
Abstract
Background
The electronic health record (EHR) is integral to improving healthcare efficiency and quality. Its successful implementation hinges on patient willingness to use it, particularly in Germany where concerns about data security and privacy significantly influence usage intention. Little is known about how specific characteristics of medical data influence patients’ intention to use the EHR.
Objective
This study aims to validate the privacy calculus model (PCM) regarding EHRs and to assess how personal and disease characteristics, namely disease-related stigma and disease time course, affect PCM predictions.
Methods
An online survey was conducted to empirically validate the PCM for EHR, incorporating a case vignette varying in disease-related stigma (high/low) and time course (acute/chronic), with N = 241 participants, aged 18 years and older residing in Germany with no previous experience with the diseases mentioned in the respective medical reports. Participants were randomized (single-blinded) into four groups in parallel: high stigma and acute time course (n = 74), high stigma and chronic time course (n = 56), low stigma and acute time course (n = 62) and low stigma and chronic time course (n = 49). The data were analyzed using structural equation modeling with partial least squares.
Results
The model explains R² = 71.8% of the variance in intention to use. The intention to use is influenced by perceived benefits, data privacy concerns, trust in the provider, and social norms. However, only the disease's time course, not stigma, affects this intention. For acute diseases, perceived benefits and social norms are influential, whereas for chronic diseases, perceived benefits, privacy concerns, and trust in the provider influence intention.
Conclusions
The PCM validation for EHRs reveals that personal and disease characteristics shape usage intention in Germany. The need for tailored EHR adoption strategies that address specific needs and concerns of patients with different disease types. Such strategies could lead to a more successful and widespread implementation of EHRs, especially in privacy-conscious contexts.
Introduction
Background
Information technology used to collect, analyze, and interpret health data is often seen as a solution for improving the efficiency and quality of healthcare delivery.1,2 An important facet of this digital transformation process is the electronic health record (EHR), in which patients’ health data (e.g. diagnoses, therapies, vaccinations, discharge reports, emergency data, and medication plans3,4) can be documented, exchanged, and viewed.3,5 As technology, the EHR promises to facilitate communication and coordination between healthcare professionals (e.g. physicians, therapists, pharmacists) and patients to, ultimately, improve patient care and reduce costs at the same time.2,6 For instance, preexisting conditions, intolerances, and medication plans could be considered during diagnosis and treatment to avoid double diagnoses, over, and undertreatment. 5 At the same time, an improved documentation may free time, which physicians could spend interacting with their patients. 7
Although the EHR has been successfully implemented in countries such as Denmark, Finland, and Estonia,8,9 implementation has been less successful in other countries (e.g. France, Australia) or is still in the implementation stage (e.g. in Germany). In Australia, for instance, 23 million EHRs have been created but remain empty and in France less than 9.5% of the population have created a record; even fewer have filled it with their health data.10,11 In Germany, three out of four citizens state that they would use the EHR, 12 but concerns about data security and data privacy of the EHR remain high. 7 Ultimately, the success of the EHR seems to depend on whether and under what circumstances it is used by patients, all the more because it is the patient who decides what data are stored, shared, and displayed in the EHR (cf. Patient Data Protection Act in Germany).5,13
Consequently, it is important to understand both which disease-specific and user-specific factors influence users’ intention to (not) use the EHR in order to improve the EHR and increase the number of users so that the EHR can realize its touted potential. In previous studies, we and others (a) have adapted the privacy calculus model (PCM) to understand privacy concerns and intentions to use a technology in the healthcare domain10,14,15 and (b) have shown that the decisions to upload a medical report in the EHR are influenced by certain characteristics of the health data to be stored in the EHR, such as the time course and potential for stigmatization associated with the disease mentioned on a medical report.7,16–18 But and whether and how disease and user-specific characteristics influence the privacy calculus and the intention to use the EHR remains an open question.
Prior work
The PCM is an established model for examining intentions to use a technology when personal data are involved.19,20 The model, originally introduced to study interactions with social network sites (SNSs), assumes that users compare potential benefits and costs of using the technology. If the sum of the benefits exceeds the costs, people will use the technology. Vice versa, people will refuse to use it if costs outweigh benefits.15,21,22 In a preliminary study, we validated a PCM adapted for the healthcare domain with a health app of a health insurance.14,23 The adapted model suggests that patients’ intention-to-use mobile health (mHealth) apps is influenced not only by common privacy calculus factors10,15 such as perceived benefits, privacy concerns, and trust in the provider, but also patients’ general attitudes to privacy, their sense of control over personal data and the societal acceptance of using these apps (social norms).
However, the intention-to-use mHealth applications is highly context-dependent. 24 Although the two systems—EHR and health insurance apps—are rather comparable (users upload and manage sensitive health data in both systems), an important difference is that the health insurance app serves as a communication platform between patients and health insurance companies, whereas the EHR connects and shares patient data with all stakeholders in the healthcare system. This difference may result in difference privacy concerns. Thus, our goal for this article is first to validate the model, which was developed for mHealth technologies in general, for the specific EHR context.
Moreover, both user and disease characteristics tend to influence the decision to use mHealth and internet of things (IoT) technology.25,26 In previous studies, we have shown that also EHR usage depends on disease characteristics as well as on different use cases (e.g. multimorbid versus previously healthy patients).16,18 Whereas for multimorbid patients suffering from various acute and chronic diseases both the time course and the stigmatization potential of a disease had an influence on the decision to upload medical reports to the EHR, 16 previously healthy patients changed their uploading behavior only for diseases with stigmatization potential.18 Hence, in this article, we examine the influence of both factors on the intention to use the EHR to help better understand user interaction with this central digital health technology.
Aim of this research and approach
To explain the intention to use the EHR in terms of time course and stigmatization potential of diseases, we briefly review the existing PCM for the eHealth context and its hypotheses. We then validate the model for the EHR use case using structural equation modeling with partial least squares (SEM-PLS). We test the influence of disease and personal characteristics on the intention to use an EHR as predicted by the model using multigroup analysis (MGA). After discussing the results, we derive theoretical and practical implications and reflect on the limitations of the study. We end our paper with a conclusion.
Model description and hypotheses
Figure 1 shows the research model of our previous study.14,23 As in the model already validated for mHealth applications, we assume that our outcome variable, intention to use the EHR, is influenced by perceived benefits, privacy concerns, trust in the provider, social norms (what we believe others think we should do as well as their actual behavior), attitude to privacy and perceived control over personal data. The derived hypotheses are summarized in Table 1.

PCM to predict intention-to-use mHealth apps. 14 .
Hypotheses regarding the research model.

Methods
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the Department of Psychology and Ergonomics (Institut für Psychologie und Arbeitswissenschaft [IPA]) at Technische Universität Berlin (tracking number: AWB_KAL_1_230311). Participants volunteered to participate in the survey, and written informed consent was required to participate. On the first page of the survey, participants were told about the experimenter, the study purpose, what data were to be collected during the study, and where and for how long they would be stored. Hence, participants were informed about the duration of the survey (we anticipated approximately 8 min) as well as the compensation for participation. Also, the participants had the possibility to download a pdf of the participant information on the first page.
Participants
The model described in Figure 1 was empirically tested as part of a bigger online survey study, which compared the constructs intention to use and actual upload behavior. 18 Following the “10 times rule” (10 times the largest number of structural paths directed at a particular latent construct in the structural model—in our case 10 times the six paths, directed at the construct intention to use), 27 we aimed for a total sample size of n = 240 participants (n = 60 participants for each of the four planned experimental conditions: acute disease with high stigmatization potential, chronic disease with high stigmatization potential, acute disease with low stigmatization potential, and chronic disease with low stigmatization potential).
Individuals aged 18 years and older residing in Germany were allowed to participate in the study. Another prerequisite was that the participants had no personal previous experience (own illness) with the diseases mentioned in the respective medical reports, as the handling of stigmatized diseases by affected persons is different from that of unaffected persons. 28 Sampling was done through Prolific, a clickworker platform characterized by high data quality. 29 The study was conducted from May 9, 2023 until May 10, 2023. Participation was compensated with 1.60€, which corresponds to the German minimum wage. The mean value of the processing time was 9:28 min (SD = 3:47 min) and the median = 8:36 min. Two hundred and seventy-five individuals participated in the study.
Design
We used a 2 × 2 between subject study design with the two independent variables (IVs) stigmatization potential and time course of the disease. The intervention involved provided participants with a medical report containing a diagnosis, where the stigmatization potential and the disease's time course were systematically varied across four experimental conditions: (a) acute disease with high stigmatization potential, (b) chronic disease with high stigmatization potential, (c) acute disease with low stigmatization potential, and (d) chronic disease with low stigmatization potential.
Stigmatization potential is associated with high risks16,30 that consequences could arise related to areas of personal lifestyle, occupation, and social life if medical findings became known.16,28 The time course is a classification of diseases in terms of their duration. These can be either acute (diseases of short duration that come on quickly) or chronic (slowly developing or long-lasting disease). In a preliminary study, respondents in a qualitative semi-structured interview described uploading medical findings of chronic diseases into the EHR as more beneficial than uploading findings of acute diseases. 16
Each participant read one of these reports at the start of the study, simulating a scenario where they had to decide whether to upload this medical finding into an EHR. This task was designed to trigger responses based on the perceived stigmatization and duration of the condition outlined in the report.
Participants were randomly (single-blinded) assigned to one of these conditions in parallel (simple randomization, ratio: 1:1:1:1) using LimeSurvey’s built-in “rand” function. The dependent variables were the constructs of the PCM: intention to use, perceived benefits, privacy concerns, trust in the provider, social norms, attitude to privacy and perceived control over personal data.
Materials
Following a common practice in technology acceptance studies,31,32 we used a case vignette to represent a typical situation in which an EHR app may be used. In particular, the case vignette depicted a situation where the participant has recently started using an EHR app and is now faced with the decision to upload a medical finding to their EHR (see Appendix 2). Additionally, the disease/injury was described in lay terms with one to three sentences (see Appendix 3). In selecting the diseases, both their stigmatization potential and their time course were systematically varied. The stigmatization potential covered different risks for professional and social life, such as depression as a disease33,34 or tests for STDs with high stigmatization potential35,36 and fractures or diabetes as diseases with low stigmatization potential. To reflect different time courses, diseases were divided according to an acute (e.g. wrist fracture) and a chronic time course (e.g. type-1 diabetes). Furthermore, diseases were selected to occur regardless of age so that they would be perceived as realistic diseases by an age-diverse sample. Table 2 shows the diseases used in the stimuli, categorized in terms of stigma potential and time course.
Diseases used in the stimuli, categorized by stigmatization potential (SP) and time course (TC).

As in a previous study, 16 an interactive prototype (a so-called click dummy) was used which was modeled after the mobile EHR application of a German health insurance company (the BARMER)—the eCare app—using a software for interface design (FIGMA). This prototype allows for a realistic interaction with an EHR. Specifically, the prototype gave participants the ability to upload findings, grant or revoke permissions to view findings, and create medication plans. Only the “Upload findings” function was used in this study. The interaction with the EHR prototype preceded the survey study.
We used LimeSurvey (version 3.28.3 + 220315) to create and conduct a five-page online survey. The EHR prototype was embedded into the survey using iFrame. LimeSurvey software was used to ensure that all questions had to be answered to complete the study and receive the compensation. As in the previous study, we tested the effect of the independent variables by querying the perceived risk and perceived benefit of uploading findings to the EHR. 16 Based on previous results, we assumed a high perceived risk when the stigmatization potential was high and a high perceived benefit when the time course was chronic. Perceived risk, perceived benefit, and all questionnaire items 14 (see Appendix 1) were measured using a 7-point Likert scale ranging from 1 (“strongly disagree”) to 7 (“strongly agree”).
Procedure
The study procedure is shown in Figure 2. The survey consisted of four parts. After giving their written informed consent according to the WMA Declaration of Helsinki, (1) the study was initiated, and participants had 1 minute to interact with the EHR prototype. (2a) Participants then read a randomly selected case vignette addressing the use of the EHR in the context of uploading a medical finding (low or high stigmatization potential and acute or chronic time course, depending on the experimental group). (2b) Subsequently, participants were asked to assess the risks and benefits of uploading the medical finding mentioned in the case vignette. (3) Afterwards the questionnaire was answered by the participants. (4) The survey was completed with the collection of demographic characteristics (age, gender, and education level) as control variables, as well as the opportunity for participants to declare their responses invalid due to lack of care in processing.

Overview of the study design.

Flow chart of participant assignment to the experimental groups and exclusions. Note. SP: stigma potential; TC: time course.
Analyses
To validate the model outlined in Figure 1, we used structural equation modeling with partial least squares (SEM-PLS). We tested the influence of disease and personal characteristics on the intention to use an EHR as predicted by the model using multigroup analysis (MGA). The SEM-PLS was carried out with SmartPLS 4 (version 4.0.9.4). All items of the questionnaire, except PB07 und SN03 due to poor standardized factor loadings, were included in the final analysis and restricted to load on the respective constructs described above and in Figure 1. The P values of the paths were evaluated with t-statistics obtained from bootstrapping with 5000 resamples. We cleaned and analyzed the data of the perceived risks and perceived benefits using RStudio (version 2023.06.0 + 421). These analyses were performed using t-tests.
Results
Survey characteristics
A total of 275 observations were collected. A total of 34 records were excluded, of which 29 were excluded because of participants’ medical history, three because of incomplete questionnaires, and two because they were marked as invalid by participants. Figure 3 shows the participation and distribution process of the participants as a flow chart.
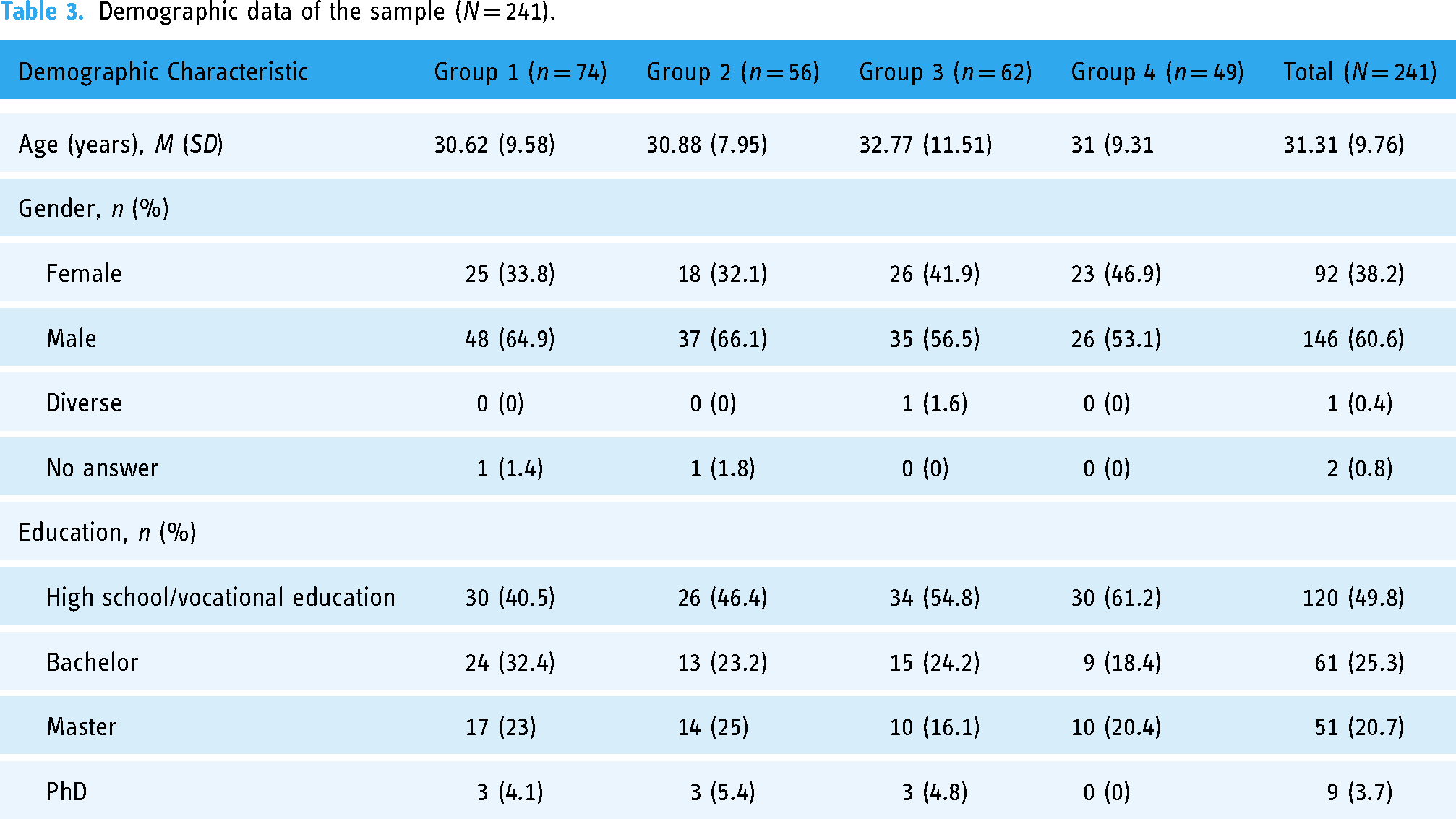
A sample of 241 observations (146 male, 92 female, one diverse, two no information) was used for further analysis. Table 3 summarizes the demographic characteristics of the sample for each group.
Demographic data of the sample (N = 241).
Risk and benefit perception
Similar to the preliminary study, 16 risk and benefit perception of uploading served as a manipulation check to test the validity of our manipulation of the stigmatization potential (risk) and the time course (benefit) through the medical findings (see Figure 4). As expected, uploading medical findings of stigmatized diseases was perceived as significantly riskier than those of non-stigmatized diseases (low: mean = 3.98, SD = 1.7; high: mean = 5.12, SD = 1.71; t239 = 5.447; p < .001). In addition, uploading findings of chronic diseases was perceived as significantly more beneficial than acute diseases (acute: mean = 5.38, SD = 1.37; chronic: mean = 5.90, SD = 1.37; t239 = 2.98, p = .003). Consequently, we assume that our manipulation was successful.
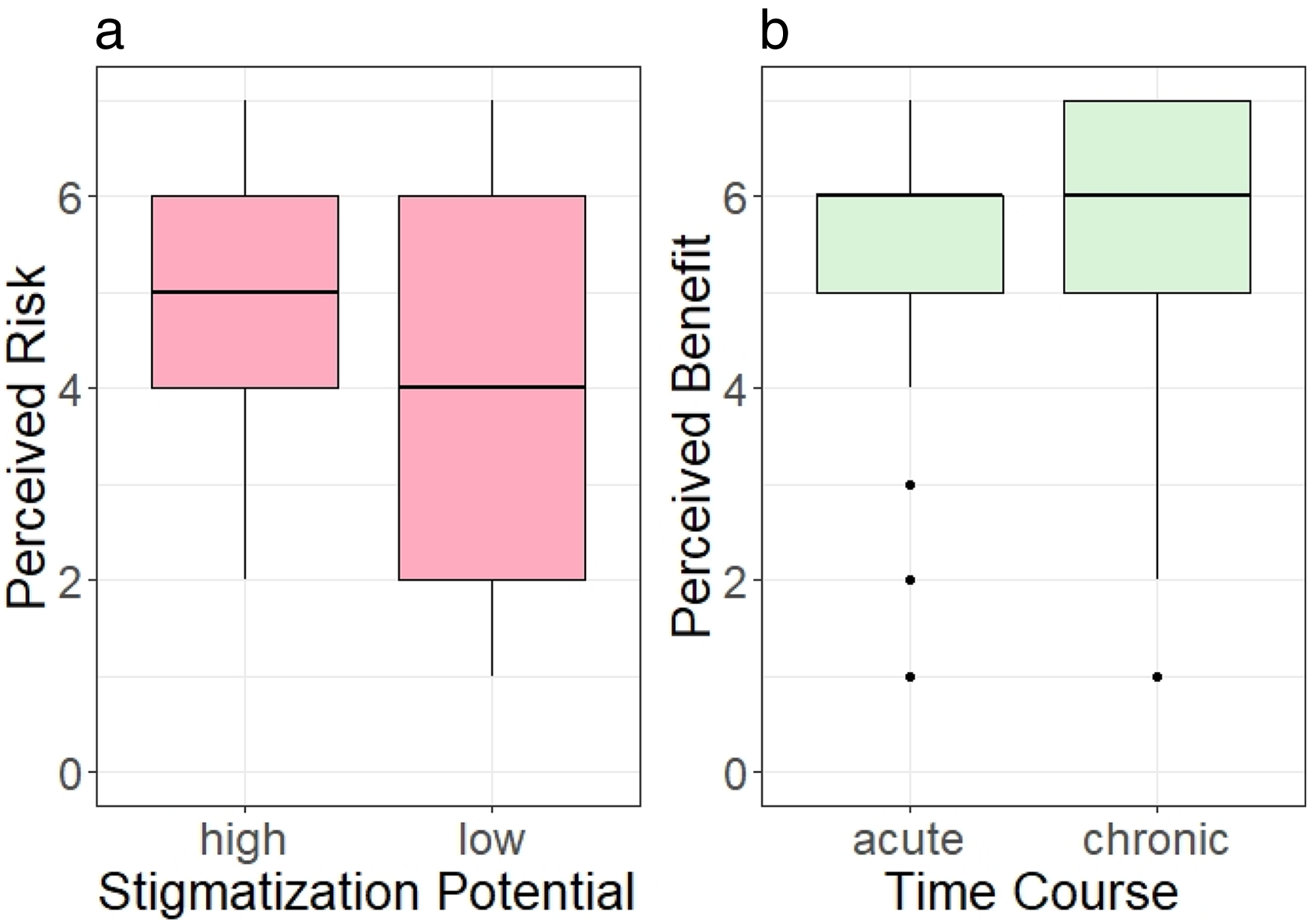
(a) Perceived risk in terms of stigmatization potential and (b) perceived benefit in terms of time course.
Assessment of the structural model
The internal consistency of the scales as well as convergent validity and discriminant validity of the measured constructs are shown in Tables 4 and 5. Internal consistency was evaluated with Cronbach's alpha with the criterion of α ≥ .7.37,38 All constructs surpass the recommended value, so that internal consistency can be assumed. The convergent validity was assessed following Hair, Black, Babin, and Anderson 38 using three criteria: (a) The significance of the factor loadings, which exceed the criterion value of 0.5; (b) the average variance extracted (AVE) should be greater than 0.5; (c) the composite reliability (CR) should surpass the minimum threshold of 0.6. After eliminating PB07 und SN03 due to poor standardized factor loadings (<0.7), 38 all subscales met these three criteria.
Quality criteria of the constructs.

Note. AP: attitude to privacy; CON: perceived control over personal data; PB: perceived benefits; PC: privacy concerns; SC: social norms; TP: trust in the provider; IU: intention to use; AVE: average variance extracted; CR: composite reliability and alpha: Cronbach's alpha. The abbreviations given in the “Item” column are explained in Appendix 1.
Measurement model—discriminant validity.
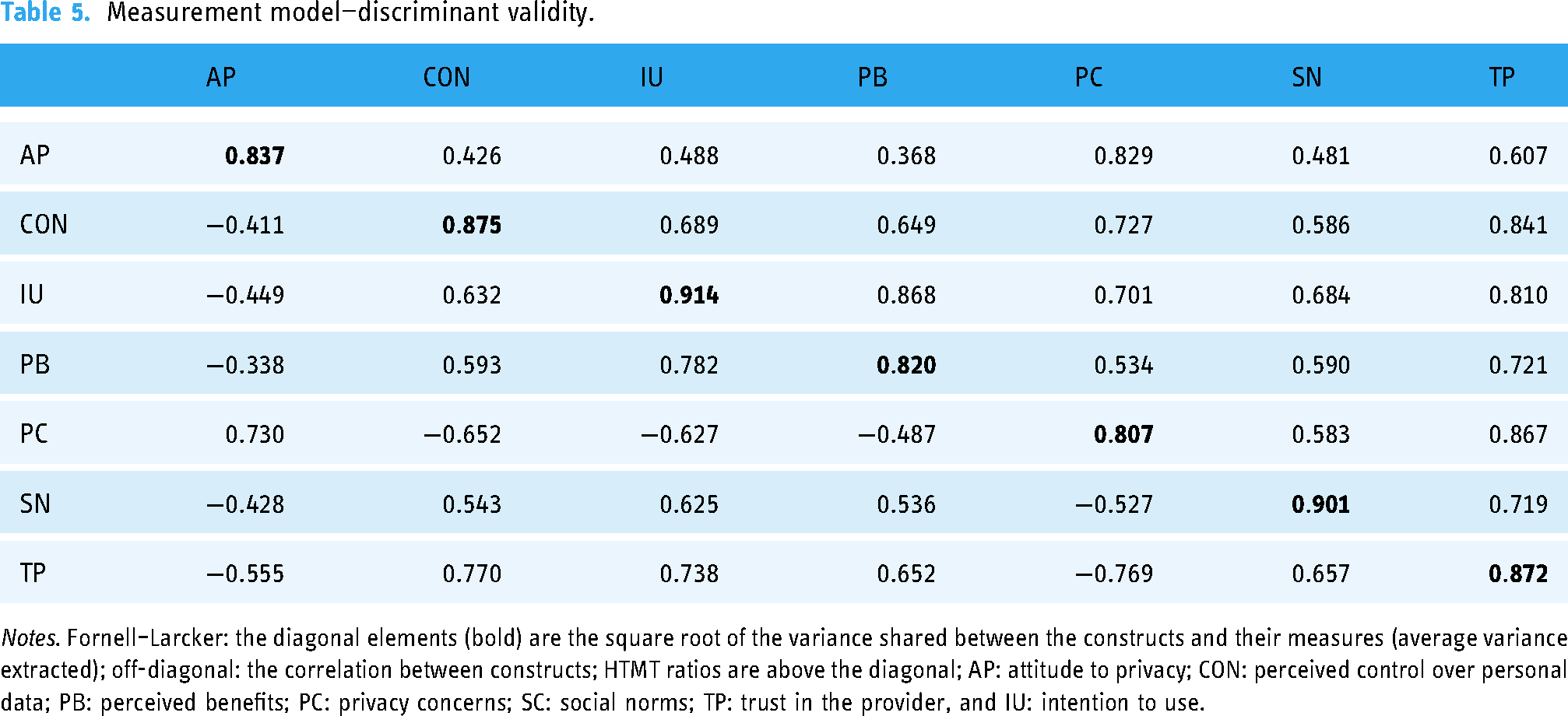
Notes. Fornell–Larcker: the diagonal elements (bold) are the square root of the variance shared between the constructs and their measures (average variance extracted); off-diagonal: the correlation between constructs; HTMT ratios are above the diagonal; AP: attitude to privacy; CON: perceived control over personal data; PB: perceived benefits; PC: privacy concerns; SC: social norms; TP: trust in the provider, and IU: intention to use.
Discriminant validity was evaluated by the Fornell–Larcker criterion.38,39 For each latent variable the square root of AVE (diagonal elements) must be larger than the correlation between this latent variable and any other latent variable (off-diagonal elements). Additionally, the heterotrait–monotrait (HTMT) ratio of correlations was used to certify discriminant validity.38,40 All constructs were below the threshold of 0.90 for conceptual similar constructs. As shown in Table 5, both criteria were fulfilled for all latent variables. The measurement model thus presents appropriate psychometric properties.
Results of the structural model
After evaluating the criteria of the measurement model, we now describe the structural model concerning the use of the EHR in more detail. The structural model was estimated by using bootstrapping (5000 samples) to generate t-statistics and to evaluate the statistical significance of the relationships. Figure 5 represents the path coefficients and the corresponding P values.

Factor relationships in the structural model. Solid lines represent statistically significant links and dashed lines represent statistically nonsignificant links. *p < .05. **p < .01. ***p < .001. ns: not significant.
The R2 values for the intention to use, privacy concerns and trust in the provider, but not for perceived benefits, far exceed the cutoff value of 0.4 41 and suggest a good model fit. Our model explains R2 = 71.8% of the variance in our main dependent variable, the intention to use the EHR. Consistent with our expectations, perceived benefits have a significant effect on the intention to use (P < .001), as well as privacy concerns (p = .018), trust in the provider (p = .010), and social norms (p = .001), supporting H1, H2, H3, and H4. Perceived control over personal data has significant effects on privacy concerns (p < .001) and trust in the provider (p < .001), thus supporting H5b and H5c. There is no significant effect on intention to use (p = .897), rejecting H5a. The attitude to privacy has significant effects on perceived benefits (p < .001), privacy concerns (p < .001), and trust in the provider (p < .001). Thus, H6b, H6c, and H6d are supported. The attitude to privacy, however, has no effect on the intention to use (p = .841). Consequently, H6a is rejected. Table 6 summarizes the detailed analysis of the path coefficients.
Overview of the path coefficients.

Results of the multigroup analysis
We conducted multigroup analyses (MGA) to examine whether the relationships in the model varied depending on the control variables (i.e. personal characteristics) and the IVs. The MGA allows for direct nonparametric tests of the path estimates in the structural model for each bootstrap sample, following the MGA procedure in PLS with a bootstrapping of 5000 samples. 42
Controls
Aside from gender (female vs. male), we recoded the demographic variables age (younger vs. older) and education (non-academics vs. academics) as dichotomous variables, because MGA are performed as two-group comparisons. The influence of gender (female: 92 cases; male: 146 cases) showed no significant difference in the path coefficients. For age, we divided the participants into two age groups by performing a median split, younger adults (participants 18–29 years of age: 128 cases) and older adults (participants who are 30 years or older: 113 cases). There were significant differences in the path coefficients between the younger and older participants regarding the influence of privacy concerns (p = .034) and trust in the provider (p = .016) on intention to use. While privacy concerns do not influence intention to use for younger participants (path coefficient −0.003, p = .980), their influence increases with increasing age (path coefficient −0.280, p = .001). For the younger participants, trust in the provider influenced the intention to use (path coefficient 0.315, p < .001), although not for the older participants (path coefficient −0.012, p = .907). For education (non-academics: 120 cases; academics: 121 cases) there were significant differences for the path coefficients between trust in the provider (p = .008) and intention to use. Trust in the provider influences the intention to use the service for non-academics (path coefficient 0.384, p < .001) but not for academics (path coefficient 0.011, p = .910).
Time course and stigmatization potential
The MGA for the stigmatization potential of diseases (low: 111 cases; high: 130 cases) showed no significant differences in the path coefficients. However, there were significant differences with respect to the time course of diseases (acute: 136 cases; chronic: 105 cases) between the path estimates between the influence of perceived benefits (p = .008), privacy concerns (p = .025), social approval (p = .011), trust in the provider (p = .012), attitude to privacy (p = .050), and perceived control over personal data (p = .012) on intention to use (see Figure 6).

Factor relationships in the structural sub-models concerning acute and chronic diseases. Solid lines represent statistically significant links and dashed lines represent statistically nonsignificant links.
When uploading medical findings to the EHR, the perceived benefits had a greater influence on intention––albeit in the same direction––when the mentioned disease was chronic (path coefficient 0.543, p < .001), than in the case of an acute disease (path coefficient 0.471, p < .001). When interacting with medical reports of chronic diseases, privacy concerns influence intention to use (path coefficient −0.188, p = .049) in contrast to acute diseases (path coefficient −0.135, p = .138). Conversely, social approval had no influence on intention to use when uploading reports of chronic diseases (path coefficient 0.092, p = .244), but they did when uploading reports of acute diseases (path coefficient 0.178, p = .001). When uploading reports of chronic diseases, trust in the provider had an influence on intention to use (path coefficient 0.215, p = .039), but not when uploading findings of acute diseases (path coefficient 0.176, p = .098). Although there was a significant difference for uploading acute and chronic findings to the EHR in terms of the influence of both perceived control over personal data and attitudes towards privacy on intention to use, the influence of both paths was not significant in both sub-models and therefore of no further importance. Table 7 presents the path coefficients and the corresponding P-values of the models of the subsamples with respect to the time course as well as the difference between the models.
Results of the MGA concerning time course.

Notes: *p < .05; **p < .01; ***p < .001. ns: not significant.
Discussion
Principal findings
This study investigated whether the PCM adapted for mHealth apps can describe the intention to use the EHR in general and in relation to personal characteristics (demographics) and disease characteristics including stigmatization potential and time course. The model provides a valid representation of the intention to use the EHR, as the proposed model explains the variance (R2) in users’ intention-to-use mHealth applications better than other reported models (where the values do not exceed 0.5),15,43 with an overall complexity similar to existing models. We examined the influence of demographic control variables on the relationships in the model, of which age and education had significant effects. Older users have more privacy concerns and less trust in the provider than younger users, which negatively influences their intention to use the EHR. Additionally, the influence of trust in the provider on the intention to use the EHR also decreased as the level of education increased. While the influence of both control variables is not uncommon in the mHealth and IoT domain,25,26 they did not appear in other SEM studies regarding EHR use thus far.10,15,44
When looking at the full model, it is evident that the intention to use the EHR is significantly influenced by perceived benefits (path coefficient = 0.499) as the overall strongest driver of intention to use. The more beneficial the use of the EHR is perceived by users, e.g. for health data management of patients with multiple chronic conditions, 45 the more likely it is that an intention to use will be formed. However, these perceived benefits were inhibited by the patient's attitude to privacy (negative path coefficient = −0.338). This means that benefits of EHR use, such as more effective treatment and less effort in managing one's health data, are devalued or ignored in the decision to use the EHR if the respective patients perceive privacy issues as important. The inhibiting influence of privacy concerns on the intention to use (negative path coefficient = −0.161) confirms similar findings of prior studies. 7 Privacy concerns were even more pronounced when general attitudes to privacy were high (path coefficient = 0.556). Nevertheless, our model suggests that privacy concerns were significantly inhibited by the level of perceived control over personal data (negative path coefficient = −0.424). The more users perceive that they can make independent decisions about whether and how to store their data in the EHR (delete, share, etc.), the fewer privacy concerns they tend to have. 44 The model also shows that the more trust is placed in the provider, the more likely it is that the EHR will be used (path coefficient = 0.193). This trust is positively associated with control over personal data (path coefficient = 0.652) unless patients have a generally high attitude to privacy (negative path coefficient = 0.287). Finally, the intention to use was also driven by social norms (i.e. social approval), that is, the opinions, experiences, and the EHR use of close relatives (path coefficient = 0.147). This is in line with findings from social psychology, which show that people tend to adopt the opinions of their peers or relatives. 46
The consideration of disease characteristics (time course and stigmatization potential) enables a more nuanced view of the factors influencing the intention to use the EHR. An important finding is that the intention to use the EHR is significantly influenced by the time course of diseases but not the stigmatization potential, which has been shown to influence actual uploading behavior.16,18
For acute diseases, the intention to use EHR is primarily influenced by the perceived benefits (path coefficient = 0.471) and social approval (path coefficient = 0.178). In the case of chronic diseases, the situation is more complex. Here, the intention to use EHR is affected by three key factors: perceived benefits (path coefficient = 0.543), privacy concerns (negative path coefficient = –0.188), and trust in the provider (path coefficient = 0.215). In other words, the significant differences regarding the acute and chronic time course of diseases can be broken down into four main points regarding perceived benefits (a), privacy concerns (b) trust in the provider (c), and social norms (d):
When comparing the impact of perceived benefits on the intention to use the EHR, their positive influence is notably stronger in the case of chronic diseases than it is for acute diseases. This is not surprising as health concerns (i.e. the personal importance of health issues) have a positive impact on the sharing of health data via the EHR.
10
It is in one's own health interest to share data about chronic diseases via the EHR so that it can be considered in future diagnoses.10,47 The impact of privacy concerns varies significantly between acute and chronic diseases. Although privacy concerns tend to decrease intentions to use the EHR in the case of chronic diseases, they do not significantly influence the intention to use EHR with acute diseases.
7
This finding is particularly striking given that previous studies suggest that patients had less privacy concerns when the use of an EHR meant an improvement in their health.10,48 Contrary to this, our observation indicates an increased influence of privacy concerns in chronic diseases, i.e. when EHR use would result in an actual improvement in users’ health. Trust in the provider had a positive influence on the intention to use the EHR only in the case of chronic diseases. This is hardly surprising, as a perceived vulnerability (i.e. awareness of a possible risk) is a prerequisite for trust. If little risk is perceived, as with the acute diseases in our study, no trust is required to upload the findings to the EHR.49,50 For chronic diseases the influence of social norms on the intention to use the EHR vanished. Consequently, when it comes to chronic diseases patients intention to the EHR is neither influenced by the approval of their social group (i.e. injunctive norms or what we believe others think we should do) nor by the behavior of others (i.e. descriptive norms or typical behavior in a situation). Instead, they seem to rely on their own perception of benefits and risks.
Implications
Our study has various theoretical and practical implications. As can be seen from the differences between the sub-models in terms of the time course of the disease as well as age and education of users, intention to use the EHR is a context-specific construct. The focus on context increases the usefulness of these models as it helps to further specify which factors should be considered when conducting studies with the PCM and how to translate its predictions into practical interventions to increase EHR adoption rates. Specifically, social norms/approval may be effective to increase EHR uptake when it comes to acute diseases (e.g. through a reward system for encouraging family members or friends) but not for chronic diseases. For chronic diseases as well as for older and higher educated users, on the other side, privacy concerns should be reduced and trust in the provider should be built, for instance, through transparent and easy-to-understand information about the high safety standards of EHR (e.g. for encrypting data) and the data stored in them (e.g. via the control of access rights). Such combined measures can help to increase the number of users, regardless of disease characteristics, and thus support implementation efforts of EHR.
Limitations and future directions
We deliberately excluded participants who already had a medical history with the diseases addressed in the stimuli to avoid bias in their responses. Individuals suffering from a stigmatized disease are more cautious to disclose the information, especially if the disease is not immediately apparent.28,51 The question arises as to what extent the behavior of stigmatized and chronically ill people can be simulated under experimental conditions, provided that the participants do not have any stigmatized characteristics or chronic illnesses. To further strengthen the validity and generalizability of our results, the perspective of people who are already affected should be examined in a follow-up study and compared with the results of this study.
Another limitation is that the chronic and acute disease patterns used in the stimuli are not readily comparable. We decided to use the diseases listed in Table 1 because they resulted in the expected effects in a preliminary study. 16 For future studies, it would make sense to use other diseases that can be more readily compared in terms of their perceived stigma and time course (e.g. gonorrhea and HIV or a wrist fracture and arthritis) to further strengthen the generalizability of the present findings. In addition, the study was conducted exclusively with German citizens due to the focus on the German healthcare system. Follow-up studies should examine the applicability of the results to other countries, as there are differences between the individual healthcare systems as well as in the willingness to share personal data online. 52 Finally, in this study, injunctive social norms were operationalized with respect to recommendations and approval of the use of the EHR by friends and families. To what extent patient's beliefs of social approval of health professionals increase or decrease intention to use 53 remains to be seen in future studies.
Conclusions
This paper highlights that disease and personal characteristics influence the formation of the intention to use EHRs. Specifically, the study found relevant differences in the intention to use based on the time course of diseases to be uploaded in the EHR. In the case of acute illnesses, the intention to use the EHR was primarily driven by perceived benefits and social norms. For chronic diseases, the study observed a significant shift. The influence of social norms on the intention to use the EHR vanished, whereas factors like privacy concerns, trust in the provider, and perceived benefits became more prominent. This suggests that patients with chronic illnesses recognize a greater value in using the EHR, but they have heightened privacy concerns due to the more permanent and risky nature of the data associated with chronic conditions. Additionally, the study found that the experiences, recommendations, and behavior of close relatives influenced the intention to use the EHR only for acute diseases. Finally, personal characteristics also had an influence on the intention to use the EHR. With increasing levels of education, trust in the provider no longer played a role in the formation of the intention to use. Similarly, compared to their younger counterparts, older users’ intention to use the EHR was less influenced by trust in their provider and more impacted by privacy concerns.
These findings imply that for effective EHR adoption, strategies must be tailored to the specific needs and concerns of different patients with different types of diseases. This more nuanced understanding can guide healthcare providers and policymakers in developing targeted approaches to increase user adoption, ensuring that the system meets the varying needs of patients with different health conditions. This is an important step for a more successful and widespread implementation of the EHR.
Footnotes
Acknowledgments
We acknowledge support from the German Research Foundation and the Open Access Publication Fund of TU Berlin. We acknowledge the Evangelisches Studienwerk Villigst and the German Federal Ministry of Education and Research for providing the doctoral scholarship to NvK, which was essential for the completion of this research. We extend our gratitude to all participants of the study for their invaluable contributions.
Contributorship
NvK researched literature and conceived the study under the supervision of MAF. NvK was involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. NvK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This Ethics Committee of the Department of Psychology and Ergonomics (Institut für Psychologie und Arbeitswissenschaft) at Technische Universität Berlin approved this study (tracking number: AWB_KAL_1_230311).
Guarantor
NvK.
Appendix 1—Questionnaire
Manipulation check (perceived risk): Rate the following statement: If the information in this finding fell into the wrong hands, it would do me a lot of damage.
Manipulation check (perceived benefit): Rate the following statement: I think it is very beneficial that physicians who treat me have access to this finding through the EHR.