
Abstract
Background
Amyotrophic lateral sclerosis disease (ALS) is also called the disease of a thousand farewells. Consequently, it is important to offer supportive care interventions that can be applied continuously during the whole course of the disease. People with ALS are interested in complementary and integrative medicine. Due to ALS’ progressive nature, digital solutions might be most feasible and accessible for people with ALS in the long-term.
Objectives
In our study, we explored with stakeholders which digital complementary and integrative medicine interventions and formats are considered as supportive for people with ALS, and which settings are needed by the people with ALS to incorporate the interventions in everyday life.
Methods
We used a participatory research approach and conducted a stakeholder engagement process, applying a design thinking process with qualitative research methods (interviews, workshops).
Results
Due to the unpredictable course of the disease on their loss of abilities, people with ALS welcome online settings because they are accessible and easy to implement in their daily life. Stakeholders considered the following implementation factors for a complementary and integrative medicine intervention as essential: short-term realization of planned interventions, short duration of interventions, and user-friendliness in terms of accessibility and applicability. Concerning the complementary and integrative medicine interventions, the people with ALS preferred mind body medicine interventions, such as breathing, mindfulness and relaxation exercises.
Conclusions
Short-term treatment intervals and short online mind body medicine interventions align with the needs of people with ALS. The complementary and integrative medicine interventions as well as the digital infrastructure must meet the special accessibility and applicability needs of people with ALS.
Keywords
Introduction
Amyotrophic lateral sclerosis (ALS) is a rare, incurable, fatal disease. 1 Known in popular media as the “disease of a thousand farewells,” ALS is progressive, and results in the deterioration and loss of function of the motor neurons in the brain and spinal cord, leading to total paralysis, also of the respiration. 2 There are three different forms of progression: spinal, bulbar, and respiratory; potentially accompanied by the dominance of upper or lower motor neurons or flail leg or arm syndrome.1,2 Life expectancy after diagnosis is on average between two to five years.1,2
As ALS is incurable and progressive, symptom management, coping, preserving quality of life, and promoting well-being practices are important treatment goals.3–7 For that reason, people with ALS are interested in complementary and integrative medicine (CIM) as supportive therapy.3–5
Systems, therapies and products that are not generally considered part of conventional medicine are often summarized under the terms “complementary” (in addition to conventional biomedical care) or “integrative” medicine.8,9 Integrative medicine includes evidence-based practices, therapies, or products that are used in coordination with conventional medicine.8,9
As part of potentially suitable CIM interventions towards the above treatment goals, mind body medicine (MBM) interventions seem especially promising.3,5,10–12 Related to salutogenesis as resource-oriented concept of human health and well-being, MBM is an integrative concept that connects body and mind, and teaches self-care.13,14 Multimodal MBM therapy concepts aim at symptom management, stress reduction, enhancing quality of life, fostering well-being, and strengthening resilience, self-efficacy and disease coping.13,14
Due to ALS’ progressive nature, it is important to offer sustainable interventions that can be executed continuously during the entire course of the ALS disease.15–18 In this regard, digital solutions might be more feasible and accessible for people with ALS in the long-term.3,15–19 They can reduce the burden of travel and accessibility to clinic buildings, and they offer additional technical solutions for paralyzed people with ALS.12,18,19
In ALS research, as in health research in general,20,21 there is a growing awareness of the importance of stakeholder engagement and patient and public involvement (PPI), which share the same aims and methods. 22 To date, several ALS stakeholder initiatives have been established to shape and inform ALS research.22–24 They aim at identifying research topics that are important to the people affected by ALS, foster the participation in clinical trials, and enhance the awareness of study results by different science communication strategies.22–24
Independent of the health conditions being studied, there are shared challenges for stakeholder engagement, and PPI in general, such as human and financial resources, power imbalances, shared language, and conflicting interests.25–27 A major challenge for ALS stakeholder engagement is accessibility in terms of technology and infrastructure due to the disabilities that evolve from the progression of the disease in people affected by ALS. 22 This includes, for example: wheelchair accessible buildings, adapted computer mice and keyboards, high-tech augmentative and alternative communication technologies, voice operating software, and offering different means of communication between the researchers and the participants adapted to the constraints of the people with ALS. 22
In our study, we explored with stakeholders which digital complementary and integrative medicine interventions and formats are considered as supportive by people with ALS, and which settings are needed by the people with ALS to incorporate the interventions in everyday life.
Methods
Participatory research process
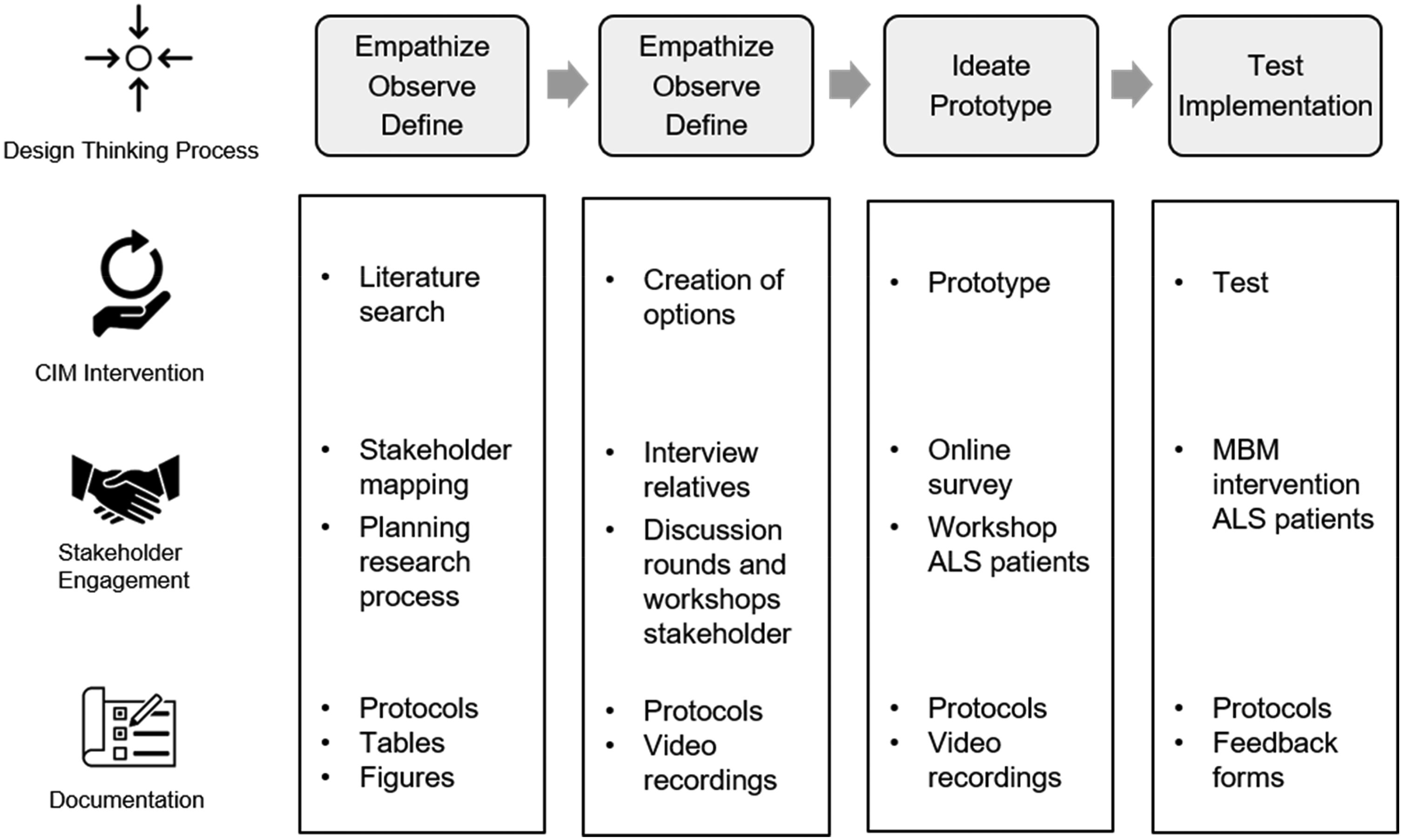
We conducted a participatory research process in 2021, with onsite and online meetings, interviews and workshops.20,28–31 We applied two methods: a design thinking process to prototype the CIM intervention (see Figure 1), 32 and “rapid qualitative evaluation” to document the research process. 33
Design thinking process with stakeholders.
A typical design thinking process is characterized by seven phases, which rather than being linear, usually are of iterative nature: (1) empathize, (2) observe, (3) define, (4) ideate, (5) prototype, (6) test, (7) implement. 32 Through creating options, ideating, prototyping, and testing, the CIM interventions for people with ALS matured from a literature overview into a participatory process with stakeholders. Figure 1 shows how the different design thinking steps are related to different stakeholder activities, to the creation of the CIM intervention, and how the process was documented.
We used a purposive sampling strategy 34 contacting different institutions and persons: three Swiss ALS patient organizations, the University Hospital Zurich, the University of Zurich, and personal professional and private contacts.
An external moderator fostered our entire process to enhance communication and participation between the researchers and the stakeholders, and to prevent power imbalances. He was experienced in working with vulnerable groups, although he had no previous experience of working with people with ALS.
Inclusion and exclusion criteria
We searched for adult people with ALS (≥18) interested in co-creating a CIM intervention through a design thinking process. We included people with ALS independent of their form of progression, disease status, and treatment. Furthermore, we searched for adult (≥18) relatives, health professionals, participatory and implementation research experts to further inform our research.
People with ALS unable to follow the study procedures due to limited German language skills or cognitive impairments were excluded.
Data analysis
To analyze the qualitative data, we followed the method of “rapid qualitative evaluation”. 33 We summarized and compiled interviews, meetings, and workshops, created spreadsheets for overviewing data, and wrote research diaries to document informal email or phone discussions with stakeholders. We used “survey monkey” 35 to collect the participants’ views on some aspects prior to the workshops. During the videorecorded workshops, we worked with “miro board” 36 to visualize the ongoing discussion. The three authors performed an intersubjective validation process for each step of the data analyses, and the participating people with ALS tested the prototype.32,34,37 We used the consolidated criteria for reporting qualitative studies (COREQ). 38 Find the checklist in appendix 1.
Ethics
We submitted the study synopsis to the Ethics Committee of Zurich, Switzerland, and after review, they stated that the study does not fall under the regulation of the Human Research Act of Switzerland (BASEC-Nr. Req-2021-00673). We obtained written informed consent from people with ALS and documented oral consent from all other stakeholders for participation and scientific publication. All data was anonymized.
Setting of the study
The Institute of Complementary and Integrative Medicine of the University Hospital Zurich is specialized in mind body medicine (MBM), and is continuously expanding its digital health service offerings for patients. The impact of the COVID-19 pandemic, and the subsequent progress in digital infrastructure, billing, and reimbursement possibilities of digital health interventions 39 accelerated the implementation of digital health services for patients.
Results
In total, 19 stakeholders participated in the project. The stakeholder groups are shown in Table 1, the patients’ characteristics in Table 2. Different stakeholders belong to more than one stakeholder group, but are listed with their main stakeholder group identification and role within the study.
Stakeholder groups.

Characteristics people with ALS (n = 7).

Creating options of the CIM intervention – The empathize, observe and define phases of the design thinking process
The aim of the first phase in the development of a CIM intervention was to create an intersection between the current state of research from the literature and the feasibility of potential CIM interventions in the context of our clinic.
Within the research team and together with the process moderator, we defined different levels of “feasibility” that future CIM interventions should meet:
Does the intervention under consideration meet the needs of the stakeholders, especially for people with ALS? Is there clinical evidence for the intervention under consideration? Does the research team and the participating stakeholders of the project consider the outcome of the intervention under consideration important and effective? How far is the intervention under consideration culturally and politically accepted in the region where the study is conducted? Within the study center and the clinic, is there the clinical expertise to implement the intervention under consideration or in the extended professional network of the clinic? Are there enough resources to implement the intervention under consideration in the clinic or extended professional network of the study center? Is the intervention under consideration covered by the public health insurance? Patients, relatives, friends: people affected by ALS living in Switzerland; interested in co-creating a CIM intervention through a design thinking process; preferably covering a variety of socio-economic background, age, gender, form of progression, disease status, and treatment Health professionals: neurologists specialized in ALS; ALS nurse experts; MBM therapists and psychologists, preferably with experience in digital health and ALS Public: Swiss ALS foundations and interest groups Science: ALS researchers; experts in implementation science; experts in participatory research “Focus on what remains”: salutogenetic MBM approach and the enhancement of patient resource efforts to strengthen resilience, self-efficacy and coping mechanisms. Maintain communication throughout the course of ALS with digital settings and technical solutions.
We additionally generated a stakeholder map to identify the key stakeholders of the project covering the domains, patients and relatives/friends, health professionals, public, and science20,25:
In a workshop with a MBM health professional, the research team further discussed the intersection between the current state of research from the literature and the feasibility of potential CIM interventions in the context of our clinic. The following focus topics for developing the CIM intervention were defined:
In a semi-structured qualitative interview, we talked to a couple (male, 54 / female, 54) on the ALS progression of their mother, and their mother-in-law respectively, who died about one year after the diagnosis. During the interview, our focus was on the progression of loss of abilities, and the feasibility of involving people with ALS and their relatives in research (see Table 3).
Summary of the empathize, observe and define design thinking phases relating to the context of the participatory process.

There were several informal phone calls and email exchanges between one researcher, and several representatives of Swiss ALS foundations and interest groups with different personal and professional backgrounds on the practical requirements needed to involve people with ALS with special needs in our stakeholder process (see Table 3).
In an exchange meeting with three neurologists specialized in ALS research and treatment of our hospital, we (the research team) discussed different topics that emerged from our previous research process (see Table 3). One topic addressed was how the neurologists maintain communication with people with ALS experiencing a decline in their speech abilities and the special tools they use to meet this (see Table 4). We further discussed their experiences with the most common ALS symptoms: dysphagia, aspiration, pneumonia, problems with respiration, musculoskeletal pain, sleep disorders, and distress. In addition, we exchanged research experiences with patient related outcome measures, such as quality of life, fatigue, or pain.
Summary of the empathize, observe and define design thinking phases relating to intervention development.

Y = Yes / N = No.
Table 3 summarizes the main findings, conclusions, and planned actions from all of the previous steps of the “empathize”, “observe” and “define” design thinking phases relating to the context of the participatory process.
In summary, as ALS is a time-critical disease, an especially careful resource and time planning of the stakeholder process is needed as well as individual participation solutions tailored to the needs and constraints of the participating people with ALS. In general, the stakeholders prefer online settings.
Table 4 summarizes the findings from all of the previous steps of the “empathize”, “observe” and “define” design thinking phases relating to the intervention development.
During our literature research phase, we started with a long list of CIM interventions that possibly met our implementation criteria. Through the continued research process, we adapted the list (see Table 4) and added “nutritional counseling” as an intervention as a result from the first stakeholder processes. We consequently included these interventions from Table 4 in the next design thinking phases. As there were not enough published clinical trials for any intervention to meet the criteria on the “clinical evidence needed”, we stepped back from the respective implementation criteria.
We sub-summarized the single interventions under four treatment modules:
Relaxation, breathing, mindfulness: Relaxation exercises; breathing exercises; meditations; mindfulness; self-hypnosis Positive psychology: Affirmations (positive suggestions); resource strengthening exercises; reflection exercises; exercises for coping with illness; self-compassion Sensory and somatosensory: Aromatherapy; (Aroma)massage; wraps and compresses; acupressure; moxibustion
Nutritional Counseling
We created the modules to be able to address types of interventions and ask for the stakeholders’ feasible priorities, avoiding an overburdening process for the people with ALS by not evaluating every single intervention.
Prototyping the MBM intervention with people with ALS – The ideate and prototype phases of the design thinking process
At the beginning of the ideate and prototype phases of the design thinking process, we conducted a workshop with an expert in Citizen Science and our process moderator to elaborate on a feasible workshop setting that meet the people with ALS’ needs and encourage their participation and collaboration while also addressing any of their constraints.
The workshop resulted in defining the key parameters of the workshop setting with the people with ALS:
The workshop will be held online according to the wish of the participating people with ALS that resulted from the previous design thinking phase. We aim to find out the expectations and preferences of the people with ALS towards which CIM interventions they would prefer for themselves, and which formats and settings they would prefer for the respective interventions. We additionally aim to find out which intervention formats and settings the people with ALS are already using. As the participating people with ALS have constraints regarding speech and use of the mouse and keyboard, we consider to elaborate on some questions via online questionnaire before the workshop. We consider conducting two workshops adapted to the needs of the participants, as half of the participating people with ALS have almost no constraints while the other half have constraints such as paralysis, limited speaking abilities, and in one case, a person near a locked-in state.
Prior to the workshop with the people with ALS, we conducted an explorative online survey with the workshop participants. We asked them about their previous experiences with digital health formats/solutions, and their priorities towards patient-related outcomes (such as anxiety, depression, fatigue, quality of life, sleep, pain, self-efficacy), and possible CIM interventions (please find the survey questions in the appendix).
In the beginning of the online people with ALS workshop, the results from the survey served as starting points for further discussions on the important topics relating to the creation of the CIM intervention.
We prepared oral and written options for participating in the workshops to enable paralyzed and speech-impaired people to engage as much as possible. Paralyzed participants that were able to speak could participate orally as we - the workshop organizers - jotted their thoughts on sticky papers in the shared Miro board. Participants that were unable to speak and paralyzed people with high-tech augmentative and alternative communication technologies could participate by writing down their answers either to the chat or in the Miro board. To make it feasible, we prepared questions that either could be answered with “yes” or “no” – people could nod or write a “y” for “yes” or a “n” for no – or they could choose from numbered answer options by writing down the number of the option they preferred.
The questions that guided the exchange in the workshop were:
Interventions: Which intervention module should be prioritized? Do you prefer a free choice of different modules or a guided process through all the modules? Setting: Do you prefer online or onsite settings? If online, do you prefer an e-learning or a guided process with a therapist? If onsite, what should be the characteristics? Do you prefer individual or group settings? Time: What are the ideal time intervals between single interventions? Exchange: With whom and when do you want an exchange? Should exchanges be moderated in general? When do you need a CIM therapist/medical doctor?
The participants’ priorities relating to these questions are summarized in Table 5.
Topics of the workshops and stakeholders’ priorities.
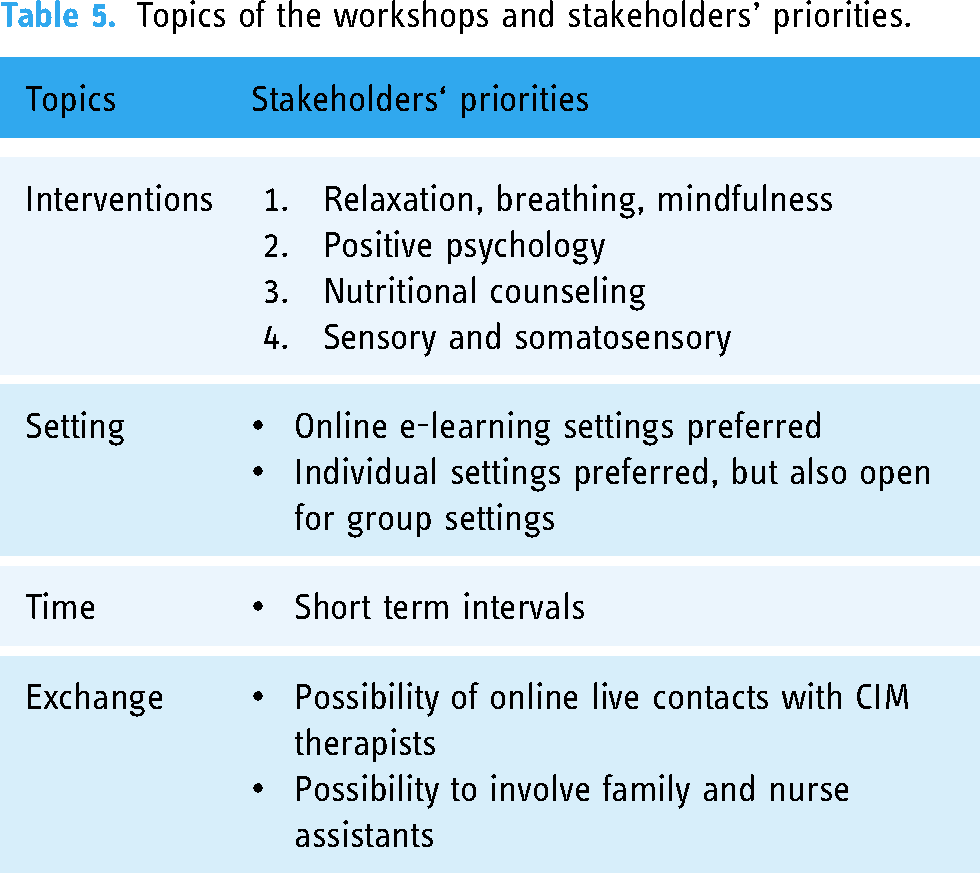
An important finding is the high degree of diversity in terms of both the disease status and progression, and the subsequent accessibility needs of the participants to be able to participate in the intervention. Therefore, it is important to offer therapy options that can be tailored to the needs and constraints of the individual patients. Online settings in short-term intervals with the possibility for live online contact with CIM therapists and the inclusion of family and nurse assistants were clearly preferred by the participants. Taking this preference into account, together with the priority for relaxation, breathing, and mindfulness interventions, we proceeded with a MBM pilot therapy option into the next design thinking phase.
Testing the MBM intervention in the clinical setting – The implement and test phases of the design thinking process
Based on the findings from the previous design thinking processes, the seven workshop participants were offered a free pilot MBM intervention at the Institute of Complementary and Integrative Medicine of the University Hospital Zurich.
During a one-hour individual online consultation with an MBM therapist of the institute, the people with ALS could choose either a breathing exercise or a mindfulness exercise to try under the guidance of the present MBM therapist. The participants could choose from: (1) Breathing exercise, (2) Mindfulness meditation, (3) Body scan, (4) Fantasy journey. 40 If the time allowed it, the participants could try more than one exercise, as it was the case with one person.
At the beginning of the consultation, there was space to discuss the individual focus of each patient considering the present symptoms and needs. At the end of the consultation, the people with ALS gave feedback about their experience. The MBM therapist shared her experiences and assessment of the pilot consultations in a feedback form as well as in a final qualitative interview with a researcher from the project team. The feedback form included three pre-defined semi-structured questions about their experience with the selected intervention, whether they planned to repeat the selected exercise independently, and whether they would recommend the selected exercise to other people with ALS. At the end, they were also asked for additional open-ended feedback.
Four of seven workshop participants accepted the offer. The consultations were conducted in March 2022. Two people with ALS selected a breathing exercise and two selected a "Body Scan". One patient opted for a coaching about the topic of self-efficacy.
The online setting was positively evaluated by the people with ALS and they were equally interested in breathing and mindfulness exercises. Find hereinafter an illustrative example of a patients’ feedback: «It was interesting and exciting to feel the breathing and to turn the focus inward. I consider the interaction of body and mind as important anyway. Connecting it with breathing certainly makes the exercise valuable for people with ALS as a mean of stress reduction». (English translation of an original feedback in German of participant nr.3)
One patient additionally asked for a recommendation for his wife, as he perceived her to be burdened and stressed. All four participants expressed the intention to repeat the exercises at home and would recommend them to other people with ALS.
In the interview, the MBM therapist emphasized that an individually adaptable approach seems important for a future intervention, as the personality, course of the disease and the main symptoms would differ among those affected. This is in line with the findings from the stakeholder process. In addition, the MBM therapist felt that personal contact between patients and those affected was important, as many people with ALS appear to be under psychological strain; but also because most people with ALS are severely restricted in their mobility and therefore spend a lot of time alone at home. Another aspect mentioned by the MBM therapist was that practicing mindfulness could also trigger a nocebo effect because it makes people aware of their own situation and the associated emotions. Having direct contact with a therapist could be a helpful way to deal with one's own situation.
Discussion
Summary of the findings
Due to the unpredictable course of the disease on their loss of abilities, people with ALS prefer short-term treatment intervals and online settings for CIM interventions because they are more accessible and easier to implement in their daily life than onsite consultations in a clinic. Stakeholders considered the following implementation factors for a digital CIM intervention as essential: short-term realization of the planned interventions, short duration of interventions, and user-friendliness in terms of accessibility and applicability. Both individual and group settings are feasible for people with ALS, but considering the physical and cognitive abilities of people with ALS, small group size should be preferred. Concerning the CIM interventions, the people with ALS preferred MBM interventions, such as breathing, mindfulness and relaxation exercises.
Digital intervention solutions for people with ALS
Digital interventions support people with ALS in terms of accessibility, flexibility and applicability relating to the different stages of the disease.12,19,41 In addition, there are evolving technical solutions for different impairments, such as high-tech augmentative and alternative communication technologies.17,42 Furthermore, remote settings showed to be supportive of involving family members and assistant nurses in both ALS care and participatory research.12,19,41
As a consequence of the COVID-19 pandemic, digital literacy, digital infrastructure, and reimbursement possibilities potentially have turned from implementation barriers before the pandemic18,22 to facilitators of implementing digital health services for the patients after the pandemic, although the societal challenges, such as the “digital divide”, are still unresolved.19,43–45 Future research is needed to confirm this hypothesis.43–45 Challenges that remain are reduced personal contacts with health professionals and the exclusion of manual CIM interventions in digital settings.
Strengths and limitations of the study
The strength of our study is the application of an innovative design thinking approach and the inclusion of stakeholders and people with ALS in all progression stages, from nearly no restrictions to a near locked in state. We intentionally fostered participation by including a citizen science expert and an external process moderator to address the common stakeholder engagement challenges of accessibility, participation, power imbalances, shared language, and conflicting interests.22,26,28 We applied different means of communication – phone, email, online surveys, informal meetings, and workshops – to support participation throughout the whole research process. As ALS is an especially time critical disease, we applied an innovative design thinking approach to create a pilot CIM intervention in a short amount of time with the stakeholders.
We also faced some challenges and limitations in our study. To enable communication and foster participation of people from all progression stages, time resources for such a personalized approach were extensive and human resources were therefore rather expensive compared to other studies we have done including people with fewer limitations. In addition, conducting an open and creative process as stakeholder engagement processes are in their nature, was partly limited due to the application of closed questions and predefined answer options to include people of every progression stage.
We limited the prototyping of a pilot CIM intervention to what we could offer and realize within our clinic. In the context of the COVID-19 pandemic, the fear of infection and enhanced digital literacy and infrastructure could be a bias concerning the stakeholders’ preference for online settings. Although, research from before the pandemic already pointed to this patients’ preference. 18
Implications for future research
The next step for our study could be the evaluation of the effectiveness of the CIM pilot intervention in a randomized controlled clinical trial, considering blended digital solutions, such as eLearnings and in-person consultations according to the stakeholders’ preferences of the study. 41 Future research should further focus on finding the best match between digital infrastructure solutions and accessibility requirements of people with ALS.15,16 Thereby, patient information about the accessibility and availability of technology must be taken into consideration.
Conclusion
Short-term treatment intervals and short online mind body medicine interventions align with the needs of people with ALS. The CIM intervention as well as the digital infrastructure must meet the special accessibility and applicability needs of people with ALS, preferably during the entire course of the disease and in every progression state. Future research should test blended digital mind body medicine interventions.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241255928 - Supplemental material for Developing a digital mind body medicine supportive care intervention for people with amyotrophic lateral sclerosis using stakeholder engagement and design thinking
Supplemental material, sj-docx-1-dhj-10.1177_20552076241255928 for Developing a digital mind body medicine supportive care intervention for people with amyotrophic lateral sclerosis using stakeholder engagement and design thinking by Claudia Canella, Carina Braun and Claudia M. Witt in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241255928 - Supplemental material for Developing a digital mind body medicine supportive care intervention for people with amyotrophic lateral sclerosis using stakeholder engagement and design thinking
Supplemental material, sj-docx-2-dhj-10.1177_20552076241255928 for Developing a digital mind body medicine supportive care intervention for people with amyotrophic lateral sclerosis using stakeholder engagement and design thinking by Claudia Canella, Carina Braun and Claudia M. Witt in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgments
We sincerely thank all of the stakeholders for their engagement in the project, as well as Lukas Stadelmann of rethink GmbH for moderating us throughout the entire process.
Author contributions
Claudia Canella, Carina Braun, and Claudia M. Witt were equally involved throughout the entire research project, from designing the research, to data collection and analyses, and science communication. Claudia Canella wrote the first draft of the manuscript and revised the following versions. Carina Braun and Claudia Witt critically commented on the manuscript. All of the authors contributed to the interpretation of the results, the shaping of the manuscript and approved the final version of the manuscript.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
We submitted the study synopsis to the Ethics Committee of Zurich, Switzerland, and after review, they stated that the study does not fall under the regulation of the Human Research Act of Switzerland (BASEC-Nr. Req-2021-00673). We obtained written informed consent from people with ALS and documented oral consent from all other stakeholders for participation and scientific publication. All data was anonymized.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded by the Renate Rugieri Foundation via USZ Foundation.
Guarantor
Claudia M. Witt.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.