
Abstract
Objective
As the world faces an aging population, the complexities of care management become increasingly pronounced. While technological solutions hold promise in addressing the dynamic demands of care, many nuances are to be considered in the design and implementation of active and assisted living technologies (AAL) for older adult care. This qualitative study, set in southern Spain, is positioned at the crossroads of healthcare challenges, as seen by the different actors involved in the care process and the technological solutions developed in response to these challenges. By investigating the complex landscape of caregiving and by examining the experiences and challenges faced by caregivers, healthcare professionals, and older adults, we aim to guide the development of vision-based AAL technologies that are responsive to the genuine needs of older adults and those requiring care.
Methods
A qualitative research methodology was used in the study. In total15 in-depth interviews and five focus groups were conducted with a diverse group of stakeholders involved in the process of care provision and reception.
Results
While the results demonstrate that there is a readiness for technological solutions, concerns over privacy and trust highlight the need for a carefully integrated, human-centric approach to technology in caregiving.
Conclusion
This research serves as a compass, guiding future discussions on the intersection of aging, technology, and care, with the ultimate goal of transforming caregiving into a collaborative and enriching journey for all stakeholders involved.
Keywords
Introduction
The relentless pace of the modern world, characterized by informational overload and rapid societal changes, has led to profound transformations in our lifestyles, mental processes, and behaviors. These changes present new challenges associated care requirements. The confluence of these factors demands a comprehensive reevaluation and restructuring of care processes to meet the evolving needs of an aging population.
In response to these complex challenges of caregiving, technological solutions have emerged as promising avenues and necessitate the establishment of novel norms. 1 A crucial component of this adaptive process is the ongoing demographic shift, as both the share and the number of older persons in the total population are growing rapidly. 2 Yet, with the growing need for care services for older people, we have fewer human caregivers available to meet this demand. 3 Moreover, alterations in family structures challenge traditional notions of care as well as aging and the for addressing the evolving demands of care. Among these solutions, active and aassisted living (AAL) technologies have gained attention for their potential to empower older adults to maintain independence, well-being, and overall quality of life, as well as address loneliness.4,5 Additionally, AAL technologies seek to alleviate the caregiving challenges of both professional and family caregivers. 6 Leveraging advancements in computer vision and artificial intelligence, visual components of these technologies have significantly strengthened their effectiveness due to their capacity to capture situations and movements in a focused and natural manner, providing comprehensive information that plays a pivotal role in detecting and preventing falls and emergencies.7,8 While computer vision-based technologies (e.g. video-monitoring systems) can accomplish more elaborate tasks, like recognizing activities, detecting emergencies, and providing elaborate digital care plans, 9 they come with their drawbacks. First, these vision-based systems bring up major concerns about people's privacy. 10 Hence, it is crucial to acknowledge these substantial privacy concerns and trust issues associated with their use in private spaces, given their potential to gather data that could be misinterpreted by unauthorized individuals. 11 Moreover, these systems are criticized for their mechanistic nature, often designed from a technologist's perspective to address specific problems without a holistic understanding of caregiving contexts, the larger ecosystem, and the comprehensive needs of the aging population.12,13 In line with this, a significant oversight in the design of AAL technologies is that they often do not fully consider the viewpoints of the people who will be using them, especially in the case of newer camera-based monitoring technologies. 14 As a result, although assistive technologies (AT) have the potential to cater to care requirements, a disconnect exists between these technologies created for older individuals and what older users really need. 15 Additionally, caregiving contexts and ecosystems exhibit substantial variability across different cultures and specific circumstances, necessitating a nuanced approach that acknowledges these differences. Because of these obstacles, it is crucial to shift to a different approach in designing technology. Instead of starting from a technical perspective and working downwards, we should start from the ground up. Older individuals possess a wealth of life experiences and knowledge that significantly influence their interaction with and utilization of AT. Designers face the challenge of tapping into this experience and knowledge to craft solutions that meet the specific needs of older adults. 16 The imperative arises to adopt a bottom-up approach to technology design, one that seeks to enrich our comprehension of the care of older adults, the complexities of the caregiving process, and the unique demands of care within each context.
For this reason, the objective of this paper is to deepen our understanding of caregiving contexts, problems and needs for older adults and those requiring care. With our research team consisting of social scientists and technologists, we seek to bridge the gap between technological aspirations and the real needs of people from the healthcare sector. Therefore, based on the insights of different care segments, we aim to provide valuable insights to technology developers and offer design recommendations for the development of vision-based AAL technologies.
To achieve this goal, the paper will address two primary sets of research questions:
What are the principal challenges and needs encoun- tered in the care process of older adults; Which emer- gency detection can provide significant benefits in the caregiving context? What are different stakeholder experiences with technology use, particularly in the context of camera-based care monitoring technologies, and what recommendations do users have for the development of such technologies for senior care?
By addressing these questions, this paper seeks to illuminate the complexities of caregiving, user perspectives, and the evolving technological landscape, ultimately guiding the development of vision-based AAL technologies that are responsive to the genuine needs of older adults and those requiring care.
Methods
In order to investigate different user perspectives on the needs and challenges of the care process, as well as their experiences with assistive technology, we employed a qualitative research methodology, in-depth interviews, and focus groups with a diverse group of stakeholders involved in the process of care provision. The triangulation of focus groups and in-depth interview methods was used with the healthcare segment representative participants of the study.
The research was conducted following the qualitative research guidelines, consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups by Ref. 17 The checklist is given in the appendix section of the paper. The manuscript was developed according to the Standards for Reporting Qualitative Research: A Synthesis of Recommendations by O’Brien et al. 18 The necessary permissions to use the instruments employed in the study were obtained.
The study's procedures were conducted with ethical considerations at the forefront. All study procedures received ethical approval from the University of Alicante Ethics Committee (Ethical Approval UA-2022-10-16-1).
The sample
We conducted 15 in-depth interviews and five focus groups, with a total of 46 individuals participating in the study. Each focus group consisted of six to seven individuals.
The recruitment of participants was facilitated through the collaboration of a healthcare professional, a case manager of a local healthcare center in the southeast of Spain. A combination of theoretical and snowball sampling techniques was employed for participant recruitment. Tentative profiles were created from the three diverse groups involved in the care provision process: older adults, family caregivers, and healthcare professionals, in a way that ensured a representation of a diversity of participants from care-receiving and caregiving segments. These initial participants then referred us to others who were relevant to the study, continuing until we achieved theoretical saturation of the obtained data.
Care-giving sector. The participants representing the care- giving sector in our study included family caregivers and healthcare professionals, totaling 36 individuals (see Table 1). We conducted a total of 13 interviews and four focus groups with these participants. Table 2 displays details of the composition them. Participants’ roles within the care provision process were diverse, encompassing private caregivers, nurses, case managers from healthcare centers, psychologists, heads of care homes, social workers, and nurse coordinators. These parties within the care provider segment brought diverse levels of experience in the care sector.
Sociodemographic characteristics of the family caregivers and healthcare professionals (N = 36).
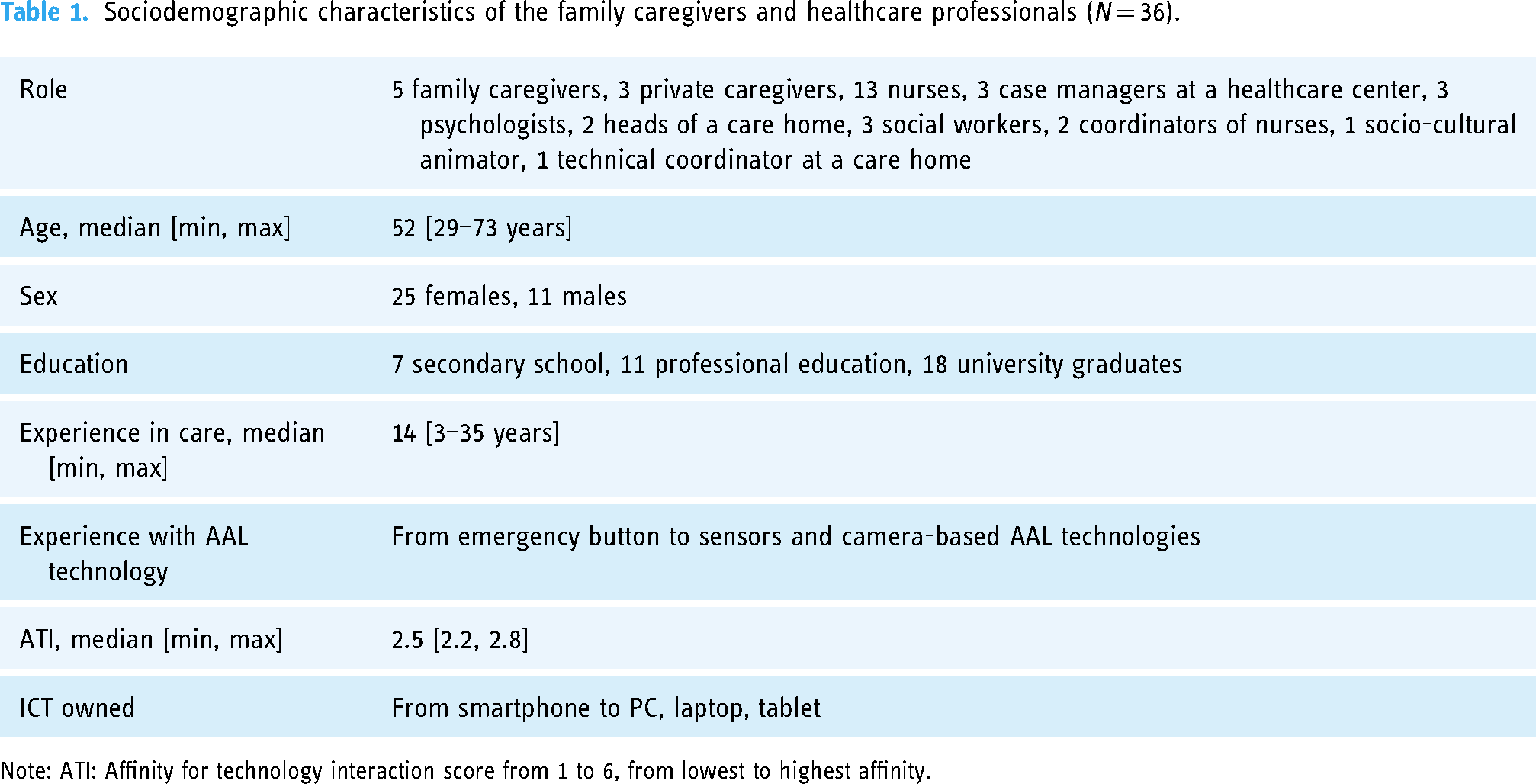
Note: ATI: Affinity for technology interaction score from 1 to 6, from lowest to highest affinity.
Composition of interviews and focus groups.

Together with other characteristics, we assessed their affinity for technology using the affinity for technology interaction scale (ATI), ensuring a comprehensive representation of diverse technological backgrounds among the study's participants. The ATI score spans from 1 to 6, signifying the spectrum of affinity for technology, ranging from the least to the highest level of affinity. 19 We employed a translated and validated version of the ATI scale tailored for the Spanish context. 20
Care receivers A focus group was conducted with six older adults living in a care home in a small town in the southeast of Spain (Table 2). One senior participant did not wish to sign the consent form, therefore their data were discarded from the study. The sociodemographic profiles of the remaining five participants of the focus group are represented in Table 3.
Sociodemographic characteristics of the senior participants of the study (N = 5).

Note: TechPH: Older people's attitudes toward technology score from 1 to 5, from lowest to highest technophilia. CDS: Care Dependency Scale, CDSsumscore ≤ 68 were classified as care-dependent, all others as independent.
As part of the sociodemographic characteristics, we also gathered information about the senior participants’ previous experience with AAL Technologies, their general attitudes towards technology (TechPH), their ownership of Information and Communication Technologies (ICT owned), and their level of care dependency (CDS). The TechPH (Older People's Attitudes Toward Technology Score) is an innovative tool designed to gauge the technological attitudes and enthusiasm of older individuals. It draws inspiration from established instruments used to measure technophilia. 21 The TechPH Score ranges from 1 to 5, with higher scores indicating a greater enthusiasm for technology. On the other hand, the Care Dependency Scale (CDS) measured the participants’ level of care dependence. 22 Those with a CDS sum score of 68 or lower were classified as care-dependent, while others were considered independent. Researchers employed a translated and validated version of the CDS tailored for the Spanish context. 23 However, the TechPH measure had to be translated ad hoc into Spanish specifically for this study.
The study procedure
We conducted visits to all study participants in their chosen settings. For senior participants, this meant their living space—a care home, while for the remaining participants, it included their work environment or a designated work cafe. In total, we collected data from three distinct care homes and four healthcare provider centers during the study.
The in-depth interviews, as well as focus group procedures, started by informing the participants about the study's purpose, providing them with an information sheet, and signing the consent form. Following this, participants were requested to complete a demographics questionnaire. This preliminary process set the stage for the core of the interview or focus group discussion, where participants delved into the study's central themes.
Interviews and focus groups were conducted by the first author of this paper (a female researcher), with the help of two additional moderators for the focus groups. The researcher's occupation at the time of the study was a PhD candidate, with MA and PhD training, resulting in 5 years of research experience.
Data collection guides. The data collection guides, which included interview and focus-group guides, covered a demographics questionnaire and were structured around four main themes: care process (challenges in the care provision/reception, needs, main emergencies, etc.), previous experiences with assistive technologies (knowledge and perceptions about AAL technologies), camera-based technology (attitudes, privacy perceptions), and future directions (recommendations and ideas for the design of assistive technologies).
The interview guides were structured to provide a comprehensive exploration of each topic, incorporating detailed questions that fostered in-depth inquiry and a profound understanding. In contrast, the focus group guide featured overarching themes that encouraged dynamic discussions among the group of participants.
Data analysis
We began analyzing the data by coding and categorizing information into themes. During the data collection process, we engaged in ongoing analysis, initially identifying basic main themes as starting points. As more data were collected, it was continually compared with existing data. This comparison helped us refine and modify existing categories and develop new ones. Throughout this iterative process, we monitored the progress towards data saturation. Saturation was considered achieved when additional data no longer introduced new insights or influenced the coding tree, indicating that the dataset was sufficiently comprehensive to reflect key themes and patterns. The determination of theme saturation involved continuous comparison across data points and among team members until no new categories or codes emerged from subsequent data.
The final data analysis was conducted under a thematic analysis framework, utilizing inductive coding to systematically categorize and tag all information in the transcripts. 24 This process began with the creation of detailed descriptive codes, which were progressively grouped into overarching categories. This eventually led to the development of a comprehensive coding tree. Codes were grouped based on their semantic relationships, and we actively searched for common patterns that aligned with our research questions. Each theme was discussed and refined through collaborative team meetings, ensuring that interpretations were consistent with the data and reflective of diverse perspectives within the team. This process continued until consensus was reached on category naming and organization.
Unfortunately, participants were unable to provide feedback on the collected and analyzed data after the data collection phase.
Results
Each interview or focus group session typically spanned a duration of 45–90 min, with the shortest in-depth interview clocking in at 37 min and the longest focus group session extending to 102 min. The focus groups were moderated by a team of at least two researchers, while one of the researchers took the lead in conducting the in-depth interviews. All sessions were audio-recorded and transcribed verbatim. Field notes were also documented by the interviewers during and immediately after each session.
Four participants’ data were discarded due to incompleteness, and one participant in the focus group did not wish to sign the consent form. Therefore, the results of the study reflect the data of 41 participants in total, divided into 13 in-depth interviews and five focus groups, with five to six participants in each focus group.
We now present our findings by first focusing on the senior needs and problems in the care process from their own perspective as well as from the viewpoint of other stakeholders involved in the provision of care. We then present participants’ insights into their experiences of AT use and recommendations that they have for the development of such technologies.
Challenges and needs in care
Problems in care management. The interviews and focus groups revealed several challenges in the practical aspects of care management. Health professionals often face the dilemma of reconciling the demands of both older adults and their family members. A case manager (P11) shared their observation: “There is already a difference between what a caregiver demands and what a patient demands. You need to tell them that your mother is asking me for this, but you are telling me no to this, so what I do is a little bit of an intermediary between the two people.” On the other hand, senior participant FG5 (older adults) emphasized the need to have agency over managing his life: “Maintaining a sense of control in my life is essential. I need to decide for myself. It gives me a sense of purpose and dignity.” According to the participants, this disconnect between the expectations of family caregivers and patients can complicate the caregiving process and the appreciation of multiple perspectives is necessary.
In care homes, the gap between theory and practice becomes evident as caregivers confront the challenge of providing care to individuals who might even resist basic activities like bathing. A nurse in a care home (P1) reflected on the complexities of real-world caregiving, emphasizing that “Practice is one thing and theory is another, the theory is very nice, but then, in practice, in 15–20 min, you cannot wash a person with dementia if that person does not want to be washed and is like no, no, no, no.”
Moreover, against theoretical advice, physical restraints are occasionally employed in care homes to manage agitated individuals, as described by several healthcare professionals: “In theory, we should not use physical restraints, but then, in reality, you wonder how can we remove them, it is simply not possible, we do not have any other way for some residents,” FG3 (healthcare experts of a care home).
Another example highlighting the disconnect between theoretical ideals and day-to-day caregiving is seen in personalized care plans. These plans aim to address the unique needs of each resident in a care home, emphasizing individualized, person-centered care for enhanced well-being. However, in reality, challenges such as staff shortages and time constraints can hinder the implementation of truly personalized care. Residents may receive more generalized care due to these practical limitations.
Additionally, a significant concern was raised about the lack of follow-up in care management, which can lead to issues in providing continuous care and support for older adults: “Perhaps the lack of follow-up. Ah, I believe that it's the biggest problem in care management,” P10 (a nurse in a health center). Furthermore, it is important to note that the results demonstrated substantial consensus among participants from the healthcare segment across both focus groups and in-depth interviews.
The shortage of caregivers, particularly in nursing homes, and curiosity for the technologies were acknowledged by several participants from the healthcare sector: “There is no one there at night, I go for 3–4 h, and the rest of the time they are alone, but they require monitoring for 24 h,” P8 (private caregiver), but also interestingly from older adults: “The fewer children are born, the more and more older people are there. And then fewer people want to work in nursing homes. I want to see if there would be technologies that could help improve the care, right, I want to see,” FG5 (older adults).
This alignment of views across different segments of the healthcare sector underlines a shared recognition of the challenges in caregiving and a collective interest in exploring technological solutions to address these issues.
Emotional underpinnings of aging. The interviews and focus groups highlight a significant deficiency in social sensitivity towards aging, which has a profound impact on both older individuals and their caregivers: “There is a lack of social sensitivity to aging. It is very hard for the older person and for the caregiver, especially when the caregiver is a relative, with affection, and love… it destroys your life,” P7 (caregiver of their mom). This lack of sensitivity is a shared sentiment among participants, described as emotionally distressing for all the parties involved.
In line with this, data demonstrates that older adults may be reluctant to communicate their needs or concerns, which can lead to undetected issues: “His sister took care of him. But he did not want to wake her up or ask for help,” FG4 (healthcare professionals). P8, a private caregiver, explained that older adults often downplay their condition, concealing their true needs and health status: “She once fell by herself and did not tell anyone, she is a woman who always said I’m fine, I’m fine, when her daughter asked she said she was fine, but the truth was she was not fine.”
An interview with an older adult (FG5) also revealed a concerning moment when she was not feeling free to open up and share her vulnerabilities with us, instead when asked about her needs in the care management process and if she was experiencing any challenges, she continuously repeated: “…here they are taking care of me very well, very well, I can’t say anything bad about how they care for me, I don’t have any problem or complaint.”
Stress and feelings of guilt also emerged as recurring themes, mostly among older adults and family caregivers: “I dońt want to be a burden, I told them [his adult children] immediately I wanted to go to the residence, they have their lives….” P4 (caregiver of their dad) shares the emotional toll of providing care to a loved one: “You constantly worry and feel guilty for not being able to provide the attention their loved ones need, or that they might need more care than you can provide….”
Family caregivers, as mentioned by P3 (caregiver of their mom), juggle multiple responsibilities, including their own households, which can significantly contribute to their stress levels: “I also had my house, my family, so it has been very difficult to manage, and I felt guilty. And I was always always worried about the falls. And then, one of the things that was most challenging for me, at least, was controlling my emotional state, my anxiety. Because you can’t sleep well at night, you’re worried, stressed, because everything becomes more complicated, you’re always worried that there might be some issue, some emergency.”
On the other hand, insights from a private caregiver (P5) shed light on a major concern among older adults—the feeling of being futile and unvalued, which can wind into depression due to perceived neglect by their families: “The major problem is that older adults do not feel useful, which leads to depression due to a lack of affection from the family,” P5 (private caregiver).
Care emergencies. The interviews also shed light on vari- ous emergencies that caregivers and healthcare professionals need to be vigilant about. Falls emerged as the prominent issue: “…She fell and I was responsible. I had to clean her floor, so she sat on the chair and I went to clean the floor and she fell, I felt very bad, I felt guilty. And then I was always on top of her so she wouldn’t fall,” P8 (private caregiver). Care home nurses also acknowledge that falls are the main emergencies they face: “Falls, falls are a major problem, they are inevitable… a care home cannot assign a dedicated nurse to follow each person,” FG1 (care home nurse).
Wandering and escape poses were among the emergencies that challenged family as well as institutional caregivers: “He used to go out on the street and get lost. It caused me a lot of distress,” P2 (caregiver of their husband). Blood pressure fluctuations are another medical concern that caregivers and healthcare professionals should monitor closely: “I think, a drop in blood pressure mm and a loss of consciousness, we need to watch out for,” P12 (case manager of a healthcare center).
Moreover, the interviews touch on issues of aggression: “… Fights too, aggression. By a part of residents among themselves and towards the sanitary personnel,” FG2 (care home nurse). However, no aggression or mistreatment issues were raised towards the care receivers during the data collection, neither by healthcare professionals nor by the older adults themselves.
Domestic accidents within care settings were named as another important emergency situation, further emphasizing the need for comprehensive emergency detection and response strategies: “For example, once the gas was left on, with no fire, just the gas on, and that gave us such a scare,” P4 (caregiver of their dad).
Video-based assistive technology: experiences and recommendations
Knowledge and experiences. The interviews revealed a diverse range of knowledge and experiences with assistive technological systems. Care home nurses from the FG2, express frustration with outdated systems, highlighting the need for technological advancement: “But it is the same system that they put 20 years ago. We do not have GPS or anything.” In contrast, a health center case manager (P11) acknowledges that some families have embraced even camera-based technologies: “I have a lot of patients who have cameras because the family goes to work and so on, and they have more safety, and they have normal cameras, and they don’t worry about privacy; it's already family, it's a family circuit, and they don’t usually worry about it.”
Additionally, a family caregiver of their husband (P2), reflects on the practical benefits of camera usage in her personal experience, describing how it offered peace of mind: “I put a camera, to watch my husband. When I was running out to do groceries, I would look at the camera on my cell phone. It's very useful; I went out calmer, much calmer.” On the other hand, an older adult from FG5, revealed a limited awareness of available assistive technologies, indicating a potential gap in knowledge: “Do you know of any assistive technologies for seniors? What I know of is a phone with larger than normal keys and this string which I can pull to call the nurse, that is it,” FG5 (older adults).
Advantages of video-based care monitoring. Participants acknowledge several advantages of video-based care monitoring, particularly emphasizing safety and continuous care: “The advantages I see in this technology are safety, which is the main one, and continuous care. The biggest problem is follow-up and continuous care. In this case, we can do continuous monitoring because there is this camera and there is a nurse in charge of the person who can check things, can see how things are going,” P10 (nurse the health center).
The ability to monitor an individual's daily life and well- being offers reassurance to caregivers and family members is another of the advantages: “I see many advantages, especially for a person who lives alone, because this way you can see how her day-to-day life is going. You can know when she is at her worst, know if she is eating well, if she is being well cared for, if she has any mobility problems, etc.,” P6 (caregiver of their mom).
For family caregivers, these technologies can significantly reduce anxiety and worry: “I would put cameras if I could, it would help so much my anxiety and worries. But we didn’t have the chance,” P3 (caregiver of their mom). Participants from the caregiving segment appreciated the visual element of monitoring: “They have this emergency button, but it is better to see if something has really happened and nothing has happened,” P5 (private caregiver).
Control vs. proof of good work, or control vs. safety. The interviews also highlight the complex interplay between the desire for control, proof of good work, and safety. Some participants note that camera-based monitoring could provide evidence of the quality of care provided: “Sometimes I would even prefer that they record me, because it's the only way to show the work that I people do,” FG4 (healthcare professionals). They view cameras as a means to ensure accountability and transparency, as the footage could serve as a record of the care delivered: “Cameras would be good, they would be safer, and the family would see what had happened,” P9 (private caregiver).
In contrast, P6, a family caregiver offers us the flip side of the coin, how installing cameras in a trusted environment can actually offend private caregivers: “We had a chance to have cameras, but we didn’t want to install it, more than anything else, thinking of the other person. We always had a carer with my mother, and we didn’t put cameras because we thought it might offend the caregiver, whom we had always trusted. It's like you’re saying to the caregiver that there's something here that doesn’t add up for me,” P6 (caregiver of their mom).
Therefore, it is essential to obtain a balance between control and privacy, as emphasized by participants. Some express reservations about excessive control, particularly if it primarily serves to monitor workers rather than to ensure the safety and well-being of older adults. The sentiment is clear in the words of a care home nurse (FG2): “It depends, of course, it depends on the purpose. Yes, if the purpose is to provide greater security for the residents yes. As long as it is something with data protection and privacy of the resident. But if the purpose is the control of the workers. I refuse it, I refuse it!.”
In line with this P1 (nurse in a care home), believes that people would prioritize the security and safety of older adults over concerns about privacy, suggesting that the primary focus should be on the well-being of older people: “I think people would value safety over privacy, given this is the end goal for the system.”
Disadvantages and concerns. While the advantages of camera-based care monitoring are evident, several participants express reservations regarding privacy and trust. A senior participant (FG5), voices concerns about the invasion of privacy, and trust: “I don’t want anyone to see the camera because that is an invasion of my privacy. I would never be sure, because it is technology, and 100 percent you never know who will see it.”
The security of camera-based systems is stated as a crucial concern. A senior participant (FG5) highlights the importance of knowing where one's data is going and the potential implications of entrusting it to private or public companies. Privacy, in this context, is a fundamental consideration: “For me, privacy is very important here. I am giving my privacy to a private company, to a public company. Who am I giving it to, huh? Because it's still my my my privacy.”
Ensuring the privacy and dignity of older adults is a shared responsibility among caregivers and healthcare professionals. A health professional from a care home (FG3), emphasizes the need to maintain an individual's privacy during care activities as well: “I always tell myself and my colleagues, that they are individuals and we have to maintain their privacy. If you wash them from the waist up, they have to be covered from the waist down. And the other way around. Because this way, they don’t feel naked. And you don’t have to humiliate that person.”
Misinterpretation of camera footage is another concern. A healthcare professional (FG4), mentions that the context of interactions may not always be accurately reflected in the footage, potentially leading to misunderstandings. Thus, the interpretation of video recordings can be subjective: “Maybe I have a close relationship with the senior, and we’re joking in a way. But if you see it on camera, you might think you’re mistreating the person, so then it depends on the interpretation of the video.”
Recommendations. Participants in the study offered a range of recommendations for enhancing camera-based care monitoring technologies. These suggestions focused on improving the overall care experience through greater understanding and emotional support, as well as tailoring the technology to meet individual needs and preferences.
A caregiver (P7) emphasized the importance of empathy and emotional support: “Empathy and emotional assistance play a vital role in improving the care experience, so more studies, understanding, and emotional support are needed for older persons.”
The ability to tailor camera settings to individual needs and preferences is also suggested as a valuable feature: “Yes, for example, if the camera can tell you if someone gets up from their bed and maybe to adjust these activity alarms according to the specific needs. That's why we’re here asking,” FG2 (care home nurses). “Depending on the room, can the camera set different configurations for each room?” was inquired by a health professional for a care home (FG3). Another healthcare professional (FG4), wished for activities for exercising cognitive and physical abilities: “There are these games for cognitive or physical skills, ones for memory or things like that, it would be great to integrate them in the system.”
Importantly, the cost and the simplicity of the system were seen as the main determinants for accessibility: “So, the cost of course, the cost should be accessible, and it shall also be technologically simple,” FG1 (care home nurses).
Establishing trust is crucial when introducing camera-based care monitoring systems. A case manager of a health center (P13) suggested that such systems should be introduced by healthcare professionals who already have a trusted relationship with the individuals involved: “This system is worth it, but should be introduced by a health professional because a relationship is already established. If that comes outside from someone they don’t know, it would not be trustworthy.”
Discussion
Senior care management is a nuanced and complex process. This paper delves into the challenges and experiences faced by caregivers, healthcare professionals, and older adults, shedding light on the multifaceted aspects of care management and the potential use of assistive technologies in this process. Through focus groups and in-depth interviews, we explored the complexities of practical care management, the emotional underpinnings of care, and the evolving landscape of assistive technology. This comprehensive examination seeks to uncover insights that can inform the development of more effective caregiving practices using AT. The complexities of practical care management present a multitude of challenges, ranging from the delicate balance between the needs and wishes of older adults and the ones of caregivers to the gap between theoretical ideals and real-world caregiving practices as shown in the literature 25 as well as in our study. Additionally, our findings indicate that care homes further amplify the gap between theory and practice and highlight the need to address systemic issues in care homes, such as staffing levels and resource allocation, to bridge the divide between theoretical goals and practical challenges in providing person-centered care.
In line with this, the increasing shortage of caregivers, both family and professional, emerges as a common concern. The demographic shift towards an aging population and a decreasing workforce compound these challenges, demanding a paradigm shift in caregiving practices as illustrated by Lester et al. 26 On the other hand, in accordance with our findings, the acknowledgment by healthcare professionals and older adults alike of the growing need for technological solutions highlights the readiness for AT implementation.
However, on the other side of this story is the emotional underpinning of care and aging, which has the potential to create an even bigger “age-based digital divide” as presented by Neves et al. 27 Our study exposes a significant deficiency in societal sensitivity towards aging, just as reflected in the literature. 28 argue that ageism plays a substantial role in the production of inadequately designed technologies for older adults. Addressing the lack of social sensitivity and fostering technological inclusiveness requires a broader societal shift in attitudes toward aging. The emotional toll exacted on both older individuals and their caregivers is noticeable in the stories shared by our participants. The call for acknowledgment and understanding from a caregiver (P7) resonates as a call for societal empathy. Moreover, the reluctance of some older adults to communicate their needs further reflects the gravity of the issue and requires a more proactive and inclusive approach to caregiving. Guilt for perceiving oneself as a burden and hence the inability to disclose their needs is a common perception among older adults, and initiatives aimed at destigmatizing aging and caregiving can play a pivotal role in fostering a more supportive and empathetic environment as also explored by Pedroso et al. 29 In accordance with the literature, stress and guilt emerge as recurring themes among all participants, painting a vivid picture of the emotional burden shouldered by seniors as well as family caregivers. The perpetual worry and guilt expressed by a caregiver (P4) reflect the need for comprehensive support systems that extend beyond the physical aspects of care. In line with this, the autonomy of seniors emerges as a crucial component, aligning with the societal shift towards person-centered care, which emphasizes individual choices and preferences, as also pointed out by Van et al. 30
On the practical side, various emergencies during care management—falls, wandering behaviors, blood pressure fluctuations, aggression, and domestic accidents were voiced by the participants. However, falls, in particular, were highlighted as a major concern by both family and institutional caregivers, which, according to the literature, indeed is among the major carers’ concerns for older people. 31
Moreover, the need for more follow-up in care management, as voiced by a nurse (P10), points to a systemic issue, necessitating a more comprehensive approach to monitoring and support. The multifaceted nature of care management and care emergencies emphasizes the need for a versatile and adaptive caregiving system which could offer context-based flexible solutions. This opens a gateway for exploring the role of assistive technology in emergency detection and response, a very much-needed research area according to the literature. 32
Our exploration into the field of assistive technology uncovers a diverse landscape of knowledge and experiences. The frustration voiced by care home nurses (FG2) regarding outdated systems highlights the urgency for technological evolution. Simultaneously, the openness toward camera-based technologies paints a picture of technological readiness among different segments of care providers.
The advantages of camera-based care monitoring are based primarily on safety and continuous care and are contrasted against privacy concerns, a tradeoff well documented in the previous studies.33,34 Morever, the acknowledgment of privacy concerns and the potential for misuse and misinterpretation of the collected data emphasize the need for an ethical integration of technology into the caregiving context, especially as privacy still stands as the major factor and barrier to adopting assistive technologies by older adults as also demonstrated by an extensive literature review by Yusif et al. 10
The call for more studies and understanding, as voiced by a caregiver (P7), has become a crucial point for, fostering a human-centric approach to care. The importance of privacy and dignity, as articulated by participants, necessitates a robust ethical framework. Yet the privacy vs autonomy trade-off for monitoring technologies, which is well documented in the literature, 35 is also reflected in our results.
Furthermore, the potential for surveillance and the associated concerns of trust and misinterpretation pointed out by our study participants, as well as previous research,36,37 call for transparency and accountability in the design and deployment of monitoring technologies. Incorporating older adults, caregivers, and healthcare professionals in the design process ensures that the resulting technologies align with the practical, emotional, and ethical dimensions of care and that seniors have control over these technologies. 38 User-centered design principles should extend beyond functionality to encompass esthetics, usability, and overall user experience. As a response to this, new design opportunities are offered in the literature to better account for the needs of older adults, 39 together with already established engaging older people using participatory design. 16
While our study provides valuable insights, it is not without limitations. While the focus groups were conducted by a team of at least two researchers, including a native speaker from the same geographical area, the in-depth interviews were led by a single researcher. And in certain instances, the in-depth interviewer was a nonnative speaker, with full proficiency in the language, yet, this could have potentially led to overlooking certain cultural nuances.
On the other hand, the diverse yet limited sample in terms of geographical outreach—southern Spanish middle-sized urban area may not capture the full spectrum of experiences and perspectives. Future research should embrace a more expansive and diverse participant pool, considering cultural, socioeconomic, and geographical variations. The dynamic nature of technology also demands continuous exploration, and future studies should be balanced to adapt to the evolving landscape.
While the study presents a range of perspectives from various stakeholders involved in the care provision and reception process, it is important to note that the research relied on a focus group comprising older adults from a care home. Consequently, a comprehensive triangulation of perspectives from diverse care-receiver groups is absent.
Our study provides a representation of experiences and perspectives at a specific moment. However, the dynamic nature of aging and technology usage necessitates an extended approach to grasp the evolving needs, challenges, and benefits truly. Lengthy studies tracking the experiences of older adults, caregivers, and healthcare professionals over an extended period can offer invaluable insights into the long-term impact of assistive technologies.
In conclusion, our study serves as a compass, guiding the way forward in the complex landscape of eldercare. The convergence of perspectives across the healthcare segment, as revealed through the triangulation of focus groups and in-depth interviews, highlights the robustness and coherence of our findings, affirming a shared understanding within this participant group. The integration of technology, driven by empathy and a deep understanding of the human experience, holds the key to transforming caregiving into a collaborative and enriching journey for older adults, caregivers, and healthcare professionals alike. As we navigate the complex landscape of aging, caregiving, and technology, a central theme emerges—the need for a human-centric approach. Technology, while a powerful tool, should be harnessed to amplify human connections, preserve dignity, and enhance the overall quality of life for older adults. Hence, we hope our study can serve as a catalyst, sparking conversations and reflections on the intersection of aging, technology, and care.
Footnotes
Acknowledgements
We would like to thank Pau Climent-Pérez and Aida Garcia-Bixquert for their assistance in this research.
Contributorship
The first author researched literature and conceived the study and was involved in every stage of the study process and article development. The second and last authors were involved in the protocol development. The fourth and the last authors were additionally involved in participant recruitment and in gaining ethical approval. The first author wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of it.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All study procedures received ethical approval from the University of Alicante Ethics Committee (Ethical Approval UA-2022-10-16-1).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the H2020 European Institute of Innovation and Technology (grant number: 861091).
Guarantor
FFR
Appendix. COnsolidated criteria for REporting Qualitative (COREQ) Research Checklist
A checklist of items that should be included in reports of qualitative research. You must report the page number in your manuscript where you consider each of the items listed in this checklist. If you have not included this information, either revise your manuscript accordingly before submitting or note N/A.
Developed from: Tong A, Sainsbury P and Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007; 19: 349–357.
Topic
Item number
Guide questions/description
Reported on page number
Domain 1: Research team and reflexivity
Personal characteristics
Interviewer/facilitator
1
Which author/s conducted the interview or focus group?
4
Credentials
2
What were the researcher's credentials? E.g. PhD, MD
4
Occupation
3
What was their occupation at the time of the study?
4
Gender
4
Was the researcher male or female?
4
Experience and training
5
What experience or training did the researcher have?
4
Relationship with participants
Relationship established
6
Was a relationship established prior to study commencement?
4
Participant knowledge of the interviewer
7
What did the participants know about the researcher? e.g., personal goals, reasons for doing the research
4
Interviewer characteristics
8
What characteristics were reported about the inter viewer/facilitator? e.g., Bias, assumptions, reasons and interests in the research topic
4
Domain 2: Study design
Theoretical framework
Methodological orientation and theory
9
What methodological orientation was stated to underpin the study? e.g., grounded theory, discourse analysis, ethnography, phenomenology, content analysis
4
Participant selection
Sampling
10
How were participants selected? e.g., purposive, convenience, consecutive, snowball
3
Method of approach
11
How were participants approached? e.g., face-to-face, telephone, mail, email
3–4
Sample size
12
How many participants were in the study?
3, 5
Nonparticipation
13
How many people refused to participate or dropped out? Reasons?
5
Setting
Setting of data collection
14
Where was the data collected? e.g., home, clinic, workplace
4
Presence of nonparticipants
15
Was anyone else present besides the participants and researchers?
4, 5
Description of sample
16
What are the important characteristics of the sample? e.g., demographic data, date
3, 4
Data collection
Interview guide
17
Were questions, prompts, guides provided by the authors? Was it pilot tested?
3, 4
Repeat interviews
18
Were repeat inter views carried out? If yes, how many?
4
Audio/visual recording
19
Did the research use audio or visual recording to collect the data?
5
Field notes
20
Were field notes made during and/or after the inter view or focus group?
5
Duration
21
What was the duration of the inter views or focus group?
5
Data saturation
22
Was data saturation discussed?
4
Transcripts returned
23
Were transcripts returned to participants for comment and/or correction?
4
Data analysis
Number of data coders
24
How many data coders coded the data?
4
Description of the coding tree
25
Did authors provide a description of the coding tree?
4
Derivation of themes
26
Were themes identified in advance or derived from the data?
4
Software
27
What software, if applicable, was used to manage the data?
4
Participant checking
28
Did participants provide feedback on the findings?
4
Reporting
Quotations presented
29
Were participant quotations presented to illustrate the themes/findings?
Was each quotation identified? e.g., participant number5–8
Data and findings consistent
30
Was there consistency between the data presented and the findings?
5–10
Clarity of major themes
31
Were major themes clearly presented in the findings?
5–10
Clarity of minor themes
32
Is there a description of diverse cases or discussion of minor themes?
5–8