
Abstract
Objective
This study aimed to investigate the similarities and differences in risk factors for suicide among adult and adolescent women in South Korea and identify subtypes of suicidal ideation or suicide attempt in each group.
Methods
Multifaceted data were collected and analyzed by linking survey and social media data. Interpretable machine learning models were constructed to predict suicide risk and major risk factors were extracted by investigating their feature importance. Additionally, subtypes of suicidal adult and adolescent women were identified and explained using risk factors.
Results
The risk factors for adult women were primarily related to mental disorders, while those for adolescent women were primarily related to interpersonal experiences and needs. Two subtypes of suicidal adult women were one with high psychiatric symptoms and mental disorders of them and/or their families and the other with excessive social media use and high online victimization. Two subtypes of suicidal adolescent women were one with high psychiatric symptoms, high ACEs, and high social connectedness, and the other with frequent social media use, high online sexual victimization, and high social assurance.
Conclusions
These findings enable a stratified and targeted understanding of suicide in women and help develop customized suicide prevention plans in South Korea.
Introduction
Background
Suicide is a significant health problem among women. Although global mortality by suicide is three times higher in men than in women, the suicide attempt rate is three times higher in women than in men. 1 Additionally, women are more likely to have suicidal ideation than men 2 and are more vulnerable to mental disorders such as depression which can result in suicide. 3 This health issue is important to both adult and adolescent women. In South Korea, which has the highest suicide rate among the Organization for Economic Co-operation and Development (OECD) countries, 4 adult women thought about suicide twice as much as adult men and adolescent women attempted suicide twice as often as adolescent men. 5 According to Statistics Korea,6,7 suicide is the leading cause of death among women aged from 10 to 40, and regarding the suicidal ideation, the prevalence was 16.1% among adolescent women, which is about twice the rate of adolescent men (9.5%). Thus, it is necessary to take dedicated governmental action to prevent suicide in women based on a broad and in-depth understanding of various factors related to suicide in South Korean women.
A comprehensive understanding of various risk factors associated with suicide is essential to prevent or reduce suicide.8–10 This is because suicide is a heterogeneous phenomenon interacting with many factors related to psychiatry, 11 sociodemographics, 12 society, 13 and social media use. 14 Previous studies on suicide in women have reported major risk factors such as older age, 12 depression, 13 family conflicts, 13 and low social support. 15 These factors differ between adults and adolescents because the circumstances and conditions facing adults and adolescents are different (e.g. unemployment vs school problems). 16 For example, Kawashima 16 studied suicide attempters in Japan and found that risk factors for adolescent women suicide attempters were school problems and parent loss while those for their adult counterparts were a history of mental disorders. Similarly, Kolves and De Leo 17 studied suicides in Australia and reported that suicides in adolescents were highly impacted by family conflicts and school problems while those in adults were highly impacted by psychiatric disorders such as unipolar depression, bipolar disorder, and anxiety disorder. In addition to their findings on high-level differences between adult and adolescent suicides, considering social media use to explain the difference between the groups is highly important. With the increasing popularity of social media, excessive use of social media, various forms of online victimization on social media (e.g. cyberbullying and sexual harassment), expression of negative moods on social media, and talking about suicide on social media are increasingly being considered as risk factors for suicide.18–20 Therefore, we need to broaden our understaning on suicide risk by exploring more fine-grained differences using various factors including social media use.
As suicide can be triggered by many different factors and traits, prevention strategies should be customized by considering suicide subtypes. 21 Researchers have attempted to investigate suicide subtypes by focusing on differences among subtypes in factors related to demographics, psychosocial aspects, and behavioral characteristics. Pfeffer 21 identified two subtypes with or without assaultive behavior among adolescent psychiatric inpatients in the US Cross and colleagues 22 studied adolescents in the United States with a history of at least one suicide attempt and found six subtypes: internalizing, externalizing, emotional dysregulation, high functioning, narcissistic, and immature. Schaffer and colleagues 23 studied Canadian suicide attempters with bipolar disorder and identified five subtypes with differences in factors such as substance abuse, history of suicide attempts, living circumstances, financial stressors, legal stressors, and interpersonal stressors. Most studies focused on suicide attempters without distinction in genders and age groups by only considering high-level factors such as employment, mental disorders, and demographics as criteria for subtyping. Furthermore, social media data have become a valuable source of understanding suicidal behavior as Gunn 24 illustrated that people freely express their thoughts and emotions on social media posts due to its anonymity.
Therefore, to have a better understanding of subtypes of women thinking and/or attempting suicide, we should consider fine-grained data collected from both survey and social media while making a clear distinction between adults and adolescents.
Objectives
This study aimed to compare risk factors for suicide between adult and adolescent women in South Korea and identify subtypes of suicidal ideation or attempt in each group. To the best of our knowledge, no study has been conducted with a similar objective, even though there has been a rise in the occurrence of suicidal ideation and suicide attempt among this population. To achieve this goal, multifaceted data were analyzed by linking survey and social media data to investigate suicide in women from various perspectives. Therefore, this study targets women who actively use social media. Survey data included 270 questions classified into 7 categories: demographics, objective psychiatric symptoms and self-reported mental disorders, internet use, online/offline social networks, social media use, interpersonal experiences and needs, and subjective wellbeing. Social media data included five variables including the number of posts and the mean sentiment score about posts. Using these data, interpretable machine learning models were built to predict suicidal ideation or suicide attempt as well as identify and compare major risk factors for suicide in the two groups. Additionally, cluster analyses were conducted using the features which were had been identified as important in predicting adult and adolescent suicide, to identify the subtypes of suicidal adult and adolescent women as well as consider their unique characteristics. The following research questions were developed, and we emphasize that the targets of our study are women who use social media. RQ1: What are the similarities and differences in risk factors for suicide between adult and adolescent women in South Korea? RQ2: What are the subtypes of suicidal adult women in South Korea? RQ3: What are the subtypes of suicidal adolescent women in South Korea?
Methods
The study consisted of three parts: data collection and preprocessing, comparing major risk factors for suicide between adult and adolescent women, and understanding subtypes of suicidal ideation or suicide attempt in adult and adolescent women. The overall process is shown in Figure 1 and each of the steps is discussed in detail in the following sections.

The process of data collection, preprocessing, and analysis.
Participants and procedures
The study protocol was approved by the Institutional Review Board (IRB) at Sungkyunkwan University in South Korea. The study participants were adolescent women aged 13 to 18 years and adult women aged 20 to 39 years who had been using Twitter or Instagram and posted at least 10 times within the past year. In data collection, we did not consider any constraints except for gender (i.e. only woman), age (13–40) and whether participants’ social media use. In South Korea, the criteria of distinguishing between adults and adolescents have recently been changed from calendar year to birthday basis and this led to situations where individuals aged 19 are sometimes classified as adults or adolescents depending on different criteria. After consulting with the online survey company that collected the data for this study, we have chosen to exclude individuals aged 19 in our study. We will discuss this in Limitations section. We collected survey and social media data from June 2020 to July 2020 for 500 adolescent women and from September 2020 to October 2020 for 500 adult women in South Korea through an online research company, Macromill Embrain. The company contacted randomly selected people in the panel to participate in our survey. If they agreed to participate in the study, they were required to read and agree to a consent statement. Throughout the data collection period, the company distributed surveys daily and provided us with the collected data every day until reaching a total of 1000 respondents. While participants were responding to the survey questionnaires, with their consent, we requested them to log into their Twitter or Instagram accounts and crawled their posts created in the past year. All personal information were modified into nonidentifiable formats. Among 1000 participants, 25 participants (20 adults and 5 adolescents) were removed because they had posted fewer than 10 posts in the past year. The final data included 480 adults and 495 adolescents. Their demographic information is available in Appendix 1. Of the 975 participants, 221 (96 adults and 125 adolescents) reported having suicidal ideation and/or suicide attempt within the past 2 weeks.
Measures
The survey questionnaires included 270 questions related to 7 higher-order constructs and 14 lower-order constructs as shown in Table 1. A detailed description of the variables is available in Appendix 2.
Description of survey data categories.

PTSD: posttraumatic stress disorder.
The survey data were linked to social media data with variables shown in Table 2.
Description of social media variables.

To calculate mean positive and mean negative sentiment scores of posts for each participant, we firstly calculated a sentiment score for each post using the Python library KnuSentiLex. 25 It was trained using the bidirectional long short-term memory (Bi-LSTM) on a lexicon of over 300,000 sentiment words. It tokenizes a post and calculates each token's sentiment score which ranges from −2 (very negative) to +2 (very positive) and reports the sum of each token's score as the final score of the post. Given a participant's all posts, after calculating each post's sentiment score, we classified them into positive or negative sentiment groups. We calculated mean scores of the posts in each of the two groups and obtained each participant's positive and negative sentiment scores.
Statistical analyses
Interpretable machine learning
To identify and compare major risk factors for suicide between adult and adolescent women, we used eXtreme Gradient Boosting (XGBoost), 26 which is a gradient boosting method with regularization and has been used by many studies27,28 to build high-performance prediction models for tabular data. Before training our models, we oversampled our data using the Synthetic Minority Oversampling Techniques (SMOTE) function from a Python library Imblearn 29 to tackle the unbalanced sample problem. To optimize performance, models were trained several times through an iterative process of feature selection using a scikit-learn library SelectFromModel 30 in a stratified 10-fold cross-validation setting. After building final models with the best performance, we visualized top risk factors and their impacts on predicting suicide using the SHAP summary plot. 31
Cluster analysis
To understand subtypes of suicidal ideation or suicide attempt in adult and adolescent women, we used the Gaussian Mixture Model (GMM), 30 which is a probabilistic model that assumes data were generated from the finite mixture distributions. 32 To achieve interpretable results, we only considered important features obtained through a feature selection processes during building machine learning models. By doing so, we aimed to deliver more distinguishable and easy-to-interpret cluster results. To identify the optimal number of clusters, we built cluster models with the number of clusters ranging from two to ten and calculated the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), entropy, and Bootstrap Likelihood Ratio Test (BLRT) scores for each model. Models with lower AIC and BIC scores, higher entropy scores, and significant p values in BLRT are considered as better fitting models.33,34 We then consulted two psychiatrists for selecting the optimal number of clusters. In this study, the psychiatrists were not asked to label individual participant because there are more than 60 features to consider when labeling and this is a laborious task which may result in incorrect results. Instead, we showed them nine candidates with the number of clusters ranges from 2 to 10 and asked them to select the number of clusters (2, 3, etc.) that best shows each cluster's distinct characteristics. The nine candidates were generated by using GMM. For example, if they think each of three clusters in the candidate with three clusters has distinct characteristics, they may choose three as the optimal number of clusters. This manual evaluation may favor smaller number of clusters due to interpretability and therefore we also considered four metrics of automated methods.
Study design and procedures
Comparing major risk factors for suicide between adult and adolescent women
First, respective interpretable machine learning models were trained to predict suicide risk for adult and adolescent women. In addition to make predictions, interpretable machine learning models describe reasoning processes of making predictions and explain relative importance of features used in predictions. 35 Second, with the predictive models, major factors were identified by exploring feature importance which indicates a feature's relative contribution to predicting suicide risk. Specifically, factors were identified that increase the probability of having suicidal ideation or attempting suicide (i.e. risk factors). Third, the two sets of major risk factors (one for each group) were compared to understand similarities and differences.
Understanding subtypes of suicidal ideation or suicide attempt in adult and adolescent women
Subtypes of suicidal ideation or suicide attempt were identified through cluster analyses. A cluster analysis detects homogeneous subgroups in a sample according to a measure of similarities among data points in the sample. 36 In this study, similarities among individuals in a group (either suicidal adult or adolescent women) were computed from the variables used in predictive models. After identifying subtypes, a two-tailed Student's t-test was used to explain the unique characteristics of each subtype.
Results
Predictive models of suicide ideation or attempt
After the feature selection process, 65 features for the adult women's model and 51 features for the adolescent women's model were extracted. The performance of the best-performing models is shown in Table 3.
Performance of the two predictive models.

The results of the models showed an F1-score of 0.92 and AUC of 0.92 in the adults’ model and an F1-score of 0.89 and AUC of 0.89 in the adolescents’ model.
Comparing major risk factors for suicide between adult and adolescent women
Figure 2(a) and (b) show the 10 major risk factors of models for adult women and adolescent women, ranked by their relative importance. Figure 2(c) shows the comparison between the two groups’ major risk factors. In Figure 2(a) and (b), given a feature, each dot denotes an individual case, and its horizontal position shows the individual's SHAP value which indicates its impact on the predictive model's output. A value of zero denotes no impact on suicide prediction, a positive SHAP value indicates its positive impact on increasing the probability of having suicidal ideation or attempt, and a negative SHAP value indicates the opposite. For instance, if someone has a positive SHAP value in adverse childhood experiences (ACEs) indicating abuse or other potentially damaging childhood experiences, 37 her ACEs then has an impact on increasing the probability of her having suicidal ideation or suicide attempt. The dot color represents feature values, with blue color representing low values and red color representing high values. Therefore, if most of a feature's red dots (i.e. high values) are associated with SHAP values higher than zero, this feature is considered a risk factor for suicide.
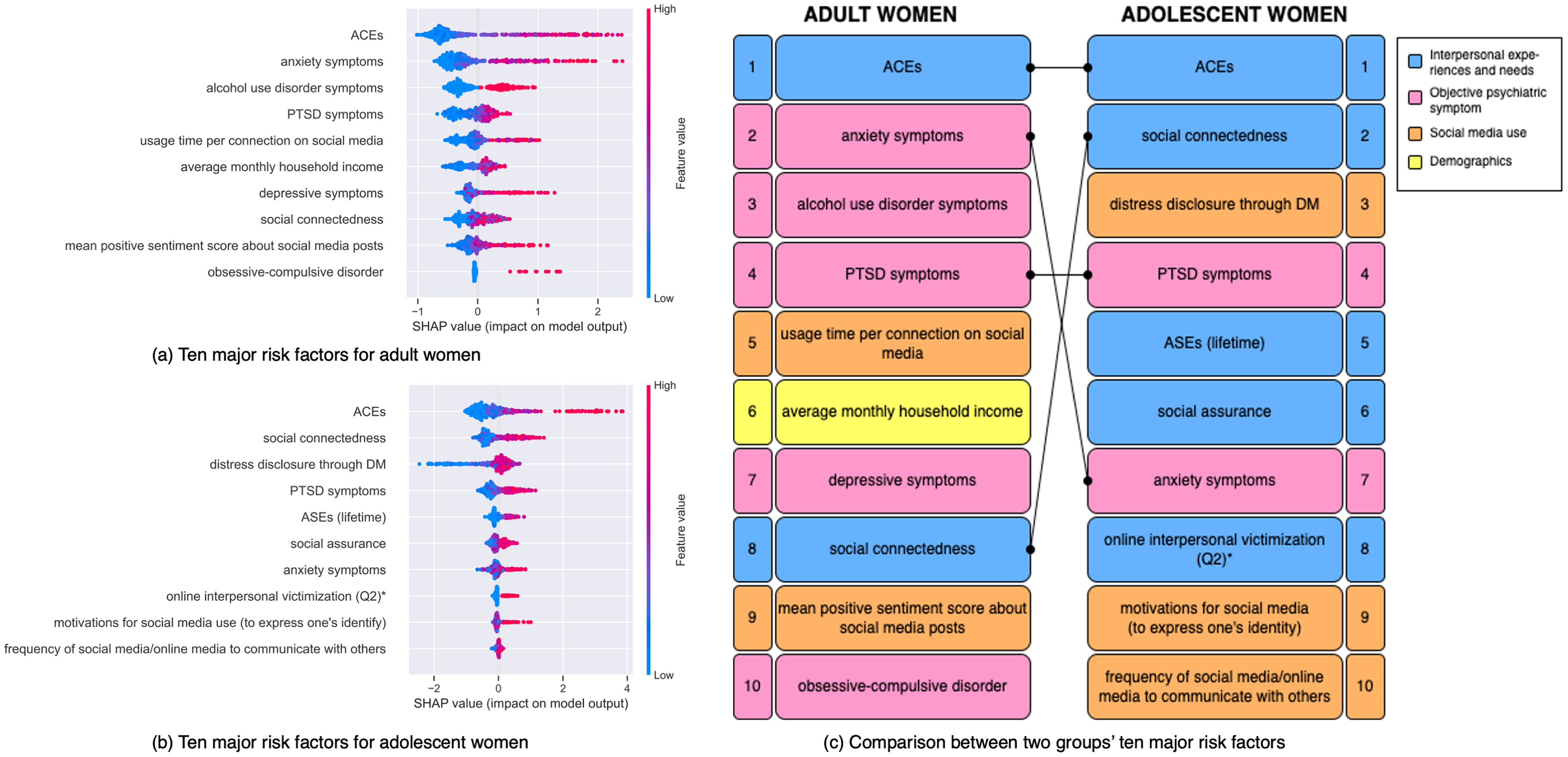
Major risk factors for suicide in adult and adolescent women. Online interpersonal victimization (Q2)* denotes the experience of having been asked about very private and sexual information online despite being unwilling.
Five findings are highlighted as follows. First, as shown in Figure 2(a) and (c), half of the 10 major risk factors for adult women were related to mental health (i.e. anxiety symptoms, 38 alcohol use disorder symptoms, 39 posttraumatic stress disorder (PTSD) symptoms, 40 depressive symptoms, 38 and obsessive-compulsive disorder). Second, compared to adult women, as shown in Figure 2(b) and (c), half of the 10 major risk factors for adolescent women were related to interpersonal experiences and needs. The most important factor was ACEs, followed by social connectedness indicating an emotional distance between self and others, 41 ASEs in lifetime indicating sexual abuse including being touched without consent, 42 social assurance indicating the tendency to rely on others to feel a sense of belonging, 43 and online interpersonal victimization (Q2) indicating experience of having been asked about very private and sexual information online despite being unwilling. 44 Third, as shown in Figure 2(c), the most important factor in both groups was ACEs and the fourth was PTSD symptoms. Fourth, although both anxiety symptoms and social connectedness were identified as major risk factors for adult and adolescent women, these factors had different importance within the two groups. Anxiety symptoms ranked second in adults and seventh in adolescents. Social connectedness ranked second in adolescents and eighth in adults. Fifth, there were different risk factors related to social media use among adult and adolescent women. Adult women had two factors related to social media use (i.e. usage time per connection on social media and mean positive sentiment score about social media posts). These were ranked as the fifth and ninth risk factors. Adolescent women had three additional factors including distress disclosure through direct message (DM), 45 motivations for social media (to express one's identity), 46 and frequency of social media/online media to communicate with others. These were ranked as the third, ninth, and tenth risk factors.
Understanding subtypes of suicidal ideation or suicide attempt
Subtypes of suicidal adult (n = 96) and adolescent women (n = 125) were identified separately using cluster analyses.
Subtypes of suicidal adult women
After generating models with different number of clusters, we found that the model with two clusters had the lowest BIC and the highest entropy (Table 4) and excelled in two out of the four metrics. In addition to the results of the automated methods, we asked two psychiatrists to review the nine candidates with different number of clusters. They agreed that two is the optimal number of clusters which shows interpretable and distinguishable results. Synthesizing the results of the automated methods and psychiatrists’ domain expertise, we selected two as the optimal number of clusters.
Results of four evaluation metrics for models with different number of clusters (suicidal adult women).

AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; BLRT: Bootstrap Likelihood Ratio Test.
Table 5 shows each subtype's representative factors and their values. Significant differences were observed in four of the seven high-level categories.
Characteristics of subtypes in suicidal adult women.

As the results suggest, subtype 1 was characterized by severe psychiatric symptoms and mental disorders. They had more problems with both their own mental health and family histories of mental disorders, and family history of mental disorders has been shown to significantly increase an individual's own suicide risk.47,48 Subtype 2 tended to spend more time on social media than subtype 1. Specifically, subtype 2 spent more than 50 min per connection on social media whereas subtype 1 spent less than 30 min. Additionally, among the various motivations for using social media, the degree of using social media to escape from school or work was significantly higher in subtype 2. They also experienced a significantly higher level of having been threatened or embarrassed by posting or sending messages about you for others to see than subtype 1.
Subtypes of suicidal adolescent women
After generating models with different number of clusters, we found that the model with two clusters had the lowest BIC, the highest entropy, and a significant p value in BLRT (Table 6) and excelled in three out of the four metrics. Again, two psychiatrists reviewed the results and agreed that two was the optimal number of clusters. Therefore, we selected two as the number of clusters for suicide in suicidal adolescent women.
Results of four evaluation metrics for models with different number of clusters (suicidal adolescent women).

AIC: Akaike Information Criterion; BIC: Bayesian Information Criterion; BLRT: Bootstrap Likelihood Ratio Test.
Table 7 shows the two subtypes’ characteristics, including the differences among five categories within the subtypes.
Characteristics of subtypes in suicidal adolescent women.

PTSD: posttraumatic stress disorder.
Subtype 1 had severe psychiatric symptoms and high general problematic internet use (GPIU) which indicates problematic use of the internet that can cause psychological or social difficulties. 49 They used social media habitually to spend time without specific purposes. They had issues related to interpersonal experiences and needs such as ACEs. They felt a great sense of emotional distance from others (i.e. high social connectedness), which may increase their suicide risk. Different from the results in adult women where the two subtypes were characterized by having either mental disorders or interpersonal problems, adolescent women in subtype 1 had both problems. While people in subtype 1 used social media without specific purposes, subtype 2 used social media for managing social relationships, including maintaining relationships with friends and/or organizing gatherings. They also had more negative online sexual experiences than subtype 1. It is noteworthy that subtype 2 had different interpersonal needs than subtype 1. Subtype 1 had high social connectedness whereas subtype 2 had high social assurance.
Figure 3 visualizes the identified subtypes in three-dimensional spaces using principal component analysis (PCA) 50 and summarizes the characteristics. As shown in the figure, the suicidal adult and adolescent women were noticeably divided into two separate distinct subtypes.

Summarization of subtypes of suicidal adult and adolescent women.
Discussion
In contrast to prior research that examined a limited range of potential factors related to suicide risk in women of all age groups in Western countries, this study analyzed risk factors specifically for adult and adolescent women in South Korea. It further explored the similarities and differences between the two groups using multifaceted data organized into 7 higher-order and 14 lower-order constructs. In addition, previous studies on suicide subtypes did not investigate women and primarily used general factors such as mental disorders to explain the subtypes.21,22,51 To fill this gap, the subtypes of suicidal adult and adolescent women were examined separately using a comprehensive set of factors. In the following, we provide a detailed discussion of our research questions. RQ1: What are the similarities and differences in risk factors for suicide between adult and adolescent women in South Korea?
To answer RQ1, we initially built interpretable machine learning models to predict suicide risk for adult and adolescent women separately. We then identified major risk factors using the concept of feature importance which indicates a feature's relative contribution to predicting suicide risk. Finally, we compared the identified major risk factors for adult women with those for adolescent women to explore similarities and differences. In common, ACEs were the most important risk factor for suicidal ideation and attempt in both adult and adolescent women. These results illustrate that adverse experiences women undergo during childhood may have long-term effects even after they grow up and their impacts are so severe that they may cause the person to think about or attempt suicide.52,53 Although both groups had ACEs as the most important factor, the extent to which they contributed to suicide risk was different. The highest SHAP value in adult women was approximately 2.5 but in adolescent women, it was 4. Thus, the negative impact of ACEs on adolescents may be much higher given that they experienced it relatively recently and are less capable of handling negative events.54,55 Government officials should consider ACEs a major risk factor for suicide in women and develop relevant prevention strategies. Although anxiety symptoms and social connectedness were identified as major risk factors for both adult and adolescent women, their importance differed. Anxiety symptoms were more important to adult women while social connectedness was more important to adolescent women. Studies reported that for adolescents who undergo social and physical changes, relationships with peers or parents are an important issue that is significantly related to emotional problems (e.g. loneliness or social isolation.)
56
Thus, social connectedness may have a greater impact on suicidal ideation or suicide attempt among adolescent women. Based on this result, we can infer that adolescent women are more vulnerable to social and interpersonal problems than adult women. Different high-risk social media use behaviors were also identified between the two groups. Excessive social media use was an important factor for suicide in adult women, whereas the use of social media to communicate with others was an important risk factor in adolescent women. Previous studies explained that excessive use of social media may cause chronic sleep loss and low satisfaction with life, which have a negative influence on mental health.57,58 For adolescents, Koutamanis
59
illustrated that adolescents who engaged in social media to communicate with others were more likely to receive negative feedback, which could lead to unhealthy mental status. Particularly, previous studies explained that engaging in risky online behaviors, such as self-promotion
60
and posting narcissistic content
61
during communication on social media, may result in receiving negative feedback. Therefore, adolescent women may need to be aware of potential negative consequences when interacting with others on social media. RQ2: What are the subtypes of suicidal adult women in South Korea?
To answer RQ2, we performed cluster analyses to identify subtypes among suicidal adult women and summarized their characteristics. During cluster analyses, we utilized 65 important factors obtained from the best-performing prediction model we had built when addressing RQ1. Results of a cluster analysis using all the features may less distinguishable, hard to interpret and provide condensed information because relative importance of features are not considered, and every feature is treated as equal. To avoid this, we performed cluster analyses in answering RQ2 and RQ3 by utilizing the results of RQ1, therefore RQ1 is a necessary step toward RQ2 and RQ3. As a result, we identified two subtypes among suicidal adult women. The first subtype was characterized by severe psychiatric symptoms and mental disorders among them and/or their families. The second subtype used social media excessively and suffered from online victimization. Thus, in addition to national efforts to promote mental health, a safe online and social media environment may be important. Protection against exposure to online victimization may be extremely important to successful suicide prevention. RQ3: What are the subtypes of suicidal adolescent women in South Korea?
To answer RQ3, we performed cluster analyses to identify subtypes among suicidal adolescent women. Again, we utilized 51 important factors obtained from the best-performing prediction model we had built when addressing RQ1. As a result, we identified two subtypes of suicidal adolescent women. The first subtype had severe psychiatric symptoms, more adverse experiences in childhood, and a large emotional distance from others. The second subtype used social media frequently, had more experiences of online sexual victimization, and was highly dependent on others. Mitchell et al. 62 reported that adolescents who were asked to engage in unwanted sexual talk online, including requests for offline contact, had high levels of distress after the incidences. Furthermore, previous studies reported that people who was highly dependent on others may use social media to fill the deficiencies in face-to-face interaction with others, and it may reduce social participation in real life and lead to unhealthy mental status.63,64 Thus, adolescents in subtype 2 may have felt a lack of social relationships in real life and used social media to solve this problem. Instead, they may have suffered more from negative sexual incidents and eventually thought about or attempted suicide. Therefore, promoting face-to-face interactions with parents and peers, developing offline social skills, and reducing adolescents’ desire to rely on media 65 may be good suicide prevention strategies.
Limitations
This study has a few limitations. First, although this study identified major risk factors using a wide range of potential factors, it did not consider physical disorders (e.g. neoplasm) or pregnancy66–68 which have been considered important factors associated with suicide in women. Thus, further research needs to include these factors for a more detailed understanding of suicide in women. Second, owing to limitations involved in data collection, this study only considered women aged between 13 and 39 years. The World Health Organization 69 reported that although the suicide rate is highest among women in this age range, it is also high among those older than 40. Third, we utilized simple metrics such as the number of posts or sentiment score derived from social media data for predicting suicide. In future studies, it would be beneficial to analyze the social media content such as linguistic patterns of suicidal users or main themes in their posts. Fourth, as the study participants were individuals who had used social media, the results may be different from those who had not used social media. Among the top risk factors for suicide in adult and adolescent women, five factors were related to social media. Therefore, the study results may have limited generalizability to individuals who do not use social media. Fifth, this study distinguished adults from adolescents based on the age of 19. That is, women over 19 were classified as adults, while those under 19 were categorized as adolescents. In addition to this criterion, some studies have examined individuals aged 18 to 25 as a distinct group (i.e. transition-aged youth or young adults) based on the assumption that they have common characteristics. Our future study will take this perspective into account when categorizing groups and understanding differences. Finally, this study used a self-reported questionnaire to identify participants’ gender and our data may include women whose self-reported gender identity is different form their biological sex. Because the study participants were randomly selected by a renowned survey company with rich experience, we believe that the proportion of gender minority in our sample may not largely different from the proportion in South Korea population. Therefore, it is difficult to attribute the high suicide rate in this study to the influence of gender minority population, but we see the limited assessment of different gender identities is a limitation.
Conclusions
In this study, by using multifaceted and linked data from surveys and social media, along with interpretable machine learning approaches, we investigated (1) major risk factors for suicide among South Korean adult women; (2) major risk factors for suicide among South Korean adolescent women; (3) similarities and differences in risk factors between adult and adolescent women; (4) subtypes of the subtypes of suicidal adult women in South Korea; and (5) subtypes of suicidal adolescent women in South Korea.
We summarize our contributions as follows. First, whereas previous studies primarily used a single type of data, we used multifaceted data by linking surveys and social media. Therefore, we investigated suicide risk among South Korean adult and adolescent women from various perspectives. Second, our study identified major risk factors for suicide separately for adult and adolescent women and compared the results enabling a stratified and targeted understanding. Third, we identified and explained subtypes in suicidal adult and adolescent women separately and further segmentalized the subjects of study. All of these mentioned contributions are further related to developing customized suicide prevention plans and programs.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241255660 - Supplemental material for Understanding and comparing risk factors and subtypes in South Korean adult and adolescent women's suicidal ideation or suicide attempt using survey and social media data
Supplemental material, sj-docx-1-dhj-10.1177_20552076241255660 for Understanding and comparing risk factors and subtypes in South Korean adult and adolescent women's suicidal ideation or suicide attempt using survey and social media data by Donghun Kim, Ting Jiang, Ji Hyun Baek, Sou Hyun Jang and Yongjun Zhu in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Mihye Seo, Kihyun Kim, and Jae-Won Kim.
Contributorship
DK contributed to data curation, formal analysis, investigation, visualization, and writing—original draft; TJ to data curation, resources, and writing—review & editing; JB to validation and writing—review & editing; SJ to validation and writing—review & editing); and YZ to conceptualization, methodology, project administration, supervision, and writing—review & editing.
Declaration of conflicting interests
Our study was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Ethical approval
Ethical approval was sought from the University ethics committee (IRB number: SKKU 2020 01-003-001).
Funding
This work was supported by the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021S1A5A8062262)
Guarantor
YZ
Supplemental material
Supplemental material for this article is available online.
Appendix 1
Demographic characteristics of participants.

| Category | Value | Adults (n:480) | Adolescents (n:495) |
|---|---|---|---|
| Age | Mean | 28.1 | 16.6 |
| Most used social media platform | 13 (2.7%) | 93 (18.8%) | |
| 387 (80.6%) | 229 (46.3%) | ||
| 78 (16.3%) | 165 (33.3%) | ||
| Others | 2 (0.4%) | 8 (1.6%) | |
| Suicidal ideation or suicide attempt | Suicidal ideation | 80 (16.7%) | 99 (20.0%) |
| Suicide attempt | 58 (12.1%) | 83 (16.8%) | |
| Average monthly household income | Lower than 880 USD (1000 K KRW) | 8 (1.7%) | 12 (2.4%) |
| 880 USD (1000 K KRW)-1760 USD (2000 K KRW) | 47 (9.8%) | 35 (7.1%) | |
| 1760 USD (2000 K KRW)-2640 USD (3000 K KRW) | 100 (20.8%) | 73 (14.7%) | |
| 2640 USD (3000 K KRW)-3520 USD (4000 K KRW) | 55 (11.6%) | 86 (17.4%) | |
| 3520 USD (4000 K KRW)-4400 USD (5000 K KRW) | 61 (12.7%) | 86 (17.4%) | |
| 4400 USD (5000 K KRW)-5280 USD (6000 K KRW) | 46 (9.6%) | 57 (11.5%) | |
| 5280 USD (6000 K KRW)-6160 USD (7000 K KRW) | 25 (5.2%) | 47 (9.5%) | |
| 6160 USD (7000 K KRW)-7040 USD (8000 K KRW) | 47 (9.8%) | 32 (6.5%) | |
| 7040 USD (8000 K KRW)-7920 USD (9000 K KRW) | 18 (3.8%) | 17 (3.4%) | |
| 7920 USD (9000 K KRW)-8800 USD (10,000 K KRW) | 17 (3.5%) | 12 (2.4%) | |
| More than 8800 USD (10,000 K KRW) | 54 (11.3%) | 34 (6.9%) | |
| No income | 2 (0.4%) | 4 (0.8%) | |
| Region | Seoul | 112 (23.3%) | 101 (20.4%) |
| Busan | 46 (9.6%) | 21 (4.2%) | |
| Daegu | 46 (9.6%) | 20 (4.0%) | |
| Incheon | 20 (4.2%) | 43 (8.7%) | |
| Gwangju | 33 (6.9%) | 26 (5.3%) | |
| Daejeon | 25 (5.2%) | 24 (4.8%) | |
| Ulsan | 9 (1.9%) | 9 (1.8%) | |
| Gyeonggi-do | 75 (15.6%) | 133 (26.9%) | |
| Gangwon-do | 5 (1.0%) | 11 (2.2%) | |
| Chungcheongbuk-do | 15 (3.1%) | 12 (2.4%) | |
| Chungcheongnam-do | 16 (3.3%) | 16 (3.2%) | |
| Jeollabuk-do | 14 (2.9%) | 12 (2.4%) | |
| Jeollanam-do | 11 (2.3%) | 12 (2.4%) | |
| Gyeongsangbuk-do | 20 (4.2%) | 10 (2.0%) | |
| Gyeongsangnam-do | 20 (4.2%) | 37 (7.5%) | |
| Jeju-do | 11 (2.3%) | 3 (0.6%) | |
| Sejong | 2 (0.4%) | 5 (1.0%) |
Appendix 2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.