
Abstract
Background
Globally, healthcare providers have faced significant difficulties in adhering to clinical guidelines. Applying mobile health systems is a crucial strategy for enhancing the dissemination and accessibility of clinical guidelines. This study aimed to assess the acceptance of mobile app-based primary healthcare clinical guidelines and associated factors among health professionals in central Gondar health centers.
Methods
A cross-sectional study supplemented with qualitative data was conducted on 403 health workers. Data were collected using a pre-test structured printed questionnaire and entered into EpiData version 4.6. Analysis was conducted using Stata version 14, which included bivariable and multivariable logistic regression analyses. For qualitative data, thematic analysis was conducted using Open Code v.4.2.
Results
Approximately 28% (95% confidence interval (CI): 23%–32%) of health professionals had utilized mobile app-based clinical guidelines. The availability of IT support (adjusted odds ratio (AOR) = 3.51, 95% CI: 1.82–6.78), good knowledge (AOR = 3.46, 95% CI: 1.5–6.78), perceived usefulness (AOR = 2.21, 95% CI: 1.00–4.99), m-Health app exposure (AOR = 2.34, 95% CI: 1.2–4.50), and ease of use (AOR = 5.77, 95% CI: 2.50–13.32) were significantly associated with the acceptance of the mobile app-based clinical guideline. In qualitative data, lack of training and supervision and access to smartphones were barriers to acceptance of the mobile app-based clinical guideline.
Conclusion
In summary, acceptance of the app is currently low. However, it can be increased by improving the availability of IT support in the workplace, offering training and supervision, and enhancing access to smartphones.
Background
Globally, healthcare providers have faced significant difficulties in adhering to clinical practice guidelines1,2 primarily due to limited training, restricted access, and lengthiness of the guidelines. 3 Applying digital health, particularly mobile health systems, is a crucial strategy for enhancing the dissemination and accessibility of clinical guidelines.4,5 Clinical guidelines (CPGs) are “concise statements intended to guide physicians and patients in making informed decisions for specific clinical conditions, ensuring appropriate and high-quality care.”6,7
The quality of patient care depends on the source of evidence used. 8 Updated and standardized clinical guidelines serve as the foundation for delivering quality healthcare services. 9 Developing countries face challenges in this regard as their primary source of evidence is paper-based clinical guidelines, which are difficult to update and disseminate promptly.10–12 Mobile-based clinical guidelines improve patient care by empowering healthcare professionals to make timely and well-informed decisions for their patients. 13 A mobile app-based clinical guideline is a digital tool. It provides healthcare professionals with access to evidence-based guidelines for clinical decision-making.” 14
Developing countries’ healthcare systems do not deliver high-quality, comprehensive, standard, and integrated care that is easy to access. This is because healthcare providers do not follow clinical guidelines well.15,16 This leads to unnecessary medical interventions and hospitalizations, as well as higher rates of illness and death. 17
To fix this gap, in 2017, the Ethiopian Ministry of Health adapted and mobile app-based primary healthcare clinical guidelines (EPHCG) from South Africa to fit the local context. Then, they implemented them at primary levels of care.18,19
These mobile-based clinical guidelines play a crucial role in achieving the Ethiopian Health Sector Transformation Agenda (HSTA). As part of the information revolution (IR), digitization serves as a key pillar within the HSTA framework. 20 It covers many medical symptoms and procedures. These include maternal and child health, infectious diseases, non-communicable diseases, and emergency care. 18
The Ethiopian Core Team and Ministry of Health policymakers conducted a phase-based evaluation of the EPHCG system, assessing 400 healthcare facilities in the first phase. They conducted the second phase to review in detail. The goal was to find health system bottlenecks during the EPHCG implementation. 19
Using the mobile app-based clinical guidelines is an effective solution. It bridges the gap in evidence-based clinical decision-making13,21 by increasing accessibility, providing standardized care, and finally improving current evidence-based clinical decision-making.22,23
The mobile app-based clinical guidelines play a crucial role in the healthcare system for care providers and patients by reducing medical errors,24,25 decreasing direct and indirect medical costs,13,26,27 enabling easy updating of medical knowledge, 28 and facilitating communication among healthcare professionals.29,30
Mobile technology adoption in sub-Saharan Africa has risen. It increased from 32% in 2019 to 43% in 2023.31,32 However, healthcare providers demonstrate limited adoption of digital clinical guidelines, including mobile health apps, primarily due to their reluctance.16,33 The sustainable use of health technology for patient care is impossible without the acceptance and support of health professionals. 34 Acceptance of digital technologies among healthcare professionals is impacted by various facilitators and barriers. 35
Facilitators, such as adequate training, user-friendly interfaces, technical support, organizational support, and app content quality, continuous support and updates, incentives and recognition, interoperability, patient engagement, trust and security, integration with other wearable devices, social support and gamification, localization, and cultural adaptation, influence the acceptance of m-Health app systems by healthcare providers.36–41
Barriers include lack of infrastructure, insufficient training, system reliability issues, limited awareness, resistance to change, inadequate technical support, lack of organizational support, lack of internet connectivity, lack of established policies, and a shortage of skilled human resources, particularly in primary healthcare settings.36,40,42–49
Moreover, literature indicated that in developing countries like Ethiopia, challenges to the sustainable adoption of m-Health apps include poor quality of training and supervision, limited digital literacy, simultaneous use of manual and electronic systems, heavy workloads, lack of institutionalization and ownership, insufficient peer collaboration, absence of clear policies and regulations, and insufficient iterative digital system evaluation.50,51
Providers who do not use mobile app clinical guidelines may have inefficiencies and errors in patient care. They may have to rely on outdated or hard-to-access printed guidelines. This reliance can lead to human errors and slow the healthcare processes. 52
Also, evidence has shown that using a mobile health (m-Health) app for clinical guidelines decreases medical errors and costs. It also improves standardized diagnosis and shortens hospital stays for medical care 14 .
Moreover, the acceptance of a mobile application for guidelines shows the growing integration of technology in healthcare provision, enabling rapid updates and revisions as new evidence and best practices become available.13,31
This study is important for policymakers, healthcare managers, mobile system developers, and patients because it provides useful knowledge for formulating policies. The findings have the potential to facilitate the integration of these guidelines in secondary and tertiary healthcare settings, ultimately improving evidence-based patient care.
To the best of our knowledge, there are no existing studies on the use of mobile app-based clinical guidelines in Ethiopia. Hence, the objective of this study is to assess the acceptance of mobile-app-based primary healthcare clinical guidelines and the factors related to them among healthcare professionals in health centers in central Gondar, Northwest Ethiopia.
Methods
Study period
A study was conducted from 19 May to 21 June 2022 in central Gondar health centers in northwestern Ethiopia.
Study design and setting
An institution-based cross-sectional study supplemented with qualitative data was conducted to determine the proportion of acceptance of the mobile app-based primary healthcare clinical guidelines among healthcare professionals in central Gondar health centers in Northwest Ethiopia from 19 May to 21 June 2022. Central Gondar is located 738 km from Addis Ababa, the capital city of Ethiopia, and 168 km from Bahir Dar, the capital city of the Amara regional state. It has 18 Woreda, 9 hospitals, and 76 health centers with an estimated total population of 2,307,773 people, 51% of whom are female. 53
Eligibility criteria
The study population comprised health professionals who had been using the mobile-based clinical guidelines for at least 6 months, worked in the selected health centers, had smartphones, and were available during data collection time.
Health professionals who had less than 6 months of working experience on the mobile-based clinical guidelines were excluded from the study.
Sample size determination and sampling procedures
For a quantitative study, we used the single population proportion formula to calculate the sample size, with the variables n representing the required sample size, Z representing the standard normal distribution value corresponding to α/2 (1.96), p representing the proportion of health professionals using the MBPHCG, q representing the proportion of health professionals not using the MBPHCG, and d representing the assumed precision of 0.05. Since no previous studies had been conducted in Ethiopia on the use of the mobile application-based primary healthcare clinical guideline, we assumed p to be 0.05. This calculation resulted in a required sample size of 384, and after accounting for a 10% non-response rate, 423 healthcare professionals were enrolled in the study.
The quantitative data were collected from study participants selected using the thumb rule of (20–30), taking into account feasibility issues and geographic dispersion. Of the initial 76 health centers, 17 were ultimately chosen in northwest Ethiopia. These included Ambageorgis, Atsedemariam, Aymba, Bira, Delegi, Dengelber, Dinkularba, Enfranze, Gedebye, Graregie, Kolladiba, Maksegnt, Minzero, Musybanb, Sanja, Serako, and Trigosgie. The number of healthcare providers selected from these health centers using the single proportion formula was chosen through simple random sampling.
For the qualitative part, seven key informant interviews (KIIs) were conducted considering the point of saturation. A purposeful sampling technique was employed to select key informants from the heads of health centers and primary healthcare clinical guideline focal persons.
Study variables and operational definitions
The outcome variable was the acceptance of the mobile app-based primary healthcare clinical guidelines and the independent variables included m
To measure the level of healthcare provider acceptance of the mobile-app-based clinical guideline, we used the following five general questions: Was EPHCG utilized for patients’ history taking and confirming symptoms? Was it utilized for national disease classification (NCOD)? Was it utilized to access medical/drug information? Was it utilized for referral reasons? Was it utilized to identify indications and contraindications in the past 6 months? These questions were adapted from studies, such as “Utilization, of Medical Records in Ethiopia,” “Utilization of a Mobile Phone Application for Reproductive Health,” “Smartphone Medical App Use by Physicians in North Ethiopia,” and the “Ethiopian Primary Health Care Clinical Guideline Implementation Manual.”18,44,54,55
These questions were designed with yes or no answer options. The acceptance scale ranged from 0 to 5, where a score of “5” indicated acceptance of the five functions in the last 6 months, and a score of “0” indicated no acceptance of any of the five functions.
Upon evaluating the distribution of the data, it was found skewed. As a result, median values were used for analysis. The median was calculated using Stata version 14. 44
Mobile app-based primary healthcare clinical guidelines
The primary healthcare clinical guidelines are delivered through a mobile app software application. 56
Data collection tools and procedures
For the quantitative part of this study, self-administered structured printed questionnaires were used. These questionnaires were adapted from Davis' study and another related study.44,59–65 The questionnaire was first prepared in English, and then translated into Amharic for data collection purposes. Later, it was translated back from Amharic to English for analysis purposes. The study included 32 questions covering the following domains: socio-demographic characteristics (eight questions), perceived usefulness (four questions), perceived ease of use (five questions), knowledge (five questions), and mobile-based primary healthcare acceptance (outcome variables five questions).
The data were collected by six health information technicians with diplomas and experience in data collection, and supervision was provided by three BSC health informatics professionals.
For the qualitative part, data were collected by the principal investigator through the use of open-ended questions. Several probes were used to obtain deep insight into participants’ beliefs, and the guide was pretested to ensure relevance and appropriateness.
Data quality control
Two days of training were given to the data collectors and supervisors based on the objective of the study, data collection procedures, data collection tools, respondents’ approach, data confidentiality, and respondent rights before the data collection date. The completeness of the questionnaires was checked every day by the supervisors before the actual data were collected. We consulted with three PhD health informaticians and senior researchers to ascertain the validity of the questionnaire. They were invited to review the tool, focusing on content validity, and make necessary revisions. The questionnaire's reliability was calculated to be α = 0.96 for the outcome variable and α = 0.94 or higher for the independent variables.
For the qualitative part, after examining pertinent literature on the barriers and facilitators of utilizing digital clinical guidelines, a comprehensive interview guide was developed for conducting key informant interviews. The responses were audio recorded, and notes were taken by the principal investigator and data collectors. Separate and quiet rooms were used to conduct the interviews.
To ensure trustworthiness and eliminate sources of bias, data were collected from different sources, including health center heads, clinical guideline focals, and healthcare providers, to ensure credibility. Additionally, the audio data were collected by an investigator, and short notes were taken by data collectors. Subsequently, both sets of data were cross-validated. Furthermore, member checking was conducted after translating the text back to the key informant respondents (health center heads and EPHCG focals) for feedback. Refinement was then done accordingly. Data were rechecked repeatedly during transcription, translation, and analysis to ensure conformability.
Statistical analysis
After carefully checking each completed questionnaire for any mistakes and completing the data cleaning process, the cleaned data were entered into EpiData 4.6. Subsequently, the data were exported to Stata version 14 for statistical analysis.
Descriptive statistics were used to describe the data, including summary statistics, frequency and percentage distributions, as well as visual representations, such as graphs and tables.
A bivariable and multivariable logistic regression model was employed to assess the factors associated with the acceptance of the app. Variables with a p-value less than or equal to 0.2 were included in the multivariable logistic regression analysis.
The presence of multicollinearity among the independent variables was checked using a variance inflation factor (VIF). Among them, the maximum VIF value was 1.95, indicating that there was no multicollinearity between the independent variables. In addition, the Hosmer–Lemeshow goodness-of-fit test was performed to assess the model fit. The obtained p-value was 0.42, which is greater than the significance level of 0.05. This indicates that the model fits the data well according to the standard p-value criterion for model fit assessment. For the qualitative analysis, Open Code version 4.2 was used for thematic analysis.
Results
Socio-demographic characteristics
A total of 403 healthcare providers participated in the study, with 223 males and 180 females, resulting in a response rate of 93%. The respondents had a median age of 31 years, with an interquartile range (IQR) of 28–35. The majority of the participants 375 (93.0%) were orthodox religious followers. More than half of the participants were married. Among the participants, 195 (48.3%) were nurses, and 190 (47.1%) had more than 6 years of clinical experience. Regarding the sources of information for evidence-based patient management, 356 (88.3%) mentioned medical books, while 145 (35.9%) mentioned mobile health apps. A total of 7 KII respondents actively participated in the qualitative study (Table 1).
Socio-demographic factors for HPs to utilize EPHCG in northwest Ethiopia in 2022.

Mobile app-related variables
Perceived usefulness
The perceived usefulness of the mobile health clinical guidelines was recognized by 195 (48.3%) healthcare professionals as beneficial. The study results indicated that 155 (38.4%) healthcare professionals confirmed that the use of EPHCG enhances their clinical effectiveness. Additionally, 160 (39.7%) healthcare professionals agreed that EPHCG empowers them to effectively manage their patients’ health (Table 2).
Perceived usefulness factors for health professionals’ acceptance of EPHCG.

SD: strongly disagree; D: disagree; N: neutral; A: agree; SA: strongly agree.
EPHCG: mobile app-based primary healthcare clinical guidelines.
Perceived ease of use
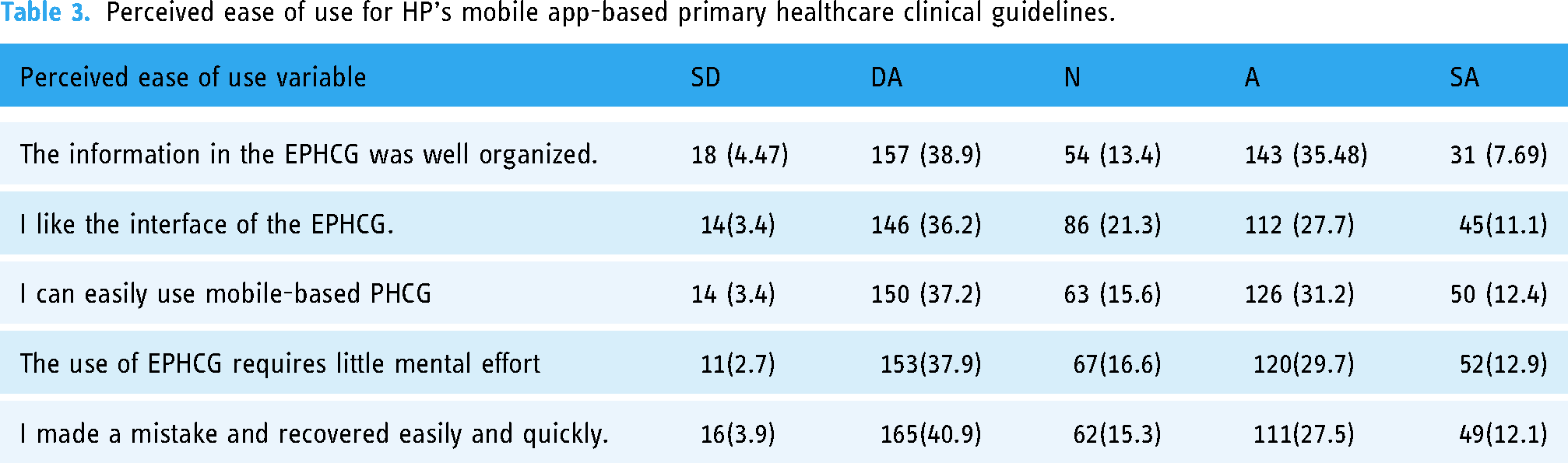
According to the data presented in Table 3, 146 (36.2%) healthcare professionals (HPs) found the user interface of the EPHCG to be complex. Additionally, 157 (38.9%) HPs reported that the content within the EPHCG was disorganized, making it difficult for them to locate the necessary information (Table 3).
Perceived ease of use for HP's mobile app-based primary healthcare clinical guidelines.
Knowledge of the acceptance of the mobile app-based clinical guidelines
More than half 227 (56.3%) of the healthcare providers had poor knowledge of EPHCG. Moreover, 200 (49.5%) HPs were found to be aware of the definition of EPHCG. However, more than half, that is, 221 (54.8%) HPs, claimed that using EPHCG for patient care did not reduce pointless referrals or transportation expenses (Table 4).
Knowledge of the acceptance of mobile app-based primary healthcare clinical guidelines.

Organizational variables of the acceptance of the mobile app-based clinical guidelines
Only 98 (24%) of the participants had access to a computer in their working area. The majority of the 382 (94.7%) HPs had not received formal training in the mobile-based guidelines. According to 351 (87.1%) respondents, EPHCG was not part of the health centers’ plan. Additionally, more than half of the health professionals, that is 298 (73.9%), were unable to access the internet. Furthermore, 93% of healthcare professionals report that no focal person had been assigned to oversee EPHCG-related activities (Table 5).
Organization- and technological-related variables on the acceptance of mobile app-based clinical guidelines.

The overall percentage of perceived usefulness, perceived ease of use, and knowledge of health professions on the acceptance of the mobile app-based primary healthcare clinical guidelines in 2022 is shown in Figure 1.
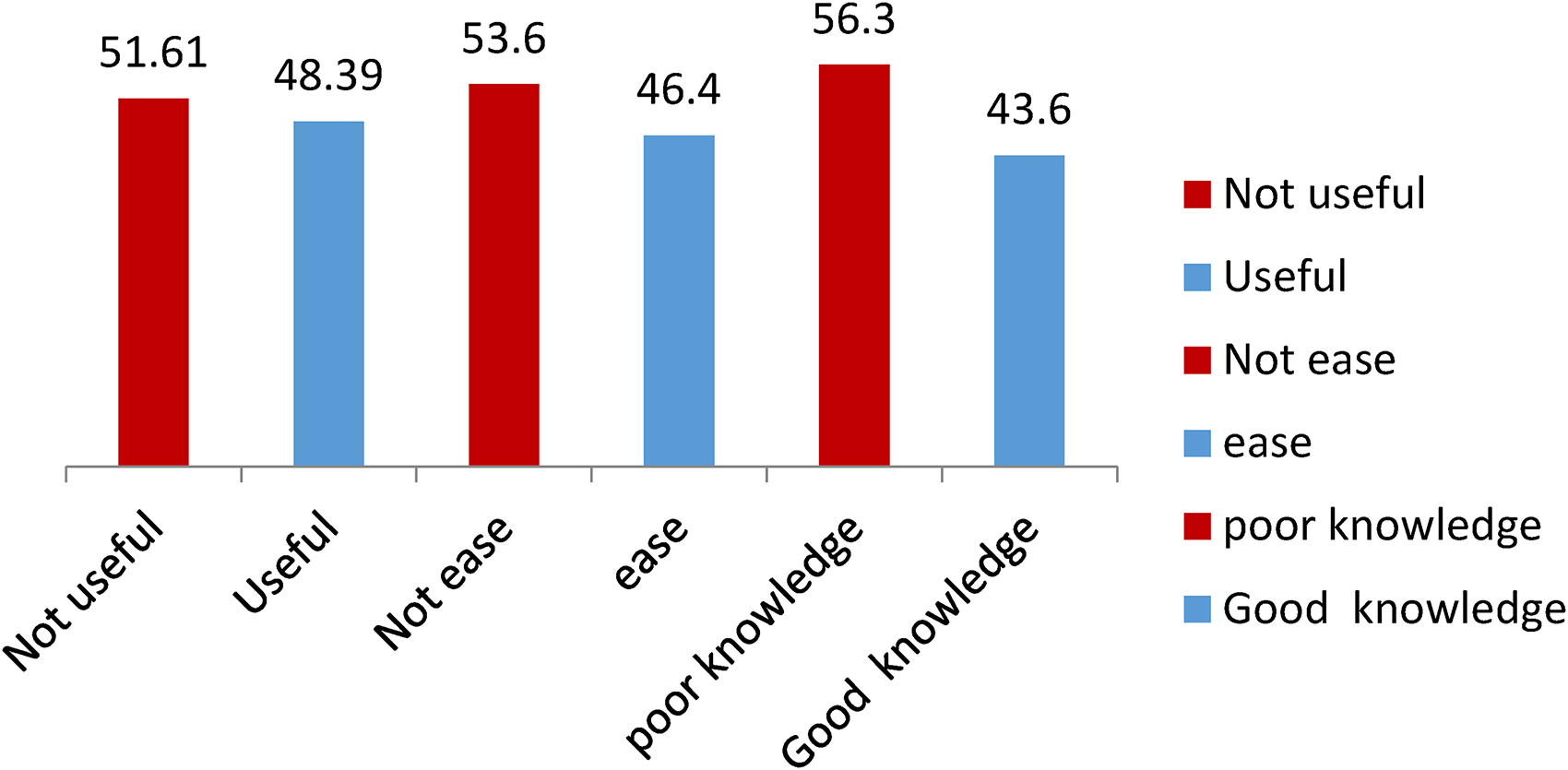
Percentage of perceived usefulness, perceived ease of use, and knowledge of health professions.
Acceptance of the mobile app-based primary healthcare clinical guidelines
Among all healthcare professionals, 28% (95% CI 23–32%) had good acceptance of the mobile app-based primary healthcare clinical guidelines, while 72% had poor acceptance of them, as shown in Figure 2.

Acceptance of mobile app-based primary healthcare clinical guidelines in central Gondar health centers, 2022 (n = 403).
Factors associated with the acceptance of the mobile app-based primary healthcare clinical guidelines
The study evaluated the factors influencing the acceptance of healthcare providers for the mobile app-based primary healthcare clinical guidelines through bi-variable and multivariable analyses. In the bi-variable analysis, significant associations were observed between the acceptance of the mobile app-based primary healthcare clinical guidelines and factors, such as IT support availability, knowledge, previous use of the m-Health app, perceived usefulness of EPHCG, and perceived ease of EPHCG (Table 6).
Multi-variable analysis of factors associated with the acceptance of MBPHCG.
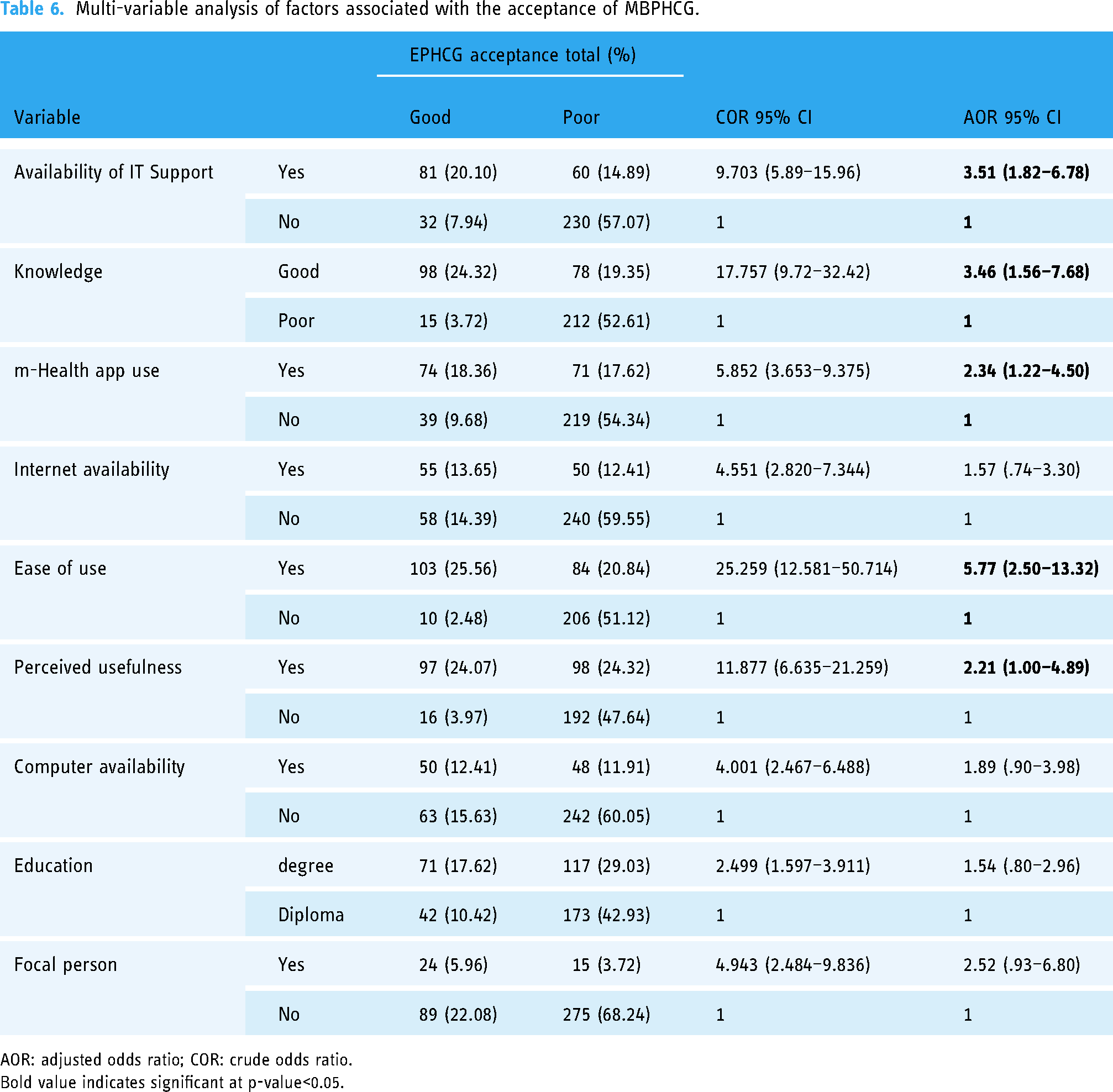
AOR: adjusted odds ratio; COR: crude odds ratio.
Bold value indicates significant at p-value<0.05.
According to our multi-variable logistic regression analysis, the availability of IT support (adjusted odds ratio (AOR) = 3.51, 95% confidence interval (CI): 1.82–6.78), knowledge (AOR = 3.46, 95% CI: 1.5–6.78), perceived usefulness of EPHCG (AOR = 2.21, 95% CI: 1.00–4.89), previous use of m-Health apps (AOR = 2.34, 95% CI: 1.2–4.50), and perceived ease of use of EPHCG (AOR = 5.77, 95% CI: 2.50–13.32) were found to be significantly associated with the acceptance of the mobile app-based primary healthcare clinical guideline.
Qualitative results on using the mobile app-based clinical guidelines
A total of seven KII respondents participated in the qualitative study. Regarding sex and age, the majority of the study participants were male and aged >30 years old.
Barriers to using the mobile app-based guidelines in clinical practice
According to the qualitative data, the main barriers to using mobile apps include long patient wait times, a lack of access to smartphones, insufficient training and supervision, and a shortage of healthcare professionals.
Patient wait time-related barriers
The majority of key informant respondents reported that one barrier to using EPHCG is extended patient waiting times. Three of our healthcare professionals have trained on the mobile app primary healthcare clinical guidelines, but do not use it due to extended patient waiting time. (33-year-old PHCG focal)
Limited access to smartphones
Key informant respondents expressed that utilizing the mobile app clinical guidelines had been challenging because not all health workers had smartphones. The problem is that some healthcare professionals at our health center do not use the app because they do not have access to them. For example, three of them do not have smartphones. (36-year-old OPD coordinator)
Lack of formal training and supervision on the digital clinical guidelines
According to qualitative findings, the majority of healthcare providers reported a lack of formal training and supervision on digital clinical guidelines, which was a barrier to utilizing the app. We have implemented the manual-based guideline, but we have not fully adopted mobile app clinical guidelines because healthcare providers have not received formal training. (39-year-old health center head)
There are a lot of apps on our phone that are easy to use, and I believe this one is as well but lack monitoring from the zonal/regional health office. (35-year-old OPD coordinator)
Facilitating factors for using the mobile app-based guidelines in clinical practice
mHealth app exposure
Respondents revealed that previous m-Health exposure was one motivator to use apps like the NCOD. …Most of our healthcare professionals are familiar with and use the mobile app clinical guideline because they have experience using the National classification of disease app. (33-year-old health center head)
EPHCG training
According to some health professionals’ feedback, those who received training used the app consistently. …We have received training on mobile clinical guidelines, comprehended their benefits, and actively utilized them in our decision-making processes. (41-year-old health center head)
Discussion
One of the biggest problems in healthcare is non-adherence to clinical guidelines. To address these challenges, in 2017, the Ethiopian Federal Ministry of Health implemented mobile application-based primary healthcare clinical guidelines.
This study aimed to assess the acceptance of mobile app-based primary healthcare clinical guidelines and associated factors among health professionals in central Gondar health centers in northwestern Ethiopia. To the best of our knowledge, this is the first study on the use of mobile app-based primary healthcare clinical guidelines.
This research has the potential to offer important information for policymakers and the Ministry of Health, guide the preparation of training programs for healthcare professionals to effectively use these tools, and play a critical role in shaping the future of primary healthcare delivery and enhancing access to quality care through the use of mobile technology.
The findings of our study showed that 28.04% (95% CI: 23–32%) of health professionals accepted mobile app-based primary healthcare clinical guidelines. This is lower than studies conducted in Gondar, Ethiopia (63.3%),
44
Saudi Arabia (42.3%),
66
Uganda (81%)
55
, Iran (40%),
67
and Canada (65%
68
). This is supported by qualitative data. The lack of formal training and supervision on the app and limited access to smartphones were barriers to using the mobile-based clinical guidelines. We have implemented the manual-based guideline, but we have not fully adopted mobile app clinical guidelines because healthcare providers have not received formal training. (39-year-old health center head)
Another potential explanation for these differences is the variation between the study area and study populations. Our study was specifically conducted in rural health centers.
Participants who had access to IT support at health centers were 3.45 times more likely to use EPHCG compared to those without IT support. These findings are in line with previous studies.44,66,69 This is a fact: having IT support available near healthcare professionals is essential for the successful acceptance of digital health. It ensures that users receive necessary technical assistance, maintenance, updates, training, and issue resolution, ultimately fostering a higher likelihood of successful adoption.
Health professionals who had good knowledge were 3.03 times more likely to use EPHCGs than those with poor knowledge. The findings of this study corroborate those from South Africa, 70 Finland, and Lithuania. 71
This is due to the fact that healthcare professionals who are knowledgeable about technology can easily understand digital health concepts and navigate the features and functionalities of digital health tools. 72
Individuals who perceived EPHCGs to be beneficial for their job were 2.21 times more likely to use them than their colleagues. This study is in line with previous studies..44,47,73–75 Healthcare professionals are more likely to utilize the mobile app-based clinical guidelines if they perceive them as enhancing their decision-making process, improving patient care, saving time, improving workflow efficiency, providing accessibility and convenience, and supporting professional development. 76
Health professionals who had experience using mobile health apps were found to be 2.28 times more likely to use mobile app-based primary healthcare clinical guidelines than those who had not used such apps before. This finding is in line with those of studies conducted in Iran
77
and Germany.
78
This result is supported by a qualitative study. …Most of our healthcare professionals are familiar with and use the mobile app clinical guideline because they have experience using the National Classification of Disease app (NCOD). (33-year-old health center head)
Those who found mobile app-based primary healthcare clinical guidelines easy to use were 5.7 times more likely to use them than their peers. This study is in line with previous studies.75,80–82 Some studies similarly demonstrated that ease of use plays a crucial role in the acceptance of mobile apps.
Ease of use plays a crucial role in the adoption and utilization of mobile app-based clinical guidelines by healthcare professionals. Therefore, developers and designers should prioritize these aspects during the development and implementation of such apps to ensure their effectiveness and impact on clinical practice. 83
Implications for practice and research
The use of mobile app clinical guidelines has significant implications for practice, research, and policymakers. Healthcare professionals can improve the quality and efficiency of healthcare delivery by accessing up-to-date clinical guidelines on their mobile devices.
This can lead to more informed decision-making and better patient outcomes. Researchers can also benefit from studying the effectiveness and impact of mobile app clinical guidelines on healthcare delivery, which can further improve their effectiveness.
Policymakers may need to consider how to regulate and standardize the use of these tools to ensure quality and consistency in healthcare delivery. Overall, stakeholders should consider these implications to effectively integrate and maximize the benefits of mobile app clinical guidelines in healthcare delivery.
Strengths and limitations
This is the first study in Ethiopia supported by a qualitative design and study of rural areas at health centers because the majority of the population receives primary healthcare at health centers.
There are a few limitations to this research; establishing temporal relationships may be difficult because the study used a cross-sectional methodology. The other limitation of the study is that it was conducted at the primary healthcare level, specifically in health centers within the Ethiopian context. The majority of participants recruited were other healthcare professionals, such as public health workers and nurses. This could make it difficult to generalize and transfer the findings given the limited participation of physicians. The self-administered questionnaire could result in the possibility of response bias.
Conclusion
Based on the quantitative findings, knowledge, perceived usefulness, previous use of the m-Health app, and perceived ease of use were found to be major contributors to the low acceptance of the mobile app-based primary healthcare clinical guidelines.
Based on qualitative findings, barriers to the use of the mobile app-based primary healthcare clinical guidelines include long patient wait times, a lack of access to smartphones, insufficient training and supervision, and a shortage of healthcare professionals.
In summary, the acceptance of the app is currently low. However, it can be increased by improving the availability of IT support in the workplace, offering training and supervision, and enhancing access to smartphones. Future research should focus on studying comparative research on private and public healthcare facilities.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241261930 - Supplemental material for Acceptance of mobile application-based clinical guidelines among health professionals in Northwestern Ethiopia: A mixed-methods study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241261930 for Acceptance of mobile application-based clinical guidelines among health professionals in Northwestern Ethiopia: A mixed-methods study by Nebebe Demis Baykemagn, Araya Mesfin Nigatu, Berhanu Fikadie and Binyam Tilahun in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to acknowledge the University of Gondar for enabling us to carry out this study. We also like to thank the central Gondar zonal health department and health centers for providing all necessary information and support. We are grateful to the individuals who participated in the study, as well as those who collected and supervised the data collection. Finally, this work would not be possible without the financial support of the Doris Duke Charitable Foundation under grant number 2017187. The mission of the Doris Duke Charitable Foundation is to improve the quality of people's lives through grants supporting the performing arts, environmental conservation, medical research, and child well-being and through preservation of the cultural and environmental legacy of Doris Duke's properties.
Availability of data and materials
The datasets for this study will be available upon reasonable request from the corresponding author.
Consent for publication
Not applicable.
Contributorship
All the authors made significant contributions to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or each author played a role in drafting, editing, and critical review of the article and agreed on full responsibility for every aspect of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was obtained from the Institutional Review Board (IRB) of the University of Gondar College of Medicine and Health Sciences, Institute of Public Health (Ref No. /IPH2124/2014). Communication with the different official administrators was made through a formal letter obtained from the University of Gondar. Written consent was obtained from each study participant after they were informed of the objective of the study. The individuals involved were informed about the advantages and potential drawbacks of the research. The data collection procedure was anonymous; their privacy was also maintained; and the study was performed according to the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
NDB
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.