
Abstract
Objectives
More and more disasters are occurring and there will be an increasing shortage of physicians in the future. Telemedicine could be a solution here to offer medical care despite the lack of physicians in the area of operation. This study analyzes whether telemedicine for lower-qualified paramedics is comparable to conventional disaster medicine.
Methods
A simulation study was conducted in which one conventional and two telemedicine groups cared for thermal-traumatically injured in a stressful situation. The telemedicine was conducted on tablets with integrated vital sign monitoring or on smartphones. The physician engagement time, the number of physician contacts, the time for relevant measures and the usage behavior of telemedicine were examined between these groups.
Results
One telemedicine group showed significantly fewer patient contacts. This can be attributed to the ongoing consultation in the intervention group with more contacts. There are no significant differences in the relevant measures.
Conclusion
Telemedicine is comparable to conventional disaster medicine in civil protection. Due to potential technical failures, it should primarily be used to compensate for the lack of physicians, and training should focus on an exit-strategy in case of a failure of the telemedicine.
Introduction
In civil protection, the aim of a treatment center is to treat several injured people at one place until transport to a hospital is possible. The concept of the Medical Task Force in Germany equips one treatment center with two paramedics (comparable to an Emergency Medical Technician Intermediate), two Emergency Medical Responders, one team leader and a physician. 1 Together, they are responsible for simultaneously caring for up to seven patients with varying triage categories. 1 The patients may be at the center from just a few minutes up to 48 h, depending on transport and hospital capacity. 1 However, due to an increasing shortage of physicians,2,3 it will become more difficult to find physicians for civil protection on-site. Additionally, physicians are often needed to serve multiple roles, such as in hospitals, civil protection and emergency medicine. As a result, it has been proposed that telemedicine could be used to compensate for the lack of physicians, and therefore, there is a need to further investigate the feasibility of telemedicine in civil protection.
In previous scenarios, telemedicine was used to connect physicians to bring medical expertise to the patient where it is needed.4,5 For example, the use of telemedicine in emergency services has already become routine. Telemedicine has also been used in the military sector or during disasters around the world.4–6 However, in both cases so-called tele-advice were used, in which physicians consult via telemedicine. To date, there are no scientific studies in which telemedicine has been used in disaster medicine by paramedics and it remains the subject of investigation. Civil protection scenarios are classified as stressful due to a wide variety of factors, which include: a shortage of staff; limited resources; and the fact that the severity of patient injuries cannot be predicted. 7
Disaster scenarios are rare and, due to the specific circumstances, not suitable for evaluating an innovation like telemedicine. To investigate in more depth whether telemedicine can be used in civil protection for a large number of patients with mild to severe thermal-traumatic injuries requiring care during a stressful situation with a lack of resources, a simulation scenario in a treatment center was developed. The aim was to investigate whether telemedicine can provide a medical treatment comparable to conventional disaster medicine by comparing the physician engagement time, the number of physician-patient contacts and whether there is a delay in critical measures.
Methods
Study design
A randomized controlled simulation study was designed, in which a team of six responders had to care for ten simulated patients with different triage categories within 1 h. The teams participating in the study were divided into three different study groups (Figure 1):
Control Group (CONT) Intervention Group A (IVA)—Teams with a tele-paramedic Intervention Group B (IVB)—Teams with a tele-paramedic and telemedicine on smartphones for all other team members

Study groups with qualifications of the responders (own illustration).
In the CONT, all responders, including the physician, are in the treatment center on-site. In the IVA and IVB the physician becomes a tele-physician, who is outside the treatment center at the telemedicine station in an adjacent room. Instead, there is another paramedic in the treatment center, who is guided through the medical treatment by the tele-physician via teleconsultation. He/She uses a special web app (University Hospital RWTH Aachen, Aachen, Germany), which is linked to a teleconsultation software based on the further developed software “TeleDoc Starter” (Docs in Clouds TeleCare GmbH, Aachen, Germany). With the use of a camera (Ulefone Night Vision Camera, Ulefone Technology Co., Ltd, Shenzen, China) and a headset (M612QD007, Xiamen Mairdi Electronic Technology Co. Ltd, Xiamen, China), communication between the tele-paramedic and the tele-physician is possible.
Additionally, different medical devices are connected via Bluetooth or cable to transmit vital signs. The medical devices are a multidevice with one-channel electrocardiogram and pulse oximetry (Viatom CheckmeTM Pro, Lepu Shenzen Viatom Technology Co., Ltd, Beijing, China), a blood pressure monitor (Riester ri-champion SmartPro, Rudolf Riester GmbH, Jungingen, Germany) and an electronic stethoscope (Riester ri-sonic PCP-USB, Rudolf Riester GmbH, Jungingen, Germany). In the special app, the tele-paramedic can document, use interactive guidelines on how to triage and treat patients in general, for critical bleeding, pain and burns. Additionally, the app includes a telemedicine function to call the tele-physician.
The IVB differs from the IVA in that each responder in this group had a smartphone (iPhone SE and iPhone 8, Apple Inc., Cupertino, USA, or Google Pixel 6, Google LLC, Mountain View, USA) in addition to the tele-paramedic. These smartphones did not have additional medical devices attached, so they could not share vital signs. However, the responders could use all other functions of the app.
The tele-physician uses the corresponding telehealth software based on the “TeleDoc Starter” (Docs in Clouds TeleCare GmbH, Aachen, Germany), which runs on a Windows notebook.
In preparation for the study, all participants received an online training session that lasted approximately 2 h. The training covered the concept of the Medical Task Force, the study's protocol, telemedicine, disaster medicine measures, including the guidelines, and important medical procedures. The participants were familiarized with the use of the technology, and the app's functions were incorporated into their training.
Participants were divided into teams according to their availability. These teams were randomly assigned to cohorts via ultimatesolver.com. The online tool was set to allocate three CONT, three IVA and four IVB groups among the ten participating teams. The tool was then used to randomize which study cohort the teams were to be assigned to. Participants were informed about the group assignments on the day of the study.
Simulation scenario
The study was conducted on five occasions. Each time there was a tent with a minimum area of 33.8 m2 (Figure 2). This was equipped with predefined medical products and devices, which were replenished for each simulation based on lists. Additionally, a telemedicine workspace was set up in an adjacent room, out of sight and hearing range from the scenario (Figure 2).
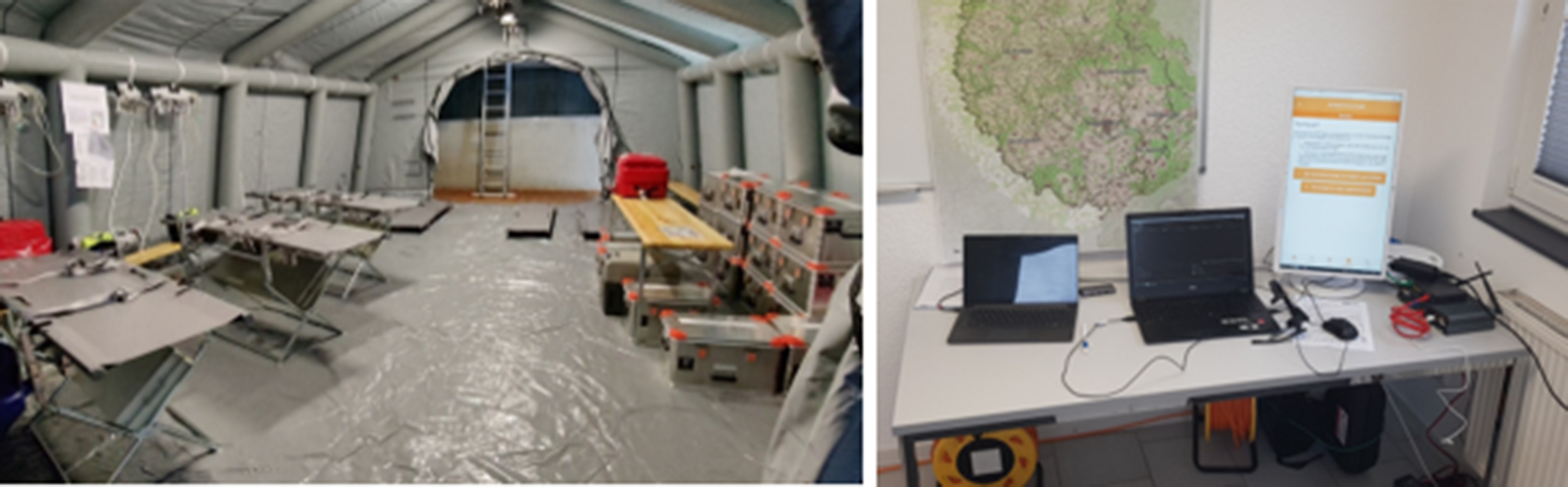
Study setup: left: treatment tent with medical equipment on the left and right side, right: telemedicine station in an adjacent room (own illustration).
The simulation followed a script (Supplemental Material) featuring ten different patients (Table 1), identical for all teams. For each simulation, eight amateur actors were recruited to play the patients, along with two simulation mannequins (Trauma Trainer Professional, Ambu, Ballerup Sogn, Denmark, and Resusci Anne Advanced Skill Trainer, Laerdal, Stavanger, Norway). The actors were professionally made up by a team specializing on realistic accident portrayal. To ensure consistency, pictures of the injuries were taken to maintain identical wound representation.
List of patients with their triage category and their injuries.

The triage categories of the patients were defined as follows: green (minor injuries); yellow (delayed treatment required); red (urgent treatment); and blue (no chance of survival, palliative care only). The study took place in a tent, and medical supplies and equipment were provided according to the concept of the German Medical Task Force. Only noninvasive measures were applied to the actors. Invasive procedures, such as inserting a laryngeal mask, were only carried out on the simulation mannequins as part of the training scenario.
During the scenario, each patient had an observer who recorded observations, provided vital signs as per the script, and answered patient-related questions. This was necessary to assist the actors when patients’ conditions changed throughout the simulation or when the simulation mannequins were considered responsive. The observers were not allowed to offer any assistance to the responders and were trained to only report the vital signs collected. Due to the expected stressful situation, which also affects the observers, and to prevent missing data, the scenario was filmed using a 360° camera. In addition, the telemedicine software was evaluated for the number and duration of consultations.
Participants
For this study, emergency responders were recruited through various aid organizations in Germany. The participants with the required qualifications were sought in the form of team leaders with experience in leading small units, physicians, paramedics, and emergency medical responders. The following inclusion criteria had to be met: Participants had to be over 18 years of age, had to meet the required qualification but not a higher one or be in training for a higher qualification, and agree to participate by providing written informed consent. The recruitment of these participants took place over a period of five months and was supported by the responsible authorities of the aid organizations at each study location.
Outcome parameters
The study aimed to investigate whether telemedicine could be used comparably to conventional disaster medicine in the setting of a civil protection scenario with a lack of personnel and material resources. The following outcome measures were used as primary parameters: The physician engagement time was measured as the amount of time the physicians were involved in patient care, both patient-related and considering the triage category. The number of patient contacts by physicians was counted as the total number of patient interactions involving the physicians.
In addition, the following secondary outcome measures were investigated: The delay in relevant interventions was measured as the time it took to successfully perform relevant interventions through conventional or telemedicine delegation. This aimed to assess whether telemedicine led to any delays in crucial medical actions. For this purpose, the times were recorded for interventions that were relevant for the patients’ survival or for the progression of the scenario. These interventions included:
Application of a tourniquet (Patient 1) Declaration of death (Patient 2) to preserve limited resources for patients with a higher chance of survival Abdominal examination (Patient 3) to detect suspected internal bleeding Recognition of unconsciousness (Patient 4) to initiate further measures afterward.
The patterns and behaviors using telemedicine were observed by counting the number and analyzing the time of the teleconsultations in the observations and the software protocol. Who started the consultation was also analyzed.
Confounders
Potential confounders could arise due to the failure or malfunction of the technology. These are also to be expected for real civil protection. The technology was tested in advance in order to keep the system as robust as possible. Further disruptive factors could arise due to the experience of the emergency responders. Particularly for volunteer civil protection responders, some of whom also work in the emergency service, different levels of experience are common. However, the goal of telemedicine should be that all paramedics can be instructed in the measures, regardless of their experience. When selecting the participants, care was taken to ensure that they each had the same qualifications. The experience could not be influenced or evaluated in advance. This is also a factor that would occur in real civil protection. In addition, an affinity for technology can also have an influence on the use of such methods and the resulting outcomes.
Statistics
For statistical analysis, IBM SPSS Statistics Version 28.0.0 was used. The statistical analysis was performed to test for significant differences. In the first step, the data were tested for normal distribution according to Shapiro-Wilk. As individual variables were ordinally scaled, normally distributed data with the one-way ANOVA test and non-normally distributed data were analyzed for significant differences using the Kruskal-Wallis test. The significance level was p < 0.05.
Ethics
This study has been approved by the Ethics Committee of the University RWTH Aachen and is registered under the number EK 139/22.
Results
A total of ten teams participated in the simulation: three in the CONT, three in the IVA and four in the IVB. During the study, one team in the IVB experienced significant technical disruptions, resulting in the inability to establish teleconsultation for approximately half of the simulation time. Consequently, this team was excluded from the analysis. Thus, each group had three teams, totaling nine teams overall.
Sixty participants were included in the study, comprising 9 team leaders (also qualified as paramedics), 9 physicians, 24 paramedics and 18 emergency medical responders, with 25 of them being female. The median age of the participants was 29 years (18 to 71 years). The physicians had various experience in civil protection (none: 6 persons; 5–10 years: 1 person; > 10 years: 2 persons).
Divided into cohorts, the CONT consisted of 3 team leaders, 3 physicians, 6 paramedics, and 6 emergency medical responders with 11 male and 7 female participants. Their average age was 27.1 ± 5.5 years. The IVA consisted of 3 team leaders, 3 physicians, 9 paramedics and 6 emergency medical responders with 10 male and 11 female participants. Their average age was 31.7 ± 13.5 years. The IVB also consisted of 3 team leaders, 3 physicians, 9 paramedics and 6 emergency medical responders with 14 male and 7 female participants. The average was 30.6 ± 10.1 years.
A total of 90 (n = 90) simulated treatments were analyzed. In all treatments, there was the option to involve a physician, either conventionally or through telemedicine. However, 13 patients were not treated by a physician, most of whom arrived at the treatment center at the end of the simulation. As a result, no physician engagement time could be determined for these cases. An overview of the results for all outcome parameters is shown in Table 2.
Mean values of all collected outcome parameters divided according to the cohorts.

Physician engagement time
The physician engagement time in the CONT, IVA and IVB groups was normally distributed (p = 0.428; p = 0.106; p = 0.106) and had average values of 53.6 ± 6.5, 32.3 ± 11.4, and 55.1 ± 5.4 min, respectively, across the entire simulation. A statistically significant difference was observed only between the IVB and IVA (p = 0.043).
While not in all groups the distribution of physician engagement time per patient within the triage categories is normally distributed, so normal distribution was not assumed simplistically. Significant differences in the duration of treatment for patients of a particular triage category were treated by each group were consistently observed for the triage categories yellow/red (Patient 4, see Table 1) and green (CONT: p < 0.001; IVA: p = 0.011; IVB: p = 0.005).
Additionally, the CONT exhibited significant differences between the triage categories red and green (p < 0.001), as well as between the triage categories yellow and green (p = 0.049). The IVA also showed significant differences between triage categories red and green (p < 0.001), as well as between red and yellow (p = 0.007) (Figure 3).
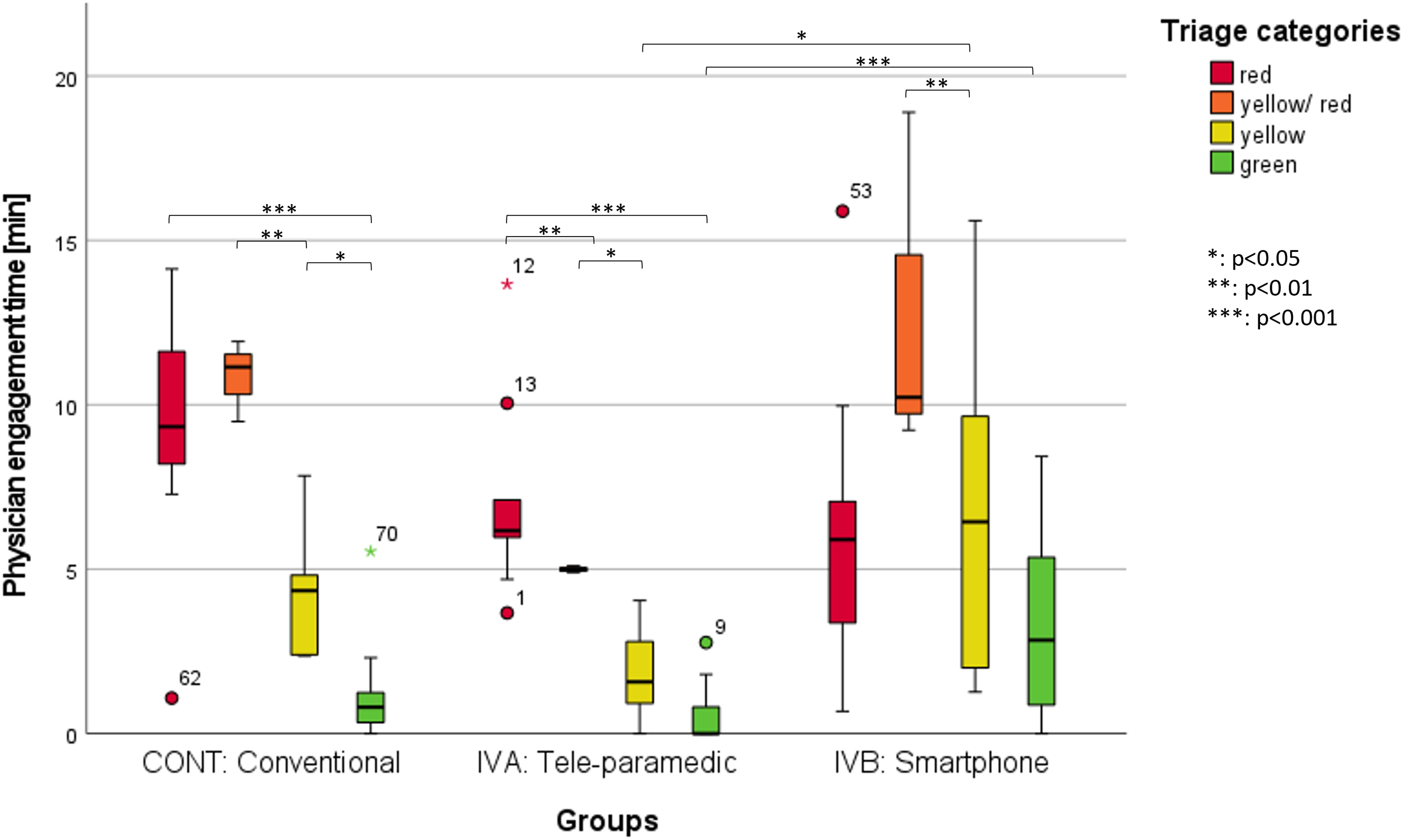
Physician engagement time (min) of each treatment regarding the triage category, with significant difference marked (own illustration).
Patient contact
The cumulative number of physician-patient contacts, regardless of whether a patient received multiple treatments, was normally distributed within the CONT, IVA and IVB (CONT: p = 0.688; IVA: p = 0.383; IVB: p = 0.165). The average number of physician contacts was 54.33 ± 7.10 (CONT), 12.00 ± 2.65 (IVA), and 36.33 ± 11.59 (IVB). The IVA had significantly fewer patient contacts than the CONT and IVB (p = 0.002, p = 0.029).
When looking at the patient contacts within a triage category (Figure 4) and comparing these between the groups, significant differences between the CONT and the IVA can be seen in each case (red: p = 0.005, yellow/red: p = 0.010, yellow: p = 0.001, green: p = 0.001), as well as between the IVB and the IVA for the red (p = 0.023), yellow (p = 0.033), and green (p = 0.002) triage categories.

Physician–patient contacts for all patients of each triage category for all groups, with significant difference marked (own illustration).
The number of patient contacts for different triage categories within the same study group was not always normally distributed; therefore, no normal distribution is assumed. Both the CONT and IVA exhibited significant differences in patient contacts between the triage categories red and green (CONT: p = 0.013, IVA: p = 0.001), as well as between yellow/red and green (CONT: p = 0.006, IVA: p = 0.007). Additionally, the CONT showed a significant difference between the triage categories yellow and green (p = 0.021). However, the IVB did not show any significant differences.
Delay of relevant interventions
No significant differences in the timing of interventions were observed between the groups. The time to apply a tourniquet took 1.28 ± 0.65 min for the CONT, 0.88 ± 0.65 min for the IVA, and 1.05 ± 0.85 min for the IVB.
Usage behavior
During the study, a total of 43 teleconsultations were initiated. The majority of these consultations were conducted by the Tele-paramedic, with only three consultations performed by other paramedics using their smartphones. In the IVA, significantly fewer consultations were initiated compared to the IVB (31 vs. 12 teleconsultations; p = 0.046), but these fewer consultations of IVB were used to maintain a continuous connection to the tele-physician over a long time.
Discussion
In this simulation study, ten simulated patients were treated by nine teams each with six responders in a treatment center with conventional disaster medicine or telemedicine. The results demonstrated that relevant measures were not delayed despite a few significant differences in physician engagement time and the number of patient contacts, based on a civil protection scenario. The IVA showed significantly less physician engagement time for some triage categories than the IVB. The patient contacts of the IVA were almost all significantly fewer than the other groups. Simultaneously, no relevant interventions were delayed in any of the groups, and there were overall no significant differences between the CONT and the IVB.
Although in the IVB, compared to the IVA, all emergency responders could have used telemedicine via a smartphone, only a few calls via smartphones can be identified. Therefore, the significant difference in physician engagement time between IVA and IVB can be explained by the continuous ongoing consultation by the IVB. The results show that physician engagement time is increased in severely injured patients, which was to be expected. Also, the deterioration of the patient's condition from yellow to red was acknowledged in most cases by a medical contact.
However, because no relevant measures were delayed, this result shows that medical treatment can also be guided in shorter teleconsultations, which is consistent with the results of Brokmann et al. 8 who also found a significantly shorter physician engagement time. The difference between this study and ours, however, is that in ours, lower-skilled paramedics as volunteers in civil protection with no or little experience in emergency medical service used telemedicine. In this case, it can therefore be assumed that the instruction of the measures for the tele-paramedic was shortened, and that the tele-paramedic is instead independently responsible for the correct implementation based on their experience and training. The tele-paramedic is thus given a high degree of confidence in his or her abilities, which depends on the measures in question.
The IVA shows significantly fewer patient contacts than the other groups. One possible explanation for this is that conventional disaster medicine has a physician onsite who can independently conduct a follow-up assessment of patients and thus generate additional patient contacts without much effort. In IVB, teleconsultation was almost continuously active, allowing for a similar effect. Here, the tele-physician can also request a patient's follow-up assessment. In IVA, on the other hand, the tele-paramedic decided whether further physician contacts were necessary.
However, a continuous consultation also means that the tele-physician is not available for other treatments outside this treatment center. Against the background of the lack of resources, the responders could thus endeavor to request as few consultations as possible to give other responders the possibility of teleconsultation. In this context, the availability of physicians for telemedicine in the event of a disaster is interesting to investigate.
Simultaneously, this connection to only one tele-physician at the treatment center facilitates patient handover, as the tele-physician is already familiar with the patient's medical history and, ideally, has an overview of the patients and their treatment priorities.
The number of patient contacts between the triage categories also shows that patients with a higher treatment priority are more likely to be contacted by a physician. Due to the severity of the injuries, it is expected that the condition of these patients may be more likely to deteriorate, either because interventions are not working well enough or because of undetected injuries. Regular and recurrent checks are therefore important.
For the most part, only the IVB did not exhibit significant differences between the triage categories, indicating that the tele-physician engagement time and number of contacts were generally similar. However, it is important to emphasize that the actual physician engagement time and the number of patient contacts should always be based on the medical needs of the patients and cannot be generalized. Nonetheless, education could raise awareness among medical responders to prioritize the treatment of red and yellow patients and focus resources accordingly, with a view to optimizing patient outcomes.
The analysis of the time points for relevant interventions, crucial for the further treatment process or resource management, does not show any significant differences. This is an indication of telemedicine being comparable to conventional disaster medicine, and enables to delegate and guide the necessary measures for injuries of civil protection via telemedicine. Although the quality of the measures was not evaluated in this study, the time to apply a tourniquet is partly comparable to the study of Hossfeld et al. 9 but with the difference that, in our study, the time to apply the tourniquet was measured from the time the patient arrived at the treatment center. Due to this, our time is a bit longer, but still in a time frame of less than 2 min.
Measures for examining the abdomen and noticing unconsciousness could also be supported telemedically or in the case where no further medical expertise was required. In many countries, there is a legal requirement that the declaration of death must be made by a physician. Studies have already shown that individual cases in which medical personnel were supported by a doctor in the telemedical declaration of death 10 or the neurological declaration of death was carried out after machine measurements, e.g. the pupil width and reaction. 11 Even if it may be ethically questionable, in the case of civil protection, the declaration of death via telemedicine should be used only with given consideration. However, palliative measures such as the administration of analgesics can also be supported telemedically. A decision should be made based on a legal regulation of the declaration of death via telemedicine in civil protection cases.
If all medical observations are summarized, it becomes clear that despite lower physician engagement time and patient contacts, the IVA did not perform any of the relevant interventions significantly later. In some cases, this cohort was the fastest. It can be deduced from this that the IVA worked more resource-efficiently with shorter physician engagement times. At the same time, however, it can also be seen that the green patients in particular usually received only very brief treatment or none at all. However, the same effect can also be seen in the CONT. It is not possible to make a definitive statement about whether IVA was the most medically effective on the basis of the data.
The usage behavior of the telemedicine app showed differences between the groups, with continuous teleconsultation leading to longer physician engagement time and more patient contacts. Although no relevant interventions were delayed, it is expected that continuous teleconsultation will have advantages for the onsite responders’ collaboration with the tele-physician. Additionally, some of the responsibility for prioritizing treatment is taken away from the tele-paramedic, allowing the tele-physician to determine priorities when a comprehensive overview is available. With technological tools, this overview could be facilitated in the future—for example, with a digital overview of the treatment center where the tele-physician can make notes about patients and their place in the treatment center.
Continuous consultation also results in the loss of app functions that could be useful for all other emergency responders, such as patient-specific displays of required interventions. Therefore, an adjustment to the app demonstrator is necessary to allow switching between patients during ongoing consultations, enabling the continued use of all app functions.
One team from the IVB was excluded from the analysis due to numerous technical problems that hindered the successful conduct of consultations. This highlights that technical problems can arise, leaving emergency responders to manage treatment on their own. To address network outages, suitable contingency strategies, such as utilizing cellular networks 12 or satellite communication,13,14 can be employed. However, these strategies may not address other technical problems that could lead to telemedicine failure. Consequently, it is crucial to have appropriate standard operating procedures (SOPs) in place, outlining step-by-step actions for handling technical failures and guiding the continuation of medical treatment as a kind of an exit-strategy if telemedicine is not available. This ensures that measures are not delayed and provides responders with the confidence to act effectively.
Furthermore, it is essential to emphasize that telemedicine should only be used as a compensation for a lack of onsite physicians and should not replace physicians in the civil protection concept. Especially in the initial hours following an event, the demand for physicians is most critical, 15 making telemedicine beneficial until additional onsite physicians arrive. Depending on the availability of onsite physicians, they can take over the care of the most critical patients if telemedicine becomes unavailable.
The results demonstrated that telemedicine can be used comparably to conventional disaster medicine. Even inexperienced users can thus handle challenging situations like a civil protection scenario under stress and treat a multitude of patients with sometimes complex injury patterns. This finding aligns with other studies on telemedicine, specifically teleconsultations in emergency medicine, which also conclude that telemedicine is feasible and comparable to conventional medicine.16–18 Moreover, real-world implementations have shown that technical difficulties can be reduced with further development, making the improvement of our system a realistic possibility. 19 Furthermore, it is essential to explore the possibility of deploying responders with lower qualifications as tele-paramedics and determine which measures can be effectively guided through telemedicine. Overall, telemedicine proves to be a valuable and viable approach in the context of emergency medical care during civil protection.
Limitations
One limitation of this study arises from the small number of participating teams, with nine teams divided into three groups. Despite efforts, additional teams could not be recruited, even after five months. Nevertheless, 90 patient treatments were included in the analysis.
The participating physicians had varying levels of experience in civil protection and their respective professional careers. The allocation of physicians was based on their availability, thus no control was exerted over which physicians were assigned to specific groups.
Each simulation day involved conducting between one and three scenarios. The actors participated in one or multiple simulation days. However, new actors were also occasionally integrated into the study. These actors became aware of the scenario details only after the initial run-through. Consequently, despite having a detailed script, there were slight variations in the performances, which could represent a limitation.
Additionally, the makeup teams changed frequently, with a total of three different teams involved. To avoid different injury representations, photographs were taken during the first session and made available to subsequent makeup teams.
No concept was given for the use of telemedicine, so the teams were able to decide independently whether they would restart telemedicine for each consultation or let the consultation run through. However, in order to be able to document patient-specifically, it was technically necessary to start the consultation again and scan a patient-related QR code. All emergency responders received this information in advance during the briefing. The fact that the IVA ended the call after each consultation, while all the IVB opted for an ongoing consultation was not planned and became apparent during the evaluation. Conclusions that can be traced back to this could therefore be included in the evaluation, although this different use should actually be assessed as a confounder that was not taken into account in advance.
The simulation was designed to compare telemedicine with conventional disaster medicine. A scenario was intentionally chosen to challenge the emergency response teams with measures and challenges some of which they had not encountered before. However, since most of the injured were actors, real medical interventions were limited, making it impossible to evaluate the correct execution of the measures. Observable errors, such as the misplacement of intravenous access in the opposite direction of the blood flow, were pointed out by observers, and these instances were considered as “not performed” until executed correctly to achieve the therapeutic goal of the script.
Conclusion
In conclusion, the analysis of physician engagement times and the number of patient contacts suggests that telemedicine is comparable to conventional disaster medicine in civil protection scenarios, as no significant delays in relevant intervention attributable to telemedicine were observed. However, it should be noted that there is a higher availability of physicians for telemedicine than for onsite civil protection. Differences in usage behavior contribute to significant variations in physician engagement time among the telemedicine groups. Addressing this issue requires the establishment of more precise guidelines for telemedicine utilization, accompanied by an enhanced contingency strategy for technical challenges, encompassing comprehensive SOPs. Additionally, further technological development should aim to create a more reliable and less error-prone system.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241272662 - Supplemental material for Telemedicine in civil protection: A controlled simulation study for the analysis of patient care
Supplemental material, sj-docx-1-dhj-10.1177_20552076241272662 for Telemedicine in civil protection: A controlled simulation study for the analysis of patient care by Anna Müller, Simon Kraus, Robert Arimond, Janosch Kunczik, Rolf Rossaint, Michael Czaplik and Andreas Follmann in DIGITAL HEALTH
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The German Federal Office of Civil Protection and Disaster Assistance funded this study as part of the TeleSAN project (FKZ: 41201/425).
Guarantor
AM.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.