
Abstract
Background
Saint Vincent de Paul Hospital is using a post-emergency teleconsultation solution (TELESCOPE). Target patients are discharged early, freeing up examination rooms and hospital beds, and the patient's clinical evolution is monitored by teleconsultation 24 hours after discharge. This study aims to evaluate this pioneering procedure, firstly to assess the impact of TELESCOPE on ED overcrowding, and secondarily to evaluate 72-hour post-emergency hospitalization rates, throughput times, and patient satisfaction.
Methods
This is a prospective, comparative, before/after type study. The National Emergency Department Overcrowding Scale (NEDOCS) score was used to measure the impact of TLC on ED congestion. It was calculated every hour, every day during the two study periods. The 72-hour post-emergency hospitalization rates were cross-compared for the patients who had a TLC, those who did not have a TLC during the same period, and those from the control period. The patient flow was evaluated by comparing the average length of stay of patients invited to a TLC against those from the control period. The patient’s satisfaction was measured through a telephone survey.
Findings
The mean difference in NEDOCS score is −3.1 [−4.14; −1.85]. Compared to the control phase, ED spent an additional 160 hours at a ‘normal’ level during the test period. The time spent in the ‘busy’ or ‘overcrowded’ categories was reduced by 129 and 19 hours. There is a significant reduction in the hospitalization rate between teleconsultation patients and all other patients. The patients discharged and invited to a TLC waited 87 minutes longer on average [56 minutes; 119 minutes]. Patient satisfaction is high (91.8%).
Interpretation
Additional statistical strength would be needed to prove a reduction in overcrowding. The low hospitalization rate reflects adequate recruitment. ED visit times were unexpectedly longer. TELESCOPE seems useful for defining a new type of care. A further multicentre study is scheduled for 2024.
Introduction
Background
Emergency departments (EDs) are increasingly overcrowded. In France, the increase in the number of admissions is continuous, significant, and > 3% per year. This results in multiple complications including longer waiting times, violence, and increased mortality.1–4 To cope with the overcrowding, we came up with the idea of discharging selected patients earlier, thereby freeing up examination rooms and hospital beds. Saint Vincent de Paul Hospital (SVPH) in Lille, France, therefore, uses an innovative post-emergency teleconsultation solution called TELESCOPE to improve patient care. 5 Started in 2020, the system was already used during the COVID pandemic 6 and demonstrated its usefulness for remote clinical reassessment and reassurance of patients during lockdown.
What is TELESCOPE?
TELESCOPE is the combination of ‘tele’ from the Greek tēle- ‘far off’ and ‘scope’ which means monitoring. The concept is to carry out a teleconsultation (TLC) within 24 hours of discharge from the ED in order to monitor the clinical evolution of targeted patients. The patients selected are patients who come to the ED for minor problems ranked class 2 or 3 according to the French Clinical Classification of ED patients (CCMU), but whose condition could deteriorate (Supplemental Appendix 1). These patients have no real clinical reason for hospitalization but are generally admitted in our seven-bed observation unit, and sometimes in the corridors of the emergency department, for a short period for monitoring and clinical reassessment. The aim is to target patients belonging to the group of non-pertinent hospital admissions (10%–30% according to literature). 7 To avoid this kind of hospitalization, patients are discharged and a video TLC is performed by an emergency physician using a secure software app and information from the medical record. If it is not possible to do a video consultation, then a telephone call is made. At the end of the TLC, either the patient can be readmitted to ED, hospitalized directly or follow-up can be stopped prescribing an early discharge and a teleconsultation is a medical decision that is made by the emergency physician in charge of the patient. The practitioners carrying out the teleconsultations are emergency doctors from the unit. This practice is integrated into the hospital's working hours. Consent to teleconsultation was signed by the patient before discharge from the ED (Supplemental Appendix 2).
The aim of this study is to assess this pioneering use of TLC. We hypothesized that post-emergency TCL via the TELESCOPE system might have an impact on the saturation level of our ED, by freeing up examination rooms and hospitalization beds and reducing waiting times.
The primary objective of this study is to assess the impact of TELESCOPE on ED overcrowding. Secondary objectives are to evaluate the rate of hospitalization within 72 hours of admission to the ED, the length of stay in the ED, and patient satisfaction (Figure 1).

Telescope workflow.
Materials and methods
Study design and setting
At the SVPH in Lille (France), we performed an observational, prospective, before and after comparative study.
SVPH is located in the centre of Lille and has a medical-surgical platform for a total of 480 beds. The short-stay hospitalization unit (SSHU) has seven beds. There is no intensive care unit in this hospital. The ED treats 40,000 patients per year. The ED had an initial physical capacity of 18,000 patients/year but was expanded in March 2021 to increase the capacity to 36,000 patients per year. Initially, the department had seven individual examination rooms, an orthopaedic area with two booths, two suture rooms and two critical emergency beds. Following renovation work, it now has 12 individual examination rooms, one casting room, two suture rooms, three critical emergency spaces and two waiting areas for eight people and three stretchers.
Study protocol and outcome measurement
The study period was chosen in order to have two comparable periods in terms of the number of hours, and less impact from the successive lockdowns due to the COVID-19 pandemic for the 2020 period. This comparative study was carried out during the following months: January, February, April and May 2019 (control period) and February, July, August, and September 2020 (test period). The inclusion period was extended to 6 months in order to obtain a larger sample to assess patient satisfaction.
To measure the impact of TLC on overcrowding we used the National Emergency Department Overcrowding Scale (NEDOCS) score (Supplemental Appendix 3). 8 The NEDOCS is a composite indicator assessing the level of overcrowding in emergency departments. NEDOCS parameters were retrospectively extracted from the local information system by the Medical Information Department, and the total score was calculated every hour from every day during the two study periods. Thresholds from the interpretation grid were then used to qualify ED crowding as normal/busy/overcrowded/severely overcrowded/dangerously overcrowded. NEDOCS was chosen because it is the most widely used indicator in the literature, and no gold standard exists to date. It is also the only score recommended by the Federation of Regional Emergency Observatories (FEDORU). It also has the advantage of being an hourly score.
To determine whether early discharge could put patients at risk, we compared 72-hour post-emergency hospitalization rates for patients who had TLC vs all the patients who did not have TLC, including the test period and the control period. Only hospitalizations within 72 hours of discharge from the ED were considered. This period was chosen because any aggravation or modification of the patient's condition can potentially be linked to the cause of the ED visit. The data were extracted from the hospital database, and therefore it only includes information relating to hospitalizations in the GHICL group.
To document the impact of the system on patient flow, we compared the average length of stay in the ED of patients invited to a TLC with all patients in the control period. Lastly, we evaluated the level of patient satisfaction through a telephone survey conducted two weeks after discharge from the ED. A four-level Likert scale was used.
Ethics
The study protocol received the approval of the GHICL's Internal Research Ethics Committee (Lille Catholic Institute Hospitals Group IRB00013355, reference study: RNIPH-2019-40). The study was qualified by the French Data Protection Authority (CNIL) as an internal study, and global information is produced by GHICL to allow patients to object to the use of their data obtained during routine care for internal research purposes.
Data analysis and statistics
The statistical analysis was performed using R software (version 4.0.5).
Qualitative data are described by numbers and frequencies, and quantitative data by means ± standard deviations.
The NEDOCS score was modelled using a linear mixed model, integrating as a fixed effect the period (control or test), and as a random effect, the time of day and the day of the week (considered as factors, the two effects being factors, and the two effects being nested with the time of day, nested in the day). This made it possible to consider the structure of the data and the autocorrelation within the data.
The average length of stay of CCMU 2 and 3 patients in the control period was compared with the length of stay for those referred for a TLC, as well as with all CCMU 2 and 3 patients in the test period, using Student's t-tests.
The hospitalization rate was compared between the two periods using a chi-square test. A significance level of 5% was used for all analyses. The statistical analysis of the questionnaires (for patients and staff) was descriptive.
Results
The total number of visits to the ED was 26,017: 13,201 for the 4 months of the control period and 12,816 for the test period.
The number of monthly visits is detailed in Table 1.
Number of visits to the ED for each month of the study.

The characteristics of all patients who came to the ED over the two 4-month periods are detailed in Table 2.
Description of the study population.

CCMU: Classification Clinique des Malades aux Urgences = clinical classification of emergency department patients; D: death; P: psychiatry.
The two populations are similar in terms of age, sex, and initial severity.
National ED Overcrowding Scale
The NEDOCS score was calculated every hour. Each value therefore reflects the level of congestion during the corresponding hour.
Table 3 describes the distribution of the NEDOCS values according to congestion levels and the study period.
Distribution of National Emergency Department Overcrowding Scale (NEDOCS) score values by crowding levels and study period.
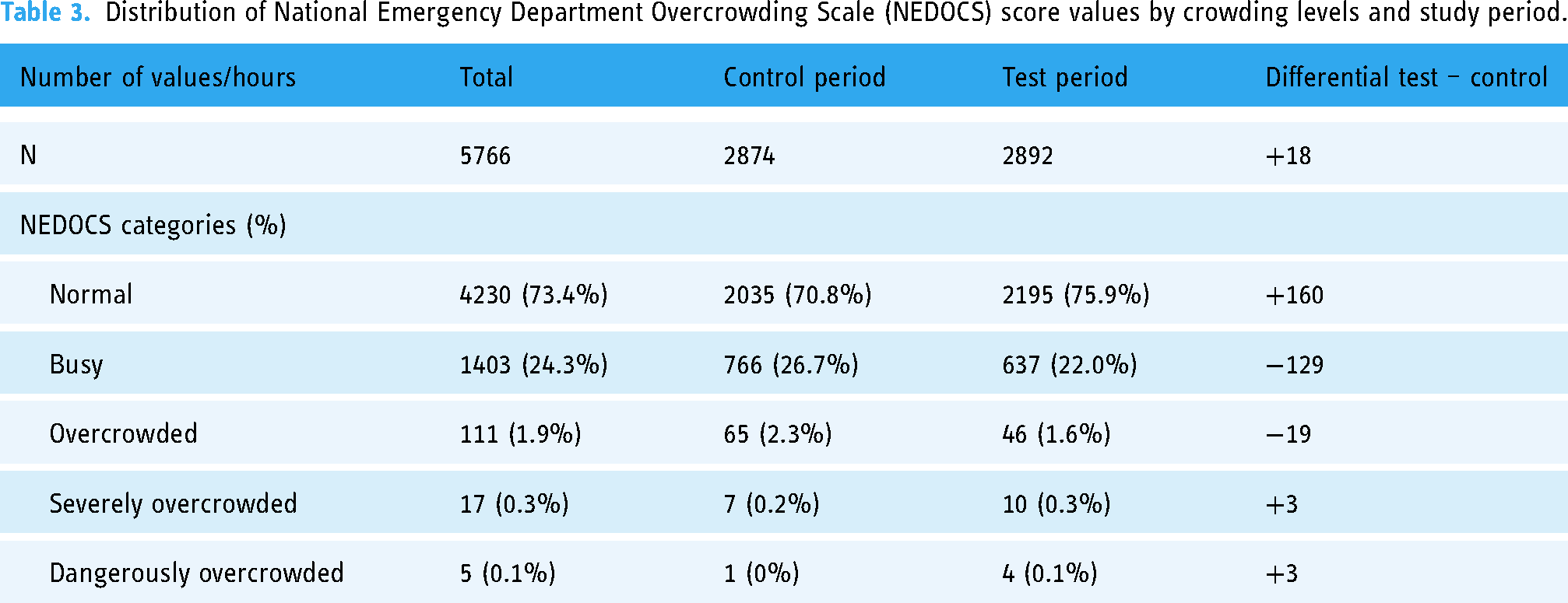
We collected a total of 5766 measurements: 2874 during the control period and 2892 during the test period.
We observed that in comparison to the control phase, the ED spent an additional 160 hours at a ‘normal’ level during the test period. The time spent at ‘busy’ or ‘overcrowded’ levels was reduced by 129 and 19 hours, respectively.
Hourly variations are described in Figure 2.
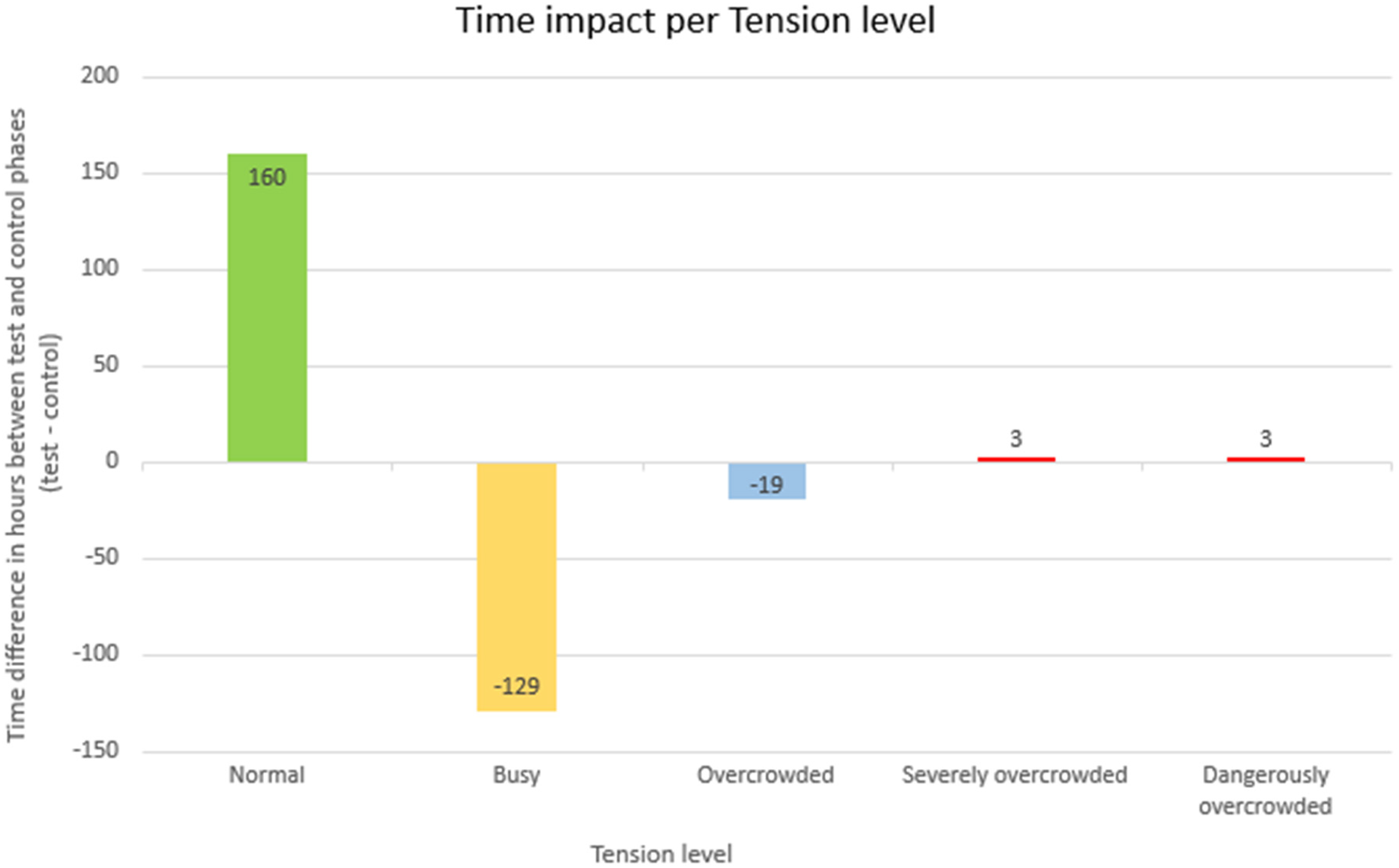
Changes in overcrowding by number of hours gained or lost at each tension level (N = test period – control period).
The mean NEDOCS score was 34.0 (± 30.6) for the control period and 30.9 (± 30.1) for the test period. The mean difference is −3.1 (CI 95%: [−4.14; −1.85]), that is, a decrease of 3.1 points over the test period. This difference is statistically significant (p < 0.001). The median score also decreased from 32.1 in the control phase to 29.2 in the test period.
Hospitalization rate
In the control period, there were 3419 hospital admissions for 13,201 visits, that is, a rate of 25.9%. In the test period, the rate was 25.6% with 3280 hospital admissions for 12,654 visits. Excluding visits followed by a TLC, the rate of hospitalization was 25.5%.
Of the 162 patients who had a TLC, 10 were hospitalized within 72 hours of the TLC, that is, 6.2%.
There is a significant difference between the hospitalization rate of teleconsultation patients, control phase patients and test phase patients who did not have a TLC (Table 4).
Hospitalization rate comparisons.

Comparison of average time spent in the ED
The control period included 10,557 CCMU 2 and 3 patients. The test period included a total of 9984 CCMU 2 and 3 patients, 162 of whom had a TLC. Overall, patients in the test period waited 31 minutes (95% CI: [25 minutes; 37 minutes]).
The difference between the waiting times was statistically significant. The patients discharged with an invitation to a TLC waited on average 87 minutes (95% CI: [56 minutes; 119 minutes]) longer than patients in the control period (Table 5).
Average visit times: control versus TLC and test.

Comparison of the average visit times of all CCMU 2 and 3 patients in the control phase, all CCMU 2 and 3 patients in the test phase, and patients who benefited from a TLC; SD: standard deviation; TLC: teleconsultation; CCMU: Classification Clinique des Malades aux Urgences = clinical classification of emergency department patients.
Patient satisfaction
We chose to use percentages to improve comprehension of the results because the inclusion period for the satisfaction survey is 2 months longer than that for the rest of the study. See Supplemental Appendix 4.
Of the patients called, 75.0% answered the telephone survey. 78.3% ‘somewhat agreed’ or ‘strongly agreed’ that TLC was appropriate for their situation after leaving the emergency room. Before the TLC, 30.7% of patients would have preferred to see their GP instead of the TLC if it had been possible. 16.1% had apprehensions about TLC. These apprehensions related mainly to technical difficulties 36.0% and the absence of a clinical examination 24.0%. Lastly, after the TLC was carried out, only 27.7% did not find it easy to install the application on their phone and 16.3% actually encountered technical difficulties (poor sound or image quality).
In terms of overall satisfaction with care, 156,91.8% of patients said they were ‘fairly satisfied’ or ‘completely satisfied’ 21.8% and 70.0%, respectively. 87.3% of patients would be willing to have another TLC.
Discussion
The prospective impact evaluation of the TELESCOPE TLC system was based on the study of ED overcrowding using the NEDOCS score, patient satisfaction via questionnaires, and the 72-hour post-emergency hospitalization rate.
Impact on the level of congestion
The NEDOCS crowding score was lower over the test period, with a statistically significant difference of 3.1 points. In hourly terms, this represents a reduction of 129 hours spent at a ‘busy’ level in favour of a gain of 160 hours spent at a ‘normal’ level. Converted to an entire day, this is, equivalent to an average of 1h20 spent at a normal crowding level. This gain is clinically significant for patients and for nursing staff working conditions.
Safety of the system
The use of post-emergency TLC for patients theoretically requiring hospitalization, but with no formal criteria for continuous use of a monitor, was safe for patients. The rate of post-TLC hospitalization was low (6.2%) and remained lower than the average hospitalization rate for CCMU 2 and 3 patients. Moreover, no deaths occurred following TLC. This rate of 6.2% reflects the appropriate use of TLC in the selected indications and also shows the relevance of medical re-evaluation by TLC. TLC thus made it possible to remotely manage 152 patients, for whom hospitalization was avoided. Reducing the number of stays by 152 in 4 months is a considerable achievement (1.2% of all patients in the test period), especially considering the seven beds of the short-stay hospitalization unit. On a weekly basis, post-emergency TLC made it possible to avoid nine short-stay hospitalizations and thus replaced the equivalent of just over one short-stay hospitalization each week.
TLC did not have any impact on overall hospitalization rates, which remained stable. This result was expected given that TLC only represents 1.3% of all emergency room visits.
Patient satisfaction
TELESCOPE gives a high level of patient satisfaction. Most of them would be willing to use TLC again.
Impact on transit times
The test period recorded longer visit times for all patients and in particular for patients who were invited for a TLC. They waited on average almost 1h30 longer than during the control period. This result is the opposite of the initial hypothesis. The selected population may be one explanation. Patients classified as CCMU 2 or 3 eligible for TLC turned out to be among the most uncertain of their categories. Indeed, although they do not have any clinical severity, they theoretically require hospitalization due to the uncertainty of their outcome.
We can then hypothesize that the length of care is extended by more frequent complementary examinations.
Moreover, the ED was expanded in March 2020, from 13 to 18 places, while there were still seven short-stay hospitalization beds. In the literature, publications by Han et al., 9 Khare 10 and Mumma 11 show that the length of stay increased as the number of beds increased. Longer waiting times in our study could therefore be consistent with previous observations and can be explained – at least in part – by the department's expansion. The computer modelling of Khare 10 even tends to reinforce the initial hypothesis that TELESCOPE should reduce the time spent in the ED. Indeed, Khare showed that increasing the rate of emergency department discharges reduced the time spent in the emergency department, despite increasing the number of beds. Han, Khare and Mumma furthermore show that increasing the number of beds does not affect the level of congestion. The expansion of the department would therefore not have interfered with the calculation of the NEDOCS.
Limitations
Our observational study was comparative, using non-contemporary before/after periods. This design has a bias, that leads to a lack of statistical strength, and further studies are required to demonstrate the efficacy of the TELESCOPE concept, such as a multicentric stepped wedge cluster randomized trial.
The impact of TELESCOPE on the NEDOCS score and on the length of time spent in the ED may be questionable, given the difference of 385 visits to the ED over the test period and insofar as TLC referrals only represent 1.3% of all ED visits. That said, the savings of 9.5 hospitalizations per week is the direct effect of TLC and has a direct impact on the problem of downstream beds.
The absolute value of this average NEDOCS score can also be questioned because it is under the threshold of 50, below which the level of tension is qualified as ‘normal’. This is not consistent with all of the ED's other overcrowding indicators: number of visits exceeding the department's capacity, workload, and staff impressions. It therefore seems that the absolute value of the NEDOCS score should be interpreted with caution. The difference in the expected result can be explained by the complexity of the data collection required to calculate the score. Indeed, the temporal data (see Supplemental Appendix 2) were not available in the computer software. Cross-checking was required to estimate these durations. Difficulty extracting elements from the NEDOCS therefore appears to be a limitation of this score.
Missing data
For the patient questionnaires, there may be a bias due to missing data. These data correspond to patients who could not be contacted by phone or who refused to answer the questionnaire. In order to reduce uncertainties, the medical files of all these patients were reviewed to collect information on their treatment and additional care following the TLC. The post-TLC hospitalization rate of 6.2% considers data from the medical records. Outcome is unknown for 63 patients (21.2%). It should also be noted that the medical records only contain information relating to care at GHICL. That said, while the post-consultation outcome is not known for these 63 patients, no claim or legal action was brought against the hospital's legal department following any complication or deterioration in their state of health.
The SARS-CoV-2 pandemic
The SARS-CoV-2 pandemic started in France in January 2020. This pandemic strongly affected ED attendance. The study period initially planned from January to March 2020 had to be postponed because of the overall decrease in the number of visits and the change in the reasons for coming, particularly from March to the end of May (imposed daytime curfew period). The difference of 385 visits between the two periods studied could therefore be explained in part by a residual effect of this lockdown. It is also necessary to bear in mind that ED attendance varies over the year. For example, the ED is less busy during the summer months. However, the test period includes the months of July and August and only has February and June in common with the control period. In addition to variations in attendance there is a seasonal variability in reasons for visits, and, therefore, in the burden of care.
Conclusion
TELESCOPE shows a statistically significant reduction in overcrowding and defines a new care pathway. While the study has moderate statistical strength, it demonstrates the feasibility of the system and its usefulness.
The procedure prevented 152 hospitalizations over four months and the post teleconsultation hospitalization rate reflects adequate recruitment. Emergency department visit times were longer, but there is a bias that needs to be eliminated in a future study. Patient satisfaction with the system was high.
A multicentric stepped wedge cluster randomized trial will be conducted at seven hospital centres in Paris and northern France in 2024 within the framework of a research program on healthcare system performance (PREPS) supported by the Ministry of Health.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241277173 - Supplemental material
Supplemental material, sj-docx-1-dhj-10.1177_20552076241277173
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241277173 - Supplemental material
Supplemental material, sj-docx-2-dhj-10.1177_20552076241277173
Footnotes
Acknowledgements
We would like to thank Dr Claeyssen Vidji, the Head of Department, for her support in this project. We would like to thank the research and statistics team for their invaluable collaboration. We would like to thank the secretaries Amélie and Kelly for their invaluable help with this project. We would like to thank Cécilia Cordova-Liendo and Liam O’Brian for their help with the English version.
Contributorship
Emmanuelle Chavda is the main writer and approved the final manuscript. Laurène Norberciak participated in the study design conception and performed the statistical analysis. She approved the final manuscript. Laurence Guedon Moreau reviewed and approved the manuscript. Enrique Casalino reviewed and approved the manuscript. Lina Williatte reviewed and approved the manuscript. Eric Wiel reviewed and approved the manuscript. Nicolas Thellier reviewed and approved the manuscript. Enrique Cordova conducted the study and reviewed and approved the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantator
Enrique Cordova. Emergency Department, Saint Vincent de Paul Hospital, Boulevard de Belfort, 59000 Lille, France: https://orcid.org/0000-0002-4888-2618, ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.