
Abstract
Background
Due to the accessibility barriers of in-person programs for active aging, the development of programs that use innovative technologies is needed. Video games can be an engaging tool for disseminating active aging interventions.
Objective
The objective of this pilot study was to analyze the feasibility of a cognitive–behavioral intervention to promote active aging administered through a video game.
Methods
Fifty-five participants (63.6% women, mean age = 53.0 years) were randomly assigned to a cognitive–behavioral intervention to promote active aging administered through an interactive multimedia online video game with a complementary app (CBI-V; n = 29) or to a control group that received nonspecific online information (CG; n = 26).
Results
Only 3.6% of the participants dropped out of the study (6.9% in CBI-V and 0.0% in CG; without significant differences between groups). The mean number of modules completed was 7.6 (SD = 0.9) out of 8 in the CBI-V and 7.9 (SD = 0.5) in the control group (CG), without significant between-group differences. In the CBI-V, the mean total time dedicated to the game was 516.8 min (SD = 94.3), including 143.2 min (SD = 31.6) of cognitive training tasks, and the mean of completed tasks was 206.2 (SD = 33.7) out of 259. Participants were highly engaged (M = 39.9, SD = 8.6) and satisfied (M = 25.8, SD = 4.5) with the intervention. After the intervention, the CBI-V group significantly improved on SF-36 dimensions of General Health (p = .0386), Vitality (p = .0283), Social Functioning (p = .0130), and Physical Summary Index (p = .0370) compared to the CG, with medium effect sizes (d = 0.56–0.75).
Conclusions
The results demonstrate the feasibility of the video game intervention to promote active aging and encourage conducting a large-scale randomized controlled trial.
Introduction
Europe is experiencing an unprecedented aging of the population, which will continue to increase in the coming decades. According to the European Statistical Office, half of the European population is 45 years old or older, and 21.1% is 65 years old or older 1 ; and it is estimated that this latter segment of the population will increase from 94.3 million in 2022 to 136.1 million by 2100. 2
The increase in life expectancy linked to the previously mentioned data on population aging is one of humanity's greatest triumphs. However, it also represents a great challenge for society and the health system because aging is associated with a higher prevalence of health problems, especially in noncommunicable diseases, 3 depression, and dementias. 4 Furthermore, even in healthy adults, aging is associated with changes in the brain that may affect some cognitive functions. Thus, brain volume has been found to decrease with age, especially in the frontal and temporal cortex and in the putamen, thalamus, and accumbens, with annual reductions of 0.5% to 1.0%. 5 Reductions have also been found in the gray and white matter, caudate, cerebellum, hippocampus, and association cortices, and the length of myelinated axons was reduced by as much as nearly 50%.5–7 Therefore, a progressive deterioration of certain cognitive abilities takes place, including memory, executive functions, reasoning, and information processing.5,6,8 These changes do not occur in a linear fashion but rather follow an inverted U trajectory throughout the lifecycle, with brain volume increasing until young adulthood, plateauing in middle adulthood, and declining as we age, with approximately age 45 (between 40 and 50 years) being the turning point in this trend. 5
However, it is possible to compensate for age-related brain deterioration, thanks to neuroplasticity. Neuroplasticity refers to the nervous system's capacity to change in response to extrinsic or intrinsic stimuli by reorganizing its structures, functions, or connections. 9 Thus, it has been found that people who stimulate their brains throughout their lives have better cognitive outcomes as they age. 10 Furthermore, early interventions to promote active aging can reduce the proportion of older people who fall below the dependency threshold. 11 For all these reasons, the World Health Organization (WHO) 11 has highlighted the need for programs that promote active aging.
One way to make these interventions accessible to the population is through video games. These modes of intervention delivery can overcome the barriers of in-person programs (e.g., schedule incompatibility, travel difficulties, and stigmatization), are fun and engaging, and can be used at home when most convenient. 12
A meta-analysis that included 21 randomized controlled trials of video game-based interventions found that they produced positive effects on physical health, and improved affective status and social health, with small effect sizes (d = 0.34, d = 0.26, and d = 0.40, respectively). 13 More recent studies have found significant differences, when compared to a control group (CG), in cognitive skills such as driving, inhibition tasks, processing speed, 14 inhibition, and working memory. 15 In contrast, one study 16 found an improvement in gait among the CG and a significant deterioration in list recognition among the experimental group. However, various theoretical, methodological, and design limitations of the included studies could restrict the scope of these results. Firstly, these studies included only adults older than 60 years, which may limit the preventive effect of the intervention. In addition, the majority did not base their interventions on a theoretical model, did not use a manualized treatment, and used non-standardized measures. The studies that utilized serious video games (i.e., those aimed at promoting behavioral changes with an educational or health purpose) were focused on cognitive training and did not consider physical and emotional health or healthy lifestyle habits. Likewise, none of these studies used a graphic adventure (i.e., a video game with a narrative thread where the protagonist interacts with the environment and other characters), even though older people tend to prefer this type of video game. 17 Some studies had dropout rates of up to 25%, despite the lack of adherence to cognitive–behavioral interventions limiting their effectiveness. 18 Finally, none of these studies combined the video game with a complementary mobile app, which could enhance generalization of skills learned in the game to real life. An intervention for subjects including those under 60 years of age based on a serious graphic adventure video game that includes strategies to improve mood, healthy lifestyle habits, and cognitive training, with a complementary app, could help promote active aging.
The main objective of this pilot study was to analyze the feasibility and acceptability of a cognitive–behavioral intervention to promote active aging administered through an interactive multimedia online video game in a graphic adventure genre with a complementary app compared to a CG. Participants in the intervention group were expected to show high acceptability, adherence, engagement, satisfaction with the intervention, and improvement in their perceived health compared to the CG.
Methods
Design
A pilot study with a parallel design was conducted in preparation for a large-scale randomized controlled trial 19 (registration number in Clinical Trials: NCT04982497; https://clinicaltrials.gov/ct2/show/NCT04982497). This pilot study consisted of a pre–post design with two groups. Participants were randomly assigned to one of the two study groups (see Figure 1): (1) a cognitive–behavioral intervention via interactive multimedia online video game with a complementary app (CBI-V) or (2) a control group that received online information about active aging (CG). The randomization sequence was automatically generated by the evaluation platform itself (blinding of randomization). Participants were assessed at baseline and post-intervention. Primary outcomes were dropouts, session attendance, inter-module homework, engagement, and satisfaction with the intervention. The secondary outcome was perceived health status.

Flowchart of study participants.
Participants
Participants were recruited from five socio-community associations and a senior university program in Galicia, a region in northwestern Spain with 2 730 337 residents. The inclusion criteria were as follows: (a) 45 years of age or older; (b) reside in the Autonomous Community of Galicia; (c) normal cognitive functioning, as determined by a cutoff point of 24 on the Mini Mental State Examination (MMSE 20 ; Spanish version by Lobo et al. 21 ); and (d) access to a smartphone or computer with an internet connection. The exclusion criteria were as follows: (a) serious medical or mental disorders (e.g., major depression, schizophrenia, bipolar disorder, dementia, dissociative disorders, substance dependence, or acute suicidal ideation); (b) had been receiving psychological or psychopharmacological treatment in the 2 months prior to the study or were participating in another study related to active aging; and (c) could not communicate in Spanish or had difficulties (e.g., sensory and physical) that made it impossible to play the video game.
The following retention strategies were used to minimize the loss of participants during the recruitment and intervention process: excluding those likely to be lost (based on the inclusion/exclusion criteria); treating participants with kindness, affection, and respect; conducting noninvasive, helpful, and engaging assessments; and encouraging participants to continue with the trial. 22
Of the 66 people assessed for eligibility, two (3.0%) did not meet eligibility criteria due to not having access to a smartphone or computer with an internet connection, and nine (14.0%) declined to participate in the study due to work, family, or time constraints. The final sample consisted of 55 participants who were randomized to the two study conditions: 29 subjects to the CBI-V and 26 to the CG.
Written informed consent was obtained from all participants. The study was conducted in accordance with the latest version of the Declaration of Helsinki, and the approval of the Bioethics Committee of the University of Santiago de Compostela was obtained (code number USC-38/2021). In addition, this study follows ICMJE Recommendations for the Protection of Research Participants and the ICMJE Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals. Lastly, participation was completely voluntary, and there was no financial aid or other incentives.
Instruments
In-person (by an independent interviewer) and online assessments were carried out at the pre-intervention measurement and online at the post-intervention measurement. Cognitive function was assessed with the MMSE 20 (Spanish version by Lobo et al. 21 ), with a sensitivity of 89.8% and a specificity of 75.1%.
Sociodemographic characteristics were assessed by a questionnaire prepared ad hoc for this study. To analyze the feasibility and acceptability of the intervention, study dropouts, adherence to treatment, engagement, and satisfaction with the intervention were considered. A record of dropouts was kept. To assess treatment adherence, the number of modules completed, time played, and time dedicated to cognitive training tasks, the number of attempts to solve the tasks, and the number of tasks between modules completed were recorded automatically by the online video game and the app in the intervention group; the number of modules completed was recorded in the CG. The User Engagement Scale-Short Form (UES-SF) 23 was used to determine engagement with the video game. This is a measure that yields a global score and four subscales (Focused Attention, Perceived Usefulness, Aesthetic Attractiveness, and Reward, with internal consistency of 0.82, 0.86, 0.84, and 0.81, respectively). The Client Satisfaction Questionnaire (CSQ-8 24 ; Spanish version of Vázquez et al. 25 ), with an internal consistency of 0.80, was used to assess satisfaction with the intervention.
The Short-Form Health Survey (SF-36) 26 was used to measure the effect of the intervention on perceived health of the participants. This instrument has eight subscales (General Health, Body Pain, Physical Function, Physical Role, Vitality, Social Function, Emotional Role, and Mental Health) and two summary indices (Physical and Mental), whose internal consistencies range between 0.81 and 0.97.
Interventions
Cognitive–behavioral intervention via interactive multimedia online video game with complementary smartphone app (CBI-V)
The intervention group received a cognitive–behavioral program to promote active aging, administered through an interactive multimedia online video game (called GAMAPEA) with a complementary smartphone app. The intervention was designed to be administered in eight modules, requiring approximately 60 min per module, at a rate of one per week, with tasks assigned between modules to practice the skills taught in the video game in the participants’ real lives. The intervention focused on three main areas: prevention of depression, healthy lifestyle habits, and cognitive training. The components of the intervention aimed at depression prevention were developed from Lewinsohn et al.'s multifactorial etiopathogenic model. 27 The components include techniques such as mood monitoring; techniques for control of psychophysiological arousal, behavioral activation, and self-reinforcement; and techniques to increase positive thoughts. The components of the program which focused on healthy lifestyle habits were based on the learning theory and social cognitive theory model28,29 and included techniques such as psychoeducation, modeling, self-reinforcement, self-observation, goal setting, development of a plan for change, identification of barriers/problem solving, and feedback. Finally, the components related to cognitive training were based on the notions of cognitive reserve 30 and neuroplasticity 31 to improve performance through online mental games and reduce the causes of memory deficits associated with aging 32 (e.g., decreased processing resources, semantic encoding deficits, and difficulties in deliberate retrieval of information). Games were developed to stimulate attention, memory, language, and executive functions (e.g., planning, decision-making, flexibility, and attention control), as well as learning and practicing strategies for encoding information to be remembered (e.g., acronyms and grouping), stored (e.g., repetition), and retrieved (e.g., external aids) (see Images in the Supplementary materials).
The techniques used in this intervention to prevent depression have demonstrated efficacy in previous short- and long-term randomized controlled trials that tested different formats of administration: face-to-face,33,34 telephone conference calls,35,36 and a smartphone app. 37 In addition, the research team piloted all techniques (i.e., prevention of depression, healthy lifestyle habits, and cognitive training) in a video game format in 25 participants and found significant improvement in perceived general health, physical functioning, social functioning, and mental health. 38
The video game is a graphic adventure based on the “French Way” of the Way of Saint James (from Roncesvalles to Santiago de Compostela) that focuses on a main character (Jacobo) with whom the participants can identify. It integrates the player into a narrative from which interactions with characters, elements of the environment, and puzzles emerge, with the aim of acquiring psychological tools and training the cognitive capacity.
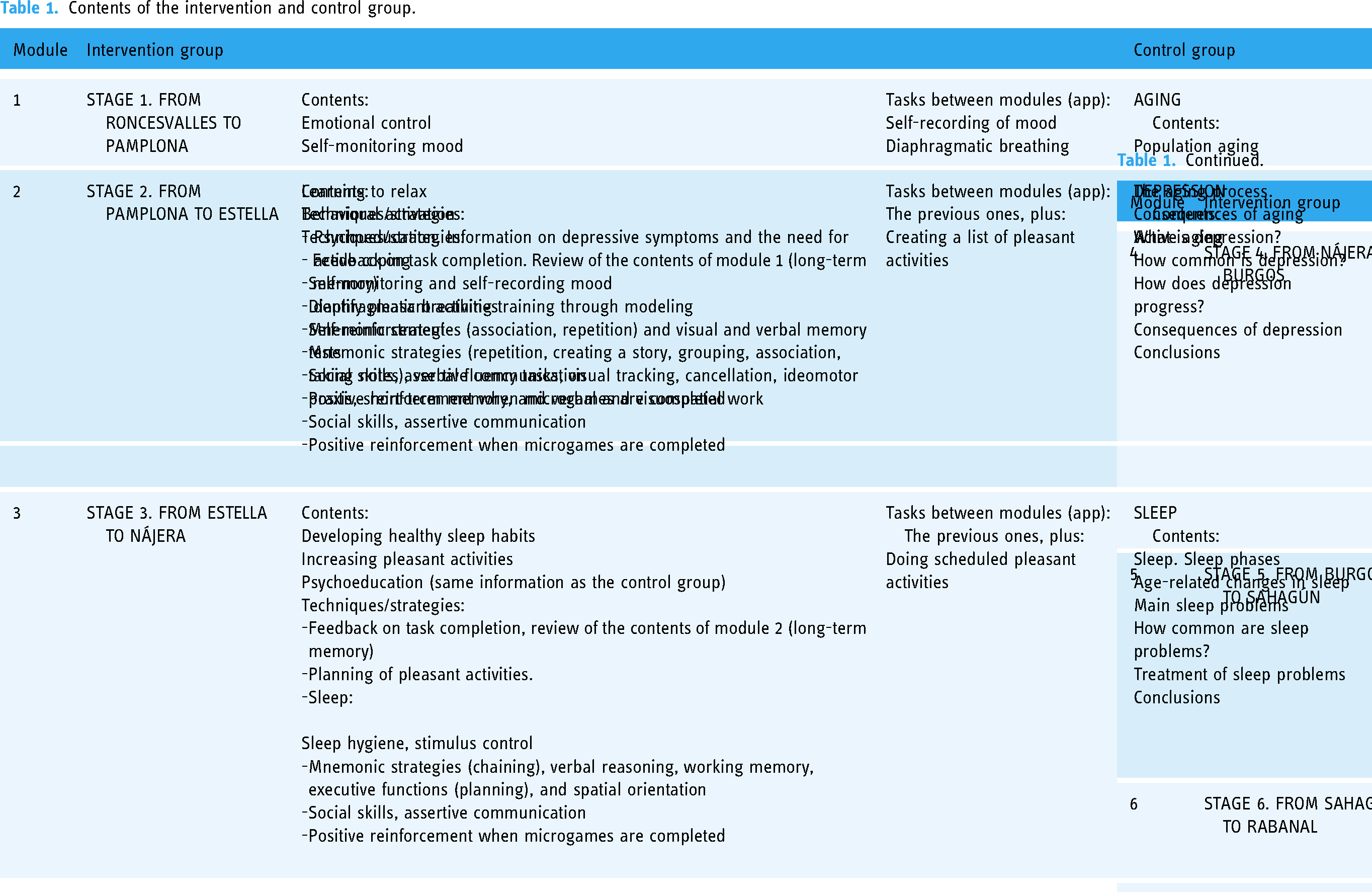
Specifically, as Table 1 shows, the first module presents information on depressive symptoms and the need for active coping, starting with self-observation and mood monitoring, along with training in deep diaphragmatic breathing. The second and third modules focus on behavioral activation, including strategies such as monitoring, structuring, and planning of pleasant activities. The third through the fifth modules introduce psychoeducation on healthy lifestyle habits (sleep, physical activity, and diet), as well as strategies to develop healthy habits (e.g., behavior record and stimulus control techniques). In the sixth and seventh modules, participants are trained to identify negative thoughts and to replace them with more rational and positive ones. The eighth module addresses building self-esteem and reviews what has been learned and maintenance of progress. Cognitive training and training in social skills are transversal contents throughout all the modules of the video game.
Contents of the intervention and control group.
The complementary app was synchronized with progress on the video game and allowed the user to review what was learned during video game play and the stages along the route of the Way of Saint James, record tasks between modules, send real-time reminders (notifications), and review progress.
To access the online video game in their homes, participants were first contacted by the research team to welcome them to the program, give them instructions for access, and provide them with the download link and individual access code for the game and the app; they were also given means to contact the research team (by phone and email) in case they needed technical assistance. The initial contact by the research team was by telephone; an email was also sent to them with the written information and the download link for the video game, and the download link for the app was also sent via WhatsApp. Each week throughout the intervention, a therapist (previously trained through a theoretical and practical seminar that lasted approximately 8 h) monitored the progress of all participants using an online platform specifically designed for this study. The therapist made a personal phone call to participants who did not progress at the expected rate of one module per week to check in on them, ask about the reasons for the lack of progress on the video game, help if needed, and encourage them to continue with the intervention.
Control group
The role of the CG was to control for contextual and nonspecific factors (e.g., participating in a study, receiving care, using a technological device, and the effect of time). The CG was matched to the CBI-V group in the administration format (online), the number of modules (eight), the frequency of module administration (once weekly), the duration of each module (reading for approximately 60 min), and the psychoeducational contents. Participants in this condition had access to nonspecific general information on general aspects of active aging, without proposing specific strategies for change. Specifically, the first module addressed issues related to aging, the second module addressed depression, the third to fifth modules examined healthy lifestyles (sleep, physical exercise, and balanced nutrition), the sixth module addressed negative thoughts, the seventh module dealt with cognitive processes, and the eighth module discussed social relations (Table 1).
Data analysis
SPSS Statistics (version 22.0) and the Package Statistical Analysis System (SAS) were used for the data analysis. Values that were missing due to attrition (i.e., data referring to the two participants who dropped out of the study) were imputed using multiple imputation procedure, PROC MI, and then summarized according to Rubin's method. 39
Frequency analysis and descriptive statistics were conducted to describe dropouts, the number of modules completed, time spent interacting with the video game (including time played, time dedicated to cognitive training tasks and the number of attempts to solve the tasks), tasks between modules completed, engagement, and satisfaction with the intervention. To assess the difference between the two groups with respect to dropouts and completed modules, Fisher's F test and the Mann–Whitney U test were performed, respectively. To evaluate differences between the two groups in perceived health (each of the subscales and the summary indices of the SF-36), the Mann–Whitney U test was performed. Wilcoxon test was used to examine pre- and post-intervention measurement points. Effect sizes were calculated using Cohen's d (d ≥ 0.20 as small, d ≥ 0.50 medium, and d ≥ 0.80 large). 40
Results
Sample characteristics
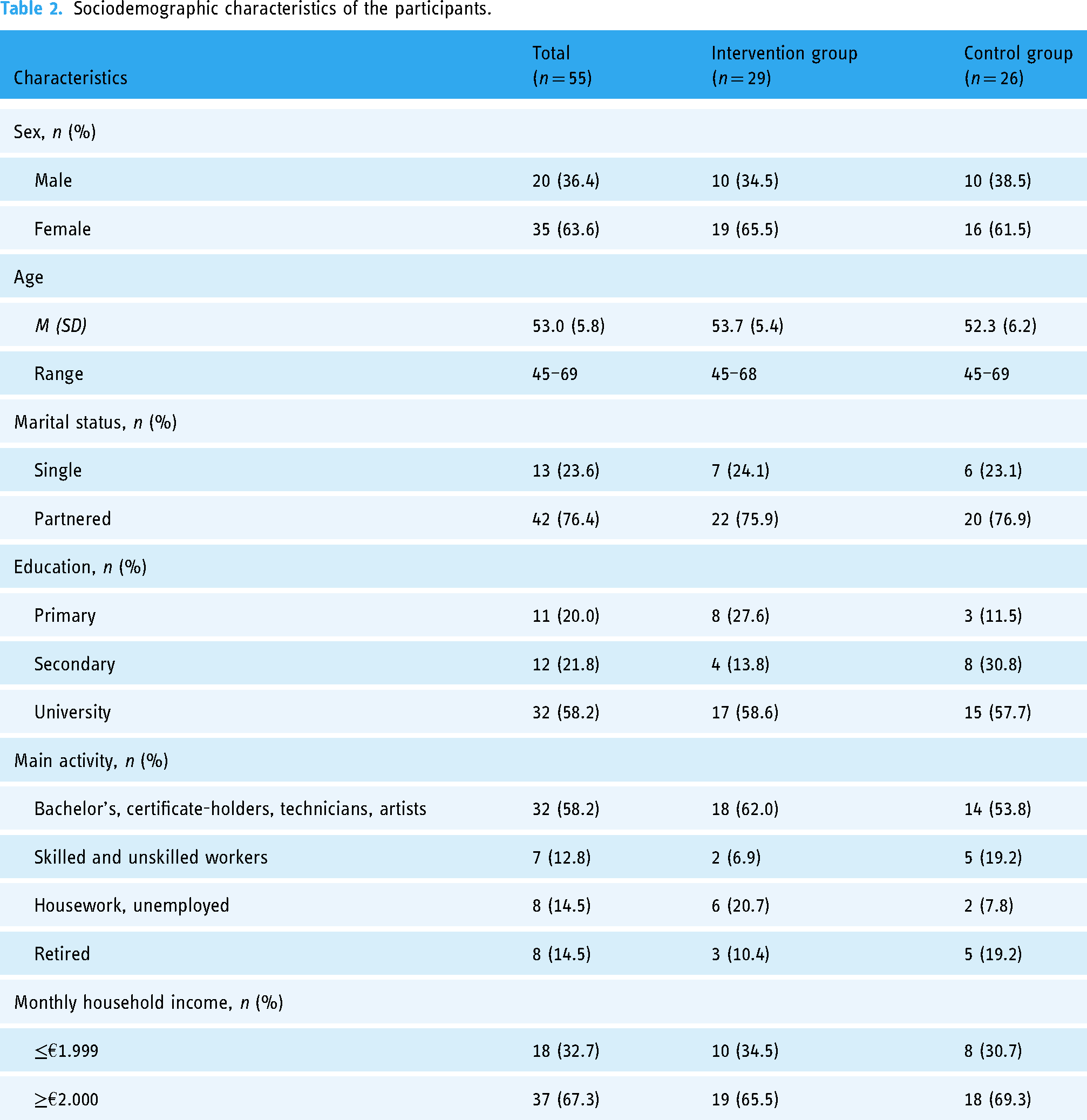
Women accounted for 63.6% of participants. The sample had a mean age of 53.0 years (SD = 5.8). Among the participants; 76.4% had a partner; 58.2% had reached the university level in their education; 58.2% were actively employed in jobs requiring a bachelor's degree, certificate, and technical certificate and/or as artists; and 67.3% reported a monthly family income equal to or greater than €2000 (Table 2). No significant differences were found between the intervention group and CG for any of the sociodemographic characteristics.
Sociodemographic characteristics of the participants.
Feasibility and acceptability of the intervention
Dropouts
Only 3.6% of the participants dropped out of the study; two (6.9%) from the intervention group and none (0.0%) from the CG, with no significant differences between the two groups (p = .492). The reasons given for the dropouts were family problems.
Adherence
The mean number of modules completed in the intervention group was 7.6 (SD = 0.9) out of 8, while in the CG, it was 7.9 (SD = 0.5), without significant differences between the two groups: U = 322.00, Z = −1.379, and p = .168. In the intervention group, the mean time dedicated to each module was 64.6 min (SD = 24.4) and the total game time was 516.8 min (i.e., 8 h 37 min; SD = 94.3). Within that time, a mean of 18.0 min (SD = 3.9) per module was dedicated to practicing cognitive tasks, with a total video game mean time of 143.2 min (i.e., 2 h, 23 min, 20 s; SD = 31.6) spent in cognitive training tasks. Specifically, the mean time dedicated to the stimulation of attention was 20.2 min (SD = 1.5; 14.1% of the total time for cognitive training); the stimulation of memory was 52.1 min (SD = 4.0; 36.4% of the time for cognitive training); the stimulation of language was 17.8 min (SD = 0.9; 12.4% of the cognitive training time); and the executive function was 53.1 min (SD = 3.4; 37.1% of the cognitive training time). There was a mean of 5.4 (SD = 3.4) attempts to solve each cognitive task per module and a total video game mean of 21.4 (SD = 13.7) attempts. In addition, an average of 206.2 (SD = 33.7) tasks were completed between modules, out of the total of 259 assigned throughout the intervention.
Engagement with the intervention
The participants were immersed in the experience of an intervention that used a video game with a complementary app, achieving an average score on the UES-SF of 39.9 (SD = 8.6) out of a maximum of 48. The mean scores were as follows: Focused Attention = 8.7 (SD = 2.3), Perceived Utility = 7.2 (SD = 0.6), Aesthetic Appeal = 8.6 (SD = 2.6), and Reward = 9.3 (SD = 2.5), out of a maximum of 12 on each subscale.
Satisfaction with the intervention
The degree of satisfaction with the intervention was high, with a mean score on the CSQ-8 of 25.8 (SD = 4.5) out of a total of 32.
Effects of the intervention on perceived health
Pre–post study differences
In the CBI-V group, there were significant improvements between pre- and post-intervention perceived health (SF-36) dimensions of: General Health (d = 0.62), Physical Functioning (d = 0.44), Vitality (d = 0.50), Social Functioning (d = 0.54), and Mental Health (d = 0.80) (see Table 3). In the CG, in contrast, there was significant worsening in the dimensions of Body Pain (d = −0.45), Physical Role (d = −0.71), Vitality (d = −0.41), and Social Functioning (d = −0.66) (Table 3). There were no significant changes in the other dimensions.
Between-group and within-group effects on perceived health.

Note. Only significant results.
From multiple imputation (Wilcoxon rank sum test or Mann–Whitney U test).
Differences between groups
There were no between-group significant differences in perceived health at the pre-intervention time point (see Table 3). After completion of the intervention, the participants in the CBI-V group achieved significantly better scores than those in the CG on the dimensions of General Health (d = 0.63), Vitality (d = 0.75), Social Functioning (d = 0.71), and Physical Summary Index (d = 0.56). There were no significant differences in the rest of the dimensions of the SF-36.
Discussion
The results of this pilot study support the feasibility of a cognitive–behavioral intervention designed to promote active aging administered through an interactive multimedia online video game with a complementary smartphone app.
Regarding feasibility, only 3.6% of the participants dropped out of the study, much lower than the dropout rates found in other active aging promotion programs, both those administered in person 41 and those administered through video games, 42 which found dropout rates of up to 58.2% and 26.7%, respectively. In addition, adherence to the intervention was high, with an average of 7.6 modules completed out of the 8 that the intervention included, an average time spent of 8 h and 37 min (including 2 h and 23 min of cognitive training tasks), and an average of 206.2 tasks between modules completed, out of the 259 assigned. Finally, the participants immersed themselves in the experience of the intervention, finding it useful, appealing, and reinforcing, and they felt highly satisfied with it, consistent with the only previous study that evaluated satisfaction. 43 All this supports the feasibility of the intervention. These findings may be due to several factors. First, this intervention format allows the participants’ flexibility to do the intervention activities in the place and at the time most convenient to them, without the need to travel, which could facilitate access to the intervention. Second, the complementary app, which sent participants reminders of tasks between modules and provided feedback on them, encouraged adherence to the intervention. Third, the gamification of the intervention makes it more innovative and appealing for the participants, increasing their motivation and satisfaction with it. 44 Fourth, in the different modules that make up the video game, special importance has been given to grading the difficulty of the challenges that the player must overcome and reinforcing progress. Lastly, the type of video game, one with a meaningful storyline, is usually preferred by older adults over other video games that require very fast and precise movements and include an element of time challenge. 17 The setting, Camino de Santiago, encourages participants to identify with significant cultural, geographical, and historical elements, contributing to the player's immersion in the experience and enhancing meaningful learning. 45
In relation to the effect of the intervention, a significant improvement in perceived health was found in the intervention group between the pre- and post-intervention time points on General Health, Physical Functioning, Vitality, Social Functioning, and Mental Health and a significant decline in the CG on Physical Pain, Physical Role, Vitality, and Social Functioning. At the post-intervention time point, participants in the intervention group significantly improved in General Health, Vitality, Social Functioning, and the Physical Summary Index compared to the CG, with medium effect sizes (d = 0.56–0.75). These results are better than those found by Kahlbaugh et al., 46 who did not find significant improvements in the SF-36 subscales after a similar intervention. However, they are like those of Karahan et al., 47 who found improvements on several SF-36 subscales. One possible explanation for these promising findings is that because it is a multicomponent intervention aimed at preventing depression, implementing healthy lifestyle habits, and providing cognitive training, it allows for improvements in both physical and mental health. This type of intervention is consistent with holistic approaches to health promotion to support active aging. 48
This study has important implications for clinical practice and research. The present study reinforces the importance of designing and administering cognitive–behavioral programs that promote active aging through video games. Given the growth of the aging population, its use could save significant personal, health, social, and economic costs. Moreover, it raises the possibility of starting interventions to promote active aging in middle age, which would be consistent with the recommendations of the WHO 11 ; that is, these interventions should be conducted throughout the life course, not just starting in older age. Administration through a video game makes it possible to increase the accessibility and attractiveness of the intervention, thereby reducing healthcare pressure and waiting lists. The use of this format is possible in this age group because 42.3% of internet users are 45 years old or older 49 and 77% of people 50 years or older have a smartphone. 50 Lastly, this study provides useful information for planning future controlled trials (e.g., sample size calculation and completeness of the study protocol).
However, the current study also has some limitations. Given the size of the sample, the results should be interpreted with caution. In this pilot study, cognitive functioning was only screened, a future randomized controlled trial could incorporate a fuller assessment of cognitive functioning (especially memory) to better understand the cognitive profile and difficulties of participants. Furthermore, because there was no long-term follow-up, it is unknown whether the effects of the intervention were maintained over time. Future studies with larger samples and extensive follow-ups are needed to corroborate these results. Additionally, the findings in the current study could be inflated due to the Hawthorne effect. However, this potential effect was minimized by the completion of study activities in a natural setting (participants performed the assessment and intervention at home, without being under the direct observation by research staff). Moreover, any possible Hawthorne effect would likely influence both groups to an equivalent extent because the CG was matched to the intervention group. Future studies could identify the mechanisms of change.
Conclusion
The results demonstrate the feasibility and acceptability of the cognitive–behavioral intervention administered through an interactive multimedia online video game with a complementary app to promote active aging. Thus, these positive findings encourage conducting a large-scale randomized controlled trial.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241233139 - Supplemental material for A randomized controlled pilot study of a cognitive–behavioral video game intervention for the promotion of active aging
Supplemental material, sj-docx-1-dhj-10.1177_20552076241233139 for A randomized controlled pilot study of a cognitive–behavioral video game intervention for the promotion of active aging by Patricia Otero, Tania Cotardo, Vanessa Blanco, Ángela J. Torres, Miguel A. Simón, Ana M. Bueno and Fernando L. Vázquez in DIGITAL HEALTH
Footnotes
Acknowledgments
We appreciate the collaboration of Imatia Innovation and Sivsa Soluciones Informáticas, as well as the spin-off of the University of Santiago de Compostela “Xuntos. Psychological and Psychiatric Care”. We also wish to thank to Red Cross (Coruña), AGADEA, GaiásTech, Network of Centers for Modernization and Technological Inclusion (Aulas CeMIT), Canal Sénior, and the Fourth Cycle of the University of Santiago de Compostela.
Author contributions
FLV conceived the study and developed the protocol. PO and FLV gained ethical approval. PO and TC recruited participants. PO, TC, and FLV completed the data analysis. PO and FLV wrote the first draft of the manuscript, and TC provided assistance. TC, VB, AJT, MAS, and AMB revised critically the draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Bioethics Committee of the University of Santiago de Compostela approved this study (code number USC-38/2021).
Funding
This research has been funded by the State Research Agency of the Ministry of Science and Innovation of Spain through Project PID2019–105052RB-I00 (AEI/10.13039/501100011033).
Guarantor
FLV
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.