
Abstract
Objective
The COVID-19 infodemic has been a global public health challenge, especially affecting vulnerable populations such as Syrian refugees with limited internet access and functional, health, digital, and media literacies. To address this problem, we developed Wikaytek, a software to diffuse reliable COVID-19 information using WhatsApp, the preferred communication channel among Syrian refugees. In this paper, we describe the systematic development of the tool.
Methods
We undertook a pilot study guided by the Humanitarian Engineering Initiative (HEI)'s user-centered design framework, comprising five stages: (a) user research, including needs assessment and desk review of interventions with target users; (b) concept design based on platform and source selection, message format, concept testing, and architecture design; (c) prototyping and implementation, encompassing software development and system operation; (d) user testing (alpha and beta); and (e) evaluation through software analytics and user interviews. We reported a qualitative process evaluation.
Results
Wikaytek scrapes validated and reliable COVID-19-related information from reputable sources on Twitter, automatically translates it into Arabic, attaches relevant media (images/video), and generates an audio format using Google text-to-speech. Then, messages are broadcast to WhatsApp. Our evaluation shows that users appreciate receiving “push” information from reliable sources they can trust and prefer the audio format over text.
Conclusions
Wikaytek is a useful and well-received software for diffusing credible information on COVID-19 among Syrian refugees with limited literacy, as it complements the texts with audio messages. The tool can be adapted to diffuse messages about other public health issues among vulnerable communities, extending its scope and reach in humanitarian settings.
Introduction
The COVID-19 infodemic
The Internet has played a significant role in the COVID-19 pandemic. On one side, research institutions, public health agencies, and governments have used the Internet to monitor the diffusion of the virus using infoveillance techniques 1 or to spread timely information about how to prevent transmission, manage outbreaks, and promote protective behaviors. However, on another side, individuals and organizations have used the Internet to share inaccurate information (i.e., misinformation) or deliberately shared wrong information and conspiracy theories (i.e., disinformation), creating panic and contributing to the diffusion of rumors2,3 and confusion among the general public and mass media, who were diffusing information received through internet resources. 4
Since its beginning, the COVID-19 pandemic has been characterized by the abundance of misinformation and disinformation shared on the Internet, which the director general of the World Health Organization (WHO), Tedros Ghebreyesus, called an “infodemic.” 5 While some research suggests that misinformation about health topics is not a prerogative of the COVID-19 pandemic,6,7 and myths and rumors were diffused on other health topics, 8 the COVID-19 infodemic contributed to an increased sense of uncertainty, which was already associated with a novel coronavirus. 9 For example, at the beginning of the outbreak in Lebanon, a study on the volume of misinformation on Twitter reported that about 25% of the analyzed posts contained misinformation, and 17% had unverifiable information spread by informal personal accounts of Internet personalities. 10
Even if misinformation or disinformation related to COVID-19 was generated by a handful of influencers on social media, 11 myths, conspiracy theories, and “fake news” endangered the work of public health organizations and governments, diffusing rumors and unverified information, diffusing mistrust in research and governmental institutions, especially when political figures were diffusing disinformation. 12 For example, the lack of trust in governments has been associated with the limited use of initiatives to counter the pandemic, including contact-tracing apps. 13 In addition, the politicization of the pandemic in several countries translated into a polarized public opinion, especially on social media, which have increasingly become ideological eco-chambers of diametrically opposing views. 14 Whether at the containment or immunization stages, misinformation and disinformation can cost lives and amplify the harm caused by the virus, making it challenging for people to find reliable sources and follow guidance. 15 For example, a study by Johns Hopkins Center for Health Security estimated that the misinformation and disinformation about COVID-19 vaccines cost the US government between $50 and $300 million daily due to the treatment of unvaccinated individuals. 16
The infodemic among vulnerable populations and refugees
The pandemic and the infodemic inequitably hit vulnerable segments of the population worldwide.17–19 COVID-19 misinformation has been linked to poor health and limited digital health literacy, which are notoriously connected with low socioeconomic status and health inequalities.20–22 Migrants and refugees from conflicts have been among the most vulnerable populations left out of a global COVID-19 response.23,24 Considering the lessons learned from the influenza pandemic, Truman et al. 25 recommended that public health organizations engage refugees by considering different cultural, linguistic, and literacy-related dimensions. The authors also highlighted the need to reach this vulnerable population through authorities such as religious leaders or institutions that gained their trust. 25 Other researchers called for a more equitable response to the pandemic and a shared responsibility to ensure that vaccines and other services are available to the most vulnerable. 26
In countries with multiple crises and weak political and economic infrastructures, it has been harder for governmental and public health organizations to manage COVID-19 public health and communication responses. Lack of trust toward institutions 27 was coupled with the difficulties in promoting effective contact tracing and quarantine enforcement. 28 Furthermore, people with chronic conditions and disabilities and refugees had even more challenges accessing health services during lockdowns in low-resource countries (e.g., Lebanon29,30).
COVID-19 response and Syrian refugees in Lebanon
Lebanon, a small country in the Eastern Mediterranean Region, is the largest refugee-hosting country per capita in the world, with an estimated 1.5 million Syrian refugees living in the country. 31 Since 2019, the country has been facing an unprecedented series of economic, financial, and social crises, deeply affecting the livelihoods of all communities residing there.32,33 Political instability at different levels is further stalling any fiscal or social reforms. The COVID-19 pandemic soon followed by the Beirut port explosion 32 accelerated the country's economic downturn and the suffering, especially for the most vulnerable segments of the population, including the Syrian refugees. The absence of viable and durable solutions results in greater vulnerability, extreme poverty, and resorting to harmful coping strategies, such as increased uptake of debt, rationing food, domestic violence, child labor, and child marriage. 31 Although the government, local communities, and multiple international organizations have been acting together to bear the brunt of the refugee influx, there still exists a gap in addressing vulnerabilities and meeting the basic needs of Syrian refugees.
Regarding health, Syrian refugees have limited access to health care due to their low rates on legal residency. Only 17% of the total estimated population is officially registered within the United Nations High Commissioner for Refugees (UNHCR). 31 The multiple crises have also undermined the local response to COVID-19, with locals generally mistrusting messages and recommendations coming from Lebanese governmental institutions, unable to contextualize and enforce infection control standards. 27 The level of mistrust was even higher among Syrian refugees, 31 who were already facing difficulties accessing healthcare services due to limited awareness, education, and discrimination; 34 they also have limited access to reliable, accurate healthcare information, living in difficult circumstances. 34 The COVID-19 pandemic exacerbated this precarious situation due to high levels of crowding, inadequate access to clean water, protective equipment such as masks, health care, and community awareness.30,34 The problems mainly affect women living in urban settings, primarily unemployed, at extreme risk of gender-based violence. 35
Initiatives to counter the COVID-19 infodemic globally
Since the beginning of the pandemic, the WHO has engaged in numerous activities to combat the infodemic, such as the first infodemiology conference, in June 2020, 36 or the “MythBusters” campaign to dispel misconceptions about the virus and its transmission. 37 At the same time, the WHO partnered with technology companies such as Meta (Facebook) and Alphabet (Google) to reduce the spread of misinformation through algorithms and semiautomated search filtering. 38 In addition, the WHO, recognizing the need for a coordinated COVID-19 infodemic response, through its Information Network for Epidemics (EPI-WIN), gathered ideas from 50 action points organizations could use to minimize the problem. 39 The main action areas include strengthening the evidence, simplifying knowledge translation, fact-checking and addressing misinformation, amplifying messages to reach communities and individuals most in need, and monitoring rumors and misinformation through “social listening.” 39 An example of an intervention that teaches how to recognize fake news (using the principles of inoculation theory 40 on critical media literacy) is the University of Cambridge's “Go Viral” game. 41 However, a recent meta-analysis of 16 interventions to counter COVID-19 misinformation found limited evidence of their effectiveness on changing beliefs and behaviors. 42 Yet, a significant limitation of these initiatives is that they were developed in high-income countries with high-resource settings. They were based on the assumption that many people have basic functional literacy and minimal digital and media literacies. 42 Media, computer, and health literacy skills are hard to transfer and take time to develop; moreover, they are rarely measured or considered in digital health intervention development. 43 Moreover, these initiatives targeted savvy social media users with access to the internet and social media, neglecting vulnerable segments of the population.
Initiatives to counter the infodemic among refugees in humanitarian settings and Lebanon
Mobile phones are commonly used as delivery modes of health communication interventions targeting refugees in low-resource and humanitarian settings. Examples of mobile-based interventions include UNRWA's Khan Younis Health Centers used text messages to improve adherence to appointments among vulnerable patients with noncommunicable diseases. 44 Another example includes a mHealth app developed to increase access to maternal and child health services among Syrian refugees living in Turkey was adapted for the pandemic. 45 Following data from user feedback, the app was successfully modified to include crucial COVID-19-related information and symptom checking, contributing to national prevention efforts. 45 Another example is the UN Women's WhatsApp service disseminating COVID-19-related information among Syrian women in Jordan. 46 While successful considering the propensity of Syrian refugees to receive information via WhatsApp, 47 this intervention did not account for different literacy levels and skills. Another technology, interactive voice response (IVR), has been used with refugees in several low-resource countries, such as India and Pakistan, where health workers host radio-like shows, and beneficiaries access the show through their mobile devices. 48 However, these interventions required dedicated staff to create and disseminate health messages to ensure the system remained operational.
In Lebanon, the UNHCR's 2022 refugee vulnerability assessment report (VASyR) found that 90% of Syrian refugees own a phone, and 89% had an active mobile data plan. 31 Furthermore, the vast majority reported using WhatsApp (93%), followed by Facebook (29%). 31 Some research shows refugees prefer Facebook and WhatsApp over traditional text services.49–51 Most refugees like WhatsApp's voice notes over texting 52 even though some other studies reported that Syrian refugee women considered text messages a reliable source of information. 53 Other forms of communication include the “Citizen Radio” initiative, which involved IVR technology and connected participants to a host, guest speaker, and other listeners through a mobile app, delivering audio-based health information to refugees. 54 IVR-based interventions have limitations because some refugees might share a phone line with other family members or need an active voice plan. 52 Yet, a recent cross-sectional study investigating eHealth literacy among people living in Lebanon revealed low literacy levels among Syrian respondents. 55
A preliminary report on COVID-19 vaccine acceptance among Syrian refugee beneficiaries of a humanitarian organization in Lebanon 56 showed that about a third refused to vaccinate. The main reasons behind this refusal were concerns about vaccine safety and effectiveness. 56 Another qualitative study argued that these misconceptions might be due to misinformation shared on informal social networks. 30 International organizations such as the local and regional WHO offices, the United Nations Children's Fund (UNICEF), the Norwegian Refugee Council, and others have attempted to develop campaigns in Arabic and English to raise awareness about COVID-19 and promote vaccine uptake among refugees. However, to our knowledge, no published reports evaluated such campaigns.
Aims and objectives
In response to these gaps in the literature and practice, the Humanitarian Engineering Initiative (HEI) at the American University of Beirut (AUB) developed Wikaytek (which means “your protection” in Arabic), a tool to disseminate credible and reliable COVID-19-related information among Syrian refugees, specifically among women living in urban settings. This report summarizes a pilot study used to develop and evaluate Wikaytek. Specifically, this pilot study was aimed at (a) describing the iterative process of developing Wikaytek, (b) evaluating its features and impact, and (c) reflecting on future applications.
Methods
Design
We conducted a pilot study to develop the Wikaytek tool according to a user-centered design framework adapted from an interfaculty-based service model of the HEI described in Najem et al. 57 The HEI team includes expert researchers from engineering and public health disciplines, research assistants, and interns working to develop solutions to humanitarian and global public health problems. Most of HEI's work has addressed Syrian refugees’ challenges in Lebanon.
The user-centered design framework 57 consists of five main phases: (a) user research and analysis through needs assessment, (b) concept design, (c) prototyping and implementation, (d) user testing, and (e) evaluation, as represented in Figure 1. We utilized social marketing as our overarching evidence-based, theory-driven planning framework 58 to define the behavioral change strategy to promote the adoption of the tool against COVID-19 misinformation among vulnerable populations. Social marketing has been applied to develop and implement COVID-19 vaccination interventions among various populations.59–61

Humanitarian Engineering Initiative's user-centered design framework. 57
Phase 1: user research and analysis
Needs assessment
A group of four female graduate students enrolled in the Master of Public Health (MPH) at the Faculty of Health Sciences in the Fall 2020 semester conducted a needs assessment on behalf of the HEI team. The HEI was the partner organization in a service-learning course entitled “Social marketing for public health” (HPCH 333), 62 a course taught by a member of the research team (MB). The students worked with HEI to develop a marketing plan to define the “product” (i.e., the platform itself) and promote its adoption. The first (JS), fifth (AG), and last author (IHE) cosupervised the MPH students along with the fourth author (MB). Before the social marketing course, the students took a qualitative research methods course as part of their MPH program, so they had some experience in undertaking qualitative research. Formal or informal formative research activities are an essential stage in developing a social marketing plan 63 and are used to gain insight into the experiences of the potential target audience.63,64 As such they follow a descriptive phenomenological qualitative research approach. 65 The purpose of the needs assessment was to understand perceived barriers, benefits, and motivating factors related to the use of mobile phones for health, particularly for using them to receive COVID-19-related information. The needs assessment allowed the team to identify the tool's basic features and develop an overarching marketing strategy for the project. This activity was deemed exempt from ethical review because it was not research aimed at generalizable knowledge and did not involve collecting personal or identifying data. This is aligned with the definitions included in the regulations of the US Department of Health and Human Services (HHS), to which the AUB refers to—see §46.104 Exempt research (Subpart A) Basic HHS Policy for Protection of Human Research Subjects. 66
Sample
A convenience sample of 10 Syrian refugee women living in urban settings in Beirut, in the suburb of Sil El Fil, in the areas of Jesr Matar, Tarik Jdide, Al-Hersh, Al-Rihab, and Al-Bashoura. We purposefully sampled women because most were homemakers or unemployed and were more likely to have sufficient time to participate in the project and disseminate the knowledge and practices acquired to their families. Women also constitute most of the refugee population in the Eastern Mediterranean region, with some estimates referring to 70%. 67 Displaced women are particularly vulnerable, as they lack basic needs crucial for health, such as water sanitation and hygiene. 68 They have also reported barriers to healthcare services due to cost, distance, lack of awareness,69–71 limited literacy, and lack of trust in local governmental organizations. 69 We chose urban settings because the refugee population seldom receives aid from governmental or nongovernmental organizations (NGOs), unlike in informal tented settlements. 72 We chose Sin El Fil because it is a “community of practice” whose municipality has a longstanding relationship with the university and the Faculties of Health Sciences and Engineering. To summarize, the inclusion criteria were Syrian refugee women of any age living in the suburb of Sin El Fil, with a mobile phone to conduct the interview, interested in participating in the project.
Recruitment
Mission Village, a local NGO dedicated to support the homeless and alleviate poverty in Lebanon, based in Sin El Fil helped recruit participants. Mission Village, which is a longstanding partner of the HEI, diffused invites to participate in the project both verbally, or via WhatsApp using their network of beneficiaries, including Syrian refugees living in the area. Mission Village collected a list of phone numbers of potential interviewees and shared it with a member of the HEI (the first author JS), who, in turn, shared the numbers with the students. The NGO provided a list of 10 participants who agreed to be interviewed. The student interviewers had no relationship with the interviewees before the interviews.
Data collection procedures
Given the limitations due to the lockdowns and quarantine imposed by the government in 2020 and to ensure safety, the MPH students conducted the needs assessment through informal interviews over mobile phones (WhatsApp) while participants were at home. As participants were women homemakers, they likely had children or other family members around them during the interview, but this was not deemed to influence their responses. The interviewers introduced themselves as students and explained that they were investigating the use of mobile phones for information related to COVID-19, as part of a project on COVID-19 information among Syrian refugees in Beirut. The students explained that the information collected was treated confidentially and that they did not collect any identifying information. They collected oral consent before proceeding with the interview, which took about 15 min. The interviews were not recorded, and students took notes without collecting personal identifiers. All 10 refugees who were contacted agreed to participate and were interviewed. No further interviews were conducted, and the students believed the information provided reached theoretical saturation.
Materials
Four students conducted the interviews following a bespoke, structured interview guide to assess the interviewees’ availability of a mobile phone, accessibility to the Internet and ability to use apps (prompted digital literacy), COVID-19-related knowledge (prompted health literacy), and ability to fact-check (prompted media literacy), as well as scientific, or functional literacy (unprompted), based on the eHealth literacy model. 73 This model was followed as a recent study showed that eHealth literacy was lower among Syrian nationals residing in Lebanon. 55 The assessment also looked at the potential use of a unified platform to receive COVID-19 information and the refugees’ preferred communication channels, to identify its features and perceived benefits. The interview guide was approved by the HEI research team but was not pilot tested. The guide is provided in the Supplemental Material.
Data analyses
All four students combined their notes to summarize findings and organize them without coding around the themes of barriers related to “technological availability,” the different types of literacies according to the eHealth literacy model (functional, digital, health, media, scientific, and information literacies), benefits, motivators for using the tool, and competition. The students validated their summary through discussions with the supervisors JS and MB. Then, JS and MB codeveloped subthemes based on the summary provided by the students. The subthemes were inductively generated, following a mixed-method, deductive–inductive thematic analysis.74,75 Themes and subthemes were then reported in a narrative summary and included in the current report. No quotations were produced as the information was gathered in an aggregate format.
Desk review
In parallel, we conducted a desk review of digital interventions targeting Syrian refugees in low-income countries and humanitarian settings to contextualize the needs assessment results. In addition, we completed a competition analysis, based on the needs assessment to identify possible solutions to promote access to the platform. Competition analysis is a tool commonly used in social marketing76,77 to understand the nature of competing behaviors, services, or products that would limit the adoption of the proposed solution.
Phase 2: concept design
This phase used the results of Phase 1 to develop a human-centered design solution, including a clear, detailed step-by-step workflow. This phase encompassed the elements of platform and information sources selection, choice of message formats, and concept testing.
Concept testing
Concept testing was done to test the workflow and acceptability of the platform before designing a prototypical software architecture. Concept testing was conducted with the help of another group of undergraduate students enrolled in another service-learning-based “social marketing” course (HPCH 204) in Spring 2021, taught by the same member of the research team (MB). The students tested the protocol for delivering the messages using a private WhatsApp group called “Wikaytek – وقايتك” which was opened to a selected group of Syrian refugee women recruited through a local religious organization based in Sin El Fil (the Church of the Nazarene). The WhatsApp group was set to private to ensure confidentiality while monitoring access and reactions to the messages.
Phase 3: prototyping and implementation
This phase involved the production of a prototype, including software and technology development. A computer science and engineering team member (CF) developed the code to automate retrieving, translating, and disseminating information to WhatsApp.
Phase 4: user testing
In this phase, the Wikaytek prototype was tested by diffusing messages in the same group of users recruited in Phase 2, following the alpha and beta testing stages of software development. Alpha testing allowed us to address bugs and refine the software. Then, before the development of the final design, beta testing was conducted to check the prototype's feasibility, usability, and acceptability. Finally, we modified the tool based on the feedback and developed a final product, which was then released to the same group of users.
Phase 5: evaluation
This phase involved the assessment of the final version of the Wikaytek operating tool, with feedback collected throughout the process, using a combination of sources of information as follows:
WhatsApp analytics
Continuous usage analytics are provided by WhatsApp's internal analytics features. These include the number of messages sent and received, the number of times audio messages were played, and the number of active users.
Qualitative evaluation
A qualitative evaluation of Wikaytek was conducted between August 2021 and March 2022 to collect users’ feedback. Similar to the needs assessment, this activity was aimed to understand the experience of users; hence, it configures as a descriptive phenomenological approach. 65
Sample
A consecutive sample of all nine “active users” of Wikaytek WhatsApp testing group—all Syrian women refugees living in the suburb of Sin El Fil. Active users meant that they read the messages and actively engaged with the messages by sharing them, liking, or responding to them. Two participants were not interviewed, because they actively (n = 1) or accidentally (n = 1) left the group.
Recruitment
Participants were recruited in Phase 2 through the Church of the Nazarene, a religious organization partnering with the HEI. A pastor of the religious organization verbally invited Syrian refugee women acolytes to share their mobile phone number for participating in the project. The pastor then shared the number list with the HEI team. All users agreed to be included in the WhatsApp group and test the tool.
Data collection procedures
A female member of the research team (RAH), at the time of the interview an undergraduate intern student in Health Communication, managed the WhatsApp group, and invited group members to participate in a brief structured interview over a WhatsApp call. The interviewer undertook qualitative research methods as part of her health communication program. The interviewer briefly mentioned the purpose of the interview and obtained assent before completing the interview, which lasted 10 min and was likely conducted while participants were at home. As in the needs assessments, participants may have had children or other family members around them during the interview, but this was not deemed to influence their responses. Participants were already familiar with the name of the interviewer and the project, as they were in the WhatsApp group since Phase 2 of the project. The interviews were not recorded, and the researcher took notes following each question. The researchers believe that data saturation was reached as the entire user group was interviewed (excluding the drop-offs).
Materials
The interviewer followed a bespoke set of questions, which were as follows: How beneficial did you find the service? What did you like about the service? What did you dislike? Would you use it again? Did you share the information with someone, if so with whom? What did you like the most about the service? The questions were approved by the research team but were not pilot tested.
Data analyses
The researcher took the interview notes and generated narrative summaries for each user without coding the answers. The researcher organized the summaries according to the questions as they were asked. A visual summary of the comments was generated through a word cloud, based on the frequency of responses.
Results
Phase 1: user research and analysis
Barriers
The barriers to digital, health, and media literacies and communication channels related to COVID-19 are summarized in Table 1, along with potential solutions deducted from interventions identified through our desk review.
Competition and needs analysis for Syrian refugees receiving COVID-19 information on the phone.

Technology availability, accessibility, and use (digital literacy)
All women had access to a mobile phone since they were interviewed through WhatsApp phone calls, but most did not have an active data plan. In fact, many accessed the internet through a shared Wi-Fi connection at home. Most participants used WhatsApp and Facebook, and a few reported using YouTube and Instagram. However, all the interviewed women had access to a phone and an internet connection during the day.
COVID-19-related knowledge (health literacy)
Most participants declared knowing basic information about COVID-19, and all participants were aware of preventive measures, such as wearing masks in public, physical distancing, washing hands with water and soap, and sanitizing products from supermarkets. They received this information mainly from the television, Facebook, and WhatsApp groups. However, many participants were not aware of how to make sure that the information they receive is accurate or comes from a credible source. Despite knowing about the preventive measures, most abided by them only seldom. Some mentioned that they hated wearing masks, which are not always available. Also, some felt obliged to shake hands in public, increasing the transmission risk. Most of them mentioned that the dire economic situation made it challenging to buy sanitizers and proper hand-washing soaps (they were using what was available at home, i.e., dishwashing soap).
Media literacy
Most participants were aware of the consequences of using noncredible information and were conscious of the benefits of seeking credible information about COVID-19. However, they needed to learn how to check facts and verify the information coming to them. Despite being able to recognize credible sources such as the Ministry of Public Health and Doctors Without Borders, most of them relied on other sources of information, including social media and their entourage, because it required less time and effort and the belief that any information even if not entirely correct is better than no information at all.
Preferred communication channels for health-related information
Almost all participants declared sharing information with their family members and friends on WhatsApp or Facebook when they felt this knowledge was worth sharing. They also showed a willingness to explore a new information platform. Most participants preferred receiving COVID-19 and health information via WhatsApp. Most participants were flexible about the format (texts, videos, or pictures). However, a few respondents could not read, and thus they stated that video or audio messages would be the most accessible for them.
Benefits
The use and installation of the mobile platform designed by the HEI at AUB will have significant health and social benefits on Syrian refugee women and their families. Participants identified the following: (a) Reliable information reduces the risk of COVID-19 exposure in the community through the implementation of accurate preventive measures; (b) a mobile platform may increase the awareness about misconceptions that prevail on social media and lessen the fear of COVID-19 since these women will be empowered to overcome this disease and the stigma surrounding it.
Motivators
Participants mentioned several reasons for using a mobile platform for COVID-19-related information: (a) Need to know how to protect themselves and their loved ones: Almost all participants had children at home or cared for older people, who needed extra attention and care; (b) Convenience: All these women have access to a mobile phone and are connected to Wi-Fi at home; (c) Need for reliable information: Participants acknowledged that not all the information they obtained from people and social media platforms was credible, but they did not have the capacity and preparedness to do fact-checking before sharing.
Competition
The perceived competing, alternative behaviors and services were: (a) Social media platforms, in particular social networking sites such as Facebook and WhatsApp, which participants already used for entertainment and connecting with others. Social media were easy to use and required less effort and energy than learning to use a new platform; (b) Personal social networks: Asking people around is much faster and easier than waiting for an answer on social media pages; (c) Existing reliable sources of information: Very-known reliable and trustworthy channels such as the UNHCR and Doctors Without Borders were perceived as more appealing than checking new platforms developed by an academic institution albeit well reputed.
Phase 2: concept design
Platform selection
Based on the findings above, we chose a platform that could overcome the barriers that the refugees mentioned. The platform had to be easily accessible, possibly without an internet connection (or work asynchronously), and lightweight (i.e., consume little data). We selected WhatsApp, commonly used among Syrian refugees, for communicating with peers and sharing information. WhatsApp allows users to read messages whenever they can establish an internet connection and does not necessitate much data to operate.
Sources of information
To address the problem of limited media literacy (i.e., the ability to discern among different sources of information), we had to provide credible information already verified. Therefore, assuming very limited or no critical media skills, we selected sources of information based on their credibility and trustworthiness among refugees and expertise in the COVID-19 response. These included the local office of the WHO (@WHOLebanon), the local and regional office of the United Nations Children's Fund (@UNICEFLebanon, @UNICEFmena), and the local office of the UNHCR (@UNHCRLebanon), and the Lebanese Ministry of Public Health (@mophleb). These sources provided information in both Arabic and English through their Twitter channels, with publicly available Tweets. However, Twitter is accessed mainly by literate, well-educated, and tech-savvy users.
Message format
The information had to be written in Arabic and include audio files to account for those unable to read.
Concept testing
With the help of a local religious organization, other nine Syrian refugee women were recruited to test the process of delivering messages through WhatsApp. A team member sent the messages selected from Twitter manually to the WhatsApp group, which were manually translated from English into Arabic. Our team also voice-recorded the messages to provide an alternative to text before sharing them in the WhatsApp group.
All participants expressed interest in receiving credible information about COVID-19 and participating in the project. After only 1 hour following the first welcoming message and after 10 COVID-19 messages were sent to the group, 80% of the members read them, demonstrating that they were interested and accepted the communication modality.
Platform architecture design
We designed an automated process to extract, filter, and push messages generated from the identified reputable sources. The process is described in Figure 2. It entails an automated retrieval of data, followed by an agent-based selection, automated text-to-speech (TTS) translation, and semiautomated scheduling of messages to the dedicated WhatsApp group.
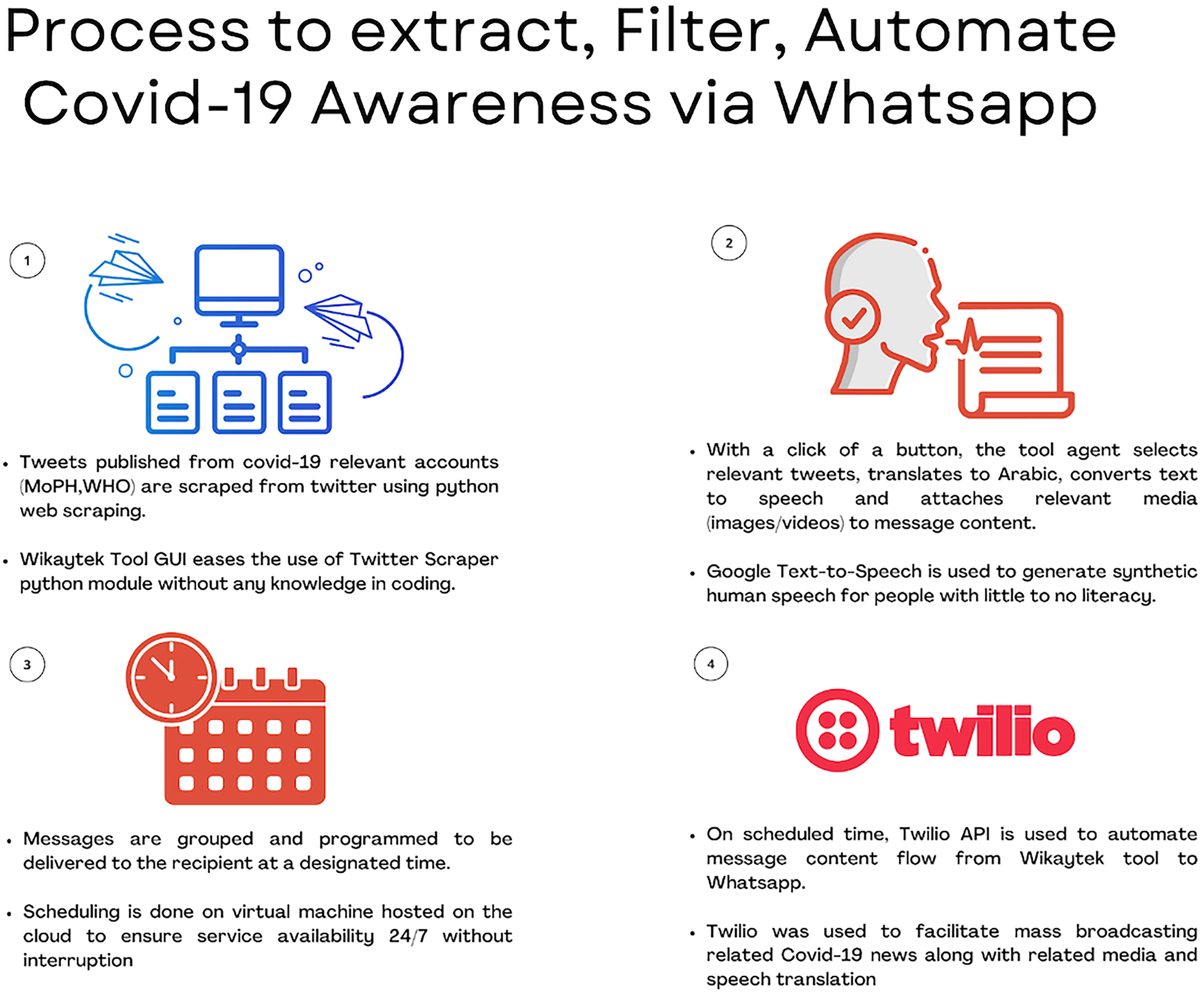
Process used to extract, filter, automate COVID-19-related information in Wikaytek.
Phase 3: prototyping and implementation
Software development
Programming language
The Wikaytek tool is written in Python, a general-purpose programming language commonly used to construct websites and apps, automate tasks, and analyze data. 79 The library for the graphical user interface (GUI) is PyQt, a Python wrapper for the open-source widget toolkit Qt that also serves as a cross-platform application development framework. Qt is a popular C++ framework for developing GUI applications for all major desktop, mobile, and embedded platforms (supporting Linux, Windows, macOS, Android, iOS, Raspberry Pi, and more).80,81 The GUI is presented in Figure 3.

Wikaytek graphical user interface (GUI).
The Python program scraped information from the Twitter accounts of selected sources, allowing the operator to choose relevant information related to COVID-19. In addition, a button was created to translate the message into Arabic (if the original message was in English) and convert the text to audio. Finally, the software allowed us to push the messages to a closed WhatsApp group automatically.
Twitter scraper
Wikaytek uses Twitter's application programming interface (API) to automatically view and import data from Twitter. Considering that Twitter API allows only 180 requests every 15 min, a modified TwitterScraper was developed. TwitterScraper is a GitHub-hosted Python scraper that scrapes tweets and user information by giving the appropriate search query, specific Twitter accounts, time range, and geolocation. 82 Our scraper circumvented Twitter API restrictions by directly collecting all query information using web scraping automation. Data are then extracted and saved as raw data before being transformed into a CSV file using the Python Pandas package. Finally, the scraped data is displayed in the Wikaytek tool GUI, making it easier for nontechnical users to import tweets.
TTS conversion and translation
We used Google Cloud TTS, a Google Cloud AI and Machine Learning product, to convert text into audio messages. TTS enables developers to generate playable audio of natural-sounding, synthetic human speech. Google TTS is appropriate for any application that provides consumers with human speech audio, turning text into natural-sounding speech in 220+ voices across 40+ languages powered by Google's machine-learning technology. 83 To collect COVID-19-related news from international sources, Wikaytek integrated Google Cloud translation services to provide immediate translation and tweet language recognition for tool agents. The Google Translation tool assisted by automatically recognizing the text language and translating the tweet into Arabic. 84 The tool allows for manual changes to be applied to the translation before converting to voice for the pronunciation to be more accurate.
Automated messaging
To automate message forwarding, Twilio services were used to facilitate broadcasting the messages, related media, and audio files to WhatsApp. Twilio API for WhatsApp allows developers to create prototypes using WhatsApp API without WhatsApp Business API, which is in beta and only available with dedicated access permission from WhatsApp. 85
Wikaytek facilitated the interaction between Google Cloud Services, Python Automated Scraping, and Twilio WhatsApp API without the necessity for programming skills on the part of the operator. The GUI sample in action is shown in Figure 4.

Wikaytek graphical user interface (GUI) with original Tweet and translated text.
System operation
After selecting the sources, the tool automatically scraped information from them. Keywords such as COVID-19, vaccine, and campaign filtered the tweets. Tweets were chosen based on their relevance to COVID-19 while considering many of the target audience's characteristics and geographical location (Sin el Fil, Beirut). The tool allowed the team to restrict the time range of the tweets. Only recent tweets were considered (1–3 days after tweets were posted). The messages shared on the Wikaytek WhatsApp group were all in Arabic. When the scraped tweets were in English, they were automatically translated into Arabic. The team added Arabic accents and phonetic signs to the text translated via Google to ensure correct pronunciation in the TTS service. Then, textual messages were converted to audio, and the audio file was sent to the WhatsApp group.
The Wikaytek tool operated from 26 July 2021, until 4 March 2022. During the pandemic's peak, COVID-19-related messages were sent 3 days a week on the Wikaytek group. One message as a text and an audio file was shared on Mondays, Wednesdays, and Fridays. The frequency of messaging was reduced with time. A team member ran the tool and sent the updates to the group.
Phase 4: user testing
Alpha testing
The alpha-testing phase for the first version of the software was conducted from 26 to 29 July 2021. During this phase, the buttons were labeled sequentially to guide the user through the button flow. A filtering feature was introduced to sort the scraped tweets based on specific keywords, making it easier to locate relevant information. After verifying all features’ full functionality, the capability to scrape data from multiple accounts simultaneously was added, and the source of the tweets was made visible through automation. Based on feedback from the testers, the TTS model was refined to sound more human like, and its speed was decreased to better accommodate individuals with limited literacy. Lastly, in addition to the scraped tweets, the media attached to the tweets was facilitated for appending during message forwarding.
Beta testing
The beta-testing phase was conducted over three days (26–29 July 2021). Generally, 1 h after receiving the welcoming and COVID-19-related messages sent to the group, seven out of nine members (80%) read the messages. Within a day, all group members listened to the audio files (9/9, 100%).
Phase 5: evaluation
WhatsApp analytics
WhatsApp analytics was used to monitor the participant's engagement with the messages and user activity. Most messages were read by most participants (80%) throughout the project period. Figure 5 shows the average number of times audio messages were played monthly, ranging from 55% in August 2021 to 65% in March 2022.

Wikaytek group WhatsApp analytics: frequency of audios played.
Qualitative evaluation
Qualitative interviews showed that participants were overall satisfied with the Wikaytek service and declared that they would use it again to get information about COVID-19. They stated that it increased their awareness and knowledge of COVID-19, and regularly shared the messages with their friends and relatives. They liked the information being provided and specifically the audio tool stating that the messages were better delivered through this modality. Below is a summary of the answers grouped by questions as these were asked:
How beneficial did you find the service?
All participants found the messages beneficial (7/7, 100%), and 5/7 (71%) found them very helpful. One participant found this service is very beneficial for their health and their kids’ health, and she was able to teach people around her about COVID-19. They liked everything about the service, especially that the information provided was credible.
What did you like/dislike about the service?
Most participants declared liking “everything about it” (6/7, 86%). One participant stated that it helped her protect herself against COVID-19 and understand the importance of taking the COVID-19 vaccine. Only one participant disliked the fact that it was impossible to interact with the service and to ask questions. The service was in fact designed to “push” information rather than provide a bidirectional communication channel with the researchers or organizations. Based on this feedback, we considered adding interactive chatbot features, such as a menu to “know more” about COVID-19 to receive other messages from the pool. However, these are features available in the WhatsApp for Business, not for closed user groups. Therefore, we considered transforming the service into an open group service, but more funding would be needed for such development.
Would you use it again?
All interviewees stated they would use the Wikaytek group in the future (7/7, 100%).
Did you share the information with someone, if so with whom?
Five out of seven users (71%) declared forwarding the messages to family members and friends in Lebanon and Syria, some even multiple times.
What did you like the most about the service?
Most participants appreciated the audio format (6/7, 86%), stating that this modality delivered the messages better than the text.
Based on the above information, we developed a visual summary of the preferred features of Wikaytek (Figure 6). We used a free online tool (freewordcloudgenerator.com) to generate a word cloud representing the keywords associated with Wikaytek most frequently mentioned in the summaries. The size of the text represents the number of times the word was mentioned by the users in the notes taken from the interviewer.

Word cloud representing the preferred features of Wikaytek.
Discussion
General findings
In this report, we described a pilot study that was conducted to develop the Wikaytek tool and its concept and process evaluation. In summary, Wikaytek (a) automatically disseminates existing verified messages, publicly available on social media; (b) it uses asynchronous communication to minimize the problem of intermittent internet connectivity; (c) it automatically translates text into audio to accommodate for illiterate individuals; and (d) it uses a platform, WhatsApp, that is commonly used among refugees.
To our knowledge, Wikaytek is the first tool that addresses COVID-19 misinformation among Syrian refugees in Lebanon and accounts for the intended users’ needs, preferences, and literacy levels (i.e., functional, media, health, and digital). 43 This project contributes to the limited literature on disseminating credible health information during the ongoing COVID-19 pandemic among vulnerable populations like refugees.23,24,36,39 Additionally, our project contributes to the humanitarian and public health literature demonstrating how a technological tool could be codeveloped with the target audience, considering their functional, health, and digital literacy levels. 43 We took a realistic and pragmatic approach to communicate information about a global public health emergency among refugees living in Lebanon,27,30 accounting for the context and political and socioeconomic determinants of health. The project specifically focused on a vulnerable segment of the population, Syrian refugees, who are generally underrepresented in the literature and marginalized by the global pandemic response.20,23,24 In addition, we decided to focus on women Syrian refugees residing in urban areas precisely because they are among the most vulnerable segment of the population, given their limited literacy and socioeconomic status.34,69–71
This project leverages mobile technology to diffuse COVID-19-related information. Wikaytek overcomes the technological and literacy barriers to disseminating reliable COVID-19-related information among Syrian refugees in low-resource settings. We elaborate on each of these dimensions in the paragraphs below.
Functional, health, and digital literacies
Existing evidence highlights that most refugee households have access to a mobile phone with an internet data plan; 25 however, some might need money to use the internet. Furthermore, not all refugees might have the digital, functional, and health literacies necessary to interpret COVID-19 messages. 55 Critical health literacy 22 and digital literacy are generally limited among vulnerable populations. 20 Hence, we developed a solution that diffuses a combination of text and audio messages on WhatsApp that refugees already use and does not require a stable and constant internet connection. 53
Previous research highlighted the value of using text messages to promote health among refugees in multiple low-resource settings during a health crisis (e.g., UN Women 46 or Kazakos et al. 48 ). Also, our project corroborates previous qualitative evidence from Lebanon and the region demonstrating the utility of WhatsApp in diffusing messages among Syrian refugees about health-related issues such as preconception and antenatal care.52,54 As done in “Citizen Radio,” 54 Wikaytek produces messages in audio format to account for low functional literacy among our target population.30,55 However, these messages can be accessed and played asynchronously, at the user's convenience, when they have an internet connection. Contrary to other available solutions or standard practices, we did not develop a new app or service that would consume the limited space on the phone and that would rely on a stable internet connection.
Media literacy and dissemination of verified information
Refugees consider text messages credible but need more critical media literacy to determine whether the sources are reliable. 50 Wikaytek includes software that collects COVID-19-related information already diffused on social media from credible and reliable sources (e.g., the WHO, various UN agencies, and the local Ministry of Public Health). By diffusing already verified and trustworthy information, Wikaytek addresses the problem of refugees’ limited media literacy (i.e., inability to fact-check and discern different media sources). 20 In addition, Wikaytek repackages the information that public health agencies diffuse on social media, channels that refugees do not regularly use. 24 While social media might have increased the reach of COVID-19-related prevention messages, it excluded those disengaged with the public discourse and those with limited critical media literacy, such as refugees.27,30 We utilized existing reliable sources for COVID-19 information, knowing that refugees rarely refugees consult those channels due to their mistrust of local governmental organizations. 27 Hence, Wikaytek can increase the reach of existing social media communications that local and international public health agencies disseminate.
Strengths, limitations, and future research
An essential strength of Wikaytek is its automation, which has excellent potential for replicability and scalability across refugees and other vulnerable communities. For example, Wikaytek could combat COVID-19 vaccine misinformation, which is high among Syrian refugees living in Lebanon. 56 In addition, Wikaytek can be used by organizations operating in humanitarian settings to diffuse messages to selected groups of users.
Another strength is our process, the user-centered design framework 57 that the HEI has used for many years working with Syrian refugees and other vulnerable communities in Lebanon. We developed this framework to maximize contextualization and adapt the solution to the users’ needs. We applied social marketing principles to define the behavioral change strategy to promote COVID-19 among Syrian refugees, knowing that it has been used in the context of COVID-19 vaccination interventions among various populations.59–61 According to social marketing and as recommended by Truman et al., 25 we codesigned a solution to deliver important COVID-19-related information.
Despite the many strengths, we need to acknowledge some limitations. First, the users who participated in this project were from one suburb of the capital city. They were highly interested in contributing to the project so that they might have different views and experiences than refugees living in smaller urban areas. Not only were they interested but also they possessed some level of eHealth literacy—which encompasses the domains of functional, computer, media, health, information, and scientific literacies. 73 While we have not formally assessed eHealth literacy like in other studies, 55 the analysis of the notes generated from the needs assessment interviews demonstrates that participants declared having good knowledge about COVID-19 protective measures (health literacy) and were familiar with social media platforms and mobile phones (digital literacy), yet they had difficulties discerning the trustworthiness of information (media literacy). The sample included participants who could read and understand Arabic (functional literacy), even though probably in a spoken format, as some of them declared unable to read. Future studies should formally assess the level of eHealth literacy (e.g., through the popular eHEALS, 86 which has been used in local studies 55 and has also been validated in Arabic 87 ), and other specific literacies such as critical media literacy, which is essential to navigating the ocean of information especially during the COVID-19 infodemic. 88
Another limitation was working with a very mobile and hard-to-reach population (i.e., Syrian refugees living in urban settings) has always been challenging. These refugees avoid being registered with the UNHCR or local municipalities to avoid discrimination or the risk of being deported to Syria. We tried to overcome these problems by recruiting users through our partner nongovernmental and religious organizations because refugees consider these trustworthy and reliable, as suggested by Truman et al. 25 Third, working with Syrian refugees in urban areas has been even more challenging due to the restrictions imposed by COVID-19 curfews and lockdowns, which limited the opportunity to visit the targeted areas and talk to our intended beneficiaries. As a result, future investigations should include a more diverse and extensive group of participants and find alternative ways to approach this invisible population.
A technical limitation that needs to be considered is the maximum number of users allowed in a closed WhatsApp group. While WhatsApp has recently increased this number from 512 to 1,024, 89 it still limits the reach of WhatsApp-based communication interventions targeting larger groups, possibly millions of individuals. A way to overcome this limitation might be to use WhatsApp Communities 90 or a WhatsApp channel. The first option would allow combining multiple groups, but scaling this up would require human resources to manage these groups.
Conclusions
Wikaytek helps disseminate credible and reliable COVID-19-related information to Syrian refugees through WhatsApp. The Wikaytek tool repurposes existing information that public health and international organizations already diffuse on social media (e.g., Twitter) and adapts to the needs and skills of Syrian refugees. As a result, Wikaytek can be used to reach this vulnerable segment of the population, who need guidance and support for protecting themselves from COVID-19. Even though the project targeted Syrian refugees living in urban settings in Beirut, the tool could be scaled up to reach other metropolitan areas or remote areas in Lebanon and different countries.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231205280 - Supplemental material for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool
Supplemental material, sj-docx-1-dhj-10.1177_20552076231205280 for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool by Juliette Semaan, Christopher Farah, Reem Abou Harb, Marco Bardus, Aline Germani and Imad H Elhajj in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231205280 - Supplemental material for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool
Supplemental material, sj-docx-2-dhj-10.1177_20552076231205280 for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool by Juliette Semaan, Christopher Farah, Reem Abou Harb, Marco Bardus, Aline Germani and Imad H Elhajj in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231205280 - Supplemental material for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool
Supplemental material, sj-docx-3-dhj-10.1177_20552076231205280 for Tackling the COVID-19 infodemic among Syrian refugees in Lebanon: Development and evaluation of the “Wikaytek” tool by Juliette Semaan, Christopher Farah, Reem Abou Harb, Marco Bardus, Aline Germani and Imad H Elhajj in DIGITAL HEALTH
Footnotes
Acknowledgments
We want to thank the refugee women who participated in this project and provided insight and the organizations that helped access this population (Church of the Nazarene and Mission Village). We also thank the Master of Public Health students enrolled in the “Social Marketing for Public Health” course in the Fall of 2020: Yasmen Baroudi, Lea Chaiban, Madison Grant, and Maya Hammoud; and the Bachelor of Arts in Health Communication students enrolled in the “Social marketing” course in Spring 2021: Sophie Abou Ghaida, Reem Abou Harb, Elissa Hamadeh, Jana Kazan, and Jalila Issa.
Contributorship
IHE, AG, and JS conceived and designed the project with intellectual input from MB. JS coordinated the project, and RAH assisted in its operation and evaluation, collecting data, and summarizing information. CF developed the platform and helped with the pilot testing and evaluation. JS and MB drafted the first version of the manuscript with input from CF and RAH, which all authors then edited. Finally, all authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was deemed exempt from ethical review by the Institutional Review Board because it was not research aimed at generalizable knowledge and did not involve collecting personal or identifying data (section §46.104, subpart A, Basic HHS Policy for Protection of Human Research Subjects, US Department of Health and Human Services). All Syrian refugees voluntarily agreed to participate in the Wikaytek project and consented to enroll in the related WhatsApp group.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Maroun Seeman Faculty of Engineering and Architecture Endowment under the Crisis Research Catalyst Grants.
Guarantor
MB.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.