
Abstract
Introduction
The COVID-19 pandemic has highlighted the significance of tele-rehabilitation in granting access to physical therapy for breast cancer patients. To mitigate the adverse effects of chemotherapy, Jacobson's relaxation techniques can be performed from the comfort and safety of patients’ homes. The aim of this research was to investigate the effects of relaxation exercises delivered via tele-rehabilitation in breast cancer patients receiving chemotherapy.
Method
A total of 64 patients, were randomly allocated to the exercise group (n = 33) and to the control group (n = 31). The exercise group performed supervised “Jacobson Progressive Relaxation” exercises in groups of up to eight participants, three times a week for 6 weeks via WhatsApp© meetings. The control group was provided with a simple relaxation exercise brochure. The primary outcome was the “pain” which was measured by “Brief Pain Inventory.” Fatigue, emotional state, quality of life, cognitive state, sleep quality, and kinesiophobia were considered as secondary outcomes. All measurements were made at the first appointment and after the intervention.
Results
The study was finally completed with 52 participants, 26 in each group. The exercise group demonstrated a statistically significant improvement in pain (all subscales p < 0.05), quality of life (symptom scale p = 0.006), cognitive function (perceived cognitive impairment p = 0.009), and (total p = 0.016) subscales, sleep quality (p < 0.001), emotional state (depression p = 0.007, anxiety p = 0.003), and fatigue scores (p = 0.017) compared to the control group in the score change before and after the intervention. No significant difference was found between the groups in terms of kinesiophobia scores (p > 0.05). Within-group results exhibited improvement across various measures in both groups, with statistical significance (p < 0.05).
Discussion
The effectiveness of telerehabilitation-based progressive relaxation exercises in improving the pain, quality of life, cognitive status, sleep quality, anxiety–depression, and fatigue levels experienced by breast cancer patients undergoing taxane chemotherapy has been demonstrated in this study.
Introduction
With the developing treatment methods, oncological rehabilitation has become an important complementary part of cancer treatment. 1 When the side effects of treatment are examined, such as decrease in functional capacity, fatigue, depression, cognitive disorders, pain, and lymph edema come to the fore in individuals with breast cancer, and the need for oncological rehabilitation increases. It is known that physical activity, exercise, and lifestyle changes have positive effects in reducing these treatment-related effects, and more studies with high evidence levels are recommended.1,2 Among exercise modalities, defined as aerobic, resistance, stretching, relaxation and calisthenic exercises have an important role in the rehabilitation of individuals with breast cancer before, during, and after treatment. 2 Considering the home environment and the patient group who will do the exercises, it can be accepted that relaxation exercises could be conducted as home exercises that patients can do in the most comfortable and safe way.
Tele-rehabilitation refers to the use of rehabilitation services through information and communication technologies. It can be used in many areas such as evaluation, monitoring, prevention, intervention, audit, training, and consultancy. Patients’ rehabilitation needs are met in the clinic, home, school, and community-based settings within the framework of ethical rules. 3 Recently, tele-rehabilitation applications have been used frequently in different cancer patients. It is recommended because of its positive effects on functional capacity, emotional state, fatigue, pain, and quality of life.4–7
Due to the COVID-19 pandemic, many individuals with chronic diseases have had to change or stop their face-to-face treatment options to avoid the risk of infection. These disruptions in healthcare increase the use of the telemedicine option. It has become important to use this option in terms of access to physical therapy in individuals with breast cancer. 8 Among different web-based programs, increased muscle strength and functional capacity have been demonstrated in breast cancer patients receiving chemotherapy.9,10 Conversely, although telerehabilitation is valid in the postoperative period, it has been reported that face-to-face rehabilitation may be more effective as it allows the construction of a specific, personalized, and targeted rehabilitation program. 11 So, the necessity for further studies with high evidence levels to support tele-rehabilitation interventions applied with different methods becomes increasingly apparent.
In this context, the aim of the study is to examine the effects of relaxation exercises performed via tele-rehabilitation on pain, fatigue, emotional state, quality of life, cognitive state, sleep quality, and kinesiophobia in breast cancer patients receiving chemotherapy.
Methods
This study was approved by the Research Ethics Committee of Bilim University (Protocol number: August 11, 2022/2022-22-08). This trial also followed CONSORT reporting guidelines 12 and has been registered on ClinicalTrials.gov (NCT04826367). A written informed consent form was obtained from each participant.
The study is a single-center, assessor-blind, randomized controlled, and home-based tele-rehabilitation intervention, conducted in a local hospital between January 2021 and November 2022. Participants consisted of individuals with breast cancer undergoing a routine taxane chemotherapy program. The participants were randomly assigned to exercise (telerehabilitation-based relaxation exercises) and control groups.
Women diagnosed with breast cancer at Stages 1–3, with a Karnofsky performance scale score of at least 90 points, aged between 18 and 65, who have undergone a taxane-class chemotherapy program, who have not engaged in regular exercise for at least 6 months and who have consented to participate in the study were recruited for the study. Individuals were excluded from participation if they exhibited communication difficulties, had a standardized mini mental test (SMMT) score of ≤23, had previously undergone chemotherapy, had a neurological, rheumatological, or orthopedic condition that precluded engagement in the study, exhibited advanced lymphedema (Stages 3–4), experienced a recurrence during the treatment period, or failed to utilize technology for tele-rehabilitation.
Participants who met the criteria will be informed by the medical oncologist involved in the study in the medical oncology clinic in the hospital and an informed consent form were provided to the volunteers who want to participate in the study. After approval of the written consent form, participants were randomly divided into two groups. To provide randomization at a 1:1 sharing ratio, two blocks were created with the “block randomization” method, and computer-generated numbers were put in sealed envelopes. The number from the envelope chosen by the patients indicated the block. Randomizations were performed by an investigator who was not involved in the study. The assessor was blind to the allocation of the groups. Health status (including Ki67, Karnofsky performance score, SMMT score, affected breast, operation type, molecular subtype, biopsy, breast cancer stage) and demographic information (including age, body mass index, education level, employment status, number of children, menopausal status and smoking–alcohol consumption) of the participants were recorded at baseline.
In order to calculate the sample size, power analysis (80% power and 5% type 1 error) was performed with the standard deviation (SD) and confidence interval data of the “pain” parameter provided from a reference article 11 similar to this study, The target sample size was determined with the aim of recruiting at least 20 participants per group, based on a power of 80% and a confidence interval of 95%, with an effect size of 0.91. With a possible 30% loss of patients to follow-up was added and totally, it was aimed to include 26 patients in each group.
Outcomes
The pain evaluation was identified as the primary outcome, while the fatigue, emotional state, quality of life, cognitive status, sleep quality, and kinesiophobia were evaluated as secondary outcomes. Each patient was evaluated in the initial session prior to chemotherapy administration. A subsequent 6-week intervention session was then conducted, with the same assessments repeated immediately following the intervention's completion.
Primary outcome
Pain assessment: “Brief Pain Inventory” (BPI) was used as the pain assessment. It is a nine-question scale that evaluates the location and severity of pain, especially with the last 24-h activities. BPI has three subscales: BPI Pain Intensity (BPI-PI), BPI Interference (BPI-I), and BPI Pain Experience (BPI-PE). 13 Scores are given between 0 and 10 points on a Likert scale; A score of 0 is defined as no pain, and a score of 10 is defined as unbearable severe pain.
Secondary outcomes
Fatigue assessment: It was assessed by the “Fatigue Impact Scale” (FIS). This scale, consisting of 40 items, evaluates the effects of fatigue on physical, cognitive, and psychosocial functions. Each item is rated on a five-step Likert scale, where 0 = no problems to 4 = extreme problems during the previous month. Ratings are summed to a total score, ranging from 0 to 160, and domain scores range from 0 to 40 for physical and cognitive functioning and 0–80 for the psychosocial functioning. Higher scores indicate greater exposure to fatigue. 14
Emotional state assessment: It was assessed by the “Hospital Anxiety and Depression” (HAD) scale. It is a Likert-type scale consisting of 14 questions, 7 of which evaluate anxiety and 7 of which evaluate depression. 15 The cutoff score for the anxiety subscale is 10/11 and for the depression subscale, it is 7/8. Accordingly, those above these scores are considered at risk.
Quality of life assessment: The European Organization for Research and Treatment of Cancer–Quality of life (EORTC QLQ-C30) questionnaire was used to evaluate the quality of life of individuals. The questionnaire has 3 subtitles and 30 questions: general health, functional score, and symptom score. The first 28 of the 30 items in the scale are a four-point Likert-type scale and are scored as 1 (not at all) and 4 (very much) points. Questions 29 and 30 are the form of the domain of general well-being. Higher scores indicate better symptom severity for overall health and functional score, and worse for symptom score. 16
Cognitive state assessment: Functional Assessment of Chronic Illness Therapy–Cognitive Function (FACT-Cog) was used to evaluate individuals’ cognitive function. The questionnaire, which consists of 37 items and 4 different subtitles, evaluates perceived cognitive skills, interpretations of other people, perceived cognitive disorders, and quality of life. Individuals determine how valid a certain statement is for them in the last 7 days with a 5-point scale that includes scores between 0 (none) and 4 (very much). Higher scores indicate better cognitive functioning. 17
Sleep quality: It was assessed by the Pittsburg Sleep Quality Index. This scale consists of a total of 24 questions with 7 components. 18 These components are; subjective sleep quality, time to fall asleep, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping pills, and daytime dysfunction. If the total score obtained from these components is above 5, it indicates the “poor sleep” quality. For scores of 5 and below, the sleep quality is considered “good.”
Kinesiophobia evaluation: It was assessed by the “Tampa Kinesiophobia Scale” (TKS). There are 17 questions in this scale, which was developed to evaluate the fear of motion/re-injury. 4-point Likert scoring (1 = strongly disagree, 4 = strongly agree) is used in the scale. The total score is between 17 and 68. The high score the person gets on the scale indicates that his kinesiophobia is also high. 19
Interventions
Telerehabilitation-based relaxation exercise group (EG)
The participants in the EG performed relaxation exercises in groups of up to eight individuals, 3 days a week for 6 weeks via the WhatsApp (© 2020 WhatsApp, Inc.) application. Relaxation exercises were performed with the “progressive relaxation exercises” (PRE) technique defined by Jacobson et al. 20 It was predicted that the expected relaxations were achieved in the hand, elbow, shoulder, hip, knee, ankle, and facial muscles with the PRE applied throughout the session. So, the instructions in Figure 1 were given to the patients. Each relaxation exercise instruction was performed three times as 5 s of contraction and 10 s of relaxation. The breathing technique (breathe in deep and breathe out slow, three times) was occasionally performed between exercises to increase the effectiveness of relaxation. Tele-rehabilitation sessions lasted approximately 40 min of each, accompanied by a physiotherapist who has 8 years of experience in the field of oncological rehabilitation. The work area was required by the participants to be well ventilated, quiet, and provide an environment in which the participants would feel comfortable. Participants were asked to take a long sitting position in comfortable chairs. Necessary recommendations were made to avoid stressful factors during exercise. Patients who missed 10% of therapy sessions were excluded from the study.

Instructions for relaxation exercises. 20
Control group (CG)
A simple brochure containing pictures with the following statements was given to the participants in this group: “Take a long sitting or lying position in a warm room. Raise your shoulders, squeeze your hands and release. Pull your knees towards you and release.” In addition, patients were advised to avoid stressful conditions at home and to engage in mild walks at home on occasion. Participants in CG were not allowed to undergo any supervised or regular exercise program. If participants accomplished any of these within 6 weeks, they were required to inform the study official and were subsequently removed from the study. Participants in CG were advised that they could participate in PRE programs for 6 weeks if the study provided beneficial effects after intervention.
Statistical analysis
SPSS version 26.0 (© IBM Corporation and its licensors 1989, 2019) program was used for statistical evaluation. A descriptive analysis was performed and the mean, 95% confidence interval, and SDs were calculated for each group. Initially, Student's t-test and chi-square test were used to check for differences between groups. Normal distribution of variables was analyzed by the Shapiro–Wilk test. Intervention effects on study variables were tested using the repeated-measures analysis of covariance. When a significant interaction occurs in the analysis, paired comparisons were made with the Bonferroni test to determine whether there is a difference in scores between groups. Also, the effect size was calculated using Cohen's d values. p < 0.05 was considered significant.
Results
A total of 69 patients were included in the study within the framework of the above-mentioned criteria. During enrollment, five patients were excluded from the study. Sixty-four patients were randomized to the relaxation exercise (n = 33) group and to the CG (n = 31). Finally, as seen in the “CONSORT Follow Diagram,” the study was completed with a total of 52 patients, 26 patients in the EG and CG (Figure 2). The rate of patients lost to follow-up is 25%, which is lower than estimated at baseline (30%).

CONSORT flow diagram.
The demographics and health status of participants are represented in Table 1. According to the analysis, there were no significant differences between the EG and CG in terms of participants’ demographics and health status (p > 0.05).
Demographics and health status.
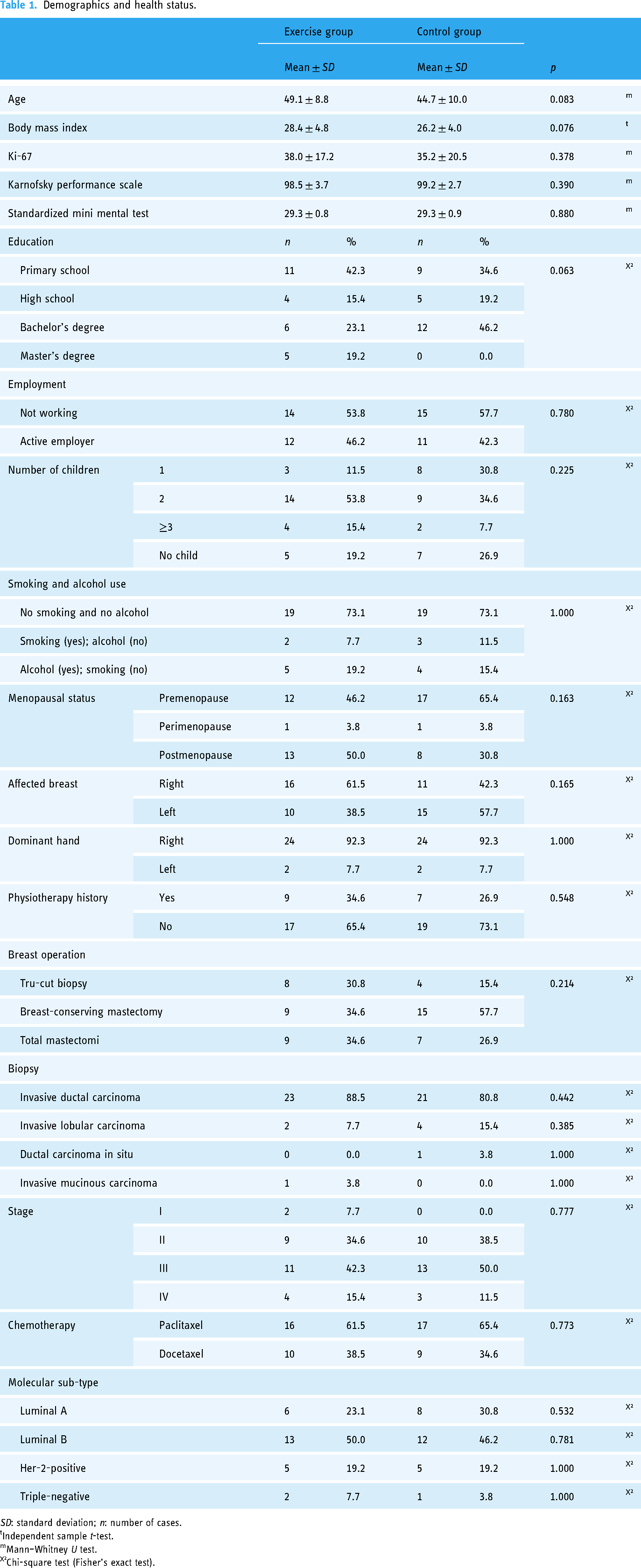
SD: standard deviation; n: number of cases. tIndependent sample t-test. mMann–Whitney U test. X²Chi-square test (Fisher’s exact test).
Compared to the CG, the EG showed significant improvement in all subscales of pain (BPI-PI r = −2.308; BPI-I r = −3.214, BPI-PE r = −3.203), “symptom” subscale of quality-of-life scale (r = −2.773), “perceived cognitive impairments” (r = −2.619) and “total cognitive status” (r = −2.398) subscales of cognitive function scale, sleep quality (r = −3.776), “anxiety” (r = −2.945) and “depression” (r = −2.706) subscales of emotional state and fatigue scores (r = −2.385) in the pre- and post-intervention score change (p < 0.05) (Table 2).
Comparison of pre- and post-intervention group evaluations.

SD: standard deviation. tIndependent sample t-test. mMann–Whitney U test. EPaired sample t-test. wWilcoxon test. Statistically significant results are shown in bold.
No significant difference was found between the groups in terms of score change before and after the intervention, in terms of kinesiophobia scores (t = −1.492), “perceived cognitive abilities” (r = −1.488), “impact on quality of life” (r = −0.984), “other people's comments” (r = −0.425) subscales of cognitive function scale and the “function” (r = −1.358) “general health” (r = −0.076) subscales of the quality-of-life scale (p > 0.05) (Table 2).
Within-group results showed significant improvement in “BPI-I” and “BPI-PE” subscales of pain scale, “perceived cognitive impairments” and “total cognitive status” subscales of cognitive function scale, emotional state scores and fatigue score for the CG (p < 0.05); “BPI-I” and “BPI-PE” subscales of pain scale, “symptom” subscale of quality-of-life scale, sleep quality and “anxiety” subscale of emotional state scores for the EG (p < 0.05) (Table 2).
Discussion
It was found to have positive effects on pain, sleep quality, anxiety, depression, and fatigue compared to the CG. In addition, it was observed that these exercises had a partially positive effect on quality of life and cognitive functions. This randomized controlled study was conducted during the COVID-19 pandemic and is the first study to observe the effect of telerehabilitation-based relaxation exercises under the supervision of a physiotherapist on breast cancer patients receiving chemotherapy.
Myelosuppressive, cardiotoxic, and hepatotoxic side effects and effects such as myalgia and arthralgia have been reported due to the use of Taxol®. 21 In addition, treatment-related quality of life, sleep, and emotional states are negatively affected in breast cancer patients, and fatigue may occur. 22 In this study, as stated in the literature, it was tried to intervene with relaxation exercises in these adverse conditions that developed due to treatment. In addition, the use of tele-rehabilitation has strengthened patients’ access to treatment during the COVID-19 pandemic.
When the studies conducted in the field are analyzed, it is understood that the effects of aerobic and strengthening exercises are mostly investigated in exercise studies conducted with breast cancer patients. 23 A meta-analysis study examining the effect of supervised exercises on cancer-related fatigue in breast cancer patients concluded that both aerobic and strengthening exercises were effective in reducing fatigue. 24 In another systematic review study showing the effects of strengthening exercises on breast cancer patients; significant improvements in muscle strength, fatigue, pain, quality of life, and small changes in aerobic capacity have been reported with strengthening exercises. 25 In this study, these effects were obtained with telerehabilitation-based relaxation exercises in breast cancer patients receiving chemotherapy. Therefore, this study thought to be unique to use a different type of exercise and perform it via telerehabilitation. This technique is gaining more importance when patients are receiving chemotherapy and when the immune system needs to be supported in situations such as pandemics.
Apart from these findings, this study showed that relaxation exercises had a positive effect only on the “symptom” subscale of the quality-of-life parameters, and no effect was found on other quality of life parameters. Courneya et al. examined the effects of aerobic and strengthening exercises in breast cancer patients receiving adjuvant chemotherapy and it was determined that these exercises did not contribute to the quality of life, but instead had an effect on self-esteem, physical fitness, and body composition. 26 Therefore, it was thought that quality of life assessments should not be considered as an isolated measurement, but should be considered together with psychosocial factors affecting quality of life in breast cancer patients. Tele-rehabilitation practices, which have been mentioned in many different studies in the past, have increased in importance with the COVID-19 pandemic. It is known that those with chronic diseases are at greater risk during pandemic periods. Tele-rehabilitation applications appear as an effective solution tool in the field of medicine in this regard. In a systematic review study conducted in recent years, it was stated that the use of technology in breast cancer patients was mostly used in the United States and that telephone, mobile applications, and web access were the most frequently used technologies. In addition, these technologies have been used for various purposes such as physical activity and functions, control of pain intensity, fitness, quality of life, dietary behavior, fatigue, muscle strength, cardio-respiratory capacity, and arm and shoulder exercises. 27 In this study, relaxation exercises were implemented using a mobile application over the phone, similar to the literature. No problems were encountered during the study as people used this application more frequently.
The findings of the studies in the literature indicate that patients with cancer who use telehealth for exercise report high levels of compliance, symptom relief, and a positive overall experience. 28 Another study found that breast cancer patients undergoing adjuvant endocrine therapy who participated in a telehealth intervention for adherence, symptom management, and distress reported high levels of intervention acceptability, enjoyment, and usefulness. 29 In this study, patients demonstrated an adherence rate exceeding expectation (78%), and the telerehabilitation intervention proved beneficial. The current study's findings are consistent with those of previous research.
In this study, no change was observed in the relaxation exercises group in the evaluation of kinesiophobia. Kinesiophobia is highly increased in patients with breast cancer undergoing adjuvant chemotherapy and is associated with poorer quality of life and higher depression and fatigue scores. 30 In a study examining the factors affecting physical activity participation in cancer patients, it was concluded that low motivation and kinesiophobia were effective. 31 In this study, the completion rate of the EG was found to be 78%. It is thought that a greater effect on kinesiophobia can be achieved by increasing this ratio.
It should be taken into consideration that there may be limitations within this study. The completion rate of relaxation exercises in the EG was 78%. Although this rate can be estimated before the study, it can be increased with national and local informative initiatives and some socioeconomic incentives. The second limitation is that the sample size of the groups is relatively small, although it was calculated from a similar study. However, it can be argued that the participants were diagnosed with breast cancer and this may have affected them physically and psychologically for the interventions. On the other hand, it is conceivable that longer-term interventions may yield more positive results.
In conclusion, this study demonstrates the beneficial effects of telerehabilitation-based relaxation exercises on pain. Furthermore, the study suggests that telerehabilitation-based relaxation exercises are effective in alleviating fatigue, improving emotional state, enhancing quality of life, stabilizing cognitive status, improving sleep quality, and reducing kinesophobia in patients with breast cancer undergoing chemotherapy during the COVID-19 period. So, it can be inferred that tele-rehabilitation has gained importance in providing patients with continued access to physiotherapy during the COVID-19 pandemic.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241261909 - Supplemental material for Relaxation training via tele-rehabilitation program in patients with breast cancer receiving chemotherapy during COVID-19
Supplemental material, sj-docx-1-dhj-10.1177_20552076241261909 for Relaxation training via tele-rehabilitation program in patients with breast cancer receiving chemotherapy during COVID-19 by Umut Bahçaci, Songül Atasavun Uysal and Esat Namal in DIGITAL HEALTH
Footnotes
Acknowledgments
Firstly, we would like to thank everyone who took part in this study and contributed to the research. We would also like to thank the nurses of the Medical Oncology Centre for their help in notifying us of incoming participants.
Contributorship
UB: conceptualization, methodology, investigation, writing—original draft preparation, writing—review and editing, and formal analysis. SAU: supervision, methodology, administration, investigation, visualization, and writing—review and editing. EN: administration, supervision, and writing—review and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Research Ethics Committee of Bilim University (Protocol number: August 11, 2022/2022-22-08) (mentioned in the Methods section).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
SAU.
Informed consent
A written informed consent form was obtained from each participant (mentioned in the Methods section).
Data availability statement
The data that support the findings of this study are available from the corresponding author, UB, upon reasonable request.
Trial registration
This trial was registered on ClinicalTrials.gov with registration number: NCT04826367.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.