
Abstract
Objective
Stroke survivors often experience residual impairments and motor decline post-discharge. While digital home rehabilitation combined with supervision could be a promising approach for reducing human resources, increasing motor ability, and supporting rehabilitation persistence there is a lack of reviews synthesizing the effects. Thus, this systematic review and meta-analysis aimed to synthesize the effect of digital home rehabilitation and supervision in improving motor ability of upper limb, static balance, stroke-related quality of life, and self-reported arm function among stroke survivors.
Methods
Six electronic databases, grey literature, ongoing studies, and reference lists were searched for relevant studies. Two investigators independently reviewed titles, abstracts, screened full texts for eligibility and performed data extraction. Meta-analysis of 13 independent studies were grouped into four separate meta-analyses. The Grading of Recommendations, Assessments, Development and Evaluations (GRADE) tool was used for evaluating the overall quality of the evidence.
Results
Meta-analyses showed no statistically significant difference between intervention (digital home rehabilitation) and control groups (home training/clinic-based) of all outcomes including motor ability of upper limb, static balance, stroke-related quality of life, and self-reported arm function. In the sub-group analysis digital home rehabilitation was associated with better quality of arm use (standardized mean difference = 0.68, 95% confidence interval: [0.27, 1.09], p = 0.001).
Conclusions
This result indicated that digital home rehabilitation has similar effects and could potentially replace home training or clinic-based services. This review highlights better-targeted digital motor interventions to examine the effects of interventions further. The quality of evidence was moderate to high in motor and self-reported arm outcomes, and low for balance and quality of life.
Introduction
Stroke, a cerebral infarction, or haemorrhage in the brain, causes physical, cognitive, and somatosensory long-term disabilities for stroke survivors.1,2 Globally, it is estimated to affect 11 million people per year worldwide. 3 Many stroke survivors have residual functional impairments, where motor sequala is reported as the most common disability, 2 especially decreased unilateral hand function and strength. 4 An European longitudinal multicentre study showed that 63% of chronic stroke survivors lacked physical therapy and found a significant decline in four motor outcomes between six months and 5 years post-stroke. 5 While the recovery tends to be more pronounced during the acute and subacute stages of stroke, with remaining disabilities often becoming more permanent, rehabilitation programmes continue to demonstrate effectiveness during the chronic phase. 6 Previous studies indicated that telerehabilitation technologies in stroke care may serve as an efficient approach to meet these challenges.7–11
Remote stroke rehabilitation, or telerehabilitation, enables a possibility for continuous rehabilitation and supervision7,9,11,12 between stroke survivors and health care professionals in many fields of care. 13 Telerehabilitation, when compared to traditional training at health institutions, has been recognized as beneficial due to its convenience and ability to overcome socioeconomic, geographical, and cultural challenges. Additionally, it may help reduce disparities and promote equity. However, further work on infrastructure is necessary to ensure widespread accessibility and opportunity. 14
Current telerehabilitation technologies have advanced over the last years and span over synchronous solutions (e.g., videoconferencing) or asynchronous (messaging or data collection) towards remote monitoring and programmes on different digital applications.13,15 Further, the past Covid-19 pandemic has led to out-sourced digital rehabilitation where an expansion of new technologies have arisen, 15 characterized as decision support systems, motion detection and sensor-guided home exercises evolved by more volume, velocity, and variety and predictive artificial intelligence.16–18 However, the utilization of digital home rehabilitation programmes is advancing at a slow pace, and maintaining consistency in engagement with these solutions presents challenges. 9 An important criteria for success are integration with care models, deeper patient engagement and patient-centred care. 10 As a complement to simple telerehabilitation solutions self-managed digital rehabilitation programmes for improving motor function can provide more intensity, adherence, and progress to rehabilitation9,11,12,16 and is preferred as it is conducted in real-life environments for better skill transfer. 19 Also, it can improve self-care and empowerment for the stroke survivors.8,9 Digital rehabilitation coupled with telesupervision allows for thorough monitoring and personalized feedback on patients’ performance. It also provides the opportunity to address challenges and rectify ongoing issues related to patient engagement in digital training. 14 The expansion of digital home rehabilitation programmes also provides an opportunity to reframe the role of therapists with motor practice self-managed at home and therapist time allocated to remote supervision, monitoring, and motivation. In this flipped model of care, self-managed rehabilitation programmes require therapist support through supervision to attain successful behavioural change, 20 and to handle low adherence to self-rehabilitation. 6
Telerehabilitation is an emerging area of research, yet the effectiveness is conflicting, and the mode, delivery, content, and processes of digital services vary. 21 Among existing systematic reviews on digital stroke rehabilitation for motor function, some show results in favour of digital rehabilitation,22–26 and others show no difference compared to conventional care27–29 (Supplemental File 1 – Existing and ongoing systematic reviews and gaps in these reviews). In these studies, the digital rehabilitation programmes are either entirely self-managed or situated within health institutions, meaning that programmes require time-intensive therapist time. 20 Despite the extensive range of digital solutions for stroke telerehabilitation, there are currently few systematic reviews examining the effects of a more stable home setting, uniform technological applications, and specific rehabilitation interventions on the improvement of both motor and self-reported outcomes.
Although the research and clinical use of digital services in home settings are progressing9,11,12,16 only one study has reviewed interventions conducted at home. 28 This 2015 review reported equal benefits compared to conventional care but noted variable outcome measures, technologies and methodological issues of various study designs. 28 Additionally, in all the home interventions provided for stroke survivors none were coupled with telesupervision. Despite research on self-managed digital rehabilitation programmes outcomes that are self-reported are rarely addressed, such as quality of life (QOL). 30 To date, only one study reviewed QOL for post-stroke survivors and further research is advocated. 31 The use of self-reported outcomes in motor function rehabilitation for stroke are clinically important for considering the individual strategies towards their attitudes. It provides insights into the subjective impacts of their stroke and establish confidence to adopt healthy behaviours and accelerate rehabilitation. 32 Another advantage is that self-reported outcomes can be remotely measured in the digital rehabilitation programmes, which might reduce the frequency of the outpatient visits required. 33 Given the rapid development and limited evidence syntheses, this systematic review and meta-analysis evaluated the effectiveness of digital home rehabilitation and supervision in improving motor ability of upper limb and static balance (primary outcomes), in addition to stroke-related QOL and self-reported arm function (secondary outcomes) for stroke survivors.
Materials and methods
Design
This review was guided by The Cochrane Handbook for Systematic Reviews of Interventions 34 and followed the Preferred Reporting Items for Systematic Reviews and Meta-analysis. 35 The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022331724).
Eligibility criteria
Inclusion- and exclusion criteria based on PICOS format were used to identify studies.
The study population comprised home-dwelling stroke survivors (age ≥ 18 years) with no exclusion based on the type of stroke. Children under 18 were excluded from this review as the incidence of stroke in this population is low, and additional challenges and barriers to paediatric delivery of digital rehabilitation programmes might exist. Studies with participants in late sub-acute or chronic phase (more than 3 months after stroke) were included in accordance with a framework for post-stroke timepoints. 36 The stroke classification was defined due to this review's focus on a population often challenging to target after hospital discharge, where most rapid brain repair processes in the first weeks-to-months post-stroke have passed and thus many fail to progress. 36 Studies including mixed neurological populations combined with other conditions than stroke were excluded unless results of the stroke cohort could be extracted separately.
The interventions included digital rehabilitation programmes combined with telesupervision as communication technology (e.g., chat, video-consultation) used on the web or application on the phone conducted in the home setting or simulated home setting. For inclusion the intervention needed to target digital rehabilitation programmes aimed at improving activity and/or mobility, rather than simple communication with health care professionals (e.g., just video conference or education). In including supervision coupled with home-based rehabilitation programmes we attempted to control for amount of time with therapists allocated in conventional care. The intervention also had to be intended for participants with stroke and not just their caregivers. Advanced technologies of robotic technology, exoskeleton-based systems or electrical stimulation systems were not excluded from this review if they were delivered via telerehabilitation technologies and fulfilled additional inclusion criteria. Yet, prediction systems (e.g., risk factor assessment) outside the scope of this review targeting rehabilitation interventions were excluded.
Studies with a comparator of non-digital conventional care provided either at clinic-based settings or as home training was included. Among the post-stroke population, the accessible rehabilitation programmes are often delivered in outpatient settings after discharged to home and often with a combination of interventions for self-management and therapist interaction.
Primary outcome of interest was motor ability. Additionally, studies reporting one or more secondary self-reported outcome(s) were included but was not restricted to report additional outcomes. All study designs were searched, but this review included only randomized controlled trials (RCTs) or pilot RCTs. This is because the review aimed to assess treatment effects, and focusing primarily on randomized trials was considered feasible for the intervention of interest. 34
Search strategy
Six electronic databases of MEDLINE, Embase, CINAHL, The Cochrane Library, Scopus and Web of Science were searched from the inception of literature to 6 February 2024. An extensive search strategy was developed with experienced medical librarians consisting of various search terms related to specifications of stroke AND a broad inclusion of digital services, e.g., ‘telerehabilitation’, OR ‘ehealth’ OR ‘mhealth’, OR ‘Internet’, OR ‘fitness trackers’, OR ‘video games’. To specify the intervention towards home settings, a broad list of search terms on home was combined with the search. Subject heading trees were examined for any accurate subject headings to be added. RCT search syntaxes were also used. Secondly, grey sources such as websites from Google, European mHealth Hub, World Stroke Organization, National Stroke Associations, and other databases such as Open Grey, ProQuest Dissertations and Clinical Trials were searched for relevant trials. Additionally, we searched reference lists of single studies and systematic reviews. The search retrieved many protocols and authors of all retrieved protocols were contacted for available data and published results. Full search strategies can be found in Supplemental File 2 – Search strategies.
Selection process
Search results were exported and managed using EndNote 20 and then Rayyan as a screening tool. Duplicates were removed electronically and then manually. Two investigators (AHM and ZAT) independently reviewed the titles, abstracts, and then independently screened full texts for eligibility and performed data extraction. Both the initial and full-text screening processes were pilot-tested and discussed before further screening. Discrepancies were discussed with a third reviewer (HGH) in the full-text screening to reach consensus on the eligibility of the studies.
Data extraction and management
Two independent investigators (AHM and HXO) conducted data extraction using a pilot-tested template developed specifically for this systematic review inspired by Cochrane's data collection form for intervention reviews for RCTs only 34 (Supplemental File 3 – Data Extraction Form and Risk of Bias Tool). Key data on study eligibility, bibliographic data (author, publication year, and country), characteristics (objective, design, population size, and characteristics), intervention and comparison descriptions, all outcome measures and validity and reliability of the instruments used, and descriptive and statistical results were extracted. Authors were contacted by email if important data was missing. Finally, the study data details of the included studies were summarized in a table of characteristics (Table 1).
Characteristics of the included studies (population and intervention) (n = 13).

Abbreviations: FRCT: feasibility randomized controlled trial; RCT: randomized controlled trial; PRCT: pilot randomized controlled trial; BL: baseline; IG: intervention group; CG: control group; NR, not reported; GRASP: Graded Repetitive Arm Supplementary Programme; ROM: range of motion; ICN: Internet continuing nursing; CI/CIMT: constraint-induced (movement therapy); IADL: activities of daily living.
Methodological quality assessment
Using the Cochrane Risk of Bias Tool 1 and 2 34 (Supplemental File 3) two reviewers (AHM and HXO) independently assessed the methodological quality of the included studies for selection, performance, detection, attrition, and reporting bias. The studies were assessed for low, unclear, or high risk. Justifications for the assessments were documented in the data extraction form.
Synthesis and statistical analysis
Mean and standard deviations (SDs) were extracted for continuous variables. Differences between the effect of the intervention and the control on outcomes were calculated as standardized mean differences (SMDs) with 95% confidence intervals (CI) in RevMan due to different scales being used to report the same outcome. A weighted average of the intervention's effectiveness in each study was calculated as Hedges’ g, which adjusts for small sample bias, where 0.2, 0.5 and 0.8 corresponds to low, moderate, and high effect estimates respectively.
34
Medians were converted to mean by using equation (37), where a and b represents the minimum and maximum value respectively, and m represents median:
Results
Study selection
A total of 9873 trials were identified through search in six databases and 1575 additional records through other sources from inception of the databases to 6 February 2024. After removal of duplicates 6179 were screened by titles and abstracts. Among these, 6085 were excluded, 94 were sought for full-text retrieval and 50 assessed for eligibility based on different arguments (see Figure 1 PRISMA chart and Supplemental File 4 – Included and excluded articles). Finally, 13 RCTs were included in this review.

PRISMA flow chart summarizing the search process and outcomes.
Study characteristics
A total of 571 stroke survivors, 290 in intervention group and 293 in control group, from 13 RCTs from seven different countries were included in this systematic review. For each included study we identified the sample size (with attrition and adherence rate), stroke onset and subtype, descriptions of the technology and intervention details, regime, outcomes, timepoints and results (see Table 1 and Table 2 of included studies).
Outcomes and results of included studies (n = 13).

Abbreviations: FRCT: feasibility randomized controlled trial; RCT: randomized controlled trial; PRCT: pilot randomized controlled trial; BL: baseline; IG: intervention group; CG: control group; NR, not reported; GRASP: Graded Repetitive Arm Supplementary Programme; ROM: range of motion; ICN: Internet continuing nursing; CI/CIMT: constraint-induced (movement therapy); IADL: activities of daily living; FMA: Fugl-Meyer Assessment; WMFT: Wolf Motor Function Test; BBT: Box and blocks; MAL: Motor Activity Log-30; SIS: Stroke Impact Scale; TSRQ-15: Treatment Self-Regulation Questionnaire-15; EQA: Functional Exercise Compliance Test; MAS: Motor Assessment Scale; SSC: Self-efficacy; SS-QOL: stroke-specific quality of life; SIS: Stroke Impact Scale; eHealths: Electronic Health Literacy Scale; WBLSES: Web-Based Learning Self-Efficacy Scale; CAHAI-7: Chedoke Arm and Hand Activity Inventory; MAS*: modified Ashworth Scale; TIS: Trunk Impairment Scale; FIST: function in sitting; BBS: Bergs Balance Test; PASS: Postural Assessment Scale for Stroke Patients; 3-BBA: Brunels Balance Assessment (stepping); POS: Participant Opinion Survey; TUG: Timed Up and Go Test; 6MWT: 6 min walk test; MBI: Modified Barthel Index Scale; +++: statistically significant effect; ++: greater improvement in intervention group than control but between group difference not significant; +: significant improvement in both groups but between group difference not reported or not significant; -: no reported change in the group(s) or improvement just in control group; x: effect-related data not shown; ^: within-group improvement not significant.
The sample size of the studies varied from 11 40 to 193 20 depending on whether it was a feasibility or multi-site RCT. Among the trials reporting attrition, the mean rate was approximately 17% and below the considered attribution rate of 20%, which raise concerns about the study validity. 41 There was a large variation in reported adherence from 30% to 98%. All trials included participants after sub-acute or chronic stroke mostly reported in years, except one trial of sub-acute participants of approximately four months onset. The remaining trials included participants with a mean stroke onset of 3.6 years. Across trials, the majority of the included stroke participants had an ischaemic subtype. All included studies targeted motor rehabilitation, with three studies20,42,43 also targeting digital stroke education, such as stroke prevention, risk factors and stroke knowledge. Most of the studies targeted upper limb motor training,13,15,19,20,40,42,44–47 two studies aimed for static sitting or standing balance,33,48 and one trial aimed for motor function without further description of intervention aim. 32 We categorized the included trials into types of intervention, technology, and control (Supplemental File 5 – Categorization of studies). Most of the included trials used virtual reality (VR) or exergaming as an intervention,13,20,33,42,44–47 four used a stand-alone app or platform15,19,32,48 and one used app and VR in combination. 40 One study used a tele-based gaming with constraint-induced movement therapy (CIMT) on a workstation. 47 Also one of the VR trials had the features of CIMT integrated into the solution. 20 The four app solutions contained supervision of educational videos, remainder functions, and data tracking. Among these one app was connected to a wearable with sensor to detect range of motion. 19 Among the gaming programmes most studies used customized rehabilitation software (e.g., Jintronix system, Gertner system and Saebo software), only one used more commercial gaming-based solutions. 42 Among the gaming-based solutions some used connected devices; one used PlayStation Move controller [Sony] or trackpad, one used magnetic receiver attached to real objects, one used task stations with built-in sensors, one used a standing frame with a build-in 3-axial tilt/inclination sensor and another a Saebo VR-glove. Five studies also used motion capture tracking, such as the Kinect system.13,40,44–46
All trials contained interventions combined with telesupervision, where 10/13 used a combination of asynchronous (data storing) and synchronous communication (e.g., videoconferences) and 3/13 only used asynchronous communication via chat.13,15,49 Additionally, many rehabilitation systems monitored the patient's data and made asynchronous adjustments in accordance with performance. The aim of the videoconferences were to communicate and observe participant's performance, adjustments on progressive level and intensity, reviewing treatment plans based on needs and goals, communication around barriers in daily life and general encouragement to use the system. Two studies also used motivational interviewing20,40 and two other studies used a behavioural contract as behavioural interventions.42,47
Total number of weeks of treatment varied from two weeks to a maximum of eight weeks with a mean duration of 5 weeks. The daily duration of the intervention varied from 15 min to 3.5 h. In the more time-consuming CIMT programmes the duration were frequently set to 45 min. Almost all trials had timed-matched controls, and many trials had dose-matched controls. One trial had longer duration and dose in the control group of a conventional balance training programme. The control groups followed programmes either as home training (n = 4) or in clinic-based settings (n = 4), or where half of the intervention was conducted at home and the other in a clinic-based setting (n = 3). Two studies lacked descriptions of the setting and content. The content and intensity in the control groups varied. Whereas some participants in the control group were provided with handbooks of knowledge and exercise, others followed intensive programmes as conventional CIMT, Graded Repetitive Arm Supplementary Programme and task-specific training.
All trials assessed motor ability, either upper limb motor ability through The Fugl-Meyer Assessment of Motor Recovery after Stroke (n = 7), Wolf Motor Function Test (n = 3), Motor Assessment Scale (n = 1) or Berg's Balance Test (n = 2). Eleven studies also assessed self-reported outcomes as the QOL by Stroke Impact Scale (n = 3), Stroke-Specific QOL (SS-QOL) Scale (n = 1), or self-reported arm function by using Motor Activity Log (n = 6), or ABILHAND (n = 1). Five studies reported more than one self-reported outcome, a combination of the above or other (see Table 2).
Most trials reported positive results in within-group differences except two trials, however three studies reported significant between-groups differences in favour of digital rehabilitation in motor ability outcomes. Yet, in self-reported outcomes five trials reported significant between-group differences or greater improvements in favour of digital rehabilitation.
Meta-analysis
In three of the included studies mean differences and SDs could be extracted directly.15,19,42 In four studies, the mean difference was calculated by subtracting the post-intervention mean from the pre-intervention mean and a combined SD calculated manually.20,33,46,48 In two studies full datasets of outcome scores for every individual were provided and could be calculated in excel.13,40 In one study median and interquartile range were reported and had to be manually converted to mean difference and SDs. 45
In two other studies mean difference could be extracted directly, but CIs were used. CIs had to be calculated to SDs by subtracting the upper CI with the mean and then dividing it by t-distribution to receive standard error and then multiplying the standard error with the square root of the number of participants.44,47 In one last study SD was not reported, only p-values, sample size and difference in means. 32 To calculate SD we used RevMan's additional calculator and used numbers calculated from between groups by finding t-value, standard error and using standard error to find SD. 34 Subgroup analyses were performed for the self-reported arm outcome by grouping data with target intervention and duration of intervention.
Methodological quality and risk of bias assessment
Two reviewers independently assessed the methodological quality of the included studies by using Cochrane's Risk of Bias tool (RoB) 1 as the version integrated in Rev Man 5.4 (see Supplemental File 6) and the updated assessment of RoB 2 (see Figure 2). Generally, there were low risks across various items in RoB 2. In RoB 2, low risk of bias was consistent across the studies for randomization process, deviations from the intended interventions and missing outcome data, except in two trials with some concerns related to allocation sequence and lack of appropriate analysis used to estimate the effect of assignment to intervention respectively. More concerns were raised in three studies due to measurement of the outcome and selection of the reported result due to lack of blinded testers and pre-specified analysis plan that was finalized before unblinded outcome data were available for analysis. Almost every trial could not fulfil blinding of participants and personnel due to the nature of interventions, except in one trial where participants were masked to study hypothesis.
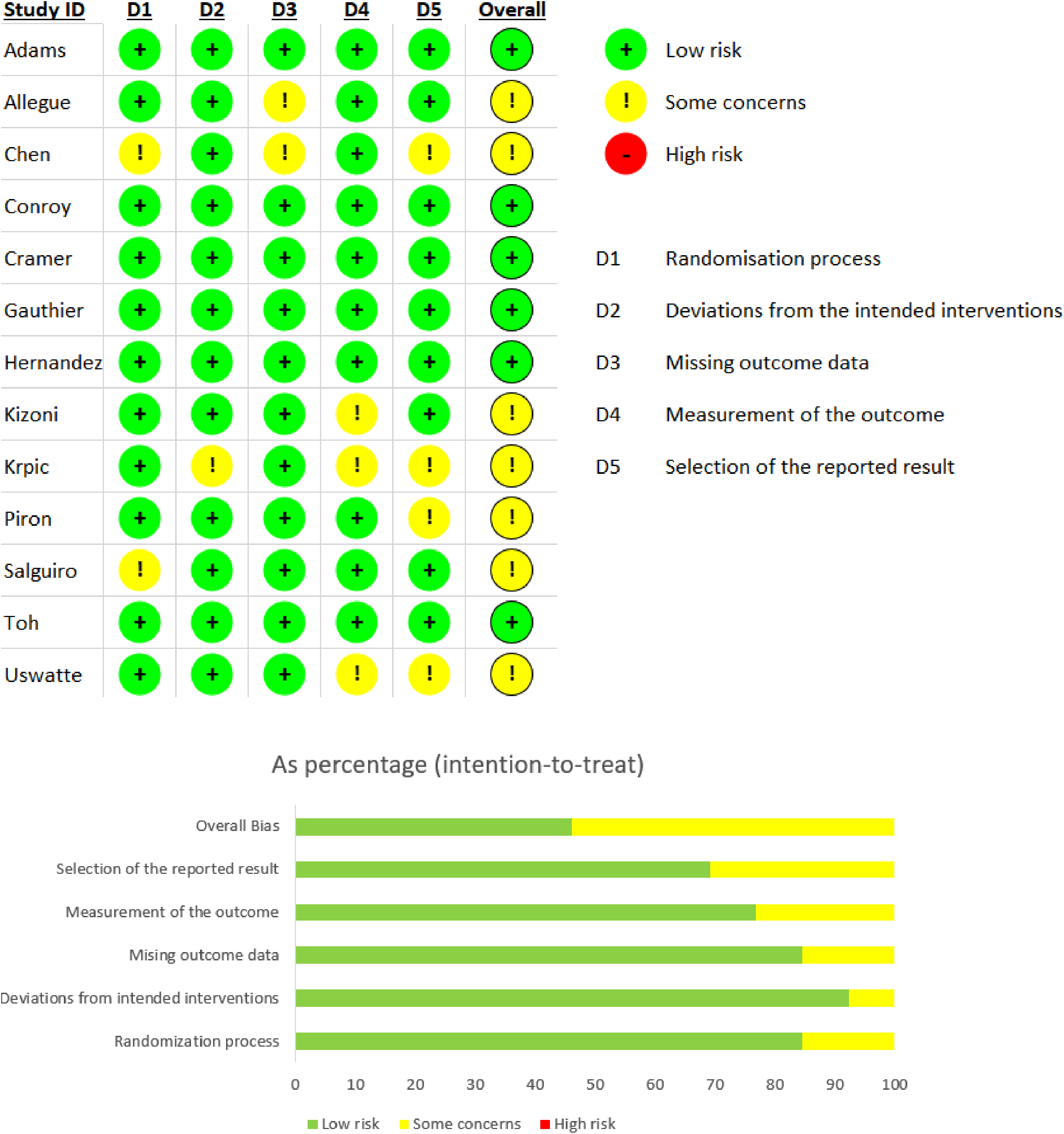
Risk of bias (RoB 2) summary of each included study and overall result (percentage).
Effects of digital home rehabilitation and supervision for post-stroke survivors
Primary outcome: Motor ability for upper limb and static balance
All 13 studies measured motor ability outcomes, mostly for the upper limb. We separated the motor ability outcomes into two meta-analyses, one analysis for the motor ability of upper limb (n = 10), and one analysis for static balance (n = 3). One of the studies measured everyday motor function and was therefore pooled with other studies measuring static balance as outcome. Ten studies measuring motor ability of upper limb (Figure 3(A)) were pooled to conduct a meta-analysis with 396 participants. The effect size was 0.09, 95% CI [−0.15 to 0.34] and not significant (p = 0.46), yet with low heterogeneity (I²=25%). Due to low heterogeneity, no sensitivity analysis was performed. However, a subgroup analysis was performed to provide estimates of treatment effects based on the comparison types of control groups (either located in home, clinic-based or combined settings). There was no statistically significant subgroup effect (p = 0.50, analysis only presented in Supplemental File 7), suggesting that the difference between controls in home or clinic-based settings did not modify the effect of digital rehabilitation. However, a smaller number of trials and participants contributed data to the different subgroups, meaning that the analysis may not be able to detect subgroup differences.

Forest plot: Meta-analysis for all outcomes. (a) Motor ability of upper limb (the higher score the better). (b) Static balance (the higher score the better). (c) Stroke-related quality of life (the higher score the better). (c) Self-reported arm function (the higher score the better).
Three studies measuring static balance (Figure 3(B)) were pooled in another meta-analysis with 123 participants. The effect size was 0.45, 95% CI [−0.14 to 1.05], and not significant (p = 0.13), with a moderate heterogeneity (I²=51%). It was decided to include studies with control groups with both home-based conventional care and in clinic-based settings as a comparison. In a sensitivity analysis, this was explored to see whether this decision affected findings and caused heterogeneity. Unlike the other studies, Krpic et al. compared their intervention with a control group receiving conventional therapy in a clinic with a larger training dose and duration and removal of this study reduced the heterogeneity to 0%. While a statistically significant effect (SMD = 0.72, 95% CI [0.33 to 1.11], p = 0.0003) appeared after sensitivity analysis (Figure 4(A)), this difference should be interpreted with caution as the sensitivity analysis was performed to explore heterogeneity and the removal of the study reduced an already small sample size.

Forest plot: Sensitivity analysis for static balance, stroke-related quality of life and self-reported arm function. (a) Static balance. (b) Stroke-related quality of life. (c) Self-reported arm function.
Secondary outcome: Stroke-related QOL
Four studies measuring stroke-related QOL (Figure 3(C)) were pooled to conduct a meta-analysis with 274 participants. The effect size was 0.15, 95% CI [−0.23 to 0.53] and not significant (p = 0.44), with a moderate heterogeneity (I²=56%). Sensitivity analysis of the outlier did not change the heterogeneity significantly, but an exploration of quality-of-life instruments and exclusion of Chen et al. 2022 being the only one using different instruments than the other studies reduced the heterogeneity to 45% (Figure 4(B)). Again, subgroup analysis was performed to provide estimates of treatment effect for clinically relevant subgroups of patients in the control group, which showed subgroup differences were non-significant (p = 0.99, see Supplemental File 8). A small number of trials and participants contributed data to the different subgroups potentially hindering to detect subgroup differences.
Secondary outcome: Self-reported arm function
Seven studies measuring self-reported arm function (Figure 3(D)) were pooled to conduct a meta-analysis with 199 participants. The use of home-based digital motor rehabilitation had a small, but not statistically significant effect in improving self-reported arm function (SMD = 0.39, 95% CI [−0.09 to 0.88], p = 0.11, I2 = 59%). Also, there was statistically significant moderate heterogeneity (p = 0.02, I2= 59%). This review included studies with a late subacute and chronic stroke population. In a sensitivity analysis, the first study with the outlier was removed and reduced the heterogeneity to 40%, without changing the effect estimate to a large degree (SMD = 0.25, 95% CI [−0.16 to 0.66], Z = 1.20, p = 0.23) (Figure 4(C)). We performed subgroup analysis to investigate sources of heterogeneity, to generate hypotheses and to provide estimates of treatment effect for clinically relevant subgroups of patients in the control group (Supplemental File 9). The test for subgroup differences indicated that there was no statistically significant subgroup effect based on comparison types of the control group (p = 0.35), instrument use (p = 0.40), or length of intervention (p = 0.20). However, it is interesting to note that the pooled effect estimate for instruments to measure the quality of arm use showed a significant effect (SMD = 0.68, 95% CI [0.27 to 1.09], p = 0.001). An uneven covariate distribution for particularly length of intervention time was present, meaning that the analysis was unlikely to produce useful findings.
In total, these results suggest that digital home rehabilitation and supervision compared to conventional care showed similar effect.
Overall quality of evidence
Table 3 summarizes the overall quality of evidence in the GRADE assessment of the four different outcomes. In this review, the overall methodological quality is moderate, and the quality of evidence varies from low to high. In all GRADE assessments the outcomes scored low on risk of bias. The motor ability of upper limb showed the highest certainty based on low inconsistency, imprecision and similarity in population, interventions, and outcomes. The exception was some variations in content and dosage in the comparison group as explained earlier, which was evident in the three other evaluations of outcomes as well. The self-reported arm function showed the second highest and moderate certainty of evidence based on low imprecision and indirectness, but moderate inconsistency, which we downgraded due to a moderate heterogeneity explored in subgroup analyses. Static balance and stroke-related QOL showed respectively low and very low certainty of evidence due to downgrades in all or some criteria suggesting for the latter the confidence in the effect estimate was low and future studies may change the effect estimate.
Overall quality of evidence assessment.

CI: confidence interval; SMD: standardized mean difference; PICO: patients, intervention, comparison, outcome. Explanations. (a) We downgraded for inconsistency due to a low number of studies, small sample size, moderate heterogeneity, and variation in point estimates. (b) We downgraded for indirectness due to variation in intervention and outcome. The population and stroke onset are quite similar, but the interventions focus on either sitting or standing static balance or is lacking information of intervention with different technology app versus virtual reality. (c) We downgraded for imprecision due to a small, pooled sample size that may have affected the reported outcome. (d) We downgraded inconsistency due to a moderate heterogeneity, which we explored heterogeneity in subgroup analyses by PICO.
Discussion
This review demonstrated that in existing studies digital home rehabilitation compared to the control group (home training/clinic-based) showed similar effects to all outcomes. This result indicated that digital home rehabilitation has the potential to replace home training or clinic-based services and was further investigated separately in subgroups for outcomes (see Supplemental Files 7–9). Still, the number of stroke survivors included in these studies were limited, which might influence the results. When comparing this overall similar efficacy with studies with controls situated in clinic-based or combined settings these results are promising. As these studies contained primarily dose-based groups except one study with even with higher training dose among controls, this result indicates that the amount of time and resources therapists interact with patients in clinics are as effective as when digitally self-managed at home with less supervision. However, when comparing the efficacy with the studies where controls trained at home with less or no supervision the results are less encouraging due to expenses related to the digital home rehabilitation programmes. Still, the results indicated a tendency of higher effect in favour of digital home rehabilitation, but with a wide CI. Most of the participants included in our review study, were middle-aged with mostly chronic ischaemic stroke partly adherent to programmes. These characteristics suggest that our results can have implications for elderly stroke participants in the moderate chronic phase.
Consistent with our findings, other systematic reviews and meta-analysis found equivalent effects between digital home rehabilitation compared to the control group on motor ability for the upper limb and balance.27,50,51 Also, other reviews with narrower interventions and particular use of VR compared with an alternative intervention or on upper limb function and activity showed no significant difference.52,53 Despite observing similar effects, one review by Schröder et al. 51 calculated a cost-efficient effect of tele-rehabilitation and VR in balance training compared to traditional therapist-supervized care.
Our meta-analysis on static balance and lower limb function only included a few studies32,33,48 and similar reviews on interventions for lower limb functions are scarce.50,54,55 A possible reason for few studies on lower limb function might be safety precautions as there is 73% increased risk of falling after regaining gait function for stroke survivors. 54
In our review, the meta-analysis showed inconsistent results and no effects of digital home rehabilitation and supervision in improving levels of QOL. Variation in the measurement of QOL might be one reason to the result's heterogeneity. Secondly, QOL as an outcome assessed on group level is not sensitive to change over intervention periods in between 2 to 8 weeks. To fully evaluate the effect of QOL for stroke survivors, individual-level assessments and possibly in combination with group level is more useful in clinical practice. We also highlight using valid and reliable instruments for stroke survivors and careful consideration into using generic or specific QOL instruments. It has been argued that generic measures fail to measure content validity and the important features of impairments specific for the stroke population. 31 However, this review evaluating the psychometric properties of both generic and specific QOL instruments for stroke survivors found that EQ5 had highest and moderate quality evidence for 3/10 psychometric properties being test-retest reliability, construct validity and responsiveness. Stroke-specific QOL (SS-QOL), as one of the used QOL instruments in this review, had moderate evidence for internal consistency and conflicting evidence on construct validity. 31
Our meta-analysis showed a small, not significant, but potential effect in improving self-reported arm function. Subgroup analysis of this outcome was explored to generate hypothesis (Supplemental File 9) and showed diversity in effect estimates for instruments measuring quality of use and quantity of arm use. It was a significant and higher moderate effect in favour of digital home rehabilitation in improving quality of arm use rather than amount of arm using the instrument Motor Activity Log-30. One possible explanation for this result might be a variation of intensity in rehabilitation among studies reporting the different items of the arm function instrument and ability to target effect. Notably, the three studies reporting on quality of arm use all featured high-intensity digital home rehabilitation aiming for repetitive range of motion using either VR or digital constraint-induced therapy. Conversely, the studies focusing on quantity of arm use displayed a wider variation in training intensity, both in the intervention and control groups. This suggests a possible, but inconsistent, relationship between meaningful intensity and challenge in digital rehabilitation and its’ effect on arm use. This is consistent with a systematic review on AR and VR in hand rehabilitation reporting a positive relationship between patients’ motivation and use of digital rehabilitation with challenge. 4 Yet, few studies were pooled in this subgroup analysis and makes it difficult to identify independent effects. The effect estimate in this meta-analysis exceeds the threshold for minimal detectable change, yet not minimally clinically important difference for patients post-stroke. 56 There is no other review assessing self-reported arm use. It is an important outcome in terms of activity and participation in the International Classification of Functioning Disability and Health (ICF) framework well adapted in clinical settings and research. So far, most studies have reviewed outcomes related to body function, body structure, and activity, but fewer on participation. 6
In our review we found no significant effect in the chosen outcomes in favour of digital home rehabilitation, however within the included studies there were other outcomes not in scope of this review that proved significantly effective between groups, for instance, kinematic outcomes with significant effects in shoulder range of motion, 19 compliance, 32 self-efficacy,32,40 or in motivation. 40 Self-reported outcomes of self-efficacy and motivation are also often lacking in systematic reviews, yet are highly relevant due to the chronic implication of stroke with individuals needing to persist with long-term rehabilitation despite small and slow progress. 55
Digital home rehabilitation in this review
The highlighted principles underlying effective neurorehabilitation are task-specific, goal-oriented, intensive training with implicit and explicit feedback. 57 Among the included studies in this review, all interventions aimed for task-specific motor rehabilitation. However, the intensity of motor tasks in the rehabilitation programmes varied significantly. The training dosage in the intervention groups varied from low intensity of 15 min five days a week in three consecutive weeks in one study, 33 to one hour five days a week for a month in another study. 46 Some research point to that intensity while training has a larger impact on motor learning than duration of intervention. 57 The duration of interventions was also explored in a subgroup analysis in this review (see Supplemental File 7), indicating no significant difference in effect estimate between whether interventions lasted more than four weeks or less. However, variations in the interventions appear according to motor relearning to have an impact on efficacy. 57 In this review there was less variation in the rehabilitation programme by Allegue with fewer games 40 in comparison to many IADL activities in studies by Adams 44 and Cramer 42 respectively. Two other studies explicitly also described different tasks based on the type of motion required with varying movement speed, range of motion, target size or level of cognitive demand.20,45 Another important principle is the ability to grade the difficulty in terms of progression, 57 where feedback, challenge, and individualized difficulty are known features of motor learning. 58 Mostly this was adjusted through telesupervision, yet in two studies19,40 level of difficulty, speed, and trajectories of arm movements were remotely and asynchronously adjusted by a therapist to obtain optimal challenge according to the participants’ improvement. In one study this kinematic visual feedback was evident for both the participant and the supervising therapist. 19 In seven out of the eight studies on exergaming or VR there were feedback in the solutions with both explicit knowledge of results (e.g., game scores) and/or implicit feedback of knowledge of performance (e.g., movement quality).13,33,40,42,44–46 Explicit motivational interviewing as feedback was present in four studies.20,40,42,47 Half of the studies included also described possibility of monitoring performance and progression, but there were large variations in possibility of reward and automatic level adaptions. The monitoring of performance, such as speed, accuracy, and score, was mainly available for the therapist33,40,42 or on company servers, 13 only few described accessibilities for the patient. 45 Also, the reward and automatic level adaptions were mainly absent except in three studies.13,44,45 The implementation of these suggested principles enhances a disability adaption necessary for scalability of purpose-designed virtual environments and increases the engagement and persistence in the tasks. 6 This intrinsic motivation can in return lead to higher adherence 55 as well as providing learning through cognitive processing. 57
Consistent with motor learning theory it was found in existing systematic reviews and meta-analysis that personalized VR games have more positive impact on motor function of stroke survivors compared to commercial systems due to greater emphasis on number of repetitions, feedback, and motivation.58,59 There is some evidence in the effect of VR to induce neural plasticity changes and functional improvements from acute and chronic phase of stroke.57,60 More advanced VR, combined with augmented reality (AR) imposing a computer-generated image of the user's real motions, seems to have benefits exceeding traditional VR. 6 In this current review, AR was accessible in six out of eight included VR studies enabled by motion tracking either by Kinect camera or other 3D motion tracking. A review reported that this feedback in of AR and VR in hand rehabilitation was linked to the patients’ motivation and adherence. 4 Looking at the results of the individual studies of VR in this review (see Table 1b) suggest a stronger effect in favour of digital home rehabilitation, except in one study 33 lacking dose-matched training between groups. Interestingly, the study by Adams 44 contained most of these recommended principles and gained a significant higher positive effect than the other trials in the meta-analysis for evaluating motor ability for upper limb. Similarly to this specific glove rehabilitation interacting with VR 44 one review 4 explained the effectiveness of haptic gloves by abilities for free hand movements in natural interactions giving the patient control over the technology. However, more studies with appropriate high intensity would need to be included to confirm this hypothesis.
All included studies in this review used a telesupervision but with only partly descriptions on content. Also, the amount of supervision varied between studies. For instance, one study only provided limited supervision, 13 yet others supervised close to three times a week during the intervention period. 40 There is evidence that incorporating motivation and behavioural interventions within motor rehabilitation emits clinically meaningful progression in function and ADL tasks. 20
Another important factor to consider is whether the included studies compared post-training and retention after a gap of no training. In this review four studies did not have a follow-up testing. Among the studies with follow-up and a continued effect of the intervention suggests how well the trained movements were learned after a retention gap.
Strengths and limitations
A strength of our review is a highly comprehensive search strategy across six databases covering grey literature and detailed interpretation of the results in the context of other evidence. This review has some limitations related to the chosen eligibility criteria and the quality of studies reviewed. First, most of the included RCTs in this review have small sample sizes which together with a relatively small amount of included RCTs might lead to underpowered results and limited statistical validation. Second, some included studies lacked description of content, dose and setting of interventions mostly related to the control groups, which makes it difficult to compare the training dose of the training programme and the interaction with therapists between intervention and control group. We chose to include stroke survivors living at home, but where some in the control group received training at home and others as outpatients at rehabilitation centres, which is the natural context of post-stroke rehabilitation. However, these two different types of control group and lack of clear descriptions in the studies lower the internal validity to some degree. We excluded studies published in languages other than English and thus some relevant studies might be missed. Due to the context of digital rehabilitation programmes delivered in the home setting we added search terms of the home to the search strategy. We are aware that this choice could lead to missing few relevant articles. To ensure all relevant studies were included we searched reference lists in all relevant existing systematic reviews and included RCT studies. Consistent with findings in this and other reviews digital home rehabilitation can entail various technologies for upper limb and lower limb aimed at improving different outcomes. The amount of heterogeneity in this review was handled by separating outcomes in different meta-analyses.
Conclusion
This current systematic review and meta-analysis demonstrated that home-based digital motor rehabilitation and supervision lead to similar effects compared to the control group (home training/clinic-based) in improving the motor ability of upper limb, balance, QOL and self-reported arm function. These results suggest that digital home rehabilitation solutions for stroke population have the potential to replace conventional training at home or in clinic-based settings. Studies providing many technological features targeting motor learning principles seems feasible for ensuring motivation. Still, dynamic solutions that encourage and engage participants with home motor rehabilitation are warranted. Rehabilitation games and VR home solutions are better targeted and might be a feasible and promising digital approach for supporting people with post-stroke impairments in the future. Still, there is a need for RCT studies of more advanced motor features (including upper limb, lower limb, social, communication and feedback functions) with particular attention to training dose and relevant and meaningful outcome effects for the stroke survivor. Further investigation of instruments for arm function as a potential rehabilitation outcome might be relevant to assess in solutions targeting upper extremity. Combined with studies of larger sample size and more specific inclusion criteria to obtain more homogenous groups, this can potentially elucidate the direction of effect favouring digital home rehabilitation.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241256861 - Supplemental material for Effectiveness of digital home rehabilitation and supervision for stroke survivors: A systematic review and meta-analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076241256861 for Effectiveness of digital home rehabilitation and supervision for stroke survivors: A systematic review and meta-analysis by Ann Marie Hestetun-Mandrup, Zheng An Toh, Hui Xian Oh, Hong-Gu He, Anne Catrine Trægde Martinsen and Minna Pikkarainen in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241256861 - Supplemental material for Effectiveness of digital home rehabilitation and supervision for stroke survivors: A systematic review and meta-analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076241256861 for Effectiveness of digital home rehabilitation and supervision for stroke survivors: A systematic review and meta-analysis by Ann Marie Hestetun-Mandrup, Zheng An Toh, Hui Xian Oh, Hong-Gu He, Anne Catrine Trægde Martinsen and Minna Pikkarainen in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank the Oslo Metropolitan University Medical Library team, particularly Malene Wøhlk Gundersen and Anne Tangen, for their guidance, conduction, and advice on the search strategy for this review. The authors would also like to acknowledge Professor Milada Cvancarova Småstuen from Oslo Metropolitan University for lending her expertise in the meta-analysis.
Availability of data
The search strategy and details of the quality assessment of each study are available in the supplemental materials. Other data will be made available up request to the author.
Contributorship
AMHM, HGH, ACTM and MP conceptualized and designed the study. AMHM and ZAT researched literature and conceived the study. HXO contributed to data extraction. All authors were involved in data analysis. AMHM wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AMHM.
Registration and protocol
The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022331724).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.