
Abstract
Objective
The purpose of this study was to investigate whether a virtual reality (VR) program designed and developed based on the hallucinogenic harm reduction and integration (PHRI) clinical model could be more effective in guiding positive thinking training, improving positive thinking awareness and ability, and, to some extent, facilitating personal efficacy and emotional state compared to a traditional VR program that places users in a virtual natural ecological environment to guide positive thinking training. We also sought to understand the factors that may influence the effectiveness of VR interventions and user experience.
Method
Seventy-six randomly recruited participants were divided into a control group and an experimental group of 38 participants, each according to a random number table, and were trained in VR meditation for eight weeks. The experimental group used a PHRI-based mindfulness program, while the control group used a traditional mindfulness meditation program. We used The Mindful Attention Awareness Scale and the PAD emotional three-dimensional scale to assess the level of state mindfulness and changes in the emotional state before and at the end of the experiment. The Immersive Tendencies Questionnaire measured the user's sense of presence and immersion in the virtual environment. The Five Facet Mindfulness Questionnaires and the Depression Anxiety and Stress Scale (DASS-21) were used at the baseline assessment stage before and at the 4-week follow-up after the experiment to assess the change in trait mindfulness levels due to the mindfulness training. The Five Facet Mindfulness Questionnaires and the DASS-21 were used to assess changes in mindfulness and mental health trait levels.
Results
At the end of the experiment, the MMSQ score was significantly lower in the control group than in the experimental group, while the ITQ score was significantly higher than in the experimental group, and both scores were statistically significant (p < 0.05). In the follow-up assessment four weeks after the end of the experiment, the FFMQ-15 score and the DASS-21 were significantly and statistically higher in the experimental group than in the control group (p < 0.05). Since the scores of the PAD scale did not obey a normal distribution, we used the Wilcoxon signed-rank test to assess the results, which proved that the experimental group had higher levels of emotional activation and arousal.
Conclusion
The VR positive thinking program developed based on PHRI can significantly increase the positive thinking state and emotional arousal and activation of the general population participants but does not directly lead to the growth of positive emotions. Moreover, this detached psychedelic scene brings users a weaker sense of presence and presence than traditional natural space scenes. Furthermore, it does not bring any intense simulator motion sickness symptoms. These findings suggest that VR programs developed based on PHRI have a more positive facilitation effect on the positive state and that this increase lasts longer than conventional VR-positive programs.
Introduction
Background
In the Global Burden of Disease, Injury, and Risk Factors Study, mental disorders are ranked as a Tier 3 cause of all types of disease. 1 Based on the 2019 research report published by the “Global Burden of Disease Study,” depressive disorders emerge as the leading mental disorder in terms of disease burden globally and in China. Globally, depressive disorders rank 13th among all diseases regarding disease burden, whereas in China, they hold the 11th position. 2 The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 presented a revised categorization and classification of mental disorders. The included disorders were major depressive disorder, dysthymia, comprehensive estimation of all subtypes of anxiety disorders, comprehensive estimation of all subtypes of bipolar disorder, schizophrenia, autism spectrum disorders, conduct disorders, attention-deficit/hyperactivity disorder, eating disorders (anorexia nervosa and bulimia nervosa), intellectual disability of unknown etiology, and residual categories comprising other mental disorders (a comprehensive group incorporating personality disorders). 1 Evidence has demonstrated the efficacy of multi-level treatment and support for individuals with mental disorders in clinical environments. However, inadequate societal understanding of mental illnesses contributes to substantial stigma and discrimination, impeding public initiatives and interventions in the healthcare domain aimed at addressing and promoting mental health. 3
Furthermore, the COVID-19 pandemic, which began in 2019, has altered the current social environment with an increase in adverse determinants for mental health. Epidemiological studies suggest that the direct psychological impact of pandemics on humans and the long-term economic and social effects may increase the prevalence of common mental disorders. 1 In addition, mental disorders have high co-morbidity rates of anxiety and depression disorders, bipolar disorder, and suicide attempts. Therefore, it is imperative to develop and improve interventions for psychiatric disorders.
Psychological interventions are the treatment of choice for mild to moderate psychiatric disorders such as depression and anxiety. 4 Among others, positive thinking training benefits mental health by helping people increase attentional flexibility and take an experience-oriented approach to reduce reliance on intuitive thinking or maladaptive emotion regulation strategies. 5 Published studies in recent years have shown that mindfulness-based interventions (MBIs) have excellent therapeutic effects,6,7 and mindfulness-based cognitive therapy (MBCT) is recommended as the treatment of choice for the prevention of recurrent depression. However, the effectiveness of mindfulness training is not only influenced by the individual's personality but also because the process of mindfulness requires conscious effort, which can be challenging to maintain for novice meditators who have already spent more cognitive resources to control their self-mediation skills8,9 summarized the empirical challenges that may be encountered during positive thinking training, including emotional demands such as cognitive effort and frustration, task demands of being in a specific situation (e.g. noisy surroundings and crowds), and adverse emotional and psychological outcomes such as boredom, frustrated thoughts, and emotions. Therefore, appropriate adaptations and adjustments to positive thinking training to reduce these challenges may increase the likelihood of successful, positive thinking interventions.
Psychological interventions are the treatment of choice for mild to moderate psychiatric disorders such as depression and anxiety (clinical in addition to personal reasons, the effectiveness of positive thinking training is primarily influenced by the skills of the psychotherapist). Artificial intelligence and the Internet have made it possible to standardize the procedures associated with positive thinking training by using the user's multisensory perception and attention. Virtual reality (VR) has recently been proposed as a mediating tool to guide people through positive thinking training. 10
VR can provide an immersive, human-controlled, and engaging visual and auditory sandbox to reduce environment-induced distractions and attention wandering during mindfulness and thus better train mindfulness skills.11–13 By creating a “sense of presence” while stimulating the user's multisensory perception, VR creates an “illusion of reality” in which the user acts like a natural person in the virtual environment (VE), even if it is computer-generated.14,15
Currently, psychotherapy combined with pharmacotherapy is usually used more often for clinical populations suffering from depressive and anxious mood disorders, 16 and hallucinogens have renewed the interest of scientists as potential drugs for the treatment of various neuropsychiatric disorders. According to previous experimental reports, psychedelics used as an adjunct to psychotherapy have shown efficacy in reducing anxiety and depressive symptoms. 17 There is a renaissance of hallucinogens, including naked caprine, N, Nʹ-dimethyltryptamine, and lysergic acid diethylamide, which have rapid therapeutic activity. A large and growing body of research has demonstrated the potential of psychedelic-assisted psychotherapy in enhancing the treatment of PTSD, depression, terminal anxiety, and substance use disorders.18,19 This enables the utilization of psychedelic substances in conjunction with psychological interventions. Mindfulness training is typically synergistically integrated with psychological interventions to enhance mental health by assisting individuals in observing and accepting their internal experiences. Psychedelic substances, in turn, can offer supplementary facilitative effects within this process, heightening individuals’ awareness of their emotions and thoughts. 20 Using this class of drugs increased the ability to relate to positive thinking. After ingesting ayahuasca, increased levels of positive thinking, self-compassion, and “distraction”can be interpreted as the ability to understand thoughts and emotions as transient mental events without becoming trapped in them. 21 Psychedelic drug use can be viewed as a transformative mystical experience, and its induction of the ability to think positively may contribute to significant increases in well-being and mood. 22 Moreover, psychedelic substances can induce alterations in consciousness, amplify individuals’ awareness of their internal experiences, and offer avenues for profound contemplation and introspection. Consequently, these effects converge with the objectives pursued through mindfulness training. 23 Published reports have also shown decreased depression and anxiety following the use of natural psychedelics during rituals and recreational activities.24,25 In contrast, positive thinking originates in Buddhist practice, a conscious, unbiased activity of awareness of the present moment. 26 However, the fact that psychedelic use causes changes in the user's brain that lead to relapse of neurobiological disorders has led to the use of such drugs becoming involuntary, that is, addictive. 27 More importantly, there are still some gaps in the research on hallucinogens, such as the inability to establish an appropriate dose criterion between the positive effects of the drug and the harms, 27 which is a significant limitation. At the same time, the mental health benefits of psychedelics diminish with the frequency of use. 28 This attenuation also underscores the importance of the attitude of the drug-using population towards such drugs, that is, using psychedelics as a transient stimulus to initiate a lifestyle/perspective that is protective of mental health rather than attempting to use such drugs as a lifelong mood regulator. A growing body of research proves that psychedelic drugs are not irreplaceable and that their therapeutic effects cannot be attributed exclusively to neurobiology. Instead, the patient's subjective experience with their post-medication psychedelic experience appears to play a crucial role in recovery from mental illness, with much of the relevant literature specifically highlighting this psychedelic experience and naming it the “mystery trip.” 29 Moreover, a related study by Davis et al. 30 pointed out that the acute psychedelic effect after taking psychedelics, which reduces depression/anxiety, is due to the crucial mediating role of psychological flexibility. While conservative scholars in the field will only use the term “psychedelic” to refer to tryptamines or phenylethylamines that trigger altered states of consciousness, the term can be applied more broadly to the experiential awareness that opens up perception and allows for altered states—with or without drugs are used. 31 Many researchers in psychedelic medicine consider awe to be one of the vital therapeutic elements of the psychedelic drug experience. Awe has also been described as “the need for expansive perception and adaptation,” leading researchers in recent years to propose a new clinical model of hallucinogenic harm reduction and integration (PHRI). Furthermore, integration (PHRI) is a cross-diagnostic, cross-theoretical model of clinical medicine that integrates the principles of psychedelic-assisted therapy, the positive thinking model, harm reduction psychotherapy, and psychodynamic therapy and provides a framework for examining and processing psychedelic experiences in clinical care without providing actual psychedelic experiences as part of treatment. 27 VR technology then provides room for this alternative philosophy to operate.
The available evidence suggests that VR is a promising tool that can support positive thinking and offer some alternatives to hallucinogens. VR-enabled psychedelic experiences as a substitute for psychedelic drug use can, to some extent, be used in conjunction with drug users to reduce addiction while providing positive thinking training support for non-clinical staff. It is not known whether VR-enabled psychedelic experiences can replace psychedelic drugs to some extent, and little is known about whether such experiences can alleviate depression/anxiety to some extent. It is worthwhile to explore what mechanisms and factors influence the effect of positive thinking activities in VEs and the extent to which the psychedelic scenarios and presence of VR technology deviate from the acute psychedelic effects of psychedelics. Research on this issue could inform design decisions for VR programs developed to intervene in positive thinking and provide a more standardized and efficient environment for implementing positive thinking training, subsequently influencing these systems’ effectiveness and application potential.
Objectives
This study explores whether a VR program designed and developed based on the PHRI clinical model can more effectively guide positive thinking training, improve positive thinking awareness and competence, and, to some extent, promote personal effectiveness and emotional states than a traditional VR program that guides positive thinking training. We also sought to understand the factors that may affect the effectiveness of VR interventions and the user experience.
Methods
Description of the VR mindfulness app
The study used a VR program, TRIPP, a VR health platform developed in a psychedelic style based on the PHRI model. Developed by the National Center for Mental Health Innovation in collaboration with Stanford University's Virtual Human-Computer Interaction Lab and the USC Institute for Creative Technologies in Medical Virtual Reality, the program was named the Best Invention of 2022 in The Times and won the CES Award for Best Health and Wellness Innovation and the Lumiere Awards for Best VR and Wellness. The software developer cited its inspiration from a paper on “the power of VR in triggering a state of awe.” It is worth noting that, unlike typical VR programs that guide positive thoughts and meditation, TRIPP does not use VR to create a highly open, free-form simulation of a natural environment but instead use VR technology with optical illusions, symmetrical repetition, and change processing to shape and recreate the visual experience based on the hallucinatory experience of taking hallucinogens in clinical medicine. Meanwhile, the VR application includes a customized positive introduction to the VE provided by a female narrator. The voiceover uses inviting language to guide the user's shift in attention and focus.
Participant recruitment
Participants were recruited from the general population through flyers distributed around the streets of Hui Long Guan in Beijing, on the Beijing University of Posts and Telecommunications campus, and within Central South University. Potential participants completed a web-based screening survey to assess their eligibility for inclusion. Inclusion requirements included being over 18, having normal hearing and vision (including normal with correction), being free of 3D vertigo and visual motion sickness, and not currently taking psychotropic medications or having a severe psychiatric disorder (e.g. schizophrenia or mood disorders). Figure 1 illustrates the recruitment process. Eighty-six participants tried the VR procedure. As shown, a total of 10 participants did not complete the entire procedure and were excluded from the quantitative and qualitative analyses (two participants made technical errors while using the VR device, three participants did not complete the measurements after use, and five participants felt physically ill while using and discontinued use) (Figures 2–4).

Recruiting process.

Experimental procedure.

Some flowcharts of the experimental group (Image credit: Self-cut within TRIPP).

Scene of the contrasts group (Image credit: Self-cut within MIND FRAME).
Study sample
Participants who have completed the investigation and can commit to an uninterrupted two-month period at our research institution, encompassing eight experiments lasting 18 min, are cordially invited to participate in the subsequent trials. Among the 76 participants in the study, 47 had either no prior experience with VR or had only encountered it once. Additionally, 22 participants had engaged in VR multiple times, while 7 participants reported regular but infrequent usage of VR less than once a month (n = 7). Regarding mindfulness practice, 28 participants were unaware of it, while 34 participants had heard of mindfulness practice without personal experience. Fourteen participants reported previous engagement in mindfulness practice. Among them, six participants had tried mindfulness practice between 1 and 5 times, and eight participants reported engaging in regular mindfulness exercises at the following frequencies: once a month (n = 6), once a week (n = 2), and daily (n = 0).
Interventions
All tests were administered at the Science Center of Central South University. After informed consent, all participants completed the baseline questionnaire, the Positive Thinking State Scale, and the Anxiety and Depression Mood Scale. The researcher agreed with the participants to participate in positive thinking training at the Science Center every Saturday afternoon for two months, with eight sessions lasting 18 min each.
After completing the baseline questionnaire, the researcher instructed the participants to wear the PICO 4 VR all-in-one machine with the TRIPP VR program pre-installed and verbally instructed the participants how to manipulate the handle and start the VR positive thinking program. This instruction aimed to help the participants understand the positive thinking process and operation method in advance, and it should have been counted in the number of positive thinking training sessions. After the instruction was completed, the participants took off the device. The researcher informed the participants of the follow-up time to come to the science center for the positive thinking training, and then the participants left. The offline experiment lasted two months, with eight sessions of positive thinking training, each lasting 18 min. Participants filled out the Positive Thinking State Scale and PAD Emotion Scale again after the fourth and eighth positive thinking training sessions. One month after completing the training, the FFMQ and the Depression Anxiety and Stress Scale (DASS-21) were distributed to the participants again online, and all scales were completed online at this visit.
VR-based positive thinking training types
Experimental group: VR positive thinking based on PHRI theory
Participants assigned to the experimental group followed the instructions provided in TRIPP to perform positive thinking. Before starting positive thinking, the program provided two short items to collect the user's emotional state, and the program automatically assigned scenarios to the user based on the user's emotional state. The participant is asked to follow the instructions and tasks by controlling the direction of breath flow and attention according to the guided voice and to rate his or her state again at the end of the task. A training session has a fixed length of time to complete, lasting 18 min.
Control group: conventional positive VR procedure
As the control group, we selected ECO-VR, one of the app store's most common VR mindfulness programs. It utilizes natural landscapes and guided voiceovers to facilitate mindfulness, adhering to crucial non-specific features of TRIPP (such as consistently guided voiceovers combined with soothing background music, brief pre-intervention psychological assessments, and matching intervention duration and frequency). In comparison to the program used in the experimental group, the conventional mindfulness VR program offers higher openness and flexibility, allowing participants to choose from multiple scenes and music options. The scenes predominantly depict natural landscapes, including streams and forests. However, it lacks specific guidance on attention and manipulation of breathing frequency. Notably, it needs a distinct style and environmental characteristics. Using this program as the control group, we can more precisely evaluate the adjunctive effects of psychedelic experiences on mindfulness. Users can manipulate the viewpoint using controllers. The conventional mindfulness program allows participants to set the duration independently. To control for the time variable, the intervention time for the control group was also set at 18 min.
Measurements
Quantification of mindfulness levels
In recent years, researchers have widely recognized the need to evaluate mindfulness states from two distinct dimensions: state mindfulness 32 and trait mindfulness.33,34
State mindfulness refers to the immediate state experienced during mindfulness practice, involving concentrated and non-judgmental metacognitive monitoring of cognition, emotions, sensations, and perceptions in the present moment, untethered by past or future experiences. To assess the immediate impact of mindfulness in our VR-guided mindfulness training, we employed a state mindfulness scale to quantify real-time levels of mindfulness and perceptual changes. These scale scores served as the primary outcome measure.
On the other hand, trait mindfulness captures the enduring individual differences in mindfulness, which can be cultivated through persistent mindfulness training. 35 To evaluate the long-term effects of our experiment on mindfulness levels, we measured trait mindfulness during both the baseline assessment and follow-up stages.
Notably, previous studies have revealed a significant covariate effect (positive effect) between state mindfulness and trait mindfulness, suggesting that improvements in state mindfulness over time can facilitate an elevation in future trait mindfulness levels. 36
Primary outcomes
The researchers employed the Mindful Attention Awareness Scale, a 21-item questionnaire, to evaluate the changes in state mindfulness levels before and after VR usage.37,38 This scale focuses primarily on assessing the frequency of mindfulness states over a specific timeframe, making it suitable for capturing immediate variations in mindfulness levels. It is widely used to measure users’ immediate mindfulness states. Notably, the scale intentionally excludes emotions, attitudes, and motivations to maintain a neutral assessment of mindfulness as a construct. 39 Ratings for each item were recorded on a Likert scale ranging from “0 = Not at all” to “4 = Very much,” resulting in a total score range of 0–84. The State Mindfulness Scale demonstrated excellent internal consistency before (Cronbach's alpha = 0.93) and after (Cronbach's alpha = 0.93) mindfulness guidance through the VR program.
Changes in the emotional dimension were assessed using the PAD Emotion Three-Dimensional Scale, derived from the PAD Three-Dimensional Emotion Theory. 40 This theory posits that emotions encompass three dimensions: Pleasure-displeasure (P), reflecting the positivity or negativity of the individual's subjective emotional state; Arousal-no arousal (A), indicating the level of physiological activation experienced by the individual; and Dominance-submissiveness (D), representing the individual's perceived control over the situation and others. The PAD model aligns with the widely accepted Stimulus-Organism-Response (SOR) paradigm, commonly employed to elucidate the impact of stimuli on human emotions, intentions, and behaviors. 41 Extensive research substantiates the effectiveness of the P, A, and D dimensions in explicating human emotions and affective experiences.
Secondary outcomes
The researchers used the Simulator Sickness Questionnaire (SSQ) 42 to examine whether there were changes in simulator sickness symptoms before and after VR use and whether there were differences in the level of discomfort associated with different VR procedures. Sixteen items (e.g. headache, dizziness, and difficulty concentrating) were included in the SSQ on a scale of “0 = none” to “3 = severe” as a measure of the presence of sensory conflict and triggers of postural instability in the procedure. Since the items in the SSQ partially overlap with those in the DASS-21 mentioned above, this questionnaire was used both before and after the VR procedure to determine the changes in physical signs brought about by operating the VR. In this sample, the internal reliability of the SSQ total score was poor before and after the use of VR, and the statistical significance was weak, so the scale was not used as a significant scale for data analysis but as a reflective indicator related to symptoms.
Researchers used the Immersive Tendencies Questionnaire, 43 which contains 29 items, to measure users’ sense of presence and immersion in VEs. With good reliability 44 in this study after excluding item (subtype data). Since immersion is a subjective mental activity that does not fit and is difficult to define with objective physiological indicators and is influenced by both environmental and individual observer characteristics, this study adopted subjective reports to measure relevant attributes of the environment and the individual assessment. Compared to the traditional Presence Questionnaire, the ITQ focuses more on measuring the individual's tendency to engage in daily life and the ability to focus on specific activities, yielding data that better explain the results of this experiment (level of positive thinking and training effects). The questionnaire is based on a semantically differentiated 7-point scale ranging from 29 to 203, with anchor points in the middle, from “0 = none” to “4 = average” to “7 = very much,” in addition to a guide at each end. “The higher the score, the greater the sense of presence and immersion in this VR program.
Data analysis
All quantitative data were processed and analyzed in IBM SPSS statistical software 26.0 and visualized graphically by GraphPad. Descriptive statistics were used to describe the samples. In analyzing the data obtained from the Positive State Scale and the SSQ scale, a two-sided repeated measures t-test was used to calculate the change in mean scores.
Results
Primary outcomes
Demographics and baseline characteristics
Table 1 provides the demographic characteristics of the sample for this experiment, with a similar proportion of males and females, with more males (n = 21; 52.3%), and a mean age of 25.05 years (SD = 4.51), with similar baseline demographic characteristics and no significant differences (p = 0.88 > 0.05).
Baseline characteristics of participants by experiment group.
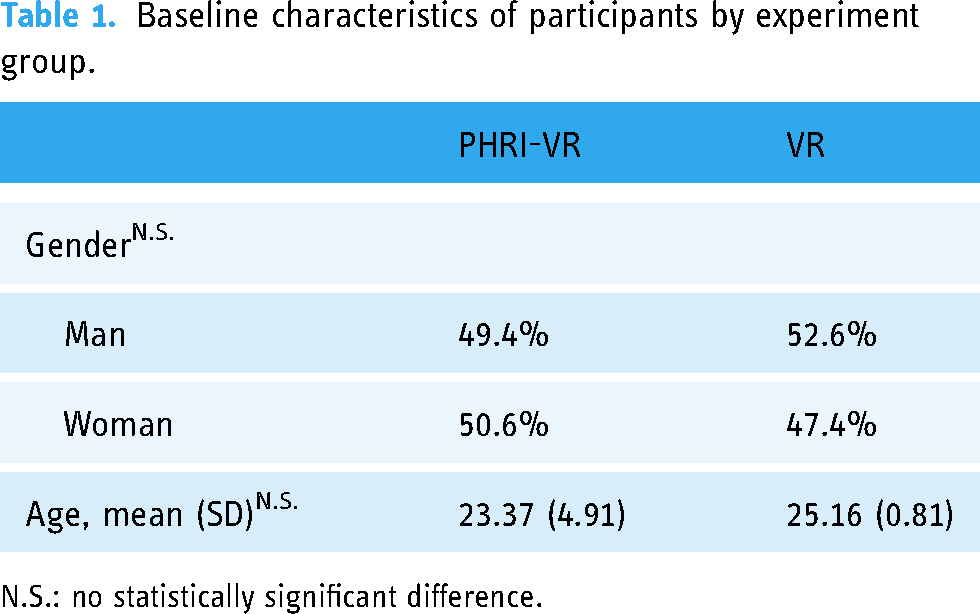
N.S.: no statistically significant difference.
Table 2 provides the mean and standard deviation of the two samples’ trait levels and mental health status before VR was used for positive thinking. Both trait positive thinking levels and mental health conditions were typically distributed across the sample, and both groups faced lower mental health distress, with no significant differences across the four treatment conditions (p-values > 0.05), consistent with the sample conditions of a randomized controlled trial.
Baseline level of mental health by experiment group.
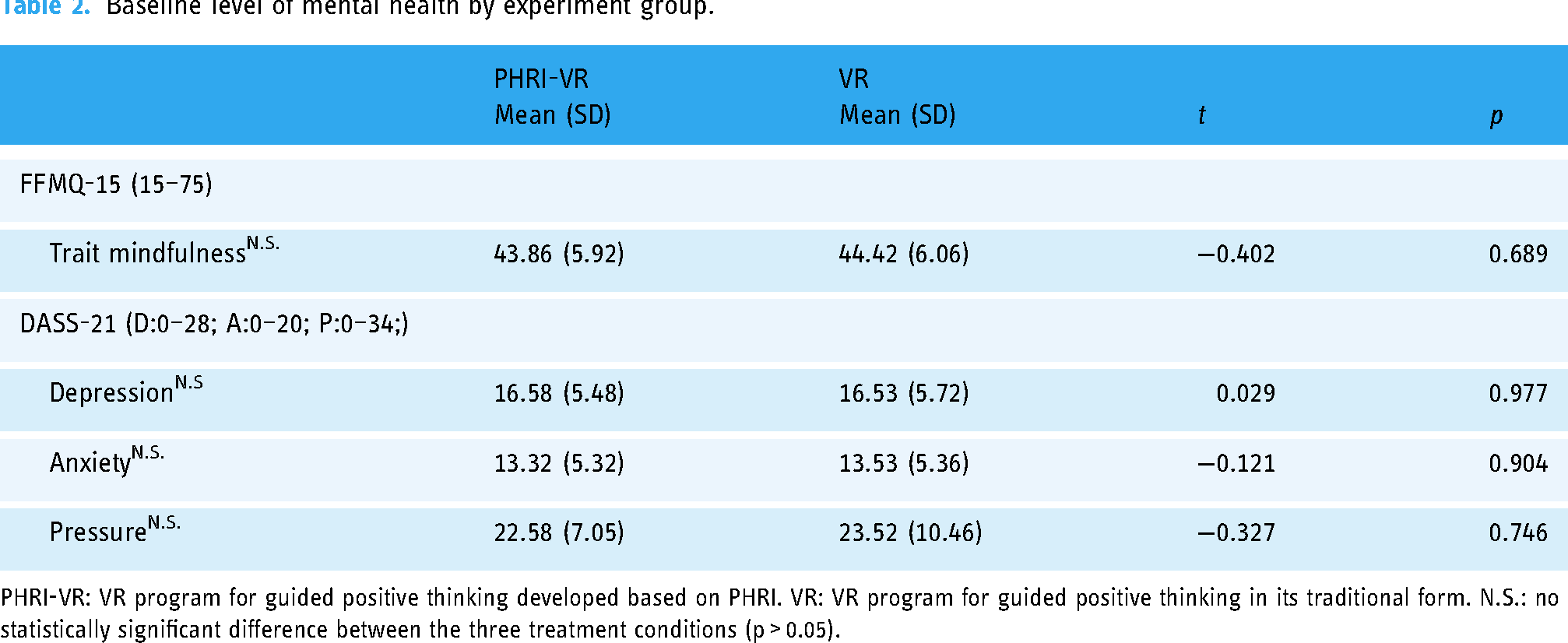
PHRI-VR: VR program for guided positive thinking developed based on PHRI. VR: VR program for guided positive thinking in its traditional form. N.S.: no statistically significant difference between the three treatment conditions (p > 0.05).
The FFMQ-15 was scored on a Likert scale from “0” to “4,” using a short form of the Five-Faceted Positive Thinking Questionnaire (FFMQ). Fifteen items were selected from the original 39 items: “not at all” to “completely.”
The scale autonomously assesses five facets of mindfulness: observation, description, awareness, non-judgmental inner experiences, and non-reactivity. Apart from evaluating an individual's mindfulness level, it also appraises the effectiveness of any previous mindfulness practices undertaken. Scores ranged from 15 to 75, responding to the degree of concentration. Overall, the FFMQ-15 demonstrated good reliability in the sample (Cronbach alpha = 0.79). The current levels of depression, anxiety, and psychological stress among the participants were evaluated using the DASS-21. The scores obtained from this assessment were utilized to measure the participants’ baseline levels of mental health. In this sample scale, the DASS-21 showed good internal reliability (Cronbach alpha = 0.87).
The level of state positive thinking
As can be seen from Table 3, there is no significant difference between the experimental and control groups in terms of positive thinking status before the experiment (p > 0.05). At the end of the 8-week experiment, the positive thinking level of both samples improved. There was a significant difference in the improvement (p < 0.05), with the experimental group's improvement being more pronounced. This indicates that the positive thinking program developed based on the PHRI model is more effective than the traditional VR positive thinking program in training symbolic positive thinking. It was noticed that the level of positive thinking improved in the experimental group compared to the control group. However, the dispersion of the data was also more pronounced. With the standard deviation of the data being more extensive in the case of a normal distribution, the raw data was screened to find out what was causing the dispersion of the data. By screening the raw data from the PHRI-VR group, we found that samples with higher pre-experimental state scores for positive thinking had more pronounced increases in their scores after the uniform positive thinking training, compared to those who already had lower scores who had a slightly less pronounced increase. This resulted in a greater dispersion of the post-test data than the mean. The lack of a large enough sample size may also contribute.
Scores of state positive thinking.

* Statistically significant differences between the two post-experimental groups (p < 0.050).
Change in emotional level
Because of the non-normality of the data obtained from the PAD scale, the Wilcoxon signed-rank test was used to examine the level of change regarding pleasure, activation, and arousal. There was a significant increase in median activation and arousal levels in the experimental group compared to before the use of VR-guided positive thinking, with activation levels increasing from (median = 0.00; interquartile range −2.00 to 2.00) to after the use of VR (median = 1.00; interquartile range 0.00 to 2.00; Z = −2.734; p = 0.006); arousal levels increasing from (median = 1.00 interquartile range: −1.00 to 2) to after VR use (median = 2.00; interquartile range −0.00 to 2.00; Z = −2.586; p = 0.01), there was no significant change in pleasantness. The control group had a statistically significant change in median pleasure (median = 1.00; interquartile range −1.00 to 3.00) after VR use (median = 2.00; interquartile range 2.00 to 3.00; Z = −2.947; p = 0.003;), with no statistically significant change in activation and arousal. Where activation ranged from (median = 1.00; interquartile range −2.00 to 2.00) to after using VR (median = 0.00; interquartile range −2.00 to 2.00); arousal ranged from (median = 1.00; interquartile range −1.00 to 2.00; Z = −0.948; p = 0.343) to after using VR (median = 0.00; interquartile range −1.00 to 1.00; Z = −0.268; p = 0.788). Thus, it can be concluded that the PHRI-based positive thinking procedure has a more significant effect on activation and arousal levels of emotion.
Secondary outcomes
Presence and general system feedback
Table 4 shows that the control group had higher ratings and more significant changes in immersion, indicating that users had a better sense of immersion in the simulated natural environment. In contrast, the psychedelic space presented for the experimental group provided a slightly weaker sense of immersion for the experimenters than the control group.
Score for proximity feedback.

* Statistically significant differences between the two post-experimental groups (p < 0.050).
Follow up
We conducted a return visit, this time online, one month after the interval following the last training session. All participants again completed the Trait Positive Thinking Scale and the Depression-Anxiety-Stress State Self-Assessment Scale, and the results were compared and assessed against the baseline measurements before the start of the experiment. Table 3 shows that both VRIs were able to improve the level of trait positive thinking to some extent, but there were significant differences in the improvement effects, with the PHRI-based VRIs showing more significant improvements. In depression-anxiety-stress, only depression and anxiety showed statistically significant improvements. Compared to the control group, the experimental group showed more significant improvement in depression and anxiety, and there was no significant difference in the reduction effect for stress (Table 5).
Follow-up characteristics of participants by experiment group.

*Statistically significant differences between the two post-experimental groups (p < 0.050).
Simulator sickness
The scoring profile of simulator motion sickness symptoms was low for all items, both before and after using the VR program. Since the item scores in this table do not follow a normal distribution (p = 0.024), the scores were assessed using the median. The median motion sickness symptom scores were at or below the mild symptom awareness threshold (SSQ ≤ 1) in both groups after VR use for positive thinking. Bonferroni-adjusted Wilcoxon signed-rank tests did not show significant differences in SSQ items before and after VR application use (all p > 0.003). At the individual level, participants in both groups were not involved in scoring items that produced severe discomfort after VR use. Participants in the experimental group who experienced mild symptoms after VR use included dizziness (n = 2, changing from “not at all” before the intervention), fatigue (n = 1, changing from “not at all” to “mild”), and mild symptoms after VR use in the control group included difficulty concentrating (n = 1, changed from “not at all” to “mild”).
Discussion
While a large number of previous studies have argued that using VR-guided positive thinking has better efficacy than traditional practitioner-led positive thinking training, few studies have explored the differences between existing VR positive thinking programs in terms of training mechanisms and user experience, and therefore cannot provide guidance for the development of more targeted positive thinking programs in the future.
The present study aimed to explore whether different VR programs produce differences in effectiveness when intervening in mindfulness practice, as well as the possibility and validity of applying PHRI, a clinical medical model, to VR technology to improve mood levels and perceptual states of conventional populations. Our research provides a basis for the future use of psychedelic experience as an intervention strategy for mental disorder-like illnesses and as an alternative to hallucinogens. To achieve these goals, we conducted a randomized controlled experiment in which 76 participants were randomly assigned to two groups to perform positive mindfulness training using different positive mindfulness VR programs, one based on the psychedelic experience positive mindfulness training built on the PHRI model, and the other using the VR to restore a natural scene and perform positive thinking training in that scene.
Our first finding is that both the experimental and control groups have improved their state positive thinking level, which again proves the feasibility and effectiveness of using VR to guide positive thinking training and is consistent with the results of previous studies. However, there is a significant difference in the improvement effect between the two, with the experimental group showing a more significant improvement in the state positive thinking level compared to the control group, which provides empirical support for applying the PHRI model to VR-guided positive thinking.
Our second finding reveals that after using the VR mindfulness program, the experimental group exhibited significantly increased alertness and activation, with no significant change in pleasure. In contrast, the control group showed a significant improvement only in pleasure. This indicates that mindfulness training does not intentionally seek to generate positive emotions but enhances mindfulness levels through cognitive and sensory activation and alertness. These results suggest that different VR mindfulness programs have varying effects, providing individuals with options to achieve different goals through mindfulness practice. This finding may further expand the population benefiting from VR-assisted mindfulness training. However, the extent to which the positive effects result solely from VR usage remains uncertain, as the content presented in VEs may also significantly influence outcomes. As observed in the experimental results, the control group experienced a stronger sense of presence in the VR environment, which may be related to their higher levels of pleasure. Natural environments have been shown to provide individuals with a sense of well-being (Bowler et al., 2010), an effect observed in both VR spaces and non-immersive settings. Future research should explore the mechanisms underlying moderate perceptual experiences, such as alertness and activation, to understand how they impact mindfulness levels.
Our third finding indicates that natural environments evoke a stronger sense of presence than PHRI-based VEs. This may be attributed to the higher authenticity and alignment with users’ existing life experiences offered by natural environments, enabling users to sustain their focus on the visual elements provided by virtual natural spaces. Presence believed to support mindfulness activities can be disrupted when compromised. Addressing the challenges faced by traditional mindfulness training, such as difficulty sustaining attention and concentration and building a profound sense of presence (inherent in immersive VR) may serve as an advantage in guiding mindfulness by facilitating immediate attentional engagement and promoting user involvement.
Finally, according to the results of the follow-up evaluation one month after the end of the experiment, the levels of trait positive thinking in the experimental group and the control group also improved compared to one month ago. Anxiety and depression were relieved, and the experimental group's improvement effect was significantly better than that of the control group. However, it is one-sided to attribute this improvement to the positive thinking training one month ago because the study group is mainly college students. Firstly, the mental and emotional state of college students is susceptible to external influences, and there are a lot of extracurricular activities and social scenes during college, so we cannot rule out that these kinds of factors can also have a good effect on traits positive thinking. Secondly, we cannot exclude the possibility that some individuals in the sample had received other treatment programs during the period. Considering only one month between the follow-up visits, we cannot conclude that positive thinking training has a stable long-term therapeutic benefit on trait positive thinking and mood levels.
Furthermore, participants expressed that although a high degree of freedom in the VR program allows for more exploration opportunities, they often experience a sense of being lost when encountering unfamiliar scenarios. Therefore, timely guidance and assistance are deemed necessary. TRIPP, the VR program under investigation, provides users with instructions during the mindfulness process to ensure alignment between attention and anchors within the VE and allows users to explore within predefined boundaries based on their personal preferences freely. As Anderson and Farb 44 discussed, individuals tend to prefer attentional anchors. Thus, accommodating users’ preferences and motivations to align with these anchors can enhance their engagement in mindfulness training and promote better adherence to mindfulness practices. 44 Moreover, Peters et al. 45 and other researchers argue that digital experiences offer significant advantages over traditional intervention approaches in improving personal motivation, engagement, and overall well-being. Users’ fundamental psychological needs, such as autonomy, competence, and relatedness, can be better satisfied when utilizing digital designs and interfaces.
Future research can explore the inclusion of clinical populations who have undergone treatment with hallucinogens as part of the study sample. By investigating the physiological and psychological mechanisms, in conjunction with the utilization of neuroimaging techniques, it can be examined whether the immersive experiences in VR experiments exhibit synergistic effects with the mechanisms of hallucinogenic substances. Additionally, there is a need to explore the development of personalized VR mindfulness programs that consider individual characteristics or specific symptomatology to achieve more effective intervention outcomes. This requires considering cognitive and psychological traits in the design of tailored VR mindfulness programs.
Limitations
It is important to recognize that the present study still has some limitations. The most important of these is that, although the experiment revealed the positive effects of continuous positive thinking training in a one-month cycle and yielded encouragingly positive results during the follow-up process, it does not sufficiently demonstrate that the VR positive thinking model developed based on the PHRI model can provide a lasting improvement in the level of positive thinking and mood. This is mainly due to the characteristics of the experimental sample itself; the recruitment process took place mainly on university campuses, and thus the sample consisted mainly of university students. College students have the characteristics of volatility and instability. Their emotions and states are easily influenced by the environment and social groups they live in, and at the same time, the university often organizes club activities and social behaviors. A variety of uncontrollable events may occur within a month, which have a certain impact on their state and psychological situation. In addition, although we screened for psychiatric disorders during the recruitment process, we could not rule out the possibility that the subjects had received other therapeutic interventions, nor could we determine whether other treatments would have affected the observed effects of what the subjects had received. Therefore, we cannot fully attribute the positive assessment results obtained at the follow-up visit solely to the positive thinking training one month earlier. It is also not possible to accurately determine how much positive thinking training contributed to the persistence of positive thinking levels and mood improvement effects, so further work is still needed to explore the mechanisms of change in this intervention.
A second limitation of this study is that before the experiment was conducted, participants were informed of the research group to which they were assigned, which may have influenced their expectations to some extent. Second, the assessment of participants’ mental health levels was conducted openly, including measures of depression and anxiety levels, and the stigma and bias associated with mental disorders may have affected the accuracy of participants’ self-reports.
Third, the study did not assess physiological discomfort after using VR. Unlike previous VE scenarios, these immersive hallucinatory environments may induce simulated illness and related symptoms in participants.
Finally, the use of hallucinogens is still strictly prohibited in China, so it was not possible to recruit subjects who had used hallucinogens for qualitative analysis or to confirm whether the app restored the psychedelic experience of the subjects to some extent.
Future research designs should aim to further explore the efficacy of psychedelic-experience-based orthomolecular training in clinical populations and during the treatment of psychiatric disorders. Such exploration should include clinical trials and long-term follow-up studies. Not only that but in countries where hallucinogens are permitted, qualitative analyses such as unstructured interviews and other similar modalities should be added in addition to qualitative analyses to determine whether current VR programs of this type have partially restored psychedelic experiences after hallucinogens are taken. The results of the interviews could determine the feasibility of utilizing this approach as a substitute for hallucinogenic drugs in a clinical setting and guide the further development and improvement of the design of such programs. Finally, consideration should also be given to combining this type of positive thinking training using VR in immersive environments with other therapeutic approaches to examine the potential effectiveness and promise of utilizing such interventions to treat mental disorders.
Conclusion
Positive thinking practice can benefit mental health by enabling an open, accepting, and non-judgmental attitude toward the experience of the present moment. By using VR applications with different scenarios and different forms of intervention, this study explored whether different VR programs differed in their effectiveness in supporting positive thinking practice and explored whether the psychedelic experience delivered by a VR positive thinking program developed based on PHRI could have significant advantages over a conventional realistic scenario positive thinking program. It investigated whether this near hallucinogenic experience might help or hinder the ability to practice positive thinking during user experience issues. We found that the PHRI-based VR orthostatic procedure significantly increased the arousal and activation of positive states and emotions in general population participants but did not directly lead to an increase in positive emotions. Moreover, this detached psychedelic scene brings users a weaker sense of presence and presence than traditional natural space scenes. Furthermore, it does not bring any intense simulator motion sickness symptoms. These findings suggest that VR programs developed based on PHRI have a more positive facilitation effect on the positive state and that this increase lasts longer than conventional VR-positive programs.
Footnotes
Acknowledgments
The authors wish to thank the study participants for their contribution to the research and current and past investigators and staff. The authors want to thank Gaoshan Zuo, Xingwei Luo and Jiahua Li for their assistance.
Contributorship
All authors conceptualized the study and its design. Yanying Chen: supervision; the conception and design of the study; revising the article for important intellectual content; final approval of the version to be submitted. Tianyang Wang: analysis and interpretation of data; drafting the article. Yuxi Tan: revising the article for important intellectual content; Duo Li: data analysis, visualization. All authors contributed to the article and approved the submitted version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was approved by the ethical review board of Central South University before data collection (No. 202312005). All methods were carried out in accordance with local guidelines and regulations. The written informed consent was obtained from each participant.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Humanities and Social Sciences Research Project of the Ministry of Education (grant number: 20YJCZH012). Innovative Province Construction Special Science Project (grant number: 2023ZK4008). CSU Graduate Student Independent Exploration and Innovation Project (grant number: 2022ZZTS0389).
Informed consent
Informed consent has been obtained from all individuals included in this study.
Guarantor
Yanying Chen.