
Abstract
Background
COVID-19 forced a rapid transition to telehealth. Little is known about the use of telephone versus video visits among people living with or at risk for HIV (PWH).
Setting
We studied electronic health record data from an urban HIV clinic. Our sample included visit- and person-level data. Visit-level data came from appointments scheduled from 30 March 2020 to 31 May 2020. Person-level data came from patients 18+ years of age who completed at least one telephone or video visit during the period of interest.
Methods
We performed a cross-sectional analysis. Our primary outcome was telehealth modality (telephone or video). We compared visit completion status by telehealth modality. We evaluated associations between patient characteristics and telehealth modality using logistic regression.
Results
In total, 1742 visits included information on telehealth modality: 1432 telephone (82%) and 310 (18%) video visits. 77% of telephone visits were completed compared to 75% of video visits (p = 0.449). The clinic recorded 643 completed telehealth visits in April and 623 in May 2020. The proportion of telephone visits decreased from 84% in April to 79% in May (p = 0.031). Most patients participated in telephone versus video visits (415 vs. 88 patients). Older age (adjusted odds ratio [AOR] 3.28; 95% confidence interval [CI], 1.37–7.82) and Black race (AOR 2.42; 95% CI, 1.20–4.49) were positively associated with telephone visits. Patient portal enrollment (AOR 0.06; 95% CI, 0.02–0.16) was negatively associated with telephone visits.
Conclusion
PWH used telephone more than video visits, suggesting that telephone visits are a vital healthcare resource for this population.
Introduction
On 11 March 2020, the World Health Organization announced the COVID-19 pandemic, prompting an immediate change in healthcare delivery. 1 Prior to the pandemic, telehealth was expanding but infrequently used in the United States: only 10% of providers had ever used telehealth, and only 14% of all care at the Veterans Health Administration was provided using telehealth.2,3 The Yale telehealth team had initiated several successful telehealth operations for years prior to the pandemic. 4 However, in the first weeks of the public health emergency in the United States, efforts to decrease the spread of COVID motivated a rapid increase in telehealth implementation for all outpatient workflows, 4 facilitated by emergency insurance regulation changes and coverage expansions, regulatory leniency for technological standards, and loosening of licensing permissions for telehealth care.5–8 This accelerated implementation of telehealth prompted concerns about disparities in telehealth access, especially as they impacted historically underserved populations. Studies early in the pandemic showed less telehealth use among older, female, and non-English-speaking patients.9–11 Trends in internet access showed slightly lower rates of internet adoption among older adults, Black and Hispanic populations, people with less formal education, and households with lower incomes. 12 Trends in internet use specifically for health information echo these findings. 13 Similarly, studies assessing the associations between patient sociodemographic characteristics and telephone or video visit use in primary care and specialty settings found that older adults, female, Black, Hispanic, and Spanish-speaking populations were less likely to use video visits.9–11,14,15 In fact, research suggests that minoritized populations and patients with less formal education are less likely than white populations to be offered the patient portal access through which much of telehealth, especially video visits, is administered. 16
There is a growing literature regarding the use of telehealth to provide care to people living with or at risk for HIV (PWH) and to those receiving pre-exposure prophylaxis (PrEP). PWH faced a number of challenges to in-person care before COVID including transportation issues, stigma, lack of insurance, and mental illness or substance use disorders.17–21 Access to telehealth visits was vital for PWH during the early phase of the COVID-19 pandemic because consistent healthcare engagement helps patients maintain lower viral loads and higher CD4 counts. 22 Furthermore, as these patients likely face psychosocial burdens including loneliness and stigma, it was imperative that they be able to receive continued multifaceted specialty care. 23 It is thus important to identify disparities in telehealth access that impact this population.
The digital divide is an important limitation to PWH's access to telehealth. Adults with lower income or less formal education are less likely to own a smartphone or to have access to broadband. 20 PWH are more likely than the general population to have lower socioeconomic status and to live in impoverished neighborhoods, and thus they likely experience reduced access to the technology and technological experience necessary to navigate video visits.18,24
Telephone consultations may provide a solution to this access problem, but only a limited number of studies report on video versus telephone consultations. 25
Our goal was to assess rates of telehealth modality (telephone or video) use in a clinic serving PWH. We also explored patient-level factors associated with telehealth modality use in this population during the early phase of COVID-19.
Methods
We performed a cross-sectional analysis using electronic health record data from an urban HIV clinic housed within a large academic health system in Connecticut. This clinic is the largest provider of comprehensive services to adults living with HIV within the state and provides multidisciplinary primary care for approximately 800 adults living with HIV and 200 adults at risk who take PrEP. The clinical team includes 16 part-time HIV specialist physicians, 2 advanced practice providers, 9 trainees (3 infectious disease fellows and 6 residents in the HIV primary care pathway), 3 HIV consultants (e.g., psychiatrist, neurologist, transplant physician), 1 pharmacist, 2 social workers, 2 nurses, 2 medical assistants, 1 medical case manager, and 1 front desk staff member. The clinic has a call center that assists in patient call triage and scheduling. Clinicians provide care through approximately 7500 medical visits per year. During the early months of the pandemic, the clinic team also consisted of students and other volunteers who helped patients enroll in and orient to the clinic's telehealth system. Nurses, front desk, and other staff assisted providers and patients with telehealth issues before and during visits as they were able. The healthcare system also held training sessions to teach staff how to best utilize video and telephone visits and to troubleshoot during visits.
We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cross-sectional studies.
Sample
We analyzed both visit- and person-level data. Visit-level data came from appointments scheduled at the clinic from 30 March 2020 to 31 May 2020 (N = 1742). We limited our research to the first 2 months of the pandemic to better understand patient choice regarding visit modality (video vs. telephone) when telehealth visits were the only option. We excluded visits for which the telehealth modality was unknown.
Person-level data came from adult patients 18+ years of age who completed at least one telephone or video visit during the period of interest (N = 503). We excluded patients who attended both telephone and video visits as there were very few patients in this category (N = 18). We also excluded patients who had only no-show, cancelled, or left without being seen for visits during this period.
Study variables
Our outcome of interest was telehealth modality: “telephone” for visits using audio methods only and “video” if using an audiovisual platform. Visit modality was recorded by front desk staff at the time of scheduling. Any visits missing information on type of telehealth visit (telephone or video) were excluded from the analyses. At the visit level, we categorized visits by visit completion status: completed, canceled, no-show, and left without being seen. 10 We then categorized visits by the month in which they were completed (April or May) to explore changes in telehealth modality use over time. For this analysis only, we excluded those visits that occurred in March as there were only 2 days in this month that were involved in the telehealth transition.
For the patient-level analyses, independent variables included self-reported age, sex, race, ethnicity, preferred language, need for an interpreter, and patient portal enrollment. All have been shown to be associated with telehealth use and are pertinent to questions of health equity.9,14,15 Age was categorized as young (18–44 years old), middle-aged (45–64), and older (65+). 14 Race was categorized as White, Black, or other race. Ethnicity was categorized as Hispanic, non-Hispanic, and other. Language categories included English, Spanish, and other.
Statistical analysis
For the visit-level analyses, we generated descriptive statistics using chi-square and Fisher's exact tests as appropriate to compare visit completion status by telehealth modality (telephone or video) and to compare telehealth modality by visit month.
For the patient-level analyses, we reported means and standard deviations for continuous variables and frequencies for categorical variables. We used t-tests to compare continuous variables and chi-square or Fisher's exact tests as appropriate to compare categorical variables. We then conducted multivariable logistic regression to identify factors associated with telephone visit use, including factors such as age, sex, race, ethnicity, preferred language, need for an interpreter, and patient portal enrollment.9,14,15 We presented adjusted odds ratios (AOR) with 95% confidence intervals (CI) and corresponding p-values. Statistical significance was set at p < 0.05. Analyses were performed using SAS 9.4 (SAS Institute).
Ethics
Our study was deemed to be exempt by the Institutional Review Board of Yale University School of Medicine (Protocol ID 2000028059), thus consent was not required.
Results
Visit-level analyses
A total of 2668 visits were scheduled at the clinic between 30 March 2020 and 31 May 2020. Of these, 926 were missing information on telehealth visit type (telephone vs. video) and were therefore excluded from the study. Of the 1742 remaining visits, 1432 telephone visits (82%) and 310 (18%) video visits were scheduled. Seventy-seven percent of telephone visits were completed compared to 75% of video visits (p = 0.449). No-show rates were significantly higher for telephone (8%) versus video visits (5%) (p = 0.025). Cancelation rates were significantly higher for video (20%) relative to telephone (15%) visits (p = 0.019).
The clinic recorded 643 completed telehealth visits in April and 623 in May 2020. The proportion of telephone visits decreased from 84% of all telehealth visits in April to 79% in May (p = 0.031).
Patient-level analyses
At the patient level, 503 unique patients completed a telehealth visit during the period of interest. Of these, 415 (83%) completed at least one telephone visit, and 88 (17%) completed at least one video visit (Table 1). Eighteen patients completed both telephone and video visits during the time of interest, and we excluded them from our study. These excluded patients differed from those we included in terms of patient portal enrollment (89% enrollment for patients who attended both modalities, 54% for those who attended only one modality, p = 0.003). Otherwise, there were no significant differences between the groups.
Patient characteristics by telehealth modality.

Missing = 1. bFisher's exact test.
Telephone was the most used telehealth modality regardless of age, race, preferred language, need for an interpreter, and enrollment in the patient portal. Those who had completed telephone visits were older than those who had video visits (54 ± 14 years vs. 47 ± 13 years, respectively, p < 0.001). They were more likely to be Black (45% vs. 24%, p < 0.001) or other race (21% vs. 11%, p < 0.001) and to require an interpreter (7% vs. 1%, p = 0.027). Patients attending telephone visits were less likely to be enrolled in the patient portal than those who used video visits (45% vs. 94%, p < 0.001).
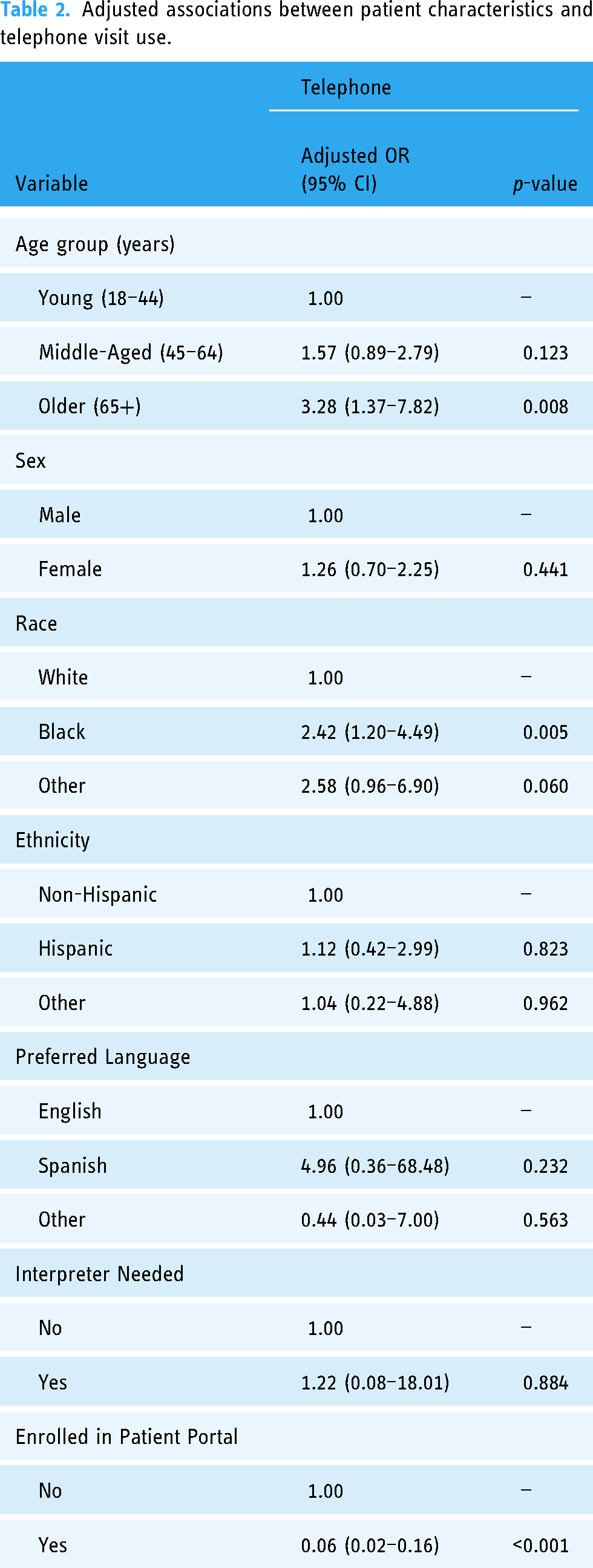
In multivariable analyses, age, race, and patient portal enrollment were significantly associated with use of a telephone visit (Table 2). Older patients (AOR 3.28; 95% CI, 1.37–7.82) and those of Black race (AOR 2.42; 95% CI, 1.20–4.49) had higher odds of telephone visits compared to patients who were under 45 years of age and those of White race, respectively. Patients enrolled in the patient portal had lower odds of completing a telephone visit compared to those not enrolled (AOR 0.06; 95% CI, 0.02–0.16).
Adjusted associations between patient characteristics and telephone visit use.
Discussion
In this study of telehealth modality use at an urban HIV clinic from March through May 2020, we found that telephone visits were far more common than video visits. There was a lower frequency of cancellations and a higher frequency of no-shows among telephone visits. Telephone visit use decreased from April to May but remained the predominant telehealth modality used. For patient-level analyses, we found that older age, Black race, and lack of patient portal enrollment were associated with use of telephone visits.
Our findings on the association between age and race with telehealth modality are consistent with those from HIV-specific clinics 18 and from other primary care and specialty clinics during the COVID-19 pandemic.9–11,14,15 The older population faces unique barriers to video visits including hearing and visual impairment, and limited technological experience. 26 Black patients are less likely than white patients to have access to broadband internet and may be less likely to use personal health technology to manage their healthcare.12,13,27 Given that older age and Black race are associated with a greater likelihood of telephone use, failure to provide telephone visits could result in the exclusion of vulnerable patients from care. There is also evidence that telephone visits facilitate access to care; the lower cancellation rate among telephone visits compared to video visits within our study may suggest that telephone visits are an accepted visit modality in the PWH population. 28 For these reasons, and because cost is a common barrier to care for PWH, it is vitally important that telephone visits be covered by insurance and that they be covered at rates commensurate with other telehealth modalities. 29
While measures to expand broadband networks or telehealth infrastructure have been implemented in recent years, our research suggests that they are insufficient for achieving video visit use.30,31 Many patients who used telephone visits were enrolled in the patient portal, suggesting that they had access to the technology necessary for video visits but still preferred telephone to video visits. Furthermore, telephone remained the main visit modality through April and May. It may be that while patients could be signed up for the portal, they lacked the knowledge and/or internet access required to use video technology. Alternatively, research suggests that clinic and provider factors, such as video infrastructure or biased assumptions about which patients can attend video visits, may be more important than patient preference in determining telehealth modality. 14 Clearly, more research is necessary to explore reasons for selecting specific telehealth modalities. However, reimbursement parity for telephone visits and technological education for both patients and providers must be part of the solution to optimize telehealth. As telehealth becomes a more integral part of healthcare, multiple modalities should be available so that providers do not discriminate against those who are unable to or who prefer not to use video technologies.
More research—both qualitative and quantitative—is required to further explore telehealth modality use among PWH. In qualitative studies, researchers have shown that both PWH and their healthcare providers have favorable attitudes toward using telehealth.20,32 Future studies should investigate why patients use telephone rather than video visits even when they have access to the necessary technology. Quantitatively, researchers have begun to study the impact of telehealth on CD4 counts and viral load, but no studies have looked at the effects of telephone versus video visits on such outcomes. 33 More evidence is required to determine the effectiveness of telephone or video visits in improving patient outcomes and the best use of each modality for various aspects of the chronic disease cascade. Furthermore, as telehealth becomes increasingly ubiquitous, studies should investigate trends in long-term modality use to best inform care for this population. Existing research suggests outcomes similar to those in our study, but more data are needed to ensure this at-risk population receives optimal care. 34
Our study had several strengths. We were able to include a larger number of patients (N = 503) and telehealth visits (N = 1742) than had been included in other, comparable studies of PWH. 18 In addition, clinic providers included PAs, APRNs, RNs, MDs, and social workers, making our findings applicable to multiple healthcare disciplines. Furthermore, our study period included only telehealth visits, eliminating possible complications from co-occurring in-person visits.
Our study also had notable limitations. First, 35% of scheduled visits during this period were of unknown telehealth modality. This was likely a product of the rapid telehealth transition faced by the clinic: providers and staff were initially unsure of how to schedule and document telehealth visits. Second, the number of telephone visits was likely underestimated, as some visits scheduled as video visits may have been switched to telephone at the time of the appointment. Third, we were unable to assess the impact of factors such as insurance coverage, income, or internet access, which prior research suggests are associated with telehealth use. We were also unable to assess the impact of differences in insurance reimbursement for video versus telephone visits. These factors should be investigated in future studies. Fourth, we could not elucidate what barriers our patients may have faced in attending a video visit, including improper technology, lack of broadband access, insufficient technological knowledge, or personal preference. It is also unclear if clinic factors (e.g., facility internet, provider technological skill or preference, availability of timely technical assistance, differences in reimbursement, and healthcare system preference) influenced visit modality. Finally, we studied a single urban clinic in a large academic institution with extensive resources available to help clinics make the transition from in-person to telehealth care. Our results may not be generalizable to non-academic or rural settings.
Conclusions
The COVID-19 pandemic forced rapid change in clinical practice. Telehealth expansion provided a chance for patients and providers to safely connect amidst an uncertain public health crisis. It also provided researchers a unique opportunity to study this previously limited practice modality, bringing to light inequities and repercussions which might otherwise have remained hidden. Our study found that PWH used telephone visits more than video visits to engage in care. We also found that differences in age and race were associated with telephone visit attendance, which is consistent with the results of similar studies from different populations. As the use of telehealth continues, we must continue to seek opportunities to provide more efficient, safe, and accessible care.
Footnotes
Acknowledgments
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of NIH.
Contributorship
HC and JAW researched literature and conceived the study. HC and AA conducted the data analyses. KHW and HP accessed the data and provided it in analyzable form. RGC, MV, PH, and LAB provided clinical and health system context for this work and contributed to interpretation of the data. HC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was granted an exemption by the Institutional Review Board of the Yale University School of Medicine (#2000028059) and is HIPAA compliant.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01 AR078715 granted to Julie A. Womack), the National Center for Advancing Translational Sciences (TL1 TR001864 granted to Andrew Arakaki), and Doris Duke Charitable Foundation and U.S. National Library of Medicine (R01LM013477 and G08LM013801 granted to Karen H. Wang).
Guarantor
JAW.