
Abstract
Background
The ability to cope with concussion symptoms and manage stress is an important determinant of risk for prolonged symptoms.
Objective
This open-label mixed-methods pilot study assessed the acceptability and credibility of a mindfulness-based intervention delivered through a digital therapeutic (DTx; therapeutic smartphone app) for pediatric concussion.
Methods
Participants aged 12 to 18 years were recruited from an emergency department within 48 hours of a concussion (acute cohort) or from a tertiary care clinic at least 1-month post-concussion (persisting symptoms cohort). Participants completed a novel 4-week mindfulness-based intervention, for 10 to 15 minutes/day, at a minimum of 4 days/week. At 2 weeks, participants completed a credibility and expectancy questionnaire. At 4 weeks, participants completed questionnaires assessing satisfaction, usability and working alliance, as well as a semi-structured phone interview.
Results
Ten participants completed the study outcomes (7 acute; 3 persisting symptoms). The intervention was perceived as credible (median/max possible = 6.50/9.00 [6.83,8.75]) and DTx was usable (median/max possible = 70.00/100.00 [55.00,82.50]). Participants rated their satisfaction with the DTx (median/max possible = 27.00/32.00 [24.50,29.50]) and the working alliance with the digital mindfulness guides (median/max possible = 3.92/5.00 [3.38–4.33]) as high. Four themes were identified from the qualitative data: (a) positive attributes; (b) negative attributes; (c) ideas for modifications; and (d) technical issues.
Conclusion
Results show modifications to the DTx, instructions and mindfulness intervention, and potential ways to increase adherence by leveraging positive attributes. A randomized control trial will assess the effectiveness of the DTx MBI to decrease the risk of persisting symptoms and reduce the symptom burden following pediatric concussion.
Keywords
Introduction
Concussion, a subtype of traumatic brain injury, is a complex pathophysiological process affecting the brain induced by external biomechanical forces, leading to physical, emotional and cognitive symptoms, as well as sleep disturbances. 1 By 14 days post-injury, most children and adolescents will have recovered; 2 however, 30–35% will experience persisting post-concussive symptoms beyond 4 weeks after injury.3,4 In addition to the burden of symptoms, a concussion can impact sports participation, social life, academic performance, mental health and quality of life. 5 Many adolescents suffer from persisting symptoms after a concussion, but few evidence-based interventions aim to prevent and treat those persisting concussion symptoms. Previous studies have shown that concussions and persisting post-concussion symptoms were associated with the precipitation/exacerbation of mental health issues,6–9 which may significantly impact recovery. Pre- (e.g., personality characteristics, resilience, coping skills and strategies and existing mental health problems), peri- (e.g., symptom burden and balance problems stemming from concussion), and post-injury (e.g., expectation and good old days biases, anger/bitterness, acute traumatic stress or post-traumatic stress disorder and anxiety and depression symptoms) factors were related to poor recovery outcomes and persisting symptoms.10–12 Teaching adolescents how to manage acute symptoms (i.e., in the days following the concussion), stress and emotions may prevent persisting symptoms or reduce the functional impact of symptoms following concussion. Moreover, teaching adolescents with persisting symptoms how to manage their ongoing symptoms and stressors may promote recovery. As such, psychological interventions may be the key components of concussion management in teaching how to manage symptoms, foster adaptive coping skills and promote recovery.
Mindfulness-based interventions (MBI) are psychological interventions designed to help people deliberately focus attention and foster non-judgmental awareness of the present moment. 13 In children and adolescents, MBIs effectively improve general well-being and quality of life and reduce negative mental health outcomes, such as depression and anxiety.14–16 Further, evidence suggests that MBIs may help treat symptoms commonly found following concussion, such as somatic symptoms, pain, fatigue, confusion, working memory issues, executive functioning problems and stress.16–21 To date, there is limited research on MBI effects in youth in the acute or chronic stage of concussion. A recent meta-analysis examining patients of all ages with persisting symptoms after mild to severe traumatic brain injuries found promising evidence that in-person meditation, yoga, and MBIs had positive effects on their symptoms by reducing fatigue and depression, and improving quality of life. 22 Further, adults with persisting symptoms found clinically meaningful improvements in quality of life and perceived self-efficacy following a 10-week group MBSR program. 23 In a pilot study of mindfulness and yoga, participants 15–60 years old reported a decreased symptom score of 50% over a 5-day intervention. 24 In youth, a pilot case series of six patients with persisting symptoms found that an 8-week mindfulness-based yoga program showed a trend towards improvement in self-efficacy across academic, social, and emotional domains. 25 Overall, in-person MBIs show promise in improving self-efficacy, quality of life, stress and depression in those recovering from a concussion and more severe forms of traumatic brain injury. However, to date, no known randomized control trials have investigated MBI in youth as a prevention strategy in the acute phase or as a treatment option in the chronic stage of concussion. While MBIs show promise for concussion treatment, there may be significant barriers for adolescents to access this care. Formal MBI programs are costly, require a trained therapist, and are only available at specific times and locations. 26 MBSR requires a commitment by participants and parents for periods of 8 to 16 weeks for in-person weekly meetings and daily at-home exercises. Further, in-person concussion care involves additional barriers to access, such as limited amounts of care providers and the predominantly urban location of concussion care clinics. 27 With the increasing use of mobile phones and tablets in youth, mobile health offers a powerful platform for increasing access to mental health interventions.28,29 Advantages of app-based interventions, broadly referred to today as digital therapeutics (DTx), include flexibility in use (i.e., time of day, location), tailored content, lower cost, and increased service capacity. Moreover, adolescents’ perspectives on telehealth services are generally positive30–32 and their digital literacy is unprecedented. Findings from populations with mental health symptoms akin to those of concussions suggest that DTx MBIs are effective for reducing stress, anxiety, sleep impairments, and fatigue, as well as improving quality of life.26,33,34 As such, DTx MBIs may be effective in targeting predisposing and perpetuating factors for concussion symptoms. Targeting these factors could prevent persisting symptoms and reduce the burden of persisting symptoms on youth. However, there is limited research on DTx MBI protocols in concussion, especially in pediatric concussion.
Previous studies indicated that attrition rates in studies using DTx MBIs are high, 35 highlighting the importance of soliciting and incorporating participant feedback into DTx design before moving forward to larger-scale feasibility and efficacy trials. Thus, while DTx MBIs may be a promising intervention for adolescents recovering from a concussion, using a mixed-methods approach to determine acceptability for adolescents is critical to develop a targeted intervention, increase adherence, and optimize recovery from a user-centered perspective.
Accordingly, this open-label pilot study aimed to determine the credibility, acceptability, and usability of a mindfulness-based DTx for symptom management and concussion recovery among adolescents who have acute post-concussion or have persisting post-concussion symptoms (>1 month).
Methods
Study design
This is a mixed-methods study using an explanatory sequential design, such that the qualitative data help explain or build upon initial quantitative results. The acute cohort was recruited from an emergency department (ED) from May 2021 to August 2021 and the persisting symptoms cohort was recruited from a tertiary care concussion clinic from May 2021 to June 2022. Patients with persisting symptoms typically present to tertiary care clinics rather than emergency departments. The study was approved by the Research Ethics Boards.
Participants
Youth were eligible if they were: (a) aged 12 through 17.99 years; (b) diagnosed with an acute concussion, as defined by the Berlin consensus statement 1 ; (c) acute cohort: presented to the ED after sustaining a direct or indirect head injury and suffered the initial injury in the previous 48 hours OR persisting symptoms cohort: were referred to the tertiary care concussion clinic by a physician, were greater than 1-month post-concussion and were experiencing at least three concussion symptoms as defined by the ICD-10 criteria for persisting post-concussion symptoms 36 ; (d) proficient in English; and (e) were able to access a smartphone or tablet with an internet connection. Patients were excluded if they had a severe chronic neurological developmental delay resulting in communication difficulties, prior psychiatric hospitalization, or prior diagnosis of a severe psychiatric disorder such as schizophrenia (diagnoses of anxiety or depression were not exclusionary; acute cohort only), or if participants were currently involved in mindfulness therapy or program (persisting symptoms cohort only). Other medical treatment (e.g., medication for psychiatric disorders) or concussion treatment (e.g., physical therapy) was tracked but was not exclusionary.
Recruitment
For the acute cohort, potential participants with a head injury were approached in the ED. A member of the research team briefly described the study. Participants who were interested in hearing more about the study were contacted by telephone the following day for screening and consent/assent.
For the persisting symptoms cohort, potential participants were approached at psychoeducational sessions which are compulsory for all new patients assessed at the persisting symptoms clinic. A research team member joined the virtual sessions to briefly describe the study. All patients were provided with a secure electronic link through REDCap37,38 to provide or decline consent to be contacted about the study later. Participants who were interested in getting more information about the study were contacted by telephone following the session for screening and consent/assent.
Both cohorts followed similar consent/assent methods and procedures. A research assistant (RA) completed eligibility screening and consent and/or assent. Eligible and willing parents, along with adolescents capable of consenting on their own behalf provided informed consent, and those children aged 12 or older unable to consent on their own behalf provided assent. The Tri-Council Policy Statement (TCPS-2) requires children's consent for research to be based on their capacity to comprehend the study's implications, rather than on a specific age.
Procedures
Procedures are visually depicted in Figure 1. The RA sent the app download link and called the participant to walk them through the download and the different app features, and to schedule a weekly texting follow-up meeting. RAs communicated once a week with participants via text or phone call to address any technical difficulties or concerns and to maintain a rapport with the participants in the hope of improving adherence (i.e., coaching system). RAs followed a detailed standardized script. Participants were required to complete questionnaires via REDCap37,38 at 2 and 4 weeks, Table 1 includes assessments collected at 2 and 4 weeks. Participants completed a qualitative semi-structured interview via phone or Zoom at 4 weeks. Participants from the acute cohort were renumerated with a $10 gift card (e.g., Chapters) for completing the study and received a letter attesting that they completed 10 hours of volunteer work. Participants from the persisting symptoms cohort received a $15 gift card for completing the interview.

Study flow diagram.
Overview of the participants’ characteristics.
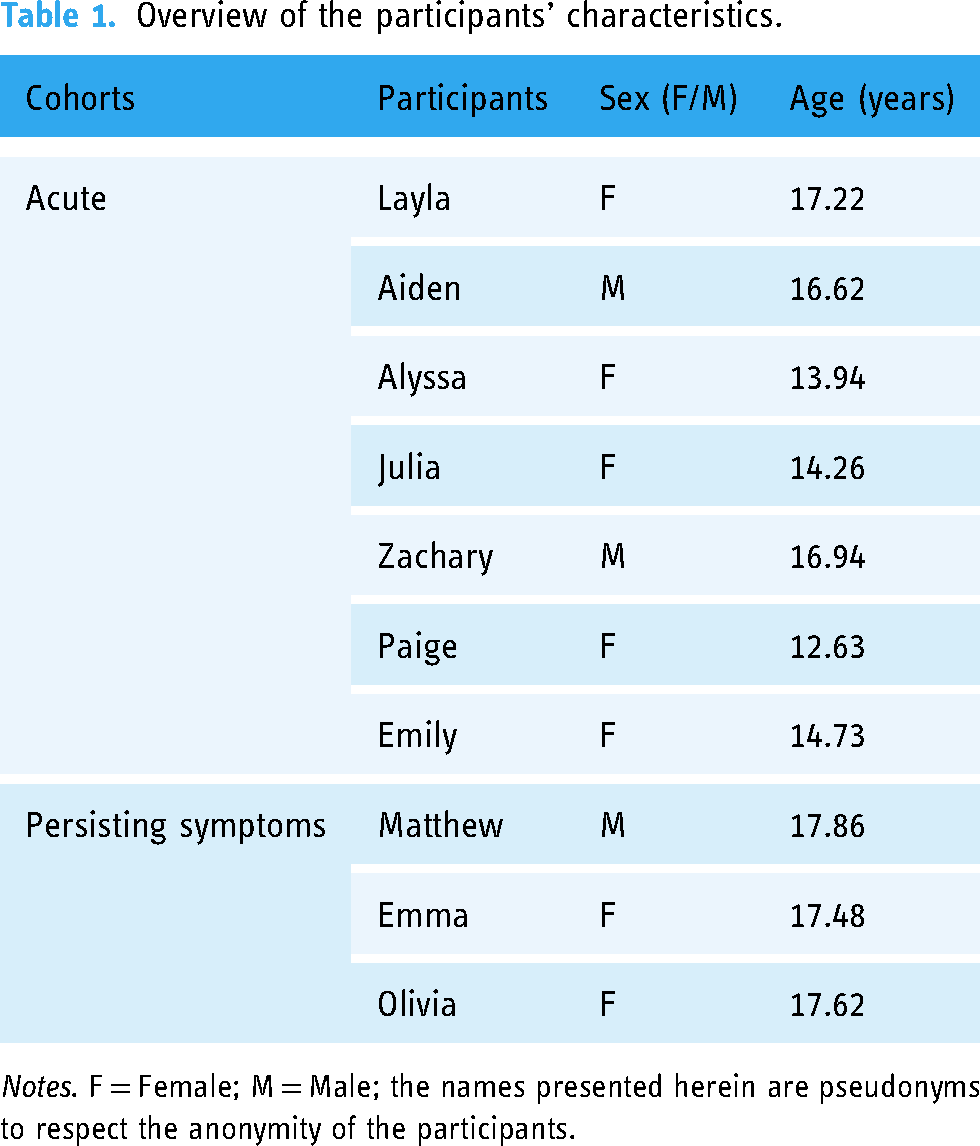
Notes. F = Female; M = Male; the names presented herein are pseudonyms to respect the anonymity of the participants.
Intervention
We partnered with the DTx developer Mobio Interactive to create an MBI on a validated DTx platform that includes subjective and objective measures of wellbeing (AmDTx, Mobio Interactive, Toronto, ON).19,39 The targeted MBI for this open-label pilot trial consists of a 4-week custom-made program for adolescents with concussion. The intervention was developed based on the structure and general content of MBSR with modifications and content specific to youth and to concussion.
It includes setting intentions and check-ins on mood and stress, audio-recorded psychoeducation, and guided meditations such as body scans, journaling and homework exercises within the DTx. Each interventional module was unlocked as the adolescents progressed through the full program, ensuring standardization of content delivery. Figure 2 showcases screenshots of the DTx's user interface.

Screenshots of the user interface of the digital therapeutics mindfulness-based intervention targeted to youth with concussions. (A) AmDTx main screen; (B) modules screen menu; (C) mindfulness practices screen menu; (D) psychoeducation or meditation practices menu; (E) journal log menu screen; and the four measurements included in the Snapshot feature: (F) psycho-biometrics measurement; (G) 4-quadrant emotion mapping board; and (H) stress level slider and personal notes using an open field text box.
Participants were encouraged to participate in the DTx MBI activities for 10–15 minutes every day, with a minimum of 4 days a week, over a period of 4 weeks. The curriculum is based on previously validated AmDTx protocols19,25,39 and team expertise in youth MBI, and was peer-reviewed by experts in the field and a parent engagement leader. Participants of the acute cohort received usual care instructions in the ED, that is patients should refrain from physical and cognitive activities for 24–48 hours after injury; 1 after 24–48 hours, they were instructed to gradually introduce activities in their routines.
Targeted approach
Our intervention was specifically designed to meet the unique needs of youth recovering from concussion. First, the modules provide psychoeducation content that addresses the symptoms commonly experienced during concussion, offers explanations on how mindfulness practices can assist youth in coping with these concussion symptoms, and includes relevant examples and guidance related to the resumption of school and sports activities, which are directly applicable to the concussion context. Second, the language was adapted for youth. We avoided jargon or complex terminology in content, broke down complex concepts, used concrete and tangible language to explain mindfulness practices, and incorporated youth culture to relate mindfulness practices to their interest. Third, we strongly emphasized user-centered design during the development of the DTx to ensure that the unique needs of individuals who have experienced a concussion were considered. This encompassed addressing specific challenges such as light, noise and screen sensitivity. We opted for a dark background with light text, and we avoided the need for scrolling by presenting the text and content directly on the screen. Moreover, we incorporated the ability to adjust sounds and ambient noises within the intervention. This feature enables individuals with noise sensitivity and headaches to personalize their experience according to their comfort levels. We also made the content predominantly audio-based, reducing the reliance on heavy reading. Fourth, to enhance engagement and motivation, we integrated gamification elements such as progress tracking and interactive features. By incorporating these concussion-specific features, our intervention aims to provide targeted support and guidance that is directly relevant to the unique challenges faced by youth during their concussion recovery journey.
Snapshot feature
AmDTx contains four easy-to-use measurement features that provide a longitudinal readout of participants’ wellbeing. Participants have the option to take these measurements before and after a session. First, cognitive stress is objectively quantified through a 30-s “selfie” video that uses an algorithm to extract heart rate and two power bands of heart rate variability from the biosignals inherent to the human face using photoplethysmography imaging principles. 40 This information is analyzed through a deep neural network trained on tens of thousands of video and stress pairings, categorizing cognitive stress as ‘very low’, ‘medium low’, ‘medium high’, and ‘very high’ with 86% accuracy. 41 Second, emotional stress levels are assessed via a digital 4-quadrant emotion mapping board (circumplex) that lists a range of emotions positioned along axes representing unpleasant to pleasant and mild to intense. Each emotion is assigned an undisclosed score to the user, which is utilized to calculate an implicit measure of mood. Third, subjective stress is obtained via a slider ranging from ‘none’ to ‘extreme’. The outputs of mood and stress slider measures have been benchmarked to standard psychological surveys. 19 Fourth, personal notes are imputed using an open field text box.
Coaching system
The coaching system consisted of standardized text messages or email follow-ups to the participant to support the participants throughout the 4-week intervention. We employed a series of standardized text messages or email follow-ups to ensure optimal engagement with the program. Our dedicated coaches (trained research assistants) reached out to participants on a weekly basis, not only to monitor any technical difficulties and provide solutions but also to provide guidance and support.
Quantitative questionnaires and outcome measures
The specific endpoints are presented in Figure 1.
Credibility and expectancy questionnaire
Treatment credibility and expectancy were assessed with the Credibility and Expectancy Questionnaire (CEQ) at 2 weeks in the intervention. 42 The CEQ is a validated and reliable 6-item questionnaire rated on a 1-to-9-point Likert scale. Items load onto two distinct factors: credibility and expectancy. The first three items of the scale load onto the credibility factor and the final three items load onto the expectancy factor. Higher scores indicate higher credibility and expectancy. Scores are averaged for each factor (range 1–9).
Client satisfaction questionnaire
Acceptability was measured with a modified version of the Client Satisfaction Questionnaire (CSQ-8) at 4 weeks (i.e., end of the intervention). 43 This is a validated, reliable, 8-item questionnaire rated on a 4-point Likert scale used to measure client satisfaction with a particular program or service. In this case, the questionnaire has been modified to assess participant satisfaction with the DTx MBI. An overall score is computed (range 8–32) by summing item responses. All items were coded such that a higher score indicates higher satisfaction.
System usability scale
DTx MBI usability was measured using a modified version of the System Usability Scale (SUS) at 4 weeks. 44 The SUS is a validated and reliable 10-item measure. For the current study, the scale was modified to measure the usability of the DTx. The responses were converted to a range of possible values from 0 to 100 that do not equate to percentages. Specifically, for the odd items, one is subtracted from the participant's response, and for the even-numbered items, the participants’ response is subtracted from five. Then, the converted responses are summed, and the total is multiplied by 2.5. A higher score indicates higher usability.
Working alliance inventory
The working alliance was assessed with the Working Alliance Inventory for guided Internet Interventions (WAI-I) at 4 weeks. 45 The WAI-I is a validated and reliable 12-item questionnaire rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). The scale has been modified to measure working alliance with the mindfulness guides of the DTx MBI. The responses are averaged into a total scale (range 1–5), and two sub-scores: task and goal agreement with the program (8 items; range 1–5) and bond with the guides (4 items; range 1–5). Higher scores indicate better alliance. Only the total score was analyzed in the present study.
Qualitative semi-structured interviews
Semi-structured interviews were used to gain a deeper understanding of factors that may impede or facilitate the use or effectiveness of the intervention. During the telephone interview at 4-week post-enrollment, the trained research member inquired about the overall experience with the DTx MBI, the guides who guided the mindfulness practice, the intervention, and the support obtained throughout the protocol. The interviewer used a standardized script and contained 20 open-ended questions, as well as prompts and probes based on participant responses. The script followed and prompts are presented in Supplemental Materials. The interviews were audiotaped.
Data analyses
Descriptive statistics were used to summarize data from the acute and persisting symptoms cohorts, as well as the total cohort. Quantitative data from the acute and persisting symptoms cohorts were reported separately to explore potential differences in acceptability, usability and credibility that could be related to differences in duration and nature of symptoms. All audio recordings were transcribed verbatim by an RA, reviewed for accuracy by the first author, and managed in NVivo. The analysis used thematic analysis, a flexible method that is widely used in qualitative health research, to analyze and code data. Qualitative data were analyzed in four stages. The first author read each transcript and highlighted key points. The first author possesses previous experience with qualitative data analysis and led the analysis and developed themes aligned with usability, acceptability, and adherence. The last author independently coded 20% of each transcript; any discrepancies were reviewed and discussed. 87% agreement on the themes between the raters was reached. After the initial coding of the themes, open coding was used to delve into specific information to find emerging subthemes or patterns. After this coding process, the findings were discussed with four additional co-authors, including coaches and the co-last author. All codes were reviewed and aggregated according to the themes and subthemes deemed appropriate and subsequently labeled accordingly. The in vivo codes were then aligned to the final themes and sub-themes. All names used to identify participants in this article are pseudonyms, to protect their anonymity. However, when assigning pseudonyms, an effort was made to choose ones that reflected the culture and ethnonational background of the participants’ names.
Results
Participant characteristics
For the acute cohort, 10 participants were enrolled; of these participants, 7 participants (5 females and 2 males; median age = 14.73 [IQR = 13.94–16.90] years) completed the MBI and the 4-week outcomes. For the persisting symptoms cohort, 6 participants were enrolled; of these 3 participants (1 male and 2 females, median age = 17.62 [17.48–17.86] years, median time since injury = 136.00 [IQR = 96.00–189.50] days) completed the MBI and the 4-week semi-structured interview, but only 2 of them had completed both sets of questionnaires. As such, a total of 10 participants were enrolled in the study. Table 1 provides an overview of the characteristics of each study participant.
Quantitative questionnaires
Descriptive values for the questionnaires are presented in Table 2. Participants from the acute cohort were younger than those from the persisting symptoms cohort. The acute cohort deemed the intervention as credible (77.8%) mid-way through the program (i.e., at 2 weeks), and they were expecting improvement through the intervention (81.4%). At the end of the 4-week program, they rated the usability of the DTx MBI as decent (62.5%), satisfaction with the app as great (90.7%), and working alliance as good (81.6%). In comparison, the persisting symptoms cohort rated the credibility and expectancy lower (respectively, 55.6% and 40.8%) at 2 weeks. At the end of the 4-week program, they rated their satisfaction with the app, the usability of the DTx MBI, and the working alliance as decent (respectively, 76.6%, 63.8%, and 65.8%).
Questionnaire outcomes.

Notes. % = scores transformed to a percentage scale. CEQ = Credibility and Expectancy Questionnaire; CSQ-8 = Client Satisfaction Questionnaire; SUS = System Usability Scale; WAI-I; Working Alliance Inventory for Internet interventions. * IQR (interquartile range) could not be computed due to the small sample size.
Qualitative semi-structured interviews
Qualitative data were categorized deductively under four themes: positive attributes; negative attributes; ideas for modifications; and technical issues. Subthemes were identified inductively. An overview of the results is presented in Figure 3. Additional quotes that supported our interpretation of the results are presented in Supplemental Materials.

Overview of qualitative results.
Theme 1: positive attributes
Participants identified positive attributes of the DTx MBI, mindfulness guides, coaching system, or intervention. They were aggregated into eight subthemes: (a) accessibility; (b) ease of use; (c) intervention; (d) variety of features; (e) mindfulness guides; (f) coaches; (g) ambiance sounds; (h) no expectations to get better; and (i) would recommend the DTx (see Table 3).
Accessibility
Participants from both cohorts appreciated the accessibility of the DTx MBI due to the flexible timing and easy access. Participants could use the intervention whenever they wanted or felt the desire to relax.
It is a lot more convenient if it is on an app. I can do it at any time. [Aiden]
I like that I can do it on my own time because I am more likely to do it because I like to do it really late at night. So doing that for five or ten minutes before I went to bed was perfect. [Zachary]
I definitely like how it was super easy to access, you always have your phone on you. […] Having the pre-recorded stuff is a lot easier to access. And I think that is probably the most important. [Matthew]
Positive attributes.

The participants also enjoyed that the intervention was delivered via a smartphone rather than in person, as they felt no social pressure during the lessons, and they did not have to leave their homes.
Having it on an app made me more comfortable with doing it by myself. [Layla]
It is kind of easier to be yourself I guess, because people can have a hard time talking to people that are in person. [Julian]
It helped because I did not need to move or go somewhere else to do it like an appointment. [Emily]
Moreover, all participants from the persisting symptoms cohort mentioned liking the short-time commitment, and that was important to their overall experience with the DTx MBI.
I like that they [the lessons] were not all that long. You did not have to put that much time during your day. You maybe spend 15 minutes. So, I thought that was really helpful. [Olivia]
One participant from the persisting symptoms cohort mentioned that the DTx MBI color scheme was adequate and was not bothering. This is especially important for concussion populations, as sensitivity to light and headaches are often reported.
Ease of use
All but one participant indicated the DTx MBI was simple to use and straightforward. A participant of the persisting symptoms cohort explained that the tutorial shows you where every button is and that contributed to the usability of the app.
There was not really anything difficult, you just had to follow where it takes you, to click on where it tells you to click. Even if it does not tell you where to click you can just discover things on your own. […] There is not really something that you can’t undo. There are no consequences if you click something. [Layla]
I thought the app was pretty easy to use once you click in. It is a pretty straightforward pathway to where you want to go and what you need to do on the app. [Zachary]
Participants from both cohorts also appreciated the user interface (i.e., the DTx design) and the fact that the different activities were embedded within the app, and that this was important to their overall experience.
I liked that there was a built-in feature to put in the log [journal events]. Sometimes they asked you to do stuff and it would open and tell you to do it instead of having to go get a notebook and do it yourself. [Emily]
One participant from the persisting symptoms cohort expressed that she enjoyed reminders to practice a given meditation exercise multiple times during the week before moving on to the next lesson, as she would have progressed to the next module without the automatic reminders or structure. When asked how those reminders impacted their experience, they answered:
I thought it was good, at least for people with concussion. Like, you have a harder time with memory. So, I think that is definitely thoughtful for us at least where “hey, we understand you might be forgetful. Here's a small reminder”. Oh, thank you. [Emma]
Importantly, most participants mentioned there was nothing they disliked about the DTx MBI or had no problems with it. This contributed positively to their overall experience with the DTx MBI.
Intervention
Participants from both cohorts appreciated the DTx MBI since they felt that the intervention was effective. This was due to multiple factors that were aggregated into 5 subthemes: (a) things they learned; (b) can use the learned techniques in real-life situations; (c) effectiveness of the intervention; (d) intervention specific to concussions; (e) did not feel like a lesson; (f) activities they liked the most.
Things they learned
Beyond the different meditation/mindfulness techniques participants learned through the DTx MBI (e.g., they specifically mentioned the S.T.O.P technique or how to deal with stress), participants mentioned they learned the purpose of mindfulness while using the DTx MBI, and that understanding the purpose of mindfulness was important for adhering to the intervention. They also learned gratitude, which is one of the modules they completed, and learned about themselves.
I just gathered a greater understanding of what mindfulness was, because I had heard about it, but I did not really understand what it was or have as deep of an understanding as I have now. I feel that is really important for me. Having that understanding of mindfulness allows me to understand the importance of it and compels me to implement it. [Zachary]
It kind of gets me thinking more and more grateful and having a more open mind about it and not thinking too negatively. [Julia]
I guess I have learned a bit more about myself. I think the app helped me realize that [my] thinking was off, because all the meditations and stuff were about not trying to change what you are feeling, but working with it, realizing what is going on and working with them. So, I think that is what really helped me. [Olivia]
Can use the learned techniques in real-life situations
Participants from both cohorts have identified different techniques (namely, the S.T.O.P technique, body scans, and walking meditations) learned through the app-based MBI program that they can use in real-life situations. Participants were happy to report that they had applied these learned skills in difficult situations.
I used a modified body scan to distance myself when I was getting frustrated at baseball. [Zachary]
One time I was studying for a physics test that I was really, really stressed out about and I had a very hard time getting to studying. And I noticed that I was thinking and guiding myself through the irrational anxiety thoughts. So I thought that was kind of good. […] I guess that is helpful in real-life situations. [Olivia]
Perceived effectiveness of the intervention
Participants perceived the intervention to be effective, which was deemed a facilitator and motivator to use the DTx MBI. Specifically, the intervention helped them with stress reduction and stress management, as well as emotional management and mood. They reported that the DTx MBI had a calming effect, which was appreciated by the participants. Using some of the techniques learned also helped one participant sleep. Moreover, through the lessons, participants learned how to be in the present moment, and they perceived themselves as having improved focus.
I knew that I was finally getting better and was not just staying the same. [Paige]
That was probably one of the main reasons I used the app. The fact that I feel like it works makes me want to use it more. [Aiden]
Everyday I would try to write in a journal. I would write how I felt that day and I would try to see how stressed I was that day. And I feel like it gradually went down and I think that was, in part, due to the app. [Aiden]
The ability to track progress was a facilitating factor in the use of the DTx MBI and increased adherence because participants felt more motivated to continue the intervention.
I think it was kind of fun to see. It would be like in the beginning or like at the end of listening to one of the audios. At the beginning, I would have a certain mood and then after, it would show how my mood improve. [Alyssa]
I also like the [feature] where you can tell how you are feeling. […] It showed you the point and then your current goal. Then you kind of feel like you did something right, I guess. [Julia]
Intervention specific to concussions
Although MBI is a practice that is not specific to concussions, we have incorporated concussion psychoeducation into the intervention so it would be targeted to concussions. Participants in the acute cohort expressed that this was important to their adherence and the effectiveness of the intervention.
It would not have been as good if I felt like it was not for me. There is the way they spoke about concussion symptoms in the app, and the fact that they addressed some of them made it feel specific to them. [Aiden]
Did not feel like a lesson
This subtheme was unique to the persisting symptoms cohort and was mentioned by one participant.
Activities/features they liked the most
On the topic of preferred activities or features, there was no prevailing activity or feature among participants. Participants identified different activities/features: walking meditations, learning how to deal with stress, psychoeducation, body scans, breathing meditation, S.T.O.P technique, journaling, and ability to track mood and stress levels (snapshot feature) were mentioned.
Variety of features
The DTx MBI includes a variety of features beyond the mindfulness sessions, including psychoeducation material, psycho-biometrics (snapshot feature), journaling, and goal setting. The participants in both cohorts indicated they appreciated this variety, which is further reinforced by the lack of consensus on the preferred activities or features.
The combination of the concussion talk and the meditation talk within one little thing [the intervention] kind of helped. Because then I did not feel pressured to meditate. But then I did not have a bunch of concussion talk. It was like welded together and- or melded together. And so, it just kind of helped you get like the concussion lecture and not be mad at your concussion and then the meditation with it. [Emma]
Mindfulness guides
When asked about what they appreciated about the mindfulness guides, all participants mentioned the guides’ pacing and tone. They described their voices as being calming and they liked the vocabulary they used.
They were really formal and helpful and calm. […] They were straightforward. […]
Participants from both cohorts thought that the mindfulness guides were knowledgeable of mindfulness and concussion
They sound like teachers. […] They had pretty good insight into various different things that I was feeling, and they had a pretty good knowledge of the material. [Zachary]
They highlighted that the guides were an important factor in the likability and effectiveness of the mindfulness program. Importantly, most participants responded there was nothing they did not like about the guides.
They are definitely a big part of [how happy I was with the app]. I would say not the whole thing. But at least two-thirds of the app was them leading you through it. So it was a pretty big part. [Matthew]
Participants from the persisting symptoms cohort said that having the choice between the guides was an important feature of the DTx MBI that contributed to their overall experience and compliance with the program.
One thing I liked is that you have an option between two different voices and people talking. Because I’ve tried a lot of different mindfulness stuff and meditation stuff. And sometimes you don’t really get a choice. So if their voice is really slow or it's a little irritating to you, you can’t change it. You just have to sit through it. [Olivia]
Coaching system
The coaching system contributed to the compliance with the DTx MBI and is an important factor in intervention implementation as the coaches would keep the participants accountable and help them reach their goals by providing support and troubleshooting promptly. The coaches were easy to reach, which was highlighted by the persisting symptoms cohort.
I like that it was texting, because I am also really bad at text. So, I could text at eight o’clock at night, but then the next day, they would get it. It would just be normal. […] When I texted, there was always a response relatively promptly, so I could text about tech issues or just how things were going. [Emma]
They even mentioned that the best part of their experience with their coach was that they were easily reachable by text messaging. Participants appreciated that the coaches would contact them as it would remind them to do the activities when they forgot. They also mentioned that even if the DTx MBI had push notifications or reminders built into it, the coaching system would still be important.
I like that they give you reminders. Reminders are good. It sets like a regularity to it and it encouraged me to keep doing it every day and sort of making a habit of it. It helped a lot. [Aiden]
At the beginning of the intervention, participants had to set three goals they would like to reach with the mindfulness program. When asked ‘Do you feel like your coach helped you work towards your goals?’, most participants answered positively. They mentioned that coaches making sure they were still on track helped them reach their goals.
Coaches provided support to the participants which was appreciated by both cohorts but being able to be contacted by an actual person was mentioned as a positive attribute by the persisting symptoms patients only.
I really liked the weekly check-ins and being able to talk to someone. I think having weekly check-ins and being able to talk to someone if you need help, or if you need anything, like that is the most important. [Matthew]
Coaches were most useful at providing troubleshooting whenever participants encountered technical issues.
Just someone to ask questions to. If I had just downloaded the app on my own, I would probably have ended up deleting it because I had the problem [technical issues] with it. So, I had someone to contact. [Paige]
Participants appreciated that the coaches would respond quickly and that allowed them to progress within the MBI program. All participants were satisfied with the level of support they received from their coach and could not think of anything else they would have wanted from the coaches.
Ambiance sounds
There is an ambiance sound during the activities, including during the mindfulness sessions. The participants can turn the volume down on the ambiance to their preferred level and can choose between pond, beach and rainforest ambient noise. The participants in the acute cohort mentioned they appreciated the ambiance, but they also appreciated they could turn it off.
No expectations to get better
A participant from the persisting symptoms cohort enjoyed that they felt no pressure to get better when using the app. The app provides tools to deal or cope with their symptoms, rather than provide a solution to their concussion.
I feel like I had one thing to help with a concussion that was not someone telling me to get better. It was helping me with, as opposed to telling me to deal with it. […] There was nothing really pressuring me to actually be healed. It was not like “At the end of using this app, you are going to be healed”, it was more of a process instead. [Emma]
Would recommend the DTx MBI
All participants said they would recommend the DTx MBI to a friend who experienced a concussion, but some mentioned they would only do so if there were no technical issues associated with the app.
And if I think that they could possibly use it, I would probably recommend it because it is a good app. I had a good experience with it. [Alyssa]
Theme 2: negative attributes
Participants identified negative attributes of the DTx MBI, mindfulness guides, or intervention. They were aggregated into five subthemes: (a) technical issues are a barrier to use; (b) mindfulness guides were boring; (c) the DTx MBI did not meet their needs; (d) sounds and lights; and (e) hard to navigate (see Table 4). Sounds and lights, and hard to navigate were overlapping for both cohorts; no subtheme was unique to the persisting symptoms cohort.
Negative attributes.

Technical issues are a barrier to use
One participant who experienced technical issues expressed that those issues would prevent or discourage them from using the DTx MBI. They felt the technical issues made the intervention hard to use and they spent a lot of time trying to resolve issues, resulting in the intervention being more of a task than a relaxation method. Without the help of the coaches, they would have stopped the intervention and uninstalled the DTx MBI.
It made it a lot harder. It made it more of a task than a relaxation method when I went to go use it. […] If I had just downloaded the app on my own, I would probably have ended up deleting it because I had problems with it. [Paige]
Mindfulness guides were boring
While some participants thought the guides were calming and soothing, others described them as ‘boring’.
Maybe sometimes they are talking a bit too slow or too calmly. For some of the meditations, they were just teaching me how to be less stressed, but they were speaking too slowly or being repetitive. I felt like I wanted to know what they were going to say. It was almost annoying. [Aiden]
DTx did not meet their needs
One participant from the acute cohort highlighted that the DTx MBI did not quite meet what they needed. They would have liked a variety of features beyond the mindfulness-based intervention.
I think that if it was more interactive with the recovery instead of just suggestions for everyday tasks. I feel like maybe more interactive options for the concussion part more than just listening to the things, because when I went to the concussion clinic, they gave me stuff for my vision, like things that move to just follow. [Paige]
Sounds and lights
Some participants from both cohorts reported that the sounds and lights in the app were bothering them. The presence of post-concussive symptoms such as sensitivity to noise or light might prevent participants from employing the DTx MBI following their concussion.
I think I disliked that when you are done with an activity and you go out, there were bright things that were really loud and annoying. [Layla]
Hard to navigate
Some participants mentioned that navigating through the DTx was difficult or had difficulty finding some features. Maneuvering through the app was difficult […] It is a lot of steps that you have to do […] At first, it was kind of confusing the way it works. [Emily]
Theme 3: technical issues
Some participants experienced technical issues with the DTx MBI. The technical issues can be aggregated into four subthemes: (a) crashing or bugging; (b) could not start or find the concussion journey; (c) progress loss; and (d) difficulties with the biometric face scanner (see Table 5).
Technical issues.

Crashing or bugging
Participants from both cohorts noted difficulties using the DTx MBI, including not being able to sign in, difficulty finding the concussion journey, lessons not starting, and the DTx MBI crashing or being unresponsive. Some of the technical issues made it impossible for the participants to use the intervention, while other issues made it so they wanted to use it less.
Every once in a while, I would open the app, it would make me re-sign in and I would click sign in and it would just be a little wheel like it is loading but then it would never load. [Aiden]
Could not start or find the concussion journey
Some participants from both cohorts were unable to find the concussion journey or start the concussion journey. Without the help of the coaches, they would not have been able to begin the intervention.
I had signed in and I just could not access the concussion one. I had to get a little bit of help the first time I used it. It had to reset or something. But after that, it was really good. [Matthew]
Progress loss
Some participants in the acute cohort experienced progress loss and they had to repeat activities that were previously completed. This issue mostly arose when the arrow to leave the completed lesson would not appear and the participants had to restart the DTx MBI. In that instance, the data were not saved.
There would be days where I would not be able to log in and after a certain point each time I got to listen to more audios, it would just completely restart how many I listened to. And so I would have to do all the ones I already did, over again just to get back to where I was. [Alyssa]
Difficulties with the biometric face scanner
Participants in the acute cohort reported that the biometric face scanner was sometimes difficult to use, as it would take some time to get it to focus. While this difficulty did not make the participants dislike the app, they found it ‘annoying’.
A lot of the time I had to sit there for an extended period of time and hold my phone in front of me with my arms up and I started shaking and it would make me redo it. [Zachary]
Theme 4: ideas for modifications
Participants were asked for ideas for the improvement of the DTx MBI to make it more useful and likable, and to increase their compliance with the intervention (see Table 6). For example, participants suggested adding a push notification system as it would likely increase their compliance with the MBI program. Further, although a few participants mentioned the length of sessions as a potential modification to the DTx MBI, there was no consensus on what the ideal length would be. Some participants mentioned that they would have preferred the first meditations to be longer, while others wanted shorter meditations at the beginning due to their limited experience with mindfulness or limited attention span. Other participants said they would have liked the length of meditations to be more consistent.
Ideas for modifications.

Discussion
The present open-label mixed-methods pilot study was conducted to assess the acceptability, usability, and credibility of a DTx MBI program for pediatric concussion in acute and persisting symptoms cohorts. Overall, the response to the MBI program and the DTx platform was predominantly positive. Technical issues experienced by participants, negative attributes revealed by the qualitative interview, or ideas for modifications provided by the participants informed modifications to the user interface, instructions, intervention and ways to increase adherence to the intervention.
Across cohorts, the DTx MBI was considered satisfactory and usable, and treatment was perceived as credible. From the qualitative data, 12 positive attributes of the DTx MBI emerged, most of which were common to the two cohorts. An important aspect of this targeted DTx MBI intervention for concussion is the potential to bring a novel and innovative preventive strategy for reducing persisting symptoms risk into the homes of all concussed youth. DTx are particularly well-suited for youth who are regular users of technology. In Canada in 2018, 97.9% of Internet users aged 15–24 years owned a smartphone. 46 In the United Kingdom in 2020, 91% of 12–15-year-olds owned a smartphone. 47 Similarly, in the United States, 53% of children have a smartphone by age 11 and 89% by age 16. 48 DTx allows increased access to evidence-based interventions for adolescents by overcoming geographical barriers to intervention delivery, reducing face-to-face discomfort or social pressure and being easily accessible at any time. In the present study, participants highlighted the accessibility of the DTx MBI and the fact that it was not in person as a positive attribute. This is in line with pilot and feasibility trials that investigated the acceptability of mobile-based interventions for youth.30–32
A limitation of prior digital technologies may be the lack of a therapeutic relationship or working alliance. In the current study, participants highlighted the importance of liking the mindfulness guides in their adherence to the MBI program. Participants across cohorts rated the working alliance as good (78.4%). The coaching system also played a role in supporting the participants in their journey as stated by both cohorts. Participants liked that they had a real person checking in weekly to see how they were doing and if they were still doing the intervention. The coaching system must be leveraged in future endeavors to increase accountability and adherence to the MBI program.
While the present study did not evaluate the clinical effectiveness of the targeted DTx MBI program for concussed youth, participants reported having learned different skills through their 4-week journey, that they were now using or planning to use in real-life situations. Participants deemed the intervention credible, and most participants expected the intervention to be helpful. Previous studies suggested that higher credibility and expectancy may exert an indirect effect on symptomatic outcomes in different populations and psychotherapies.49–53 Here, participants from both cohorts subjectively reported the DTx MBI helped them with emotional management, stress management and reduction, and calming down, which can have an impact on concussion recovery. When asked about what they liked the most in the intervention, participants identified different features or skills. This interindividual variability highlights the benefit of having a variety of features and a balance of psychoeducation lessons, meditations, journaling, and other activities, which is typical for MBI curriculums.
Most participants expressed that the DTx was easy to use; however, some had problems navigating the app. Participants provided suggestions to improve the navigation, including reducing the click path and changing the display of meditations on the main screen: these modifications were implemented. Moreover, because participants identified technical issues as a barrier to using the DTx MBI, all technical issues experienced by the participants were fixed, which we expect will quantitatively and qualitatively increase its usability. This also highlights the importance of the coaching system to provide support and troubleshooting in a timely manner for unexpected technical issues. To increase accessibility for patients experiencing post-concussion symptoms such as headaches, sensitivity to light and sounds, and dizziness; the lights and sounds that were bothering the study participants were removed.
Beyond the modifications to the DTx MBI, we made modifications to the coaching scripts. Indeed, some of the suggested modifications provided by the participants are already available in the DTx MBI, including more ambiance sounds, push notifications and a tutorial. We will ensure that it is mentioned to the participants that these options exist and where to find them during the orientation session. Moreover, some participants wanted more activities or to continue with the MBI beyond 4 weeks. As part of the pilot study, only 4 modules were available to the participants, but the full intervention includes 8 modules.
Some suggestions for modifications could not be implemented and some negative attributes could not be fixed due to feasibility and personal preference (e.g., some guides are ‘boring’, length of meditations, incorporate daily goals, add more structure and add prompts for journaling). One participant did not think the DTx MBI program was supporting what they needed and requested a multidisciplinary intervention including oculomotor rehabilitation, which was outside of the scope of the MBI program.
Importantly, this mixed-methods pilot included two cohorts of concussed youth at different stages of injury. Most subthemes revealed by the qualitative data were similar across cohorts. Yet, the needs of these two cohorts may have been entirely different, as one has suffered from symptoms for weeks or months, while the other was acutely injured. The difference is highlighted by the subtheme ‘No expectations to get better’ that was reported by the persisting symptoms cohort and not by the acute cohort. Indeed, the goal of the MBI is not to cure or heal the concussion, but rather to provide participants with tools and skills to better cope with their symptoms, which can ultimately help reduce the symptom burden and promote recovery. Experiencing persisting symptoms may have deleterious effects on school, work, social and sports activities, and reduce the quality of life. 5 As such, these patients may try different interventions that are time and financially expensive. Developing evidence-based interventions that are widely accessible, easy to use and user-centered is critical.
A potential limitation of this study is the inclusion of two different cohorts. Recruitment approaches and participant compensation differed between the acute and persisting symptoms cohorts. We aimed to ensure fair compensation for participants’ time and involvement in the study while adhering to the guidelines and requirements set by the respective institutions involved. Although the disparity in compensation may have impacted the retention rates, other factors, such as distinct symptom profiles between the two groups, may have played a role. Notably, individuals with persisting symptoms after a concussion often exhibit elevated rates of depression and anxiety symptoms, 54 which can contribute to reduced motivation and challenges in completing an intervention. Moreover, the differences in recruitment, compensation and symptom profiles could potentially introduce variations in participants’ perceptions of the intervention. By examining and comparing the acceptability and usability of the DTx in the two distinct cohorts, we aimed to gain insights into whether the intervention's features and content adequately addressed the unique needs faced by each group. This approach allowed us to explore the potential differences in their perceptions of the DTx MBI. During the iterative analysis of the qualitative data, we observed a considerable overlap in the themes and experiences of both groups. Importantly, subsequent feasibility trials will investigate factors involved in retention and adherence and will be conducted separately because the goals of the studies will ultimately be different (prevention strategy versus treatment option).
This study did not assess the clinical effectiveness of the MBI program in promoting recovery and preventing persisting symptoms in youth with a concussion. However, with the adaptations mentioned in this study, we are conducting a randomized control trial to thoroughly evaluate the clinical, somatic, emotional, cognitive and neurophysiological recovery effects of MBI training in concussed youth. 55 Our targeted DTx MBI program for concussion may engage youth who typically would not seek help through traditional intervention routes.
The present mixed-methods study and the iterative approach to intervention design we are using will ensure better translation and impact of interventions for youth with concussions. By including the perspectives of patients in the DTx design and development process, we ensure that the DTx is user-centered, relevant to their needs, and with their limitations/symptoms in mind.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241248296 - Supplemental material for Acceptability, usability, and credibility of a mindfulness-based digital therapeutic for pediatric concussion: A mixed-method study
Supplemental material, sj-docx-1-dhj-10.1177_20552076241248296 for Acceptability, usability, and credibility of a mindfulness-based digital therapeutic for pediatric concussion: A mixed-method study by Veronik Sicard, Kiarah O’Kane, Olivier Brown, Lauren Butterfield, Rachel Kardish, Esther Choi, Katherine Healey, Noah Silverberg, Andra M Smith, Gary Goldfield, Bechara J Saab, Clare Gray, Kristian Goulet, Peter Anderson, Craig Mackie, Sonja Roth, Martin Osmond, Roger Zemek, Molly Cairncross and Andrée-Anne Ledoux in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors thank the Emergency Room research assistant volunteers who initially approached participants to gauge interest in the study.
Contributorship
VS was involved in formal analysis, writing of original draft, and review and editing, and visualization. KO was involved in data collection and writing of original draft. OB, LB, RK, EC and AAL were involved in data collection. KH and AAL were involved in data curation and project administration. NS, AMS, GG, CG, KG, PA, MO and AAL were involved in conceptualization and writing, reviewing and editing. BS was involved in software. GG, CM, SR, AAL and MC were involved in the development of the mindfulness-based intervention. AAL and MC were involved in conceptualization, methodology, formal analysis, resources, supervision and writing, reviewing and editing. AAL and RZ were involved in funding acquisition. All authors have approved this manuscript as submitted.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AAL reported being one of the authors of the Mindfulness-Based Intervention for Concussion protocol used in this study, she did not receive any financial benefit. AAL received funding from the Ontario Brain Institute NERD program for a separate component of the study. AAL has no other conflict of interest to disclose. BJS is the Chief Scientist and CEO of Mobio Interactive PTE LTD (Singapore), the parent company of Mobio Interactive Inc. (Toronto, Canada), and he owned approximately 22% of the company at the time of manuscript submission. BJS exclusively served as a technical liaison for the study and did not contribute to the specific study design, or select the outcome measures, nor did he directly contribute to, or have influence over, data collection or analysis. RZ is the cofounder, Scientific Director, and a minority shareholder in 360 Concussion Care, an interdisciplinary concussion clinic. RZ holds a Clinical Research Chair in Pediatric Concussion from University of Ottawa, and is on the concussion advisory board for Parachute Canada (a non-profit injury prevention charity). VS receives royalties for the publication of a book on concussion by Flammarion. The remaining authors have no conflicts of interest to report.
Ethical approval
The study was approved by the Research Ethics Board at CHEO Research Institute (project # 20/72X) and the University of British Columbia (project # H20–00120-A008).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: internal grants from the Alternative Funding Plan for the Academic Health Sciences Centres of Ontario (CHAMO)'s Innovation Fund (PI: AAL and RZ), the CHEO Research Institute Research Growth Award (PI: AAL), the University of Ottawa Brain and Mind Research Institute Team Grant (PI: AAL), and Canadian Institutes of Health postdoctoral fellowship (VS).
Guarantor
Dr Veronik Sicard, PhD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.