
Abstract
Objective
This study aimed to examine clients’ experiences with telehealth use for contraceptive implant consultation.
Methods
An online, self-administered survey was conducted with women who used contraceptive implants and faced adverse effects, inquired about side effects, or had concerns. Clients received consultations via LINE, which is a free chat application widely used in Thailand. Participants completed a questionnaire regarding their experiences and satisfaction within 7 days after using the service and a follow-up questionnaire to inquire about the need for in-person services 30 days after using the service.
Results
The participants were 200 women, with a response rate of 82%. Overall, 94% of participants were satisfied with the consultation. Moreover, 37.5% received a message response within 6 hours, and most (89.5%) got a response within 24 hours. The three most frequently reported symptoms were abnormal bleeding or spotting, mood swings, and itching or pain at the surgical site. Most adverse effects were managed through online consultation. Approximately one-third of the participants required in-person visits 30 days after telehealth consultation.
Conclusions
Telehealth consultation for contraceptive implant follow-up resulted in high client satisfaction. Most adverse effects could be managed using telehealth services. Therefore, telehealth could ensure sustained accessibility to reproductive healthcare during and post-COVID-19.
Keywords
Background
Contraceptive implants are a form of favorable long-acting reversible contraception (LARC). 1 They continuously release extremely low levels of progestin into the blood and prevent conception by stopping ovulation, increasing cervical mucus, and causing endometrial atrophy. 2 This safe and cost-effective contraception method offers women reliable contraception with a clinical success rate greater than 99% for up to 3–5 years.3–5 Although contraceptive implant use was previously low in Thailand, it is continuously increasing. According to the National Statistical Office of Thailand, contraceptive implants accounted for 0.4% of contraceptive methods among married women aged 15–49 years in 2009, 6 which increased to 1.6% in 2019. 7 This is especially true among adolescents, who receive government benefits and free contraceptive implants. There was a significant increase in the use of contraceptive implants among Thai teenagers from 2.5% in 2015 to 14.1% in 2019.7,8
Early discontinuation of contraceptive implants has been widely reported worldwide, which could put women at risk of negative health consequences.3,4,9,10 Unscheduled menstruation, prolonged bleeding or spotting, and other undesirable side effects, which can be managed successfully with over-the-counter medicine, 11 have been reported as a common cause for early discontinuation. 9 According to the US practice recommendations, insertion should be performed by trained healthcare professionals, with clear consultation regarding the possible adverse reactions and complications of the insertion procedure. Once the placement of a contraceptive implant has been confirmed, it does not necessitate the user's attention to maintain its high level of effectiveness. 3 However, post-insertion follow-up visits are common in Thailand. We believe that appropriate consultation and monitoring after insertion may reduce client concerns and mitigate early discontinuation rates.
During the worldwide health crisis caused by the COVID-19 pandemic, the social distancing policies were implemented aimed at minimizing physical interactions and preventing the spread of the virus, leading to the temporary suspension of various public and private activities, including medical services. Non-urgent care and elective procedures, including family planning and contraception services, were postponed. The COVID-19 pandemic has significantly impacted the utilization of LARC, especially insertion and removal procedures which required an in-person visit. 12 Approximately 20% of healthcare providers reported a cessation of both LARC insertion and removal procedures during the pandemic. 13 Healthcare providers have increasingly adopted telemedicine as a safe and effective means to deliver contraceptive counseling services.13–15 Telemedicine become a “new normal” type of medical service across various fields provided in Thailand in the wake of the COVID-19 pandemic, for example, home isolation of COVID-19 patients, noncommunicable disease and postpartum care.16–19
After the outbreak of COVID-19 in Thailand in June 2020, the Family Planning and Reproductive Health Clinic of King Chulalongkorn Memorial Hospital launched telehealth follow-up services via an official account using LINE, which is the most popularly used free chat application in Thailand. Based on data from Hootsuite Analytics in 2019, it was found that around 84% of internet users in Thailand were actively using LINE accounts. 20 Choosing to incorporate LINE into our service provides an additional benefit, as this platform enables users to exchange text messages and share photos. This feature allows for convenient and efficient communication between clients and our healthcare providers. This telehealth service was initiated to comply with the Thai government's social distancing policy and continue to provide effective family planning services. Our service is developed for assessing adverse effects after initiating contraceptive implants and offering general advice for contraceptive implants at no additional cost. During the COVID-19 pandemic, telehealth has been widely utilized in contraceptive services.15,21,22 However, previous studies have not assessed consultation for contraceptive implants via LINE. This study aimed to investigate the experience, satisfaction, and intention of contraceptive implant users regarding LINE consultation services. In addition, this study explored the participants’ preferred telehealth for contraceptive services. Our findings could facilitate healthcare providers, contribute to providing superior family planning services, and encourage the government to include telemedicine as part of contemporary family planning policies.
Methods
Study population and procedure
An online self-administered survey was conducted with women who initiated contraceptive implantation at the Family Planning and Reproductive Health Clinic of King Chulalongkorn Memorial Hospital between April 2022 and October 2022. Women who initiated contraceptive implant treatment and decided to undergo post-insertion follow-up via telehealth during the study period were eligible to participate. We included only clients who experienced adverse effects of contraceptive implant initiation and who used the services to inquire about side effects or concerns regarding contraceptive implants. These services were available at any time after contraceptive implant initiation, and clients could use the services more than once. This study only included the first episodes of clients who used the services. Within seven days of using the service, the clients received an invitation to the study via LINE message, and those who were interested discussed the information about the study via LINE. Participation was voluntarily, and participants were informed that they could withdraw from the study at any time. All participants provided electronic informed consent before participation. The first part of the questionnaire was distributed to all participants via LINE, and the follow-up questionnaire was distributed within 30 days of completing the first part. Participants who consented to participate but could not complete the questionnaire were reminded every three days, up to five times in total. Participants who completed the follow-up questionnaire received a compensation of 100 THB (approximately US$3.5). The confidentiality and anonymity of all participants were maintained throughout the study. We used electronic data capture tools hosted at Chulalongkorn University to collect data23,24 and conducted the study in accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board of the Faculty of Medicine at Chulalongkorn University (IRB 1025/64).
Study setting
During the study period, contraceptive implant initiation was fully reimbursed by the government for adolescents and those who underwent safe abortions. Partial reimbursement was provided to those residing in Bangkok. At the Family Planning and Reproductive Health Clinic of King Chulalongkorn Memorial Hospital, all women who initiated contraceptive implants were provided with the option to undergo seven-day post-insertion follow-up consultation via LINE or in-person visits at the clinic. Clients who decided to participate in telehealth follow-ups were provided a QR code to access the LINE account. When clients log into LINE, they receive an automated message regarding registration and an explanation of post-insertion services. According to the protocol of our telehealth service, all clients were asked to send in their contraceptive ID card, which included information regarding the type of implant used, day of initiation, and photo of the surgical site seven days post-insertion. In addition, they were offered online consultation services through LINE without additional fees. They could communicate with the staff through LINE, including text, audio, and video messages. Participants who received a consultation for post-insertion surgical site-related complications were asked to send photos of the implant site. Brief history-taking, including associated symptoms, underlying medical conditions, current medication, and concerns, was performed via chat. The medical consultation team (two trained doctors and two nurses) evaluated the client's history and implantation site using the photos. They provided all clients with suggested management strategies, including self-management or advising them to return for in-person visits. Self-management, such as changing dressings, performing cold compression at the surgical site, and taking pain relief medication, was advised as appropriate. One of the most common questions was regarding abnormal uterine bleeding or spotting, for which the consultation team performed comprehensive history-taking to assess the need for self pregnancy tests and endometrial sampling. 25 If history suggested bleeding or spotting from the contraceptive implant, with no medical history that prohibits combined oral contraceptives (COCs), 26 the team suggested COCs, which are over-the-counter medicine in Thailand, as the first option and ibuprofen 400 mg three times daily for seven days as an alternative. A follow-up message was sent to clients who inquire about this issue one week after consultation to assess treatment efficacy. Clients with persistent bleeding or spotting were requested to return to the clinic for a follow-up.
Questionnaire
An online self-administered questionnaire was modified from Stifani et al. with permission (2021) (Supplementary Material). 14 Two family planning experts (UJ and SS) approved the questionnaire. We translated all questions into Thai. A pilot test was conducted to check comprehension with the patients. A reliability test was performed using the test-retest method, which produced a score of 0.8–0.9. The first part of questionnaire included participants’ sociodemographic characteristics, issues for which they were seeking consultation, telehealth consultation characteristics, experience and satisfaction with family planning services, preferred telehealth services, and intention to access reproductive healthcare via telehealth. The questionnaire assessed the ‘participants’ satisfaction with the telehealth services for post-insertion consultation, and responses were rated on a five-point Likert scale (1 = very dissatisfied; 5 = very satisfied). 27 The follow-up questionnaire inquired whether an in-person visit regarding the original issue was required within 30 days after using the telehealth service, and if so, the reason for this visit.
Statistical analysis
We used Stifani et al. 14 as references to calculate the required sample size. Stifani et al. 14 reported that 86% of the participants were “very satisfied” with telemedicine consultations; therefore, the sample size was calculated assuming a less than 5% probability that tested data could have occurred under the null hypothesis. Thus, a sample size of 200 was considered sufficient. 28 SPSS Statistics version 22 was used for data analysis. All continuous data were presented as mean with standard deviation (SD), where categorical data were presented as frequencies with numbers and percentages.
Results
A total of 244 women met the eligibility criteria and were invited to participate, and 200 respondents completed the first questionnaire, with a response rate of 82.0% (Figure 1). Of these, 190 (95%) completed the follow-up questionnaire, with a response rate of 77.9% (Figure 1). Participant characteristics are listed in Table 1. The participants’ ages ranged from 15 to 48 years, with a mean (SD) age of 27 (7.1) years. The ethnicity of all participants was Thai. Nearly half of the participants (47%) had a bachelor's degree, followed by 35% with a high school or lower education. Moreover, 44% of the participants reported being married. Most participants were nulliparous. More than half of the participants reported receiving interval insertion of contraceptive implant (61.5%), and only one received an implant after an abortion. One-fifth of the participants initiated contraceptive implants in the early postpartum period, including 11% in the immediate postpartum period and 9.5% 4–6 weeks after the postpartum period, whereas 17.5% were continuous contraceptive implant users. Nearly half of the participants (47.5%) initiated contraceptive implantation because they required more effective birth control methods. Most participants (63%) received contraceptive implants free of charge through the government policy.
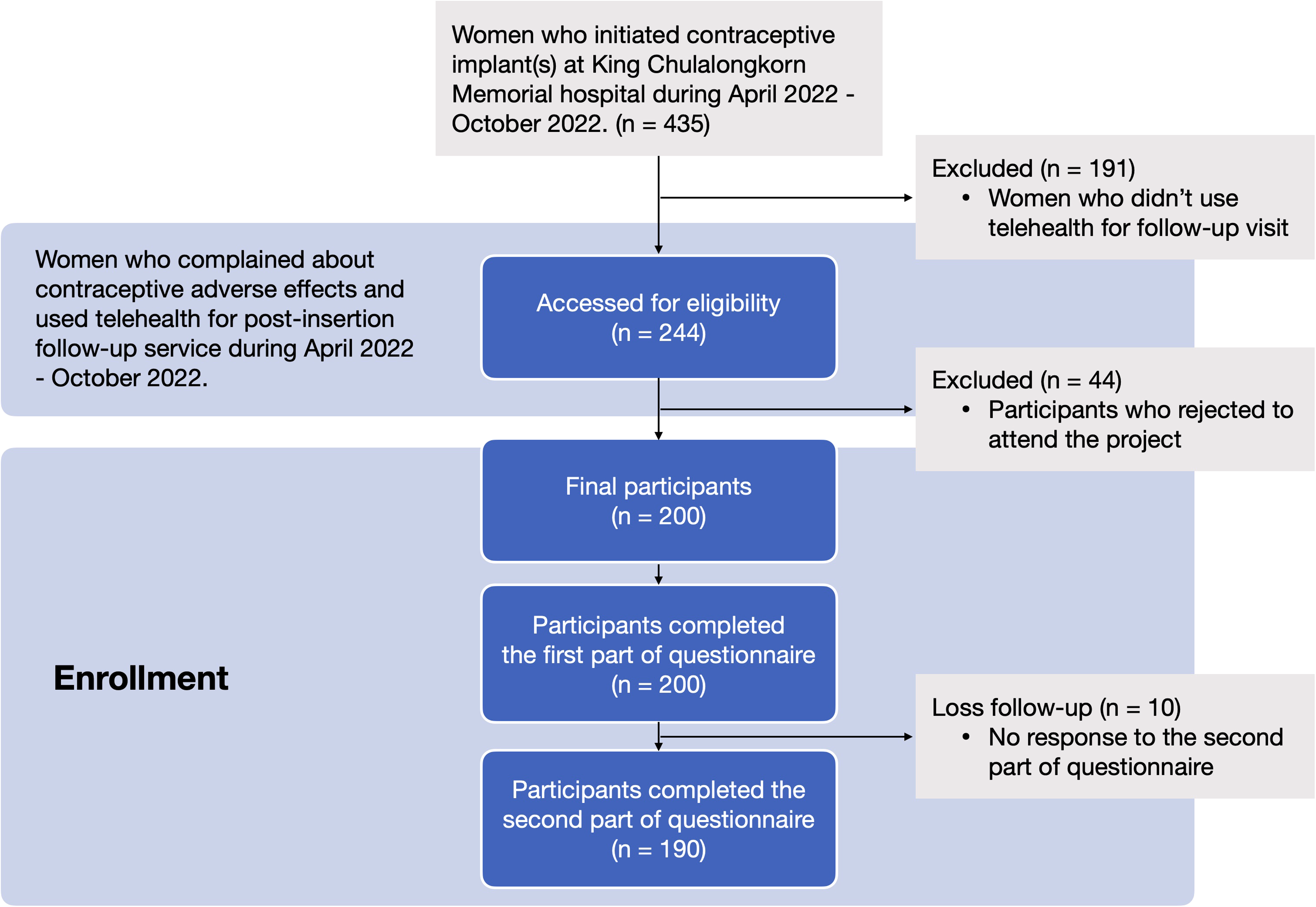
A flow chart of recruiting participants.
Basic characteristics of participants (N = 200).

Others: unemployed, freelance, working with studying.
1 USD = 33.8 THB.
Furthermore, 61 participants (30.5%) experienced adverse effects from contraceptive implants and used the service to find a solution. Nearly 30% of the participants complained of complications at the contraceptive implant surgical site, whereas most (37.5%) participants inquired about other implant-related issues. The three most frequently reported adverse effects were abnormal bleeding or spotting, mood swings, and itching or pain at the implant site. In addition, the participants reported minor adverse effects, such as amenorrhea, acne, breast tightness, headache or dizziness, and weight gain or loss. The most common complication was a small ecchymosis at the surgical site. Moreover, itching due to adhesive use and numbness in the affected arm were mentioned. Approximately one-third (33.5%) of the participants inquired when they could return to sport-related activities, such as diving, yoga, and weightlifting. Out of 45 cases of abnormal bleeding or spotting, half were reassured that changed menstruation patterns are common among contraceptive users. The remaining participants were advised to use over-the-counter medicine, including COCs and ibuprofen. Three participants were instructed to come in for in-person visits with their gynecologists due to heavy menstrual bleeding that may not be associated with contraceptive implant use.
Most women reported using the call function of mobile phones (94%) and chat applications (91%) for their daily life communication (Supplementary Table 1). Approximately 80% of participants primarily sought family planning advice via search engines, such as Google. Several participants sought in-person consultation. Most participants (89.5%) received message responses from medical staff within 24 hours, and 37.5% received responses within six hours. The majority of participants (95.5%) used the telehealth consultation service at home, and smartphones were the most common device (90%) (Table 2). Most (94%) participants expressed being satisfied with the family planning consultation via LINE, and 132 reported being “very satisfied” (Graph 1). The telehealth service met approximately 60.5% of the participants’ needs, and they did not require an in-person visit (Graph 2). Moreover, half of the participants were concerned about their privacy during online consultation.
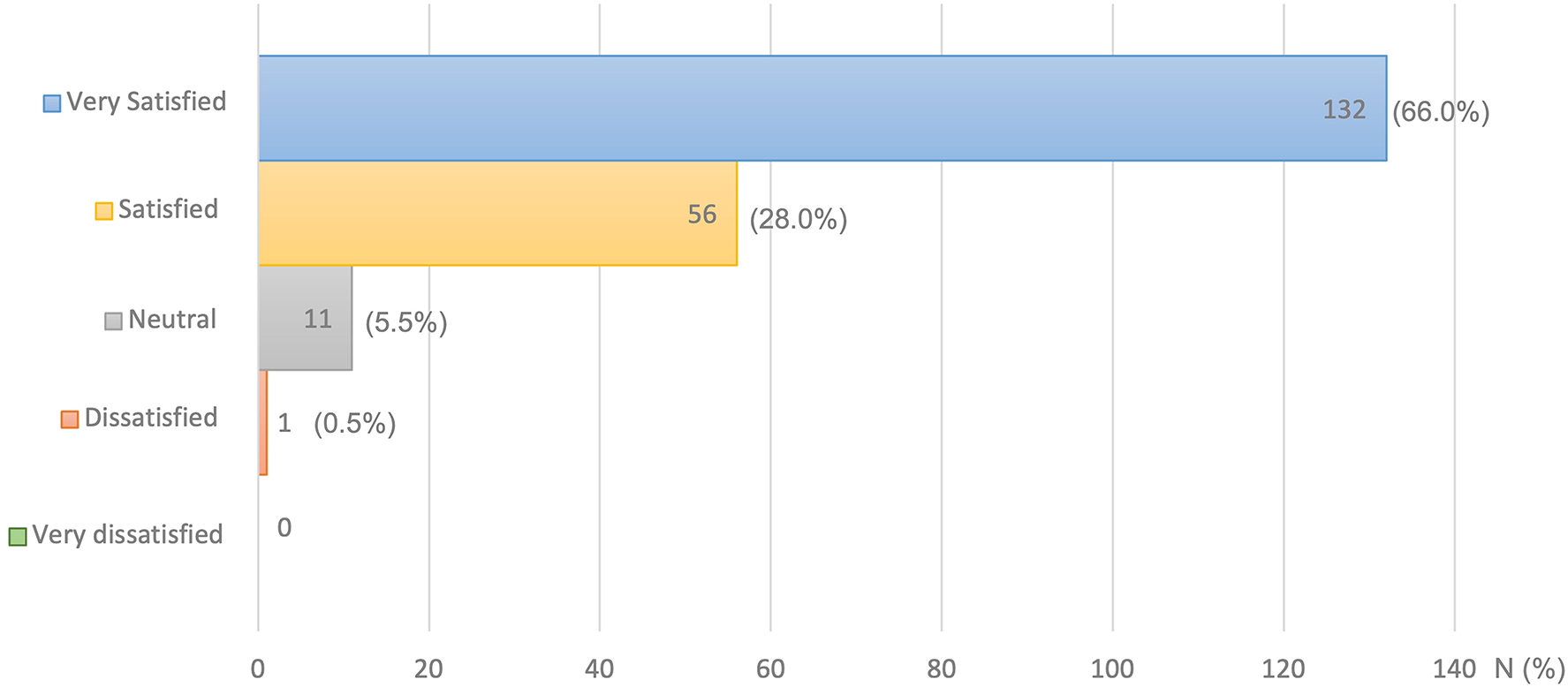
Satisfaction in family planning counseling and contraceptive implant post-insertion follow-up service via telehealth (N = 200).

The counseling via telehealth completely meet their needs (N = 200).
Experience in family planning counseling via “Line OA.”

Others: hospital, personal car.
The participants indicated that chatting via text messages or exchanging photos via LINE were their most preferred telehealth methods for contraceptive follow-up. Video calls and medical care mobile applications, such as the Chulalongkorn Hospital Care application, were also reported as acceptable. In addition, 34% of the participants required a response within one hour, and 18.5% required an immediate response. To assess the possibility of providing rapid responses, we asked the participants whether chatbot message response should be part of subsequent contraceptive telehealth, and 45% of the participants responded positively (Table 3). Moreover, we inquired regarding the extension of telemedicine to other reproductive health services, such as contraceptive methods, adverse effects from other contraceptives, preconception consultation, and provision of abortion medication. Most participants responded positively to incorporating further telehealth interventions as part of healthcare services. Furthermore, 153 participants (76.5%) indicated that telehealth consultation for adverse effects of contraceptive use was their most preferred service.
Ideal telehealth.

Of 190 participants who completed the follow-up questionnaire, 69 (36%) required in-person visits within 30 days of using the service. Most (94.2%) of the participants who required in-person visits needed more information regarding adverse effects of contraceptive implants, and three participants (4.3%) requested early discontinuation of contraceptive implants (Table 4).
In-person visit after 30-day telehealth counseling service.

Discussion
This study demonstrated that most clients were highly satisfied with telehealth consultations for post-insertion contraceptive implant follow-up. While there was no prior report specifically addressing satisfaction with telehealth for post-insertion contraceptive implant counseling, a previous study indicated that 81% of clients who received reproductive health counseling through telehealth during the COVID-19 pandemic reported being satisfied with this service. 29 Consistent with a previous report conducted prior to the pandemic, where 97% of respondents reported being either very satisfied or satisfied with the telehealth option for contraceptive care. 30 More than half of our clients thought that telehealth could replace in-person follow-up visits without disadvantages. Many factors could explain this high satisfaction rate. In addition to providing comprehensive consultation by trained healthcare providers, satisfaction with these telehealth services may have been because most adverse effects were minor and could be managed through observation. As previous reports have indicated that patients across various disease domains are inclined to continue utilizing telehealth consultations,31–36 following the COVID-19 pandemic. However, it is important to note that when it comes to surgical cases, only one-third of patients have expressed their agreement to continue using telemedicine. 37 Abnormal bleeding or spotting was the most common side effect of contraceptive implants. If it occurs after a thorough pelvic examination and cervical cancer screening post-insertion, it is suspected to be a hormonal side effect. It may not require an in-person visit for a repeat physical examination. Abnormal bleeding or spotting occurred in approximately one-fourth of the participants. Moreover, abnormal bleeding was the most common reason for contraceptive implant discontinuation in Thailand9,38–40 and globally. 41 This study revealed that over 90% of cases involving abnormal uterine bleeding after contraceptive implant insertion could be effectively managed using telehealth services. Providing adequate information and reassurance to clients and suggesting over-the-counter hormonal medication was sufficient. However, we recommend using over-the-counter medications only for young patients who exhibit a vaginal spotting pattern and have no contraindications for hormonal use based on the medical eligibility criteria for contraceptive use. If persistent or recurrent bleeding occurs, we recommend in-person visits for further investigation. A previous cohort study showed that half of bothersome uterine bleeding beyond patient expectations resulted in medical management, with a similar initiation rate for in-person and telehealth consultation. 42
Short waiting time is another important factor that influences client satisfaction. Most participants received a response within 24 hours, which may be compatible with non-urgent issues, such as contraceptive services. However, while most participants indicated that a response within 12–24 hours was acceptable, half of the participants thought that the ideal response time should be within 1 hour. Rapid responses could improve satisfaction with telehealth services. Regardless of the mode of telemedicine used (synchronous or asynchronous), high levels of satisfaction were consistently observed in various types of telehealth services. 43 Understanding client needs can help develop telehealth services that meet individual needs and preferences. It is important to continue evaluating the effectiveness and satisfaction of these services to ensure that they meet client needs. Furthermore, the participants’ digital literacy may explain the high satisfaction rate, as most participants used mobile phones daily and chat messages as one of their main communication venues. In addition, the COVID-19 pandemic has enhanced the acceptance of novel digital health platforms.14,44,45 Moreover, as the clinic was located in the center of Bangkok, this could be a contributing factor to the participants’ satisfaction, as most people could access the Internet via their mobile phones in this area. In addition, the use of LINE, which is Thailand's most popular chat application, likely influenced the participants’ satisfaction. Most (94%) of the participants used LINE in their daily lives, with slightly higher rates than data reported by Hootsuite Analytics 2019, which indicated that approximately 84% of Thai Internet users have active LINE accounts. 20 The participants reported that their preferred telehealth services included active text and photo messages, which can be provided by LINE. We suggest that regularly using digital platforms in daily life and familiarity with responses might enhance acceptance. As reported in various studies, the utilization of social networking sites such as Facebook and WhatsApp, which are commonly used across different countries, has shown potential to improve contraceptive knowledge and promoting a significant increase in the utilization of long-acting reversible contraceptives (LARCs) compared to conventional education programs.46–48
Privacy concerns regarding the use of telehealth services must be considered. Half of the participants reported that they were concerned about privacy, and several participants reported being very concerned. However, this study did not explore specific privacy concerns. Telehealth-related data privacy and security concerns have been reported worldwide.49–53 Different contexts of telehealth produce various concerns, such as the use of video recording, sensitive personal information, and data leakage. Some telehealth users are concerned that the application developer may collect and use their data. 53 Adequate security and privacy protection, clear declarations, and informed consent may create trust and reduce client concerns. The use of a reliable telehealth platform is an important aspect of security.
However, post-insertion follow-up visits are not necessary, according to recommendations of the Centers for Disease Control and Prevention. 54 Cultural and contextual differences exist between Thailand and the United States regarding follow-up services after surgical procedures. At our clinic, we recommend one-week and three-month post-insertion follow-up visits for all women who receive contraceptive implants. The primary purpose of these follow-up visits is to effectively manage any side effects that may occur after insertion, such as unscheduled menstruation, prolonged bleeding or spotting, and other undesirable effects that have been reported as common causes for early discontinuation.9,38–41 By addressing these side effects promptly, we aim to mitigate early discontinuation rates, which can have a significant impact on contraceptive effectiveness. The observed rate of contraceptive implant discontinuation within the first year of use in our clinic was 2.3 per 100 person-years, 9 which is notably lower than the previously reported rate of 8.9% in a previous study conducted in Thailand, 38 as well as the reported global average of 9%. 55 Although the specific causes cannot be determined solely from our follow-up visits, they are likely contributing factors to this favorable outcome.
Before the COVID-19 pandemic, all our follow-up visits were conducted in-person. Telehealth has been used in several contraceptive services since the onset of the COVID-19 pandemic.15,21,22 In our clinic, as well as Thailand, telehealth has emerged as a groundbreaking service for both healthcare providers and clients. However, within the cultural context, a significant proportion of clients still express reluctance to embrace telehealth as a substitute for in-person visits. Our study, during the designated period, revealed that approximately 45% of clients (191/435) declined the utilization of the telehealth services we offered. On the other hand, our telehealth consultation service has shown the potential to reduce in-person visits by approximately two-thirds of clients within a 30-day period. As previously reported, from a patient's perspective, the most common advantages of telehealth include time saved due to reduced traveling and waiting times, improved accessibility to healthcare services, enhanced convenience, and cost efficiency. 43 Due to the increasing trend of contraceptive implant use in Thailand,6–8,56 telehealth services may reduce the clinic cloud while providing convenient and efficient care. The COVID-19 pandemic has negatively impacted LARC insertion and removal and caused a significant increase in the use of telehealth for contraceptive services. 13 Furthermore, telehealth improves the continuity of contraceptive use. 45 Despite this, digital platforms for contraceptive services are limited and contribute to only a minor part of public healthcare in Thailand. The disruption of healthcare during the COVID-19 pandemic forced healthcare providers to rapidly expand telehealth services to continue providing contraceptive care while limiting viral exposure. Telehealth via LINE could be integrated as a part of contraceptive implant services and replace routine in-person follow-up visits, which were standard before the pandemic, as providing adequate information, assessing, and correcting side effects may promote contraception continuation.57,58
Our study specifically targeted the contraceptive implant service, as it has the potential for surgical site complications after insertion and the need for intervention to address associated side effects. Another reason is that most contraceptive implant cases were supported by government policies that provided them free of charge, as part of efforts to reduce unintended pregnancies. Therefore, our telehealth services were designed to minimize early discontinuation rates and maximize the cost-effectiveness of the government policy. In this regard, telehealth via LINE offers a valuable solution by enabling clients to share photos for evaluation and assessment of any such complications. The participants reported that telehealth services via LINE to evaluate surgical site complications after contraceptive implantation and adverse effects of contraceptive implant use were effective and highly satisfactory. This was an adjunct service in response to social distancing policies in Thailand during the COVID-19 pandemic. This service helped reduce client anxiety and the need for in-person visits. Approximately two-thirds of clients did not require in-person visits 30 days after consultation. Most participants stated that they would use telemedicine for contraception after the COVID-19 pandemic. This was in line with previous studies in the United States, which reported positive experiences with telemedicine for contraceptive consultation.14,44,45 The participants appreciated the convenience of telemedicine visits and receiving information regarding contraceptive options.
This study had several limitations. First, this study did not conduct a comparative follow-up for long-term outcomes, such as discontinuation and continuation rates, and changes in satisfaction and acceptance. This information may be important for the development of digital platforms for contraceptive telehealth services. Second, this study did not provide insight into the sustainability of the services. Our services were provided free of charge. Healthcare providers dedicated their time beyond their regular hours to provide telehealth services without compensation. Therefore, for long-term viability, it is necessary to evaluate the cost-effectiveness of the services. The client's satisfaction may differ if there are cost differences associated with telemedicine and in-person follow-up services. Third, the telehealth service was not a real-time interaction, and there was no limit regarding the response time. This may affect satisfaction with the telehealth service. Furthermore, 17.1% of eligible clients did not respond to the survey, which may have been due to selection bias. However, we compared the demographic characteristics of the respondents and non-respondents and found no difference in the selection for participation. Finally, this study was conducted during the COVID-19 pandemic, when telehealth services were novel and rapidly expanding. As remote healthcare service increased, this may have caused reluctance to seek in-person services. In addition, the severity of the COVID-19 outbreak may have affected client satisfaction, as telehealth facilitated social distancing. While previous reports have indicated high levels of satisfaction with the telehealth option for contraceptive care before the pandemic, 30 it is important to acknowledge the differences in cultural and contextual factors between countries. Therefore, future studies should focus on evaluating telehealth services specifically in the context of Thailand after the pandemic, taking into account the unique cultural considerations that may influence the acceptance and effectiveness of such services.
Nevertheless, this study reported experiences with contraceptive telemedicine services from the client perspective, which is novel information for reproductive health services in Thailand. We implemented a clear workflow system and assigned staff to individual clients until the end of the follow-up period. We utilized a consultation protocol in which each staff member could provide the same information pattern to every client. For any complicated questions or adverse events, nurses were required to consult a doctor before answering the client. This service was available free of charge via LINE, which is the most popular chat application in Thailand, eliminating the barrier to telemedicine service access. In addition, this study assessed the participants’ preferred telehealth services. Mobile applications with rapid responses have the potential to improve contraceptive telemedicine services. Further studies could determine the factors that impact the acceptance and accessibility of telemedicine services to improve user satisfaction.
Conclusions
The participants were highly satisfied with telehealth follow-up consultation for contraceptive implants. Most adverse effects were managed using telehealth services. Telehealth could replace in-person follow-up visits and ensure sustained accessibility to reproductive healthcare during and after the COVID-19 pandemic.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231203877 - Supplemental material for Client experiences with telehealth using LINE for consultation and assessment of adverse effects of contraceptive implants during the COVID-19 pandemic in Thailand
Supplemental material, sj-docx-1-dhj-10.1177_20552076231203877 for Client experiences with telehealth using LINE for consultation and assessment of adverse effects of contraceptive implants during the COVID-19 pandemic in Thailand by On-anya Phianphitthayakul, Jiayu Li, Ratthapong Rongkapich, Parichart Karroon, Jarika Vatrasresth, Unnop Jaisamrarn and Somsook Santibenchakul in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231203877 - Supplemental material for Client experiences with telehealth using LINE for consultation and assessment of adverse effects of contraceptive implants during the COVID-19 pandemic in Thailand
Supplemental material, sj-docx-2-dhj-10.1177_20552076231203877 for Client experiences with telehealth using LINE for consultation and assessment of adverse effects of contraceptive implants during the COVID-19 pandemic in Thailand by On-anya Phianphitthayakul, Jiayu Li, Ratthapong Rongkapich, Parichart Karroon, Jarika Vatrasresth, Unnop Jaisamrarn and Somsook Santibenchakul in DIGITAL HEALTH
Footnotes
Acknowledgements
Availability of data and materials
The datasets used and/or analyzed during the current study available from the corresponding author on reasonable request.
Contributorship
OP contributed to the literature review, study concept design, primary manuscript drafting; JL was involved in the primary manuscript drafting and editing; RR contributed to the statistical analysis; PK contributed to the data acquisition; JV contributed to the manuscript editing and revision for intellectual content; UJ contributed to the study concept design; and SS contributed to the study concept design, data acquisition, manuscript editing, and revision for intellectual content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University (IRB 1025/64) and was conducted in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Somsook Santibenchakul.
Informed Consent
All women signed and dated written electronic informed consent forms approved by the Faculty of Medicine, Chulalongkorn University Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.