
Abstract
Objectives
The objective of this study was to analyze factors of regional variation in national cancer screening rate in Korea using regional cancer screening rate data. In addition, during the COVID-19 pandemic in 2020, we tried to identify factors affecting cancer screening rate, including COVID-19 situation in the region.
Methods
Data provided by the National Health Insurance Service Center were used for the national cancer screening rate index data in 2020 in 229 regions. A correlation analysis was conducted to find correlation between national cancer screening rate and variation factors in the national cancer screening rate in the region to be analyzed. In addition, to confirm spatial dependence of the national cancer screening rate among regions, a global spatial autocorrelation (Global Moran's I) analysis was conducted.
Results
In the 2020 COVID-19 situation, variable factors affecting the national cancer screening rate among regions in Korea were the regional number of populations of cumulative COVID-19 confirmed cases, concern of damage caused by COVID-19 infection, income level, the proportion of the population graduating from middle school or lower, the average daily access time to general hospitals by car, and the average daily access time to hospitals and clinics by public transportation or walking.
Conclusions
Results of this study can be used to establish national digital health policies that reflect regional variation factors in situations such as the COVID-19 pandemic. It is believed that they can contribute to policies to promote community health in the future.
Introduction
Globally, medical activities such as diagnosis and treatment have significantly decreased compared to previous levels due to the direct and indirect impact of COVID-19. 1 Of 105 countries that responded to the WHO survey on health care utilization during the COVID-19 pandemic, 76% reported a decline in outpatient care rates and 66% reported providers canceling appointments. 2 The need to monitor the use of medical services for not only COVID-19 diseases, but also non-COVID-19 diseases such as cancer, heart surgery, and acute diseases whose diagnosis or service has been delayed is being raised.3–5
Cancer is a disease with high morbidity and mortality, and many countries have implemented programs for the effective management of cancer.6,7 The WHO reports that cancer deaths can be reduced to 8 million by 2040 if cancer control programs are implemented effectively. 8 Cancer prevention can be divided into primary prevention, which suppresses the occurrence of cancer, and secondary prevention, which prevents death due to cancer by detecting and treating cancer at an early stage. 9 According to recent foreign research data, cancer patients decreased during the Corona 19 pandemic in 2020.10,11 This is not because the actual number of cancer patients has decreased, but because the rate of cancer screening that detects and diagnoses cancer has decreased. During the COVID-19 pandemic in 2020, a study reported that the number of cancer screening tests performed decreased by at least 60% to a maximum of 82%, and cancer diagnosis also decreased by at least 19% to a maximum of 78%. 10 Another study has predicted that the cumulative number of deaths from breast cancer would increase by 0.52% by 2030 if breast cancer diagnosis and treatment are delayed due to a sharp decline in mammography. 11
In Korea, in order to detect and treat the most common cancers such as stomach cancer, colorectal cancer, liver cancer, breast cancer, and uterine cervix cancer at an early stage in Koreans, the country provides free health checkup services to the public. 12 In Korea, during the COVID-19 pandemic, the screening rate for free national cancer screening in 2020 decreased by 6.4%p compared to that in 2019, with screening rates for stomach, liver, colon, breast, and cervical cancers all decreased. 13 Regular cancer screening is very important for early detection of cancer. If early cancer diagnosis is delayed due to a decrease in cancer screening rate, it might have a negative impact on patient prognosis and mortality.14–17 In order to maximize the effectiveness of national cancer screening, it is necessary to find factors that cause no cancer screening and manage them. The National Health Insurance Service (NHIS) Center of Korea discloses total cancer screening rate and cancer screening rate by region in Korea. There are regional differences in national cancer screening rate in Korea.18,19 To reduce regional disparities, it is necessary to identify regional variations in national cancer screening rate. Previous studies related to cancer screening were mainly conducted through surveys targeting residents of one region or individual-level studies using secondary data.20–24 However, medical use is affected not only by individual characteristics, but also by population structure, disease structure, and socioeconomic environment of the area to which the individual belongs.18,25 Research on this is lacking. Recently, attempts to take a spatial approach are diversifying, such as using geographic information systems (GIS) for cause analysis and prevention of diseases, including cancer.25–27 Research is being conducted to reveal spatial distribution characteristics of diseases using global and local spatial autocorrelation analysis, linear regression analysis, and geographic weighted regression analysis considering spatial heterogeneity.18,25,28
This study aims to analyze factors of regional variation in national cancer screening rate in Korea using regional cancer screening rate data. In addition, during the COVID-19 pandemic in 2020, we tried to identify factors that might affect cancer screening rate, including COVID-19 situation in the region.
Methods
Data collection
In this study, 229 administrative areas in Korea were defined as target areas for analysis. Data provided by the National Health Insurance Service Center were used for national cancer screening rate index data in 2020 in 229 regions. During the COVID-19 pandemic, to identify variation factors in Korea's regional cancer screening rates, the Korea COVID-19 website, Korea Disease Control and Prevention Agency's Community Health Survey, the National Health Insurance Service Center's regional medical use statistics, the Health Insurance Review and Assessment Service's health insurance statistics of Korea, and transport accessibility index data of the Korea Transport Institute were used.
Variable definitions
The dependent variable was cancer screening rate provided through the national cancer screening of each city, county, and district. The 2020 National Health Insurance Service health screening statistics were used. The national cancer screening rate by region used the percentage (%) of the number of people who had actually undergone national cancer screening among subjects of national cancer screening by region for gastric cancer, colorectal cancer, liver cancer, breast cancer, cervical cancer, and lung cancer. This is a cancer screening rate that applies all data from January to December 2020, and the pandemic began in Korea with the first confirmed case of COVID-19 in January 2020. Cancer screening recommendations in Korea vary according to age and gender, and the cancer screening rate refers to subjects who completed applicable cancer screening during this period.
Independent variables were defined using collectable regional indicator data based on community vulnerability factors during the COVID-19 pandemic. Independent variable was referenced US community vulnerability index. The US Surgo Foundation grouped the US community vulnerability index into six themes. Table 1 shows variable definitions of variables for the national cancer screening rate by region in this study based on COVID-19 community vulnerability indicator (CCVI) index in the United States and previous studies.29–31
Definition of national cancer screening rate factor variables.

Statistical analysis
In this study, IBM's SPSS Statistics 27.0 (Armonk, NY, USA) program and ArcGIS pro 2.6.0 (Esri, Redlands, CA, USA) program were used for analysis. Descriptive statistical analysis was conducted to identify general characteristics of the national cancer screening rate and variation factors in national cancer screening rate in the region to be analyzed. A correlation analysis was conducted to find correlation between the national cancer screening rate and variation factors in the national cancer screening rate in the region to be analyzed. In addition, to confirm spatial dependence of the national cancer screening rate among regions, regional distribution of the Korean national cancer screening rate was identified through mapping and a global spatial autocorrelation (Global Moran's I) analysis was conducted. Global spatial autocorrelation (Global Moran's I) analysis is a representative spatial statistical technique that can measure spatial autocorrelation to identify spatial dependence. Moran's index is a spatial autocorrelation index calculated through global spatial autocorrelation analysis. It ranges from −1 to 1. If Moran's index is greater than 0, close to 1, and statistically significant, it can be judged that the Korean national cancer screening rate, which is the target area, has spatial dependence, which is a spatially strong cluster. If it is judged that there is spatial dependence between regions in the national cancer screening rate in Korea, it is necessary to reflect spatial characteristics between regions and identify factors of regional variation. Thus, a geographically weighted regression analysis was conducted to identify factors of variation in national cancer screening rates by region in Korea. In geographic weighted regression analysis, the kernel function type for geographic weighting uses an adaptive method that assumes that locations of observed cases are irregularly distributed within the study area.
Results
General characteristics of study regions
Descriptive statistics of general characteristics of the area to be analyzed are shown in Table 3. The average national cancer screening rate was 48.72%. The region with the lowest cancer screening rate was 38.65% and the highest was 56.0%. Regional average of the number of populations of cumulative COVID-19 confirmed cases per 100,000 was 98.08. The average of concern about COVID-19 infection was 68.12%. The average of concern about damage caused by COVID-19 infection was 73.40%. As for epidemiological factors of the analyzed region, the average prevalence of hypertension in adults aged 30 years or older was 19.37%, the average prevalence of diabetes was 8.39%, and the average prevalence of obesity in adults aged 19 years or older was 31.38%. The average number of national cancers screening medical institutions per 100,000 population in the analyzed region was 12.29. Daily average access time to general hospitals by car was 24.12 min and daily average access time to general hospitals by public transportation and walking was 49.12 min (Table 2).
General characteristics of study regions.

EQ: Maximum value – Minimum value.
Correlation analysis of national cancer screening rate and variation factors.
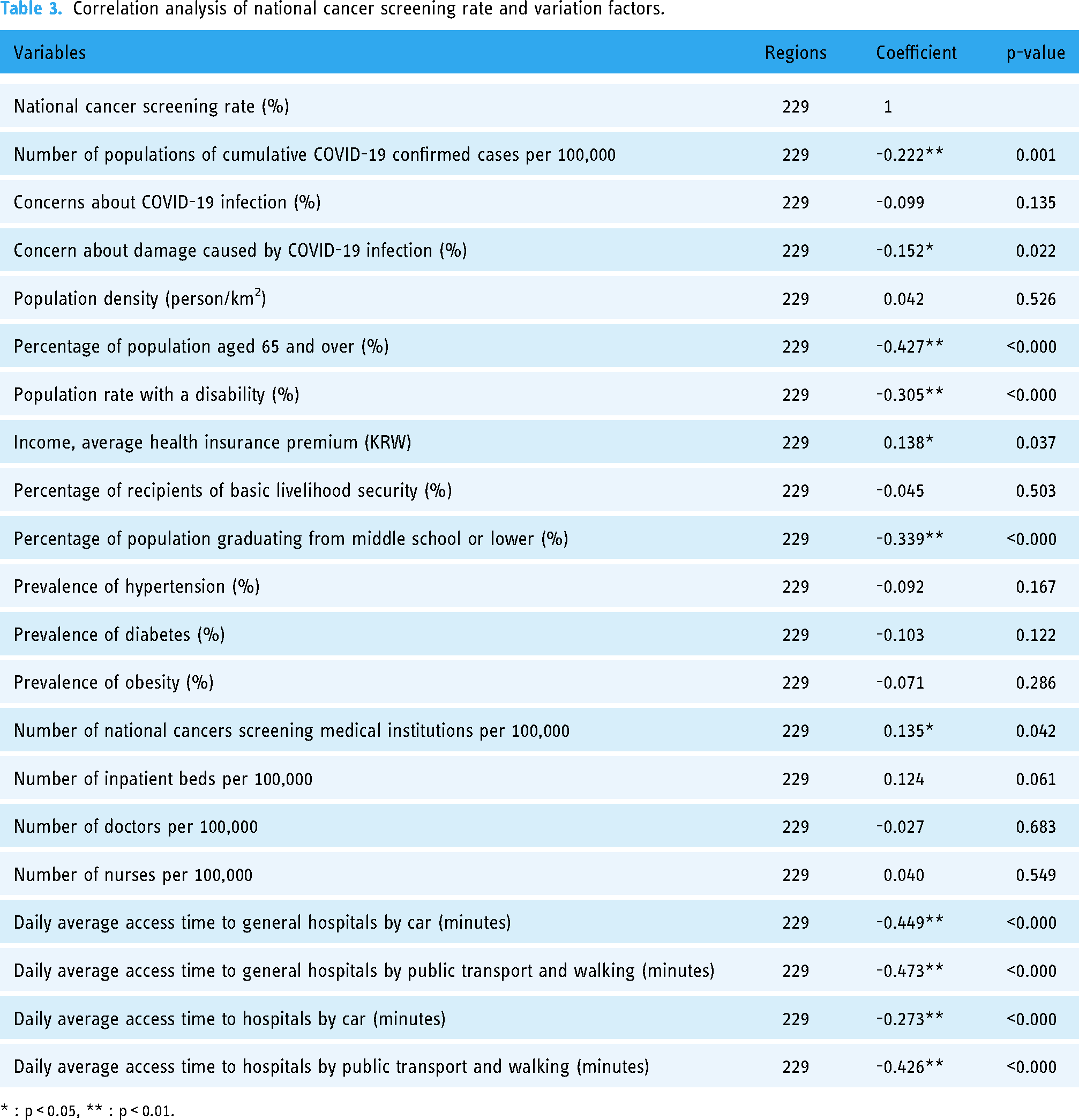
* : p < 0.05, ** : p < 0.01.
Correlation analysis of national cancer screening rate and variation factors
Table 3 shows the results of correlation analysis between the national cancer screening rate and variation factors by region. As a result of the analysis, variables with statistically significant (P < 0.05) positive correlations with the national cancer screening rate were income level and the number of national cancers’ screening medical institutions per 100,000 population. It was also found that the national cancer screening rate was statistically significantly (P < 0.05) lower in regions with a high the number of populations of cumulative COVID-19 confirmed cases, regions with a high risk of damage concern from COVID-19 infection, regions with a high proportion of population aged 65 years or older, regions with a high proportion of disabled population, regions with a high proportion of population who graduated from middle school or less, and regions with low accessibility to general hospitals and clinics by cars, public transportation, or walking (Table 3).
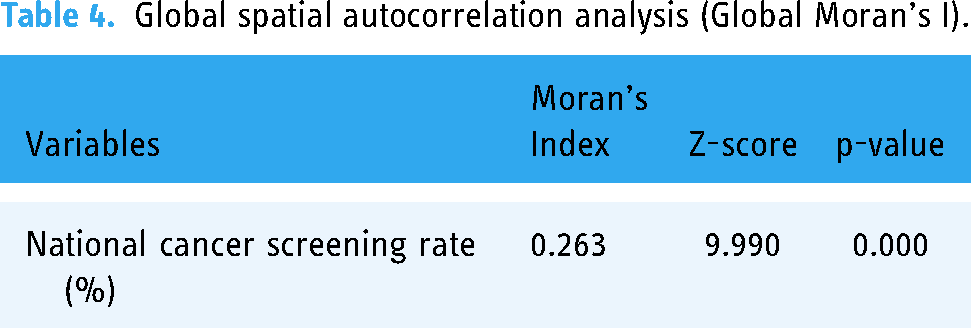
Global spatial autocorrelation analysis of national cancer screening rates
Figure 1 shows a graphical map of regional distribution of national cancer screening rate in Korea. The darker the color, the higher the national cancer screening rate. It could be seen that there was a difference by region. It was also found that Korea's national cancer screening rate tended to cluster among regions (Figure 1). Therefore, a global spatial autocorrelation analysis (Global Moran's I) was conducted to identify spatial autocorrelation of cancer screening rate by region. As a result of the analysis, Moran's index was 0.263 with a p-value of Moran's index of 0.000, indicating that cancer screening rates by region were statistically significantly clustered between regions. This confirmed that Korea's national cancer screening rate had spatial dependence between regions (Table 4).

Regional distribution of national cancer screening rates.
Global spatial autocorrelation analysis (Global Moran's I).
Geographic weighted regression analysis of regional variation factors
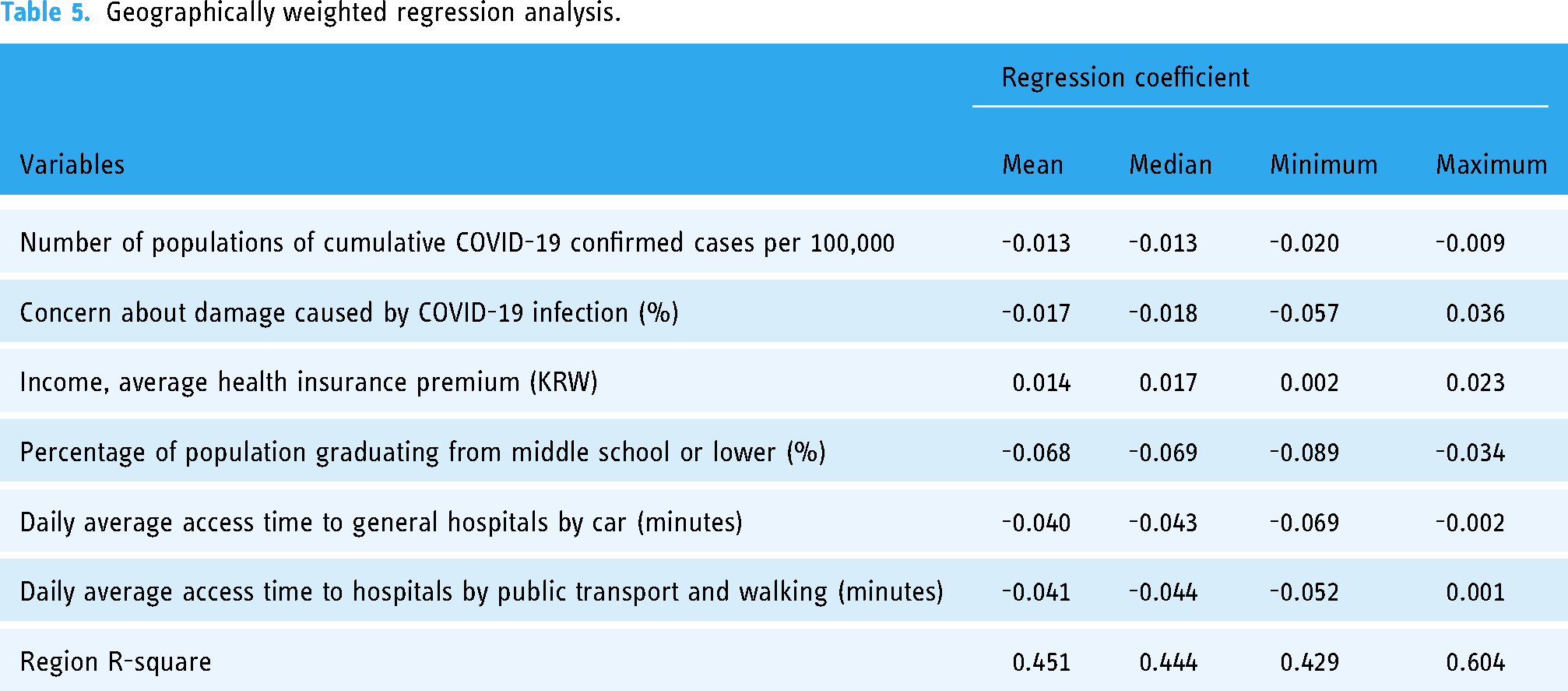
A geographically weighted regression analysis, a spatial statistical technique, was conducted to identify factors of regional variation in Korea's national cancer screening rate by reflecting spatial characteristics of each region (Table 5). As a result of a geographically weighted regression analysis, in the 2020 COVID-19 situation, variable factors affecting the national cancer screening rate among regions in Korea were regional number of populations of cumulative COVID-19 confirmed cases, concern of damage caused by COVID-19 infection, income level, proportion of the population graduating from middle school or lower, average daily access time to general hospitals by car, and average daily access time to hospitals and clinics by public transportation or walking. Percentage of population graduating from middle school or lower (%), which has the highest absolute value of the regression coefficient by region, based on the mean and median of the regression coefficient by region, had the strongest effect.
A total of 229 regression models were calculated for each administrative region and the explanatory power of the regression models ranged from 42.9% to 60.4%. Based on average and median values of regression coefficients, areas with a high number of populations of cumulative COVID-19 confirmed cases, areas with a high risk of damage concern from COVID-19 infection, areas with a high proportion of population who graduated from middle school or less, areas with a longer daily average access time to general hospitals by car, and area with longer the daily average access time to hospitals and clinics by transportation or walking had lower national cancer screening rates. In addition, it was found that the higher the income level, the higher the national cancer screening rate (Table 5).
Geographically weighted regression analysis.
Discussion
In order to identify regional differences in screening rates of cancer screening services provided by the state in the COVID-19 situation and to find out regional factors related to this, data that could represent regional characteristics were collected and analyzed. In the context of the COVID-19 pandemic, attention should be paid to decreased use of medical services because it could lead to a vacuum and disconnection of medical services for patients who absolutely need them. It could also worsen health outcomes.29,32
In this study, an ecological methodology was used to identify regional variations in national cancer screening rate and related factors. Research based on ecological methodology has compared health frequencies and characteristics between groups using population groups as a unit of analysis. 33 Since this study aims to identify regional differences and variations in national cancer screening rate, it can be said that it is appropriate to apply ecological methodologies and use national-based regional health statistics and welfare statistics. Therefore, in this study, regional variation and spatial dependence were identified using geographically weighted regression analysis and global spatial autocorrelation analysis. According to the first law of geography of previous studies, “Everything is related, but spatially close things are more closely related”, cases sampled in spatially close locations tend to have similar values, which is called spatial dependence.34,35
As a result of global spatial autocorrelation analysis of national cancer screening rates, it was confirmed that Korea's national cancer screening rates had a spatial dependence between regions. As a result of geographic weighted regression analysis to identify factors for regional variation in national cancer screening rates, results showed that regions with a high number of populations of cumulative COVID-19 confirmed cases, regions with a high risk of damage concern due to COVID-19 infection, regions with a high proportion of population who graduated from middle school or less, regions with a longer daily average access time to general hospitals by car, and regions with a longer daily average access time to hospitals and clinics by transportation or walking had lower national cancer screening rates. It was also found that the higher the income level, the higher the national cancer screening rate. Through this study, it was confirmed that the national cancer screening rate in Korea has spatial dependence between regions. This suggests that in order to effectively improve the national cancer screening rate, it is necessary to establish a national cancer screening rate improvement strategy that reflects regional and spatial effects. Therefore, it is necessary to support policies such as manpower, resources, and budget considering the demographic and socioeconomic characteristics of the region and the accessibility of medical care. In addition, in order to maximize the spatial effect of the national cancer screening rate, health promotion activities should be carried out in cooperation with neighboring regions.
The decrease in national cancer screening rate in regions with high number of populations of cumulative COVID-19 confirmed cases and regions with high concern of damage from COVID-19 infection is consistent with domestic and foreign preceding research results showing that medical activities such as diagnosis and treatment have significantly decreased by direct and indirect effects of COVID-19.1,3,36 Kim et al. have reported that the number of outpatient visits by diabetic patients is increased when the incidence of COVID-19 patients is decreased, 36 consistent with results of this study showing that the local COVID-19 incidence rate and the use of medical services had negative correlations with COVID-19 infection and that its psychological effects had emerged as concerns about infection, affecting community health management such as national cancer screening. This suggests that a strategy to increase the national cancer screening rate through trust in the national health policy is needed in the future, even in this pandemic situation.
According to a number of previous studies, the higher the income level of an individual, the more people will undergo cancer screening.22,23 In addition, one study has shown that the probability of receiving cancer screening is high when the degree of recognition of the income level of the region is high. 37 In this study, the income level of the region was expressed as an average health insurance premium per capita. Results of previous studies are consistent with results of this study, which showed that the higher the average health insurance premium in the region, the higher the national cancer screening rate. 37
Results of correlation analysis showed that the higher the number of national cancers’ screening medical institutions, the higher the national cancer screening rate. This coincided with results of previous studies showing that more local medical resources were associated with more medical usage.38–42 Kwak et al. have analyzed difference in medical use according to the distribution of health care resources among regions and suggested that when more medical resources such as the number of hospital beds, doctors, and medical equipment are supplied, medical use is increased. 38 The number of medical institutions and areas with high distribution of medical resources also mean accessibility and equity of medical care. In this study, the national cancer screening rate was significantly lower in regions where daily average access time to general hospitals and clinics was higher. This means that a policy that considers medical accessibility and regional equity in the distribution of medical institutions is needed.
The significance of this study is as follows. The pattern of medical use is influenced not only by individual characteristics, but also by various environmental factors surrounding the individual. Therefore, this study analyzed regional factors that could affect the national cancer screening rate during the COVID-19 pandemic. In addition, the results of this study have important significance in that they can be used for interventions to prevent cancer occurrence and death targeting target regions with low cancer screening rates. Results of this study could be used as basic data necessary for establishing health policies to improve the national cancer screening rate considering characteristics of each region.
Limitations of this study are as follows. First, this cross-sectional study was conducted with data from the 2020 COVID-19 pandemic period, with time-series analysis and spatio-temporal variation factor analysis by year not performed. Second, the dependent variable of this study was the national cancer screening rate, which could not reflect private cancer screening rate due to data limitations. Third, there is a limitation that the analysis of influencing factors including data on comorbidities of cancer screening subjects could not be performed due to lack of budget. In the future, it is necessary to carry out multi-year studies including data on private cancer screening rate and comorbidities in the region to conduct additional studies with more specific analysis of regional factors.
Conclusions
As a result of analyzing the national cancer screening rate by region in Korea during the COVID-19 pandemic, it was confirmed that there was a spatial difference between regions. It was found that the national cancer screening rate was lower in regions with a high number of populations of cumulative COVID-19 confirmed cases, regions with a high concern of damage from COVID-19 infection, regions with low levels of education, and regions with longer access times to general hospitals and clinics. In addition, it was confirmed that the higher the income level, the higher the national cancer screening rate. These results can be used to establish national health policies that can reflect regional variation factors in situations such as the COVID-19 pandemic. It is believed that results of this study can contribute to digital health policies to promote community health in the future.
Footnotes
Acknowledgements:
Not applicable
Conflict of interest:
The authors have no conflicts of interest to declare.
Contributorship:
JL and JP conceptualized and designed the study. JL obtained funding. JP data collection and data analysis. JL wrote the first draft of the manuscript.
Ethical approval:
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived for this study because it used anonymous public open indicator data, not an individual's personal data.
Funding:
This work was supported by the Dong-A University research fund.
Informed consent:
No patient consent was required for this study. All data used in this study were obtained from a public open database and data that complete anonymity guaranteed.
Guarantor:
None.