
Abstract
Background
Differential access to healthcare is associated with disparities in maternal outcomes. Telehealth is one approach for improving access to maternal services. However, little is known regarding how health systems leverage telehealth to close the access gap.
Objective
This study examines how health systems have approached decisions about using telehealth for maternal services before and during the COVID-19 public health emergency and what factors were considered.
Methods
We conducted semi-structured interviews with 15 health system leaders between July and October 2021 and June and August 2022. We used a rapid analysis followed by a content analysis approach.
Results
Five health systems did not provide maternal telehealth services before the PHE due to a lack of reimbursement. Two health systems provided limited services as research endeavors, and one had integrated telehealth into routine maternity care. During the PHE, all transitioned to telehealth, with the primary consideration being patient and staff safety. At the time of the interview, key considerations shifted to patient access, patient preferences, patient complexity, return on investment, and staff burnout. However, several barriers impacted telehealth use, including coverage of portable devices and connectivity. These issues were reported to be common among underinsured, low-income, and rural patients. Health systems with particularly advanced capabilities worked on approaches to fill access gaps for these patients.
Conclusion
Some health systems prioritized telehealth to improve access to high-quality maternal services for patients at the highest risk of adverse outcomes. However, policy and patient-level barriers to equitable implementation of these services persist.
Introduction
Higher maternal mortality and morbidity have been reported among people living in rural and underserved areas, including Black, Indigenous, and low-income people.1–4 These outcomes are partly attributable to inequitable distributions of health-enabling resources and environments (e.g., safe work conditions; residential contexts across the life course),1,5–13 which affect a wide range of health, functioning, and quality-of-life outcomes. 14 This includes inequities in healthcare access and quality of care, economic stability, and social needs (e.g., housing, social support, transportation, employment).15,16 Most importantly, Medicaid covers approximately 41% of births in the US, and those birthing people experience high rates of health insurance coverage losses during and after pregnancy. 17 Most US states have now adopted the policy of covering pregnant Medicaid beneficiaries for up to 12 months postpartum to enable care continuity and improve maternal health outcomes. 18 However, these populations often lack paid leave, leading them to work during pregnancy and return to work following childbirth, hindering their ability to access needed maternity services in the critical postpartum period. 19 Access to maternal services is also a critical issue in rural areas. According to the American College of Obstetrics and Gynecology, a standardized perinatal regionalization and risk-appropriate maternal care system exists in the United States, constituting basic care, specialty care, subspecialty care, and regional perinatal health care centers. 20 Despite this infrastructure, many rural counties have lost hospital obstetric services, exacerbating disparities in outcomes, including increases in out-of-hospital births, births in a hospital without an obstetrician, and preterm births.21,22 Prior studies have identified maternal telehealth innovations as a potential strategy to address access gaps and poor maternal outcomes.23,24
The Health Resources and Services Administration of the US Department of Health and Human Services defines telehealth as “the use of electronic information and telecommunications technologies to support and promote long-distance clinical health care, patient and professional health-related education, and public health and health administration. Technologies include videoconferencing, the internet, store-and-forward imaging, streaming media, and landline and wireless communications.” 25 Before March 2020, telehealth was used for various maternal services, including prenatal care, maternal-fetal medicine consultation, fetal heart rate monitoring, genetic counseling, and remote chronic illnesses.23,26 A review of maternal telehealth strategies by Cantor et al. showed that the only randomized controlled trial conducted before the COVID -19 pandemic comparing reduced visits plus virtual visits with usual care showed higher satisfaction among the intervention group. 26 Similarly, a cohort study with a similar treatment and control group reported lower rates of preeclampsia in the treatment group and the same rates of gestational diabetes in both treatment and comparison groups. 26 The review showed that all the studies reported statistically significant differences in patient surveys, favoring reduced visits plus virtual visits. 26 However, none of these studies were conducted in rural areas. Furthermore, telehealth programs have been shown to increase access in areas with health workforce shortages; for example, phone-based pregnancy applications have been shown to increase the utilization of perinatal services by Medicaid beneficiaries. 27 Systematic reviews and meta-analyses of telehealth services illustrate their benefits. For example, transmitting patient-generated data through remote monitoring and mobile phones in high-risk obstetrics led to better blood sugar and blood pressure control and fewer scheduled outpatient visits for managing diabetes and hypertension.28–30 Ming et al. conducted a systematic review and meta-analysis of randomized controlled trials testing telehealth innovations for pregnant individuals with gestational diabetes. 30 Seven trials in the meta-analysis demonstrated a modest but statistically significant improvement in HbA1c associated with telehealth technology. 30 The trials showed that the HbA1c of women with gestational diabetes using telehealth was 5.22% (SD 0.70) compared with 5.37% (SD 0.61) in the standard care group. 30 Despite its promise to improve outcomes and care access in the US, telehealth was underutilized for maternal health services before the pandemic due to the lack of reimbursement. 31
In March 2020, at the onset of the COVID-19 pandemic, the US declared a Public Health Emergency (hereafter PHE), which expanded executive powers, enabling the federal Centers for Medicare and Medicaid Services (CMS), the de facto regulatory agency for health care to issue guidance for provision of telehealth services and increase reimbursements for telehealth services. 32 As a result, telehealth adoption and use rapidly increased, expanding access to healthcare services in the prenatal, perinatal, and postpartum periods.33–36 Moreover, the PHE also entailed a freeze on disenrollment from Medicaid, the public insurance plan for low-income and disabled beneficiaries, which enabled care continuity in the postpartum period. 37 Several federal agencies have emphasized telehealth to improve access to maternity care for underserved populations and promote health equity.38,39 Studies have shown promising results in this regard.40–43 For example, a randomized control trial for postpartum hypertension shows that black women in the postpartum telehealth group had more than 90% utilization of services compared to 33% in the traditional in-person group. 40 Furthermore, evidence suggests that patients value having telehealth as an option. A 2022 systematic review comparing hybrid (i.e., telehealth visits combined with in-person) versus in-person-only visits found no differences in preterm births or neonatal intensive care unit admissions but did show greater satisfaction with the hybrid model. 44
With the emerging effectiveness evidence, changing funding landscape, and support from federal agencies, maternal service delivery expectations are changing, presenting an opportunity to optimize telehealth utilization.44–46 Presumably, maternal telehealth provision is currently neither as prevalent as it was during the early phase of the PHE nor as underutilized as it was pre-PHE. 34 Little is known about decision-making within health systems regarding how much maternal telehealth to provide, specifically, which services to provide via telehealth and the circumstances under which they are offered. This study examines decisions made by health systems about telehealth for maternal services before and during different phases of the PHE, including who made the decisions, factors considered, and types of support needed to improve and sustain maternal telehealth service offerings beyond the PHE. This study will generate evidence about how health systems leverage telehealth for maternal services, which could be critical for closing the existing access gap in the United States.
Methods
We conducted semi-structured qualitative interviews with health system leaders and providers to understand the factors considered for decision-making for implementing maternal telehealth services. This qualitative study design is congruent with the research question as it enabled us to capture system-level perspectives with frontline provider perspectives. We used purposive sampling and snowballing to recruit 15 health system leaders and providers from affiliated practices representing each US census region. 47 These sampling strategies helped us identify health system leaders knowledgeable about maternal telehealth services. More specifically, we aimed to recruit a health system leader and a provider from participating health systems in four to six states. We selected health systems based on several criteria, including region within the US; academic versus non-academic health systems; health systems with hospitals offering different levels of care that had practices or hospitals in rural counties; and size of the hospital determined by the number of beds, number of outpatient clinics, and number of obstetric providers. This sampling strategy allowed us to maximize the diversity needed to understand complex decision-making at the health system level and the broader system-level reach of those maternal telehealth-related decisions. The study was reviewed by the author's institutional review board and determined to be exempt, and verbal consent was deemed sufficient.
We recruited individuals at health system leaders via email and phone outreach. We contacted 48 health systems in six states, of which five declined to participate, nine accepted to participate, and others did not respond. To capture different perspectives within a given health system, we requested interviews with a health system leader and maternity care provider, resulting in 15 interviews. Our sample included representatives from nine health systems and six affiliated practices. Semi-structured interviews were conducted in two rounds—July–October 2021 (n = 7) and June–August 2022 (n = 8). The research team (CS, MA, and BB) debriefed after each interview to reflect on the data collection effort, which helped us prioritize topics for subsequent interviews. Conducting interviews in two rounds enabled us to use preliminary analysis of the first round to evaluate the quality and completeness of our data, revise our interview guide to focus on priority topics, and capture perspectives at different time points within the PHE. We invited individuals from the first round of interviews to participate in the second round if there had been changes to their maternal telehealth offerings and/or decision-making approaches. One participant was interviewed in both rounds.
Participants were offered a $100 gift card. All the interviews were conducted on Zoom. Verbal consent was obtained at the beginning of the interview. Each interview lasted 45–60 minutes and was recorded and transcribed. Of the three interviews (MA, CS, and BB), two were females, and one was male. All are trained in qualitative research and implementation science. No one besides the interviewers was present during the interview. There was no prior relationship between interviewees and the interviewers. Interviewers ensured that leading questions were not asked to prevent undue influence on study participants. These best practices were followed to reduce any bias that may be introduced during the data collection process.48,49 Moreover, all interviews met after every interview for feedback and reflexivity to discuss how questions were asked and the influence of interviewer characteristics on the interviewee. Since telehealth was included in routine maternity care out of necessity during the PHE, most health systems had a similar experience regarding the considerations for adopting telehealth for maternal services and barriers to telehealth implementation. We stopped collecting data when thematic saturation was reached for these domains. There was some variation in how participating health systems perceived future telehealth opportunities.
The interview guide was designed to encompass several domains: (a) decision-making about maternal telehealth services; (b) barriers and facilitators to telehealth implementation; (c) the impact of telehealth on maternal health disparities; and (d) the future of maternal telehealth services. We iteratively developed separate but related interview guides based on the participant role: health system leader or provider. The open-ended questions were designed to elicit detailed descriptions from participants related to the abovementioned domains. The interview guide is available in the supplemental file.
We used both rapid and thematic analytic approaches. The results of rapid analysis informed the coding scheme used in thematic analysis. Furthermore, using two analytic approaches allowed us to compare the consistency across them, which could inform advances in qualitative research. We used the rapid analysis process (RAP), similar to several rapid analytic approaches described in the literature, which has been shown to reduce analytic time.50–53 First, the research team identified 28 topics and sub-topics based on the interview guide, first impressions of the data, and existing literature. Second, we monitored how topics interacted within and across health systems and their affiliated practices to enable systematic comparison. Additional topics or sub-topics not captured in the initial list were identified during the analysis. The research team met frequently to review the matrix and discuss discrepancies in coding or topic interaction. This approach informed the content analysis of the data.
For content analysis, we coded transcripts using Dedoose software. We used a hybrid approach to coding during content analysis because there was a possibility that some topics were missed during rapid analysis. 54 First, we developed a codebook deductively based on the rapid analysis results. Then, we added codes inductively as new themes highlighting differences or similarities in decision-making and challenges with telehealth emerged in the data. The resulting codebook had the same 28 codes as in rapid analysis, of which 10 were divided into sub-codes. Two research team members independently coded the first four transcripts to assess the adequacy of the codebook. Team members met regularly to establish agreement about the appropriate application of codes. Overall, agreement was strong, with most disagreements concerning the interpretation of codes. This iterative process led to minor changes to the codebook. One team member then coded all transcripts. The team discussed uncertainties that arose during the coding process to maintain agreement on definitions, interpretations, and emergent themes.
The codes that were similar across rapid and thematic analysis were uniquely applied 183 times to the data. The average agreement between code applications in rapid analysis and thematic analysis for these codes was 84% (same application 155 times). The codebooks and details of the comparison between rapid and thematic analysis are provided in the supplemental file.
Results
Sample characteristics
Of the nine participating health systems, five were non-academic, and four were academic (Table 1). Three participating systems served mostly urban patients, three served primarily rural patients, and three served a mix of rural and urban patients. Of the 15 participants in our study, 10 were female. Nine were clinicians with administrative positions, such as the Department of Obstetrics and Gynecology chairs. Five were clinicians with no administrative role, and one held only an administrative position.
Participant characteristics.

MD = Doctor of Medicine; NP = Nurse Practitioner.
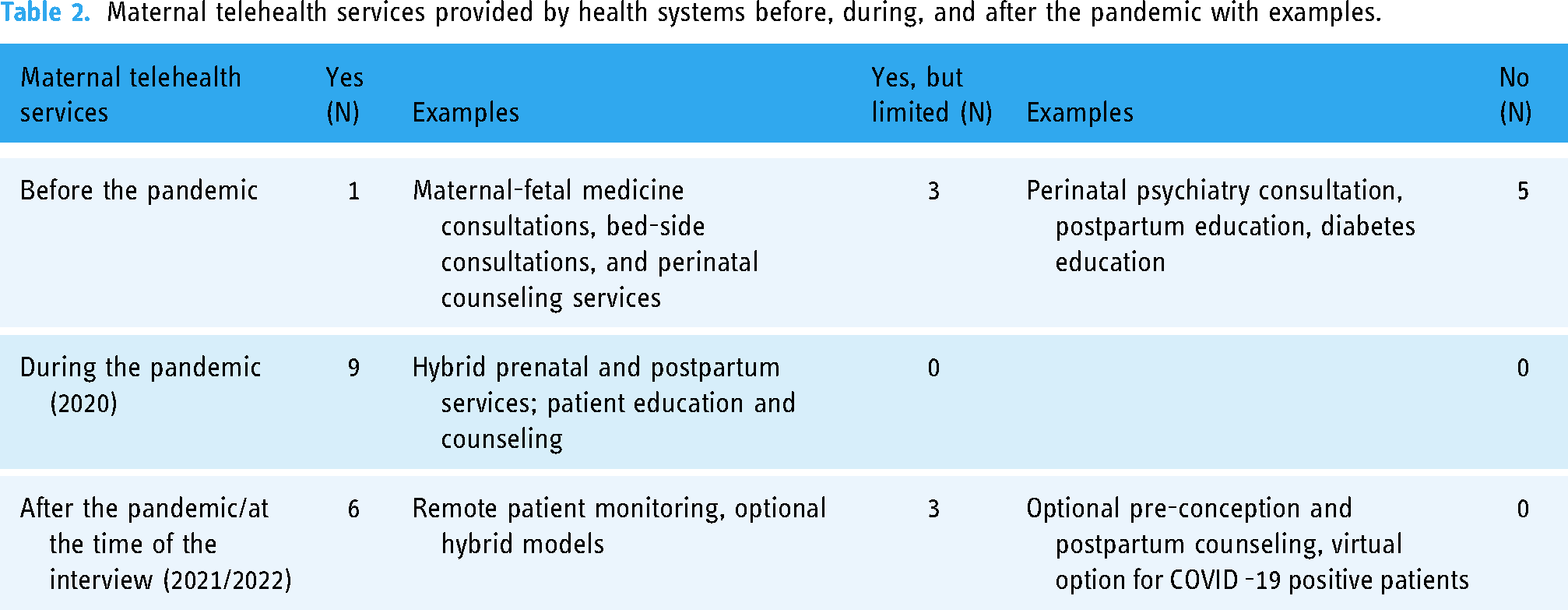
One health system had a full scope of maternal telehealth services before the PHE, sustained by its provider-sponsored health plan, in which the health system also owned an insurance organization that provided coverage for its employees and eligible patients. 55 Three systems provided limited telehealth services, primarily via research, and the remaining five had not provided maternal telehealth services before the PHE (Table 2). During the PHE, all the systems ramped up telehealth, providing a broader range of services. Six systems (four from round one and two from round two) continued to offer telehealth services at the time of the interview. Three used telehealth for COVID-related visits for pregnant patients or optional counseling or education sessions.
Maternal telehealth services provided by health systems before, during, and after the pandemic with examples.
Participants described their decision-making process for using telehealth for maternal services before and during the COVID-19 PHE, barriers, facilitators to telehealth implementation and strategies to address them, perceptions about the impact of telehealth on disparities in maternal health outcomes, and opportunities for the future of maternal telehealth. Below, we discuss each topic. Table 3 presents these topics with illustrative quotes, and Figure 1 provides an overview of the factors affecting telehealth implementation.

Factors affecting telehealth implementation for maternal services.
Key topics, sub-topics, and illustrative quotations.

Maternal telehealth decision-making
Centralized versus decentralized decision-making
Three health systems, two academic and one non-academic, described centralized decision-making for using maternal telehealth with variations in how decision-making evolved over time. For instance, one system began with individual provider champions and then took a more centralized approach to scale up telehealth services several years before the PHE. Other systems with centralized decision-making had either not provided telehealth services before the PHE or had provided them as a research endeavor. A leader at an academic health system, described their decision-making and scale-up approach as follows: We started offering telehealth in 2008 …. And then we sort of got to know that we were all doing what we were doing and there was a sort of central motivation to try to build an economy of scale and like many health systems were probably pretty aggressive about this. We were trying to centralize and invest in and try to retain all of the, the great qualities of it, but do a degree of standardization to disseminate it. (Participant#2)
The decision to provide maternal telehealth services was made at the departmental or individual provider level in six health systems, with an equal number of them being academic or non-academic. Before the PHE, one health system had started its decision-making process about telehealth offerings and continued to refine its prenatal hybrid models and other telehealth services. Others rapidly transitioned during the PHE and had either scaled back or planned to use it more systematically. A Chief Operation Officer at a non-academic health system described: The decision for telehealth would remain local to the practice that is going to be doing it. However, there's really been very little time to regroup and reprioritize outside of kind of emergency focused operations to look at that more strategically. But it is something that we definitely want to do. (Participant#4)
Despite the type of decision-making, most participants described a consensus-based process for identifying specific maternal services to provide via telehealth at the departmental level. Some had a more elaborate stakeholder engagement process with department heads, clinicians, staff, and patients to develop hybrid models of care. A leader and provider from an academic institution described: We've put a lot of work into stakeholder engagement in terms of structure and timing and for prenatal care - the content of what's done at each visit. We talked to every practice, like administrator, physician lead, and others, and we talked to every prenatal care practice. We did like big meetings, and we did essentially one on one or small group meetings with every practice. (Participant#1)
These stakeholders were engaged using several approaches, such as surveys, interviews, listening sessions, work groups, websites, and bulletins. Others reviewed the literature and guidance from the American College of Obstetrics and Gynecology or identified services based on their experience. Academic health centers had more elaborate stakeholder engagement during the decision-making process and continued to embed telehealth services into their routine maternity care after the PHE.
Factors considered in decision-making
The most common factors considered before and after the PHE were patient access and patient preferences. Five health systems were using telehealth to expand access for populations facing access barriers, which included racial and ethnic minorities, low-income, publicly insured, and rural populations. However, each system had a unique approach to ensuring equitable access. For example, two systems were focused on capturing data on quality metrics that could be stratified by these population groups to understand ongoing access issues better, demonstrate value-added, and motivate providers who would otherwise stop using telehealth. Another system used a remote monitoring app, which “reduced in-person visits for those patients and opened up some appointments for Medicaid patients” who faced barriers to using the app or telehealth in general (Participant#7). Other systems planned to expand Maternal Fetal Medicine (MFM) services in rural areas by collaborating with local clinics. An MFM specialist from a non-academic health system described: We're beta testing it in one of our more rural practices. That came from literature and some experiences in other parts of the country that we wanted to bring down. We knew that this technology existed, and we have plenty of need in areas outside of [city] that don't have ready access to maternal-fetal medicine and have a significant quality issue in terms of getting care to the patients. (Participant#6)
Patient preference was another commonly considered factor before and after the PHE. Five health systems, three academic and two non-academic, described the utilization of telehealth for maternity services as mostly driven by patient choice. A leader and a provider at an academic health system described: The goal is to really let the patients’ preferences and needs guide the care plan, not the clinician and health system decide what's right for the patient. and that is one of the key points of equity that we brought in that the patient is the one deciding what's right for them. (Participant#14)
Other factors in the decision-making process included the complexity of patients, return on investment, and clinician burnout. Most systems leveraged telehealth for low-risk pregnant and postpartum individuals and remote monitoring of gestational diabetes or hypertension. For patients with uncontrolled conditions, when the medications were changing or invasive diagnostic testing was required, in-person follow-up visits were preferred over telehealth visits as described by a leader and provider at a non-academic health system as follows: And it varies with the comfort and complexity of the patient, the patient's condition. For our chronic hypertensives, we still don't have a remote solution for antenatal testing, for non-stress tests, so that brings them to the clinic more often. (Participant#12)
Financial considerations for continuing maternal telehealth services included continued payment parity for telehealth, balancing cost savings by telehealth, and losing facility fees for hospitals with affiliated provider practices. Lastly, two health systems reported provider burnout due to additional telehealth work was reported as described by a provider and leader at a non-academic health system. If it's a virtual visit, it [the electronic template] pops up first, right? Like there's just some automation that could occur except relying on me to choose one of the 10 best templates. But that's my part with burnout. It's always like default to doctor. (Participant#7)
Telehealth implementation
Above, we reported the key factors considered when deciding whether to offer maternal telehealth services. In addition to those considerations, participants described factors affecting the implementation of telehealth, which have implications for the extent to which maternal telehealth services are provided—in other words, which services are provided, to whom, and by which providers.
Planning/preparation/implementation
Providing education and training and ensuring the availability of technology across ambulatory obstetric practices was common among all health systems. The platform used varied across systems. Two participants from systems with centralized decision-making reported switching platforms due to technical and privacy concerns. Other changes included creating workflows and decision aids for triaging patients into telehealth or in-person visits.
Barriers and strategies
At the beginning of the PHE, the most common barriers included technical challenges, such as secure transmission, coverage of portable devices, and lack of patient and provider education about telehealth (Table 4). Health systems integrated telehealth into electronic health records (EHR) for secure data transmission and documentation. Those systems without EHR telehealth integration telehealth were either planning to do so or had significantly reduced telehealth offerings.
Implementation barriers and strategies used by health systems and their affiliated practices during the PHE (2020–2022).

Coverage of portable devices, such as blood pressure cuffs, varied by state. In some states, health systems worked with Medicaid to ensure coverage of portable devices at the beginning of the PHE. A provider from an academic health system-affiliated practice described: I think that sometimes devices can be a barrier, too, in terms of getting people the blood pressure cuffs, like, depending on the situation with their insurances, etc. (Participant# 9)
Typically, if they [patients] are coming to the brick and mortar, they see me and we also schedule a visit with other ancillary services [social worker] on that same day. And I think some of that falls through the cracks when I have a virtual visit and somehow, they don't get also virtually hooked up with the diabetes educator and the social worker, which is clearly what they need more than me. (Participant#7)
Participants from affiliated practices shared patient-level barriers, including distracted patients and the quality of data shared by patients for remote monitoring. For example, four participants reported frustration with having a telehealth visit while their patient was “driving a car or shopping in a store” because the “quality of communication deteriorated.” (Participant#10) Regarding the data quality, participants reported needing to provide additional patient education on how to use a glucometer or blood pressure cuff and share results with the provider. Moreover, participants identified connectivity, access to mobile phones, digital literacy, privacy concerns, the perceived value of telehealth by providers and patients, and reluctance due to religious and linguistic discordance as barriers to optimal telehealth use. Technology-related barriers were common among rural, low-income populations. Participants shared that their publicly insured or uninsured patients did not have the resources to pay for data plans. In these instances, telehealth service was provided by telephone (audio only), which was not viewed as a sustainable option from reimbursement or care-quality perspectives.
Supports for telehealth implementation used or needed
The most common supports reported were existing communication channels between health-system leaders and providers, IT support through the health system or vendors, and support from health-system leadership (e.g., investment in virtual care departments).
Participants identified payment parity, “pay us as we would if we saw them in person” as common support still needed to sustain telehealth services. (Participant#5) Participants also called for policy and plan-level changes to cover portable devices and provider incentives to sustain the use of telehealth. Furthermore, participants from affiliated practices reported that incentives received by health systems typically do not reach individual providers.
Impact on patients
Participants identified characteristics of patients for whom telehealth is more convenient than in-person visits, including working patients, patients with childcare/caregiving needs, multiparous patients, those having to travel longer for in-person care, and postpartum patients. Participants also commented on certain patient characteristics who preferred in-person visits, including first-time mothers, those with generalized or pregnancy-related anxiety, and those who could afford to take time off from work. None of the participants noted racial differences in telehealth utilization in their populations (Table 5).
Impact of telehealth on perinatal patients.

Impact on disparities
Most interviewees described telehealth as essential for equitable access to high-quality care but did not have outcome data currently to demonstrate that impact. The health systems still planning to integrate telehealth into routine care were unsure whether and/or how individual patient needs would be considered when making telehealth decisions. A few participants shared concerns about the potential to exacerbate disparities, particularly for publicly insured people of color, because of the lack of cellular and internet infrastructure needed for successful video-based visits.
Opportunities for the future
Participants described the potential of telehealth to expand to more robust provider-provider consultations, provider-patient consultations, antenatal testing, integration of health education and mental health services, and automation of clinical decision-making (Table 6). Provider-provider consultations were described to be important for improving access to specialists. Having telehealth consultations was described as an opportunity for providers in hospitals providing basic maternal services to get expert advice when handling situations they are not accustomed to, like postpartum hemorrhage. Provider-patient consultations were described as critical for improving access to maternity services. However, participants also described needing a validated pregnancy screener to identify patients who would benefit from telehealth.
Opportunities for future maternal telehealth.

Moreover, patient preferences and the patient's trust in the quality of telehealth services were described as the major factors that would impact the uptake of maternal telehealth in the future. Home-based antenatal testing was described as one of the future opportunities to advance services provided through telehealth as it would ease the patient burden of frequent provider visits. However, participants acknowledged the need for more research to determine the efficacy of home-based antenatal testing. Integration of health education and mental health services during pregnancy and postpartum period were seen as opportunities that could be effectively provided via telehealth. Several participants described working on integrating these services into routine maternal services.
Most of these opportunities were described in the context of equitable implementation in rural hospitals and level I/level II acute care facilities to improve access for the populations with the highest need.
Discussion
Although participants reported widespread use of telehealth during the PHE, decision-making processes about continued use varied. For those who continued to offer maternal services via telehealth, implementation factors affected the extent to which they were provided. Some described less utilization of telehealth by publicly insured and rural individuals and the desire to increase utilization for these populations. However, they faced policy-level barriers to equitable telehealth implementation, such as a lack of insurance coverage for portable devices, inadequate access to the internet, and a lack of language interpretation services integrated with telehealth. These findings align with the existing literature on less utilization of maternal telehealth services by rural, low-income, publicly insured pregnant and postpartum individuals and those whose primary language is not English.43,56,57 Policymakers and payers could support health systems and practices by providing better access to blood pressure cuffs and other portable devices to prevent further exacerbation of disparities. Moreover, amid known geographic disparities in broadband availability and access, it is critical to consider how telehealth adoption may widen pre-existing disparities in access and outcomes—and find solutions to minimize them. 58
Participants reported that patient preference was a key consideration when offering maternal telehealth services. They also identified population groups that preferred hybrid models over the current standard of care due to their social or financial circumstances. Again, these results elaborate on the reasons for patients’ preference for telehealth visits or vice versa.59–63 For example, Lui et al. found that the study participants preferred in-person prenatal care over telehealth. Our study elaborates on these findings by identifying reasons for this preference, such as the desire of patients to detect fetal heartbeat, particularly first-time mothers, that may be limited during a telehealth visit. 63 Studies have also shown patient preference for telehealth visits. Kissler et al. found that pregnant women using telehealth found care accessible and reduced care costs. 61 Another study by Mehl et al. found that patients who had to travel longer distances and had childcare needs preferred telehealth over in-person visits. 62 These factors can help health systems understand the reasons for variable uptake of maternal telehealth services in their context and devise targeted strategies to demonstrate the effectiveness and quality of maternal telehealth services to their patient population. In our sample, a minority of participating health systems had tailored hybrid models or remote monitoring for high-risk pregnant individuals, reflecting variation in how health systems have leveraged telehealth services even with reimbursement parity for video visits. The variation could be potentially explained by skepticism about the continuation of telehealth coverage, provider resistance, or lack of evidence-based guidelines for maternal telehealth services.
Physician burnout was another common consideration identified, consistent with concerns about patients’ expectation of fast provider response to messages or lab results.64–66 The empirical evidence regarding the impact of telehealth innovation on provider burnout is limited. Even though some evidence shows provider preference for telehealth or hybrid maternal services,45,67–69 experts have raised concerns about the administrative burdens of healthcare telehealth solutions, including charting, responding to messages, following up with patients on laboratory results, etc.65,70 The administrative burden could lead to provider burnout if telehealth innovations in maternal services are not optimized and automated when appropriate. Health systems must work with telehealth vendors and policymakers to design efficient processes and streamlined documentation of telehealth encounters to improve provider buy-in and satisfaction.
Our study extends the literature on barriers to telehealth implementation by distinguishing barriers to maternal telehealth implementation at the health system and practice level.46,71–73 While the barriers identified at the system level were related to infrastructure, staffing, and insurance coverage, the practice-level barriers were related to workflow, provider satisfaction, and patient preference. The participants described several strategies to address most of the barriers, such as using alternate funding sources for portable medical equipment (e.g., blood pressure cuffs) when coverage by health insurance agencies is limited. Generally speaking, strategies were identified based on stakeholder input, the context of the health system, and the feasibility of using the strategy. Future research is needed to understand the application of these strategies in other contexts. A barrier that was not addressed by most health systems was the integration of social services and interpreters. Services provided by social workers and interpreters are vital to patients with greater unmet needs. Participants identified the integration of these services in telehealth workflow as an unsolved barrier, which may be a reason for the lower utilization of telehealth services by patients who need these ancillary services.74,75 Health systems must center equity when designing and implementing telehealth innovations for maternal services by learning from areas that have shown successful efforts to promote telehealth equity and decrease the digital divide.58,76–79 Future research must focus on testing and evaluating the strategies for integrating ancillary services in telehealth visits to prevent unintended consequences for vulnerable populations.
Our study also extends the literature on the potential opportunities for maternal telehealth services in the future.61,80 For example, Olenski et al. reported the need for a hybrid delivery model consisting of telephone consultations with some face-to-face consultations for pregnant individuals with diabetes in the future. 80 We further these results by identifying the scope of clinical care that would advance the quality of clinical care, such as provider-provider consultations and antenatal testing when access can be difficult otherwise.
This study has several limitations. First, our sample reflects perspectives from health systems from only six states. Although we used purposive sampling to identify participants from all regions of the US, they may not be representative of all health systems. Despite this limitation, our findings reveal details about maternal telehealth planning and delivery that were previously undocumented and could inform policy and future research—for example, assessing the extent to which our findings represent a broader pool of health systems. Second, data were collected during the early phases of widespread telehealth implementation and constant policy changes, and some of the factors considered for decision-making may have been addressed since these data were collected. Future research should focus on the decision-making considerations for telehealth adoption and equitable implementation after the sunsetting of the COVID-19 PHE and its attendant policy changes. Third, inequitable access to material telehealth services may exist for different racial groups, which is not evident in our results. Future research must focus on understanding the experience of pregnant and postpartum individuals with telehealth services to inform equity-focused decision-making and the design and implementation of maternal telehealth innovations. Lastly, health system characteristics may determine the successful adoption and implementation of maternal telehealth services, which our data cannot delineate. Future cross-sectional or longitudinal research may examine how health system characteristics like organizational structure, funding, and technological readiness affect the implementation of maternal telehealth services in the US and globally.
Conclusions
Some health systems have prioritized telehealth to improve access to high-quality maternal services. However, policy and patient-level barriers to equitable implementation of these services persist. Payment parity, insurance coverage of portable devices, and incentives were commonly identified as the support needed for sustaining telehealth services. When implementing maternal telehealth innovations in the US and globally, addressing persistent barriers with such strategies, as well as other strategies tailored to specific contexts, could promote telehealth equity, enhancing access to maternal services for populations with the highest need.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241259858 - Supplemental material for The evolution of health system planning and implementation of maternal telehealth services during the COVID-19 Pandemic
Supplemental material, sj-docx-1-dhj-10.1177_20552076241259858 for The evolution of health system planning and implementation of maternal telehealth services during the COVID-19 Pandemic by Monisa Aijaz, Burcu Bozkurt, Arrianna Marie Planey, Dorothy Cilenti, Saif Khairat and Christopher M Shea in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241259858 - Supplemental material for The evolution of health system planning and implementation of maternal telehealth services during the COVID-19 Pandemic
Supplemental material, sj-docx-2-dhj-10.1177_20552076241259858 for The evolution of health system planning and implementation of maternal telehealth services during the COVID-19 Pandemic by Monisa Aijaz, Burcu Bozkurt, Arrianna Marie Planey, Dorothy Cilenti, Saif Khairat and Christopher M Shea in DIGITAL HEALTH
Footnotes
Monisa Aijaz: Conceptualization (equal), investigation (lead), formal analysis (lead), writing – original draft (lead). Burcu Bozkurt: Conceptualization (equal), investigation (supporting), formal analysis (supporting), writing – review, and editing (equal). Arrianna Marie Planey: writing – review, and editing (equal). Dorothy Cilenti: Conceptualization (supporting), writing – review, and editing (equal). Saif Khairat: writing – review, and editing (equal). Christopher M. Shea: Conceptualization (lead), funding acquisition (lead), supervision (lead), investigation (equal), formal analysis (supporting), writing – review, and editing (lead).
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Office for the Advancement of Telehealth (OAT), Health Resources and Services Administration (HRSA), US Department of Health and Human Services (Grant number 6 U3GRH40003-01-03).
Ethical approval
This study was deemed exempt by the Institutional Review Board at the University of North Carolina at Chapel Hill (#20-3350).
Guarantor
MA
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.