
Abstract
Background
The e-DENT program, initiated by Montpellier University Hospital's Department of Dentistry, seeks to enhance dental care access for individuals with special needs through teledentistry. This five-year retrospective study focuses on the program's impact, particularly assessing patients’ mood and behavior during telemedicine dental examinations and the influence of these factors on diagnostic quality and feasibility.
Methods
This retrospective, multicentric observational study analyzed data from January 1, 2018, to April 24, 2023, involving residents of medico-social institutions who participated in the e-DENT program. The study utilized a scoring system based on the PANAS scale, which is used to brief measures of positive and negative affects. We aimed to evaluate mood and behavior. The statistical analysis was conducted using R software, incorporating mixed logistic and linear regressions to assess the impact of various factors on patient behavior, mood scores, and the quality and feasibility of diagnoses.
Findings
The study included 682 patients, revealing that the majority exhibited cooperative behavior during their telemedicine consultations, with a median mood score of 2.5. Analysis showed a significant improvement in mood scores from the first to subsequent consultations. The mood score positively correlated with diagnostic feasibility and negatively with visit duration. Specific factors such as type of disability, fear of dental instruments, and patient cooperation significantly influenced the quality of videos taken and the feasibility of diagnoses. Facilities catering to different disability types showed varied mood scores, suggesting tailored approaches may be necessary.
Interpretation
The findings underscore the efficacy of teledentistry in providing dental care to individuals with special needs, highlighting the importance of patient mood and behavior in improving diagnostic outcomes. The study suggests that teledentistry can be a well-accepted and effective mode of dental care delivery for this patient group, with implications for optimizing telemedicine practices in medico-social settings.
Keywords
Introduction
Since 2014, the Department of Dentistry at Montpellier University Hospital has developed a telemedicine program in dental care called e-DENT. 1 This program aims to improve dental care access for individuals with special needs. The initial step in care provision involves assessing the patient's needs through remote diagnosis. To optimize diagnostic feasibility, these assessments are conducted in medico-social facilities within the hospital's territory, close to the targeted patients.
The e-DENT system comprises the following: (a) A Soprocare® intraoral camera (Acteongroup, Mérignac, France) utilizing fluorescence technology, enhancing remote diagnostic quality, particularly for carious lesions and gingival inflammations. 2 (b) A laptop connected to the intraoral camera via USB. The laptop, requiring internet access for data transmission, is equipped with specific software for recording patient information and videos. (c) The e-DENT by Conex software (Conex Santé, Labuège, France), designed to collect all necessary information for remote diagnosis by the dentist. This software also streamlines data entry for the operator. (d) A secure server for data storage and compliance with the General Data Protection Regulation (GDPR). Personal health data used for telemedicine activities are transmitted to this server, and dentists access the data through secure authentication.
The e-DENT telemedicine dental examination follows an asynchronous four-step process: (a) The visit: A nurse trained in basic dentistry and device usage captures the necessary information for remote diagnosis by the dentist. Data includes the patient's medical history and current health status, a clinical examination using the intraoral camera in fluorescence mode to record videos of each dental sector, and the patient's behavior during the examination. (b) Data transfer: Since the telemedicine process is asynchronous, constant internet connectivity is not required. After the visit, the nurse finalizes the record, which is automatically sent to the central server upon internet connection. (c) Analysis: Once the visit data reaches the secure central server, the designated dentist accesses and analyzes the patient's information and videos to diagnose and propose a personalized care plan. (d) Diagnostic feedback: After the dentist completes the diagnosis and report, the nurse accesses the central server to retrieve and either print or save the report in the patient's digital records.
The e-DENT program, operational since April 14, 2014, primarily serves medico-social institutions but is also widely used in prisons
3
and Montpellier University Hospital's medical services.
4
Initially targeting individuals with special needs, identified as the most significant need in the region by the Regional Health Agency (ARS),5,6 the program has been under review for the last five years, particularly regarding patient perceptions of the visits. As mentioned by WHO, While mHealth provides great opportunities, it also entails challenges to employ mobile technologies in a way that ensures everyone benefits and that inequalities in health and oral health are reduced instead of contributing to further widening the gap and leaving people behind.
7
We decided to consider especially patients who suffered from inequalities in access to dental care.
Even though the e-DENT project was 10 years old this year, the policymakers are still doubtful about the acceptability of teledentistry by people with specific needs. There is no article in the literature presenting results on this aspect. We decided to focus on the subject to reduce the huge gap in knowledge.
The primary objective of our study is to evaluate the mood and behavior of patients with special needs during a telemedicine dental examination. Secondary objectives include the following: assessing the impact of repeated procedures on patient behavior, evaluating average visit durations based on facility types and patient behavior, characterizing patients, especially in terms of general pathologies distribution, identifying proposed care pathways, assessing patients’ oral health status, and evaluating dental urgency levels and the necessity for emergency appointments.
Materials and methods
Trial design
The e-DENT program has been recognized as a medical activity since its endorsement by the Regional Health Agency in November 2015, following its pilot phase. This study is a retrospective, multicentric observational analysis. Our research is confined to the analysis of data from the past five years, spanning from January 1, 2018, to April 24, 2023. The study protocol received approval from the “Sud Méditerranée III” Human Research Ethics Committee at the initiation of the program, complying with French regulations under the number: 2014.02.05 bis, dated March 6, 2014. Every patient or their legal representative signed a consent to be part of the study and to be diagnosed using teledentistry.
Protocol
(a) Residents of medico-social institutions participating in the e-DENT program (or their legal representatives) consented to telemedicine dental examinations and the research protocol. (b) Nurses at these institutions conducted ‘visits’ and collected necessary diagnostic information (medical records, clinical examination via intraoral camera, patient behavior). There was one designated nurse per institution. (c) After data transmission, the diagnoses made by teledentists and the resultant reports were sent back. All anonymized data were extracted from the telemedicine software and compiled into an Excel® spreadsheet. (d) Statistical analysis of the data was then conducted.
Objectives
The primary objective was to evaluate the behavior and mood of patients with special needs during telemedicine dental procedures. There was no specific existing classification for this evaluation. We used the same scale than used in the previous study. 8 For mood assessment, we adapted the work of Watson et al.,9,10 which focused on measuring positive and negative effects. We proposed using eight descriptive adjectives to characterize patient behavior: four positive (“Was the patient: attentive, interested, proud, enthusiastic.”) and four negative (“Was the patient: restless, hostile, scared, nervous.”). Each adjective was assigned a score ranging from 0 to 4 for positive and −4 to 0 for negative descriptors, as outlined in Table 1.
Indicators and weighting of patient behavior and the score for each response.

Scoring system: The results ranged from −16 to +16. Nurses completed these indicators at the end of each visit using the specific software system.
Behavior evaluation: To assess patient behavior during teledentistry activities we also used the same five key questions that were developed in the previous study 8 : Does the patient fear the electric toothbrush? Does the patient bite the camera? Does the patient have difficulty keeping their mouth open? Is the patient resistant? Is the patient cooperative? These questions were selected as they were potential obstacles to the successful completion of the procedure. The fear of toothbrushes was included because the intra-oral camera resembles an electric toothbrush in appearance. The one on biting and the one on keeping the mouth open were monitored as such behaviors could negatively affect the teleconsultation and the treatment by the dentist. The resistance and the cooperation of the patient were recorded to have the feedback from the health professional who recorded the video.
These questions aimed to evaluate the acceptability of the camera usage and to anticipate potential care needs.
Time measurement: At the end of each visit, nurses were also required to record in the software the time spent with the patient. We monitored this indicator because it was always a question from the policymakers and the medico-social facilities’ director. The time spent by nurses to record data should be transferred into salary money. This indicator was very relevant.
Additional medical data collection: Other data collected in the medical record by the nurse included type of disability (psychiatric, mental, or multiple disabilities), epilepsy, bruxism, swallowing disorders, and salivation disorders.
Teledentist analysis and diagnosis: The teledentist analyzed the data and performed a diagnosis that included tooth-by-tooth diagnosis using the CAST classification, 11 presence of plaque or tartar, need for care, urgency level of required care, 12 and type of care to consider: private dentist, specialist dentist, and general anesthesia.
Additionally, the teledentist evaluated the quality of videos taken by the nurse (poor, good, or excellent) and the feasibility of the diagnosis (impossible, partial, or complete).
Facilities inclusion criteria: All medico-social institutions contracted with Montpellier University Hospital for teledentistry activities and using the e-DENT system were included. The study encompassed 27 facilities, categorized based on the type of disability/state: 4 long-term care homes for the elderly, 3 facilities for children with disabilities, facilities where people with low facilities leave, 8 medicalized reception centers for people with middle disabilities, specialized medicalized reception centers for people with high disabilities.
Patients inclusion criteria: Inclusion criteria were residency in a contracted facility and consent to teledentistry activities and the study. Exclusion criteria included refusal to consent, patient refusal despite legal representative approval, and medical team refusal due to patient health status.
Study intervention: Teledentistry procedures, as described in the introduction, were performed for all individuals within the participating facilities.
Statistical analysis
Continuous data were presented as medians with quartile ranges. Qualitative data were expressed as numbers and percentages.
The receiver operating characteristic 13 (ROC) curve is used to evaluate the performance of a binary classification model, using sensitivity and specificity. An ROC curve of the mood score for video quality prediction was drawn by plotting the sensitivity against the specificity of score results. The area under the ROC curve (AUC) was calculated along with its 95%CI was estimated. The threshold was determined with the Youden index to optimize both sensitivity and specificity. The statistical measures of the threshold performance (sensitivity, specificity) were calculated.
Mixed logistic regressions on video quality, diagnostic feasibility, behavior scores, and mixed linear regression on mood score were performed, with significant variables presented in multivariate analysis.
Statistical analyses were conducted using R (V.4.3.1)
Results
Description of the studied population: During the five-year analysis period, 682 patients received at least one telemedicine dental procedure (Figure 1). The gender distribution was 56% male (379) and 44% female (303). The patient categories were as follows: 6%) were dependent elderly persons; 10%) were children with disabilities; 4%) were adults with disabilities, of which: 4%) lived in low-disability life homes; 154 (22%) resided in medium-disability medicalized reception centers; 8%) were in high-disability specialized reception homes.

Inclusion flow.
A total of 1210 telemedicine dental procedures were performed on these 682 patients over the five years: 7.8%) had 2 telemedicine procedures; 95 (13.9% of the total and 24.1% of those who had 2) had 3; 32 (4.7% of the total and 33.7% of those who had 3) had 4; 7 (1% of the total and 21.9% of those who had 4) had 5.
The overall figures for inclusion and telemedicine procedure completion are summarized in Figure 2.

Distribution of first visits by patient profile and per year.
Medical overview
About the medical history of the patients, 144 (25.95%) had a mental disability; 263 (38.6%) were on at least one psychotropic medication; and 114 (22.94%) had diagnosed swallowing disorders.
74% (503) of the patients had not seen a dentist for over a year before their first telemedicine procedure. 12% had not seen a dentist for more than 10 years.
Visit procedure
Duration of visit
At the end of each appointment, the nurses recorded the time spent with the patient to complete the entire visit. We described the results in Figure 3.

Visit's time for the first one.
The median duration of the visits was 15 min, with the first and third quartiles being 10 and 20 min, respectively.
Behavior and mood during the visit
We observed that 62.7% (427) of the patients who received a telemedicine procedure were not resistant at all during their first visit.
The median mood score was 2.5, with the first and third quartiles at −2 and 8, respectively, among the 682 patients who underwent a telemedicine procedure. The distribution is summarized as follows (Figure 4).

Distribution of mood scores after the first act.
The average mood score varies depending on the type of facility where the patients are housed. It is negative for facilities hosting children and those for adults with severe disabilities (MAS), with scores of −0.68 and −0.92, respectively. Conversely, the score is positive in retirement homes and facilities for adults with mild and moderate disabilities, with scores of +7.25, + 2.81, and +5.43, respectively (Figure 5).

Distribution of average score based on disabilities.
It should be noted that the median visit time for patients with a negative mood score is higher than the overall median, standing at 20 min, with the first and third quartiles being 10 and 25 min, respectively.
Evolution of mood over successive telemedicine dental procedures
It was particularly noteworthy that the Wilcoxon paired test revealed a statistically significant median increase of 1 in mood score from the first to the second consultation, with a p-value <0.001 and a 95% confidence interval of [0; 2]. Similarly, the increase in mood score from the first to the third and fourth consultations was also statistically significant with an alpha risk of 5%. While the increases in mood score from the second to the third consultation, and from the third to the fourth, were not statistically significant, they nonetheless indicated a clear upward trend (Figure 6).

Evolution of mood score based on the number of procedures performed over 5 years.
Relationship between patient mood, visit duration, video quality, and diagnostic feasibility
The analysis of visit duration per patient, their mood score, and the feasibility of diagnosis by the teledentist indicated that an increase in mood score corresponded to improved diagnostic feasibility (Figure 7). Additionally, longer visit durations were associated with decreased diagnostic feasibility (Figure 8).

Distribution of diagnostic feasibility based on mood score; −1 = not feasible; 0 = partially feasible; 1 = feasible.

Distribution of diagnostic feasibility based on visit duration (minutes); −1 = not feasible; 0 = partially feasible; 1 = feasible.
To identify a mood score threshold that best discriminates video quality (“Good/Excellent” vs. “Poor”), an ROC curve is performed. The area under the curve (AUC) was 0.801 with a 95% confidence interval of [0.754; 0.849]. The threshold identified using Youden's Index was −0.5, associated with a specificity of 0.650, a sensitivity of 0.854, a positive predictive value (PPV) of 0.838, and a negative predictive value (NPV) of 0.678. So, we achieved a correct classification rate of 78.9%.
We also investigated which variables could explain the mood and behavior of patients during the visit, as well as video quality and diagnostic feasibility. Initially, a univariate regression was performed on variables that might affect the aforementioned parameters. Variables with a global p-value <0.15 in univariate were included in the multivariate model, ensuring no collinearity issues.
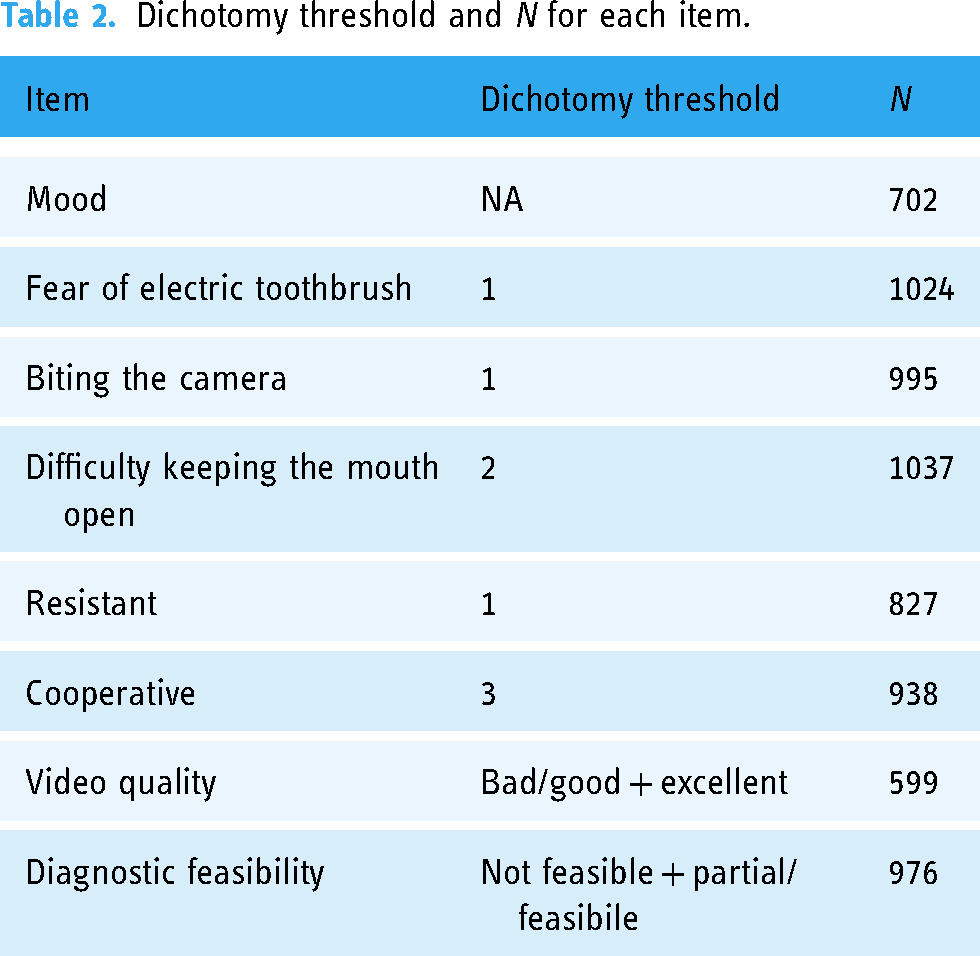
For each of the five behavior variables, the variable was dichotomized by cutting at the median of the first visit. The video quality and diagnostic feasibility variables were also dichotomized. The N for each variable varied.
All these elements are summarized in Table 2:
Dichotomy threshold and N for each item.
As an example, here is the model used for mood evaluation. (Table 3)
Synthetic table of statistic.
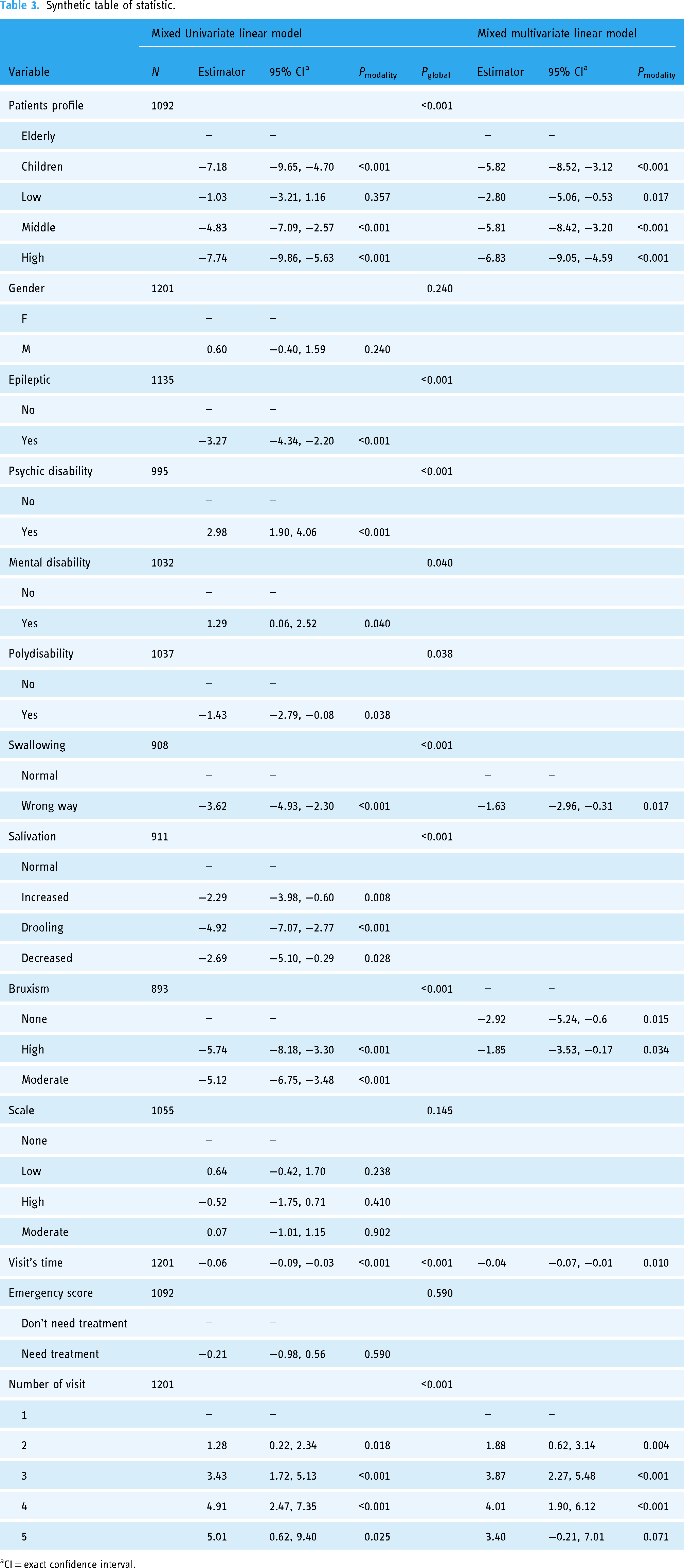
CI = exact confidence interval.
From these various analyses, it has emerged that different variables impact the studied parameters:
Type of disability/living environment: A child in an EEAP has 5.82 points less in mood score compared to an elderly person in an EHPAD. A person living in FDV has 5.81 points less in mood score compared to an elderly person in an EHPAD. A person living in MAS has 6.83 points less in mood score compared to an elderly person in an EHPAD.
When the patient had a mental disability: They had a 2.37 times higher risk of being afraid of the electric toothbrush. The quality of videos decreased by 43%. The feasibility of diagnosis decreased by 50%.
When the patient was polyhandicapped: They had a 3.61 times higher risk of having difficulty keeping their mouth open. Their cooperation decreased by 77%. The feasibility of diagnosis decreased by 84%.
When the patient had a psychiatric disability: They had a 54% higher risk of biting the camera.
Mood score: When the mood score increased by 1 point: The risk of being afraid of the electric toothbrush decreased by 18%. The risk of biting the camera decreased by 26%. The risk of having difficulty keeping the mouth open decreased by 27%. The risk of opposition decreased by 39%. Cooperation was 1.53 times stronger. The quality of videos was 1.06 times stronger. The feasibility of diagnosis was 1.08 times stronger.
For an additional minute of visit: The mood score decreased by 0.04. The risk of biting the camera increased by 1.06 times. The risk of having difficulty keeping the mouth open increased by 1.02 times. Cooperation decreased by 5%. The quality of videos decreased by 3%.
When the patient had a swallowing disorder: Their mood score decreased by 1.63 points. They had a 2.61 times higher risk of being oppositional. The quality of videos decreased by 40%.
When the patient was afraid of the electric toothbrush: The feasibility of diagnosis decreased by 53%.
When the patient had difficulty keeping the mouth open: The quality of videos decreased by 51%. The feasibility of diagnosis decreased by 48%.
When the patient was oppositional: The quality of videos decreased by 50%.
When the patient required care: The risk of opposition decreased by 64%. Cooperation was 2.25 times stronger.
A person with significant bruxism had 2.92 points less in their mood score. A person with moderate bruxism had 1.85 points less in their mood score.
This study evaluates the impact of different disabilities and living environments on mood scores and teleconsultation parameters using tools like electric toothbrushes and intra-oral cameras. Children in specialized educational support facilities (EEAP) and adults in foster homes for disabled individuals (FDV) record significantly lower mood scores, 5.82 and 5.81 points, respectively, compared to elderly individuals in nursing homes (EHPAD). Those residing in specialized medical assistance facilities (MAS) experience an even greater decrease in mood scores, amounting to 6.83 points below those in EHPAD. The study further reveals that mental disabilities increase the risk of fear toward electric toothbrushes by 2.37 times, decrease video quality by 43%, and halve the feasibility of diagnosis. Multiple disabilities exacerbate difficulties in keeping the mouth open by 3.61 times, severely hinder cooperation, and drastically reduce diagnostic feasibility by 84%. Additionally, psychiatric disabilities significantly raise the likelihood of patients biting the camera. Mood improvements correlate with decreased behavioral challenges and enhanced cooperation and diagnostic capabilities, underscoring the importance of mood management in teleconsultation settings.
A person making a second visit had 1.88 points more in their mood score. A person making a third visit had 3.87 points more in their mood score. A person making a fourth visit had 4.01 points more in their mood score. A person making a fifth visit had 3.40 points more in their mood score.
Discussion
This initial study on the impact of mood quality and patient behavior during a telemedicine oral and dental procedure highlights several intriguing findings. Firstly, in the organizational dimension of such a program implemented in medico-social structures, and secondly, in identifying influential parameters on diagnosis execution and patient experience.
A well-accepted practice by individuals with specific needs: We observed that only 5.3% (Figure 1) of attempted visits could not be completed due to a lack of patient cooperation. Considering that telemedicine activities were conducted with a population of individuals with specific needs, it is natural to view this low percentage as a success. It is worth noting the 12.8% of individuals who were considered “very” oppositional during the nurse's visit. On the other hand, 62.7% were classified as “not at all oppositional,” and 41% were identified as “very” cooperative. We can conclude that telemedicine in oral and dental care seems to be well-accepted by individuals with specific needs. Interestingly, 25.7% seemed to be “very” proud of having undergone a telemedicine examination. Nurses reported that this sense of pride among patients was an argument to convince those who were less motivated to participate. 14
The mood score used in this study indicates that telemedicine in oral and dental care appears to be better appreciated by elderly individuals living in nursing homes (+7.25) as well as by individuals with mild or moderate disabilities (scores of +2.81 and +5.43, respectively). Even for children with disabilities and individuals with severe disabilities, the mood score is not extremely low, as it is just above −1, with a maximum minimum of −16.
Unfortunately, it is impossible to objectively compare the difference in patient mood during a telemedicine procedure versus a “traditional” face-to-face oral and dental examination, as there is no literature evaluating this. However, a study examined the deployment of telemedicine in oral and dental care in medico-social structures and found that patients seemed more comfortable with nurses than with dentists who visited the facilities because they knew them and were known by the nurses. 14
Familiarity with this practice by individuals with specific needs shows a real improvement in the acceptability of telemedicine in oral and dental care, with a significant increase in mood score when patients receive multiple procedures over time (Figure 6). This suggests that as telemedicine activities continue to develop, individuals are likely to become more accepting, as is often the case in this population. 15
The identified visit duration in our study does not seem excessive, considering the specificity of the patients. A median of 15 min seems reasonable (Figure 3). A Brazilian study shown that the average time of an oral consultation in primary care is 24,39 min. 16 So, even if we had the average time of 8 min that the “teledentist” need to analyze the video 3 the time needed for a teleconsultation on a patient with specific need is shorter that a face-to-face consultation on general patient. It is important to understand that these 15 min encompass the entire visit, not just the time spent recording images. This time includes patient preparation, information gathering, and video recording.
It is also interesting to note that when the visit duration increases, it has a negative impact on the mood score and video quality. We think that it is due to poorer cooperation and a higher risk of biting the camera and experiencing difficulty in keeping the mouth open. This is confirmed by Figure 1, which shows that the median visit duration for patients with a negative mood score increases to 20 min, and Figure 7, which shows that diagnostic feasibility is higher when the visit duration is short.
Our study showed that a mood score of −0.5 is the threshold at which video quality transitions from “good” or “excellent” to “bad.” We also identified that when the mood score increased by 1 point: The risk of biting the camera decreased by 26%; The risk of having difficulty keeping the mouth open decreased by 27%; The risk of opposition decreased by 39%; Cooperation was 1.53 times stronger; Video quality was 1.06 times better; Diagnostic feasibility was 1.08 times better. The mood score could serve as a filter for conducting the visit, especially for video recording. Evaluating the mood score before capturing videos could determine whether it is appropriate to proceed. If the mood score is less than −0.5, there is a 78.9% chance that the recorded videos will be “bad.” Furthermore, the risk of biting the camera will be higher, and diagnostic feasibility will be lower. Therefore, calculating this mood score before video recording during the preparation phase or when initial attempts to insert the camera into the patient's mouth result in a mood score below −0.5, it might be wiser to postpone video recording to a time when the person has a higher mood score and, thus, greater cooperation.
Similarly, in the context of deploying telemedicine across a territory, it appears that some facilities are more conducive to rapidly achieving positive results in telemedicine procedures. This is due to the most frequently encountered types of disabilities in these facilities. Indeed, nursing homes, FAMs, FDVs, and ESATs have higher mood scores. However, we should not exclude EEAPs and MASs from such programs because, even though they have moderately negative mood scores, patient adaptation could lead to quality videos and smooth diagnostic procedures with telemedicine in oral and dental care.
By considering broader elements than just cavities, edentulism, and periodontal pathologies, we observed associations with visit completion. One surprising finding is the link between individuals with swallowing disorders. Our study revealed that their mood score decreases by 1.63 points compared to those without swallowing disorders. Likewise, they are 2.61 times more likely to be oppositional, which impacts video quality as it decreases by 40%. We attempted to understand why swallowing disorders have such a significant impact on telemedicine activities. Analysis of the literature suggests that swallowing disorders are closely related to poor oral health, 17 but we did not find a clear link between swallowing disorders and difficulties in accessing the mouth.
Similarly, we found that individuals with significant or moderate bruxism had significantly higher mood scores, by 2.92 and 1.85 points, respectively, compared to non-bruxism patients. We believe that the muscle and dental pain caused by bruxism 18 could explain this, as well as the nervous and/or anxious state that typically leads to bruxism, 19 which could account for the lower mood score.
Finally, our study also showed that individuals in need of care were less oppositional and even 2.25 times more cooperative. This suggests that even individuals with mental, psychological, or psychiatric disabilities may feel the need to cooperate in order to receive care.
Conclusion
These results suggest that telemedicine in oral and dental care can be effective for individuals with specific needs, but factors such as the type of disability, mood score, and visit duration should be considered to ensure the success of remote examinations. This study provides valuable insights for improving telemedicine in oral and dental care and could contribute to the implementation of best practices for managing individuals with specific needs in this field.
Footnotes
Acknowledgments
The authors would like to thank Ms. Célia Vidal and Ms. Fanchon Herman for their invaluable assistance in statistical analysis, as well as all healthcare professionals involved in the field of telemedicine in oral and dental care across various medico-social institutions.
Contributorship
Camille Inquimbert: performed analysis and wrote the paper; Céline SABOURIN: performed analysis; Nicolas Sepashvili: collected the data and performed analysis; Jean Valcarcel: conceived and designed; Abid Bossouf: performed analysis; Nicolas Giraudeau: conceived and designed, collected the data, performed analysis, and wrote the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding from Regional public health agency, University Hospital of Montpellier, and University of Montpellier.
Guarantor
NG