients to report fatigue or tiredness in any of the tests. We drew a cross on a wall 1 m away from the participant as a fixation point.
MATLAB/OCTAVE routines were employed for offline analysis of the inertial recordings. The time series were detrended, interpolated to 100 Hz and band-pass filtered between 0.1 and 20 Hz using a second-order Butterworth filter. The quantification of the static balance control was based on the following parameters: path (in m/s²), root mean square in the mediolateral (RMS ML, in m/s²) and anteroposterior (RMS AP, in m/s²) axes, and area of the body sway (in m²/s
Statistics
We used Jamovi software for the statistical analysis. The normality of the data was assessed using the Shapiro–Wilk test. To compare the visual acuity and balance control before and after cataract surgery, paired t-tests. We also used t-tests for independent samples to compare demographic characteristics between controls and patients and one-way analysis of variance to compare the balance features between control, pre-, and post-surgery data from patients. The significance level was set at 5% for all statistical procedures.
Results
Demographic characteristics
Table 1 shows a comparison of the demographic characteristics between controls and patients with cataracts. We observed that both groups were matched in male/female proportion, age, height, and weight (p > 0.05).
Demographic characteristics comparison between controls and patients.

Description of the cataracts
Initially, all participants included in the study had cataracts in both eyes, and the description of cataracts in both is shown in Table 2.
Description of the cataracts.
Evaluation of the visual acuity
We measured the visual acuity of the participants before and after the cataract surgery and found a significant improvement in visual acuity was observed following cataract surgery (p < 0.05). Specifically, the mean visual acuity before surgery was 0.51 ± 0.27 LogMAR, whereas after surgery it improved to 0.21 ± 0.18 LogMAR.
Evaluation of the static balance control
Figure 1 illustrates the accelerometric recordings acquired before and after cataract surgery in open and closed-eye conditions from a representative participant.

Inertial recordings obtained in open and closed eyes conditions of a participant at two time points: before and after surgery for cataract removal. Upper plots represent the acceleration during sway in the ML axis, intermediate plots represent the acceleration in the AP axis, and lower plots represent the correlation between the acceleration along both axes in the static balance task.
Table 3 presents the mean values and standard deviations of the quantitative parameters for static balance control in pre- and post-cataract surgery and under open- and closed-eye conditions and controls. In open eyes conditions, the patients in the pre-cataract surgery period had more postural instability than controls as indicated by higher values in the parameters path, area, and RMS AP. After cataract removal, path and RMS AP continued higher than controls. Area values returned to control levels after cataract removal. RMS ML values in pre- and post-cataract removal were similar to the controls. In closed eyes conditions, the patients in pre-surgery conditions had RMS AP values significantly higher than controls, which was recovered after cataract removal. All other parameters in pre- and post-surgery were similar to the controls.
Comparison of the static balance evaluation before and after the cataract surgery and controls, mean values (standard deviation).

p1: control versus pre-surgery; p2: control versus post-surgery; p3: pre-surgery versus post-surgery; RMS ML: root mean square in the mediolateral; RMS AP: root mean square in the anteroposterior.
*p-value < 0.05.
The comparison between pre- and post-cataract surgery results indicated that there were significant differences for all static balance control parameters in the open-eye condition, demonstrating improved balance control after cataract surgery. Conversely, in the closed-eye condition, only the ML RMS parameter exhibited a significant difference, indicating improved balance control after surgery. However, no significant differences were observed for the other parameters.
Discussion
The present study showed the feasibility of smartphones for detecting the expected enhancement of static balance control after cataract surgery. Notably, improvements in static balance control were predominantly observed in the experimental condition of open eyes. Additionally, we observed that before surgery the patients had significant postural instability compared to controls that were partially recovered after cataract removal.
The implications of smartphone validation for static balance assessment in people with cataracts are enormous. Cataracts are one of the most prevalent health problems worldwide and can lead to balance loss and falls. 8 Falls can result in increased morbidity and mortality, 9 higher healthcare expenses, 10 longer hospital stays, 11 and lower quality of life. 12 Identifying balance loss in people with cataracts can break this negative cycle of consequences.
We observed more significant improvements in balance control after cataract surgery in the open-eye condition. Compensatory mechanisms mediated by somatosensory and vestibular systems may be activated to maintain balance control in the absence of visual information. 13 It seems that patients with cataracts may not have enough time for the nervous system to develop compensatory mechanisms to maintain balance control. We followed the patients one month after surgery and we found partial recovery of the static balance of the patients. Future studies could follow patients for a longer period than what we did in the present study.
Cataracts can significantly impair distance visual acuity, which can affect a person's ability to perceive their environment accurately. This impairment can increase the reliance on other sensory inputs, such as proprioception and vestibular function, to maintain balance during activities requiring mobility. 14 In real-life mobility activities, such as walking, climbing stairs, or navigating obstacles, static balance control influences the ability to initiate movements, maintain stability during transitions, and recover from perturbations. While static balance control alone may not fully predict performance in these activities, it is an essential component of overall balance and mobility function. 15 Other functional tests such as Timed Up and Go, sit-to-stand test, and four-meter gait speed could contribute a lot to the whole monitoring of the motor functional profile of patients with cataracts.
Although the present study still achieves its goal as proof of concept, we consider that the sample size is a limitation, and large populations of cataract patients could be recruited in future studies. We recruited only elderly participants, we did not control their different forms of cataracts, visual acuities, and interocular visual acuity differences. Future studies can be conducted to determine the static balance control between individuals with different forms of cataracts since the data show the study was conducted primarily among persons with nuclear cataracts. Additionally, taping the phone to the sacrum is not representative of day-to-day phone use. It would be useful to know if the same findings are seen when the phone is in a patient's pocket.
Our results hold significant implications for public health policies focused on screening balance control in larger populations to prevent falls, given the wide availability and accessibility of smartphones.
Conclusion
The present study confirmed the applicability of using smartphones to detect static balance impairments in patients with cataracts, who exhibited partial recovery one month after the surgical removal of the lens.
Footnotes
Acknowledgements
Not applicable.
Contributorship
GSS, NQFJ, and AAMR created the manuscript concept and wrote the draft of the manuscript. LSA, MAMA, LAXN, and GISB were involved in the ophthalmological evaluation and balance evaluation of the participants. LSA carried out the data analysis. EGRS, GHLP, and AB programmed the application for balance evaluation. AACS, ASC, BC, RCS, and KJSC contributed to the manuscript concept and refinements. GSS conceived the study and acquired funding. All authors contributed to the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and informed consent
The present investigation adhered to the Declaration of Helsinki of 1964 and all procedures were approved by the Ethical Committee for Research with Humans of the Federal University of Pará (report no. 5.264.473). Informed written consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research grants from the Brazilian funding agencies CNPQ-IC UFPA, PAPQ-PROPESP-UFPA, Amazon Paraense Foundation of Studies (FAPESPA, No. 2019/589349), and the Research Funding and the National Council of Research Development. GSS was a CNPq Productivity Fellow (#309936/2022-5). EGRS and LSA are undergraduate fellow of the program for scientific initiation of the Federal University of Pará. BC is CNPq post-doc fellow. The funders had no role in the study design.
Guarantor
GS.