
Abstract
Objective
Augmented reality (AR) is a relatively new technology that merges virtual and physical environments, augmenting one's perception of reality. AR creates a computer-generated environment that evokes a unique perception of reality, where real and virtual objects are registered with one another, which operates interactively and in real time. Recently, the medical application of AR technology has dramatically increased with other assisted technologies, from training to clinical practice. The ability to manipulate the real environment extensively has given AR interventions an advantage over traditional approaches. In this study, we aim to conduct a systematic review of the use of AR to have a better understanding of how the use of AR may affect patients with mental health-related conditions when combined with gamification.
Method
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines by searching Pubmed and Web of Science databases.
Results and Conclusion
We identified 48 relevant studies that fulfill the criteria. The studies were grouped into four categories: Neurodevelopmental disorders, anxiety and phobia, psychoeducation & well-being, and procedural & pain management. Our results revealed the effectiveness of AR in mental health-related conditions. However, the heterogeneity and small sample sizes demonstrate the need for further research with larger sample sizes and high-quality study designs.
Keywords
Introduction
Augmented reality (AR) is a relatively new technology that blends virtual and physical environments, enhancing one’s perception of reality. 1 Unlike virtual reality, which creates a computer-generated environment that evokes a unique perception of reality, real and virtual objects are registered in AR, which operates interactively and in real time. 2 Recently, the medical application of AR technology has dramatically increased, as demonstrated in the increased number of publications, 3 with various assisted technologies used for training and clinical practice such as surgical procedures, 4 psychiatric treatments, 2 and nursing practices. 5 The ability to manipulate the real environment extensively has given AR interventions an advantage over traditional approaches. This technology is easily gamified, especially for children, which can increase their attention span and enthusiasm for using it.
AR has become a helpful tool for diagnosis, treatment, and management in the mental health area due to its flexibility and increased accessibility. It can be conveniently delivered through various platforms, including smartphones and tablets. 6 Integrating this technology into mental health encompasses a wide range of fields. For instance, AR has been used for phobia exposure therapy with similar efficacy and lower refusal rates. 7 Additionally, AR has been used for general well-being via serious games, exercise, and psychoeducation interventions. 8 However, Although the use of AR is promising, the updates take time to follow. The devices are diverse in hardware and software, which can affect the study results. 9 The application of AR requires a multidisciplinary team that includes clinicians, engineers, and software developers. 10 Besides, cybersickness, tiredness, and dizziness have been reported in previous studies. 11
In the pediatric population, AR and new technologies were studied for the intervention of neurodevelopmental disorders that include autism spectrum disorder (ASD), attention-deficit hyperactivity disorder (ADHD), and intellectual disabilities (ID). Studies demonstrated that serious games and virtual reality interventions could improve the daily functioning of children and enrich their academic learning experience.12,13 Although AR is relatively less studied than other technologies, its gamification and easy application to traditional management modalities have made it a focus of research. 14 AR technology has the potential to enhance various cognitive and emotional processes, social communication, and theory of mind skills, including facial emotion recognition and attention, as well as functional and motor abilities. 6 The other important area for AR in pediatric populations is procedural and pain management. Children usually experience significant anxiety while encountering medical professionals and undergoing procedures. 15 Although the mainstream management is sedation and analgesia for pediatric procedures, the literature has demonstrated that children who participated in psychological programs were better able to control their anxiety and display lower levels of worry. 16 Studies have shown that new technologies, such as virtual reality, can be an effective tool for pediatric hospital settings compared to standard care; however, they are still not frequently used in routine practice. 17
This study aims to determine the extent of AR usage in mental health conditions and evaluate its effectiveness in treating such conditions. Based on our investigation of the current literature, AR has primarily focused on specific mental health-related areas. Therefore, we classified our findings into four main areas: 1. Anxiety & Phobias, 2. Neurodevelopmental Disorders, 3. Psychoeducation & Well-being, and 4. Procedural & Pain management in this review. We hypothesize that when used in conjunction with evidence-based approaches, AR is an effective intervention tool in the mental health area with significant potential for growth and many advantages.
Methods
This systematic review was conducted following the PRISMA guidelines. 18 The protocol of this systematic review was not registered.
Search strategy
The bibliographic search was conducted on two databases by two independent authors, Web of Science and Pubmed, on 28th April 2022. The search terms used included phrases such as: ((“augmented reality”) OR (“mixed reality”) AND (storytelling OR gaming OR play OR intervention OR therapy OR psychotherapy OR psychoeducation OR psychiatry* OR treatment OR relaxation OR psychosocial OR “procedural support” OR consultation OR support OR “child life” OR “play therapy” OR “medical play” OR “cognitive behavioral therapy” OR CBT OR Emotion* OR therapeutic* OR psychology* OR mental) AND (Child* OR Adolescent OR Teenage* OR adult OR patient OR individual OR participant OR parent)).
Eligibility criteria
Articles in English that meet the following criteria were included without publication date limit in April 2022: Treating or alleviating a mental health condition with AR or improving well-being; Symptoms controlled with before and after the use of AR or compared control group when possible.
Our exclusion criteria include reviews that did not present original research; Studies that included geriatric population; Conference abstracts, editorials, commentaries or opinion pieces, case reports, preprints, and study protocols; Studies that are not published in a peer-reviewed journal; Studies that are not written in English.
Two independent authors screened and selected the studies that are eligible for inclusion, the final selection of the articles was determined through a joint meeting involving all authors to reach a consensus for conflicts.
Data extraction
Two independent authors extracted the following relevant data from the eligible studies: The author, year, title, the study’s aim, design, sample size, groups, age range, intervention, assessment tools, and outcome.
Quality assessment of the studies
We used The Joanna Briggs Institute (JBI) critical appraisal tools to assess the quality evidence of the included studies. 19 We used JBI Critical Appraisal Checklist for Randomized Controlled Trials, JBI Critical Appraisal Checklist for Quasi-Experimental Studies, and JBI Critical Appraisal Checklist for Cohort Studies tools according to the design of the study. Two independent reviewers performed a critical appraisal of the included studies. In cases of disagreement, a third author made the final decision following a discussion to reach a conclusion. The critical appraisal results are given in Supplementary Tables 1 and 2. The studies with survey design were not included in the quality assessment.
Characteristics of the studies investigating the effect of AR on ASD.
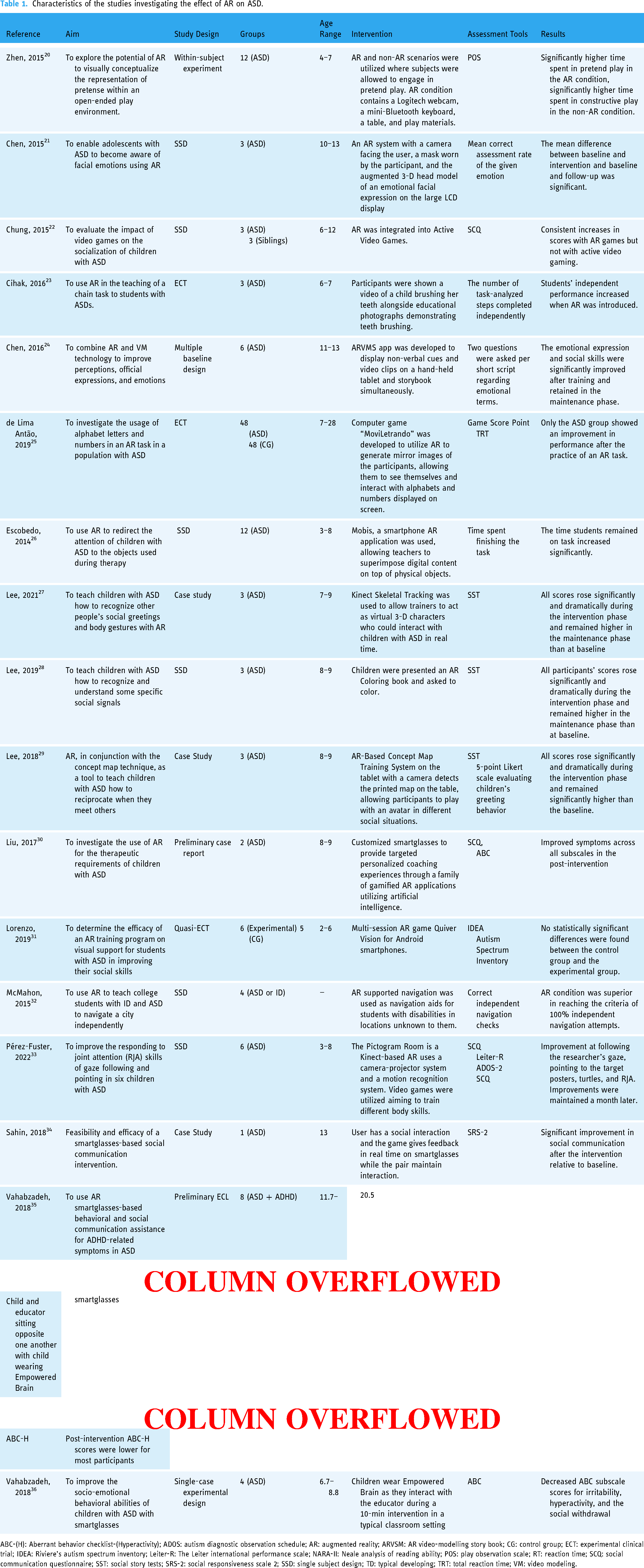
ABC-(H): Aberrant behavior checklist-(Hyperactivity); ADOS: autism diagnostic observation schedule; AR: augmented reality; ARVSM: AR video-modelling story book; CG: control group; ECT: experimental clinical trial; IDEA: Riviere's autism spectrum inventory; Leiter-R: The Leiter international performance scale; NARA-II: Neale analysis of reading ability; POS: play observation scale; RT: reaction time; SCQ: social communication questionnaire; SST: social story tests; SRS-2: social responsiveness scale 2; SSD: single subject design; TD: typical developing; TRT: total reaction time; VM: video modeling.
Characteristics of the studies investigating the effect of AR on ADHD.

AR: augmented reality; ATA: advanced test of attention; ECT: experimental clinical trial; CG: control group; IM: interactive metronome; NARA-II: Neale analysis of reading ability; WWL: WordsWorthLearning© Programme.
Results
Study selection
2191 articles from Pubmed and 1151 from Web of Science were extracted. After removing duplicate records, 3061 articles were extracted for screening. Two researchers screened the abstract of every article; in case of conflict, a third researcher made the final decision. Two hundred eleven studies were selected for full-text reading, and an additional 17 articles were added, which were not identified in the initial search but were mentioned by other systematic reviews and meta-analyses. After full-text analyses, 180 articles that did not meet the eligibility criteria for this review were excluded. The flowchart below shows that 48 articles were included in the qualitative summary (Figure 1).
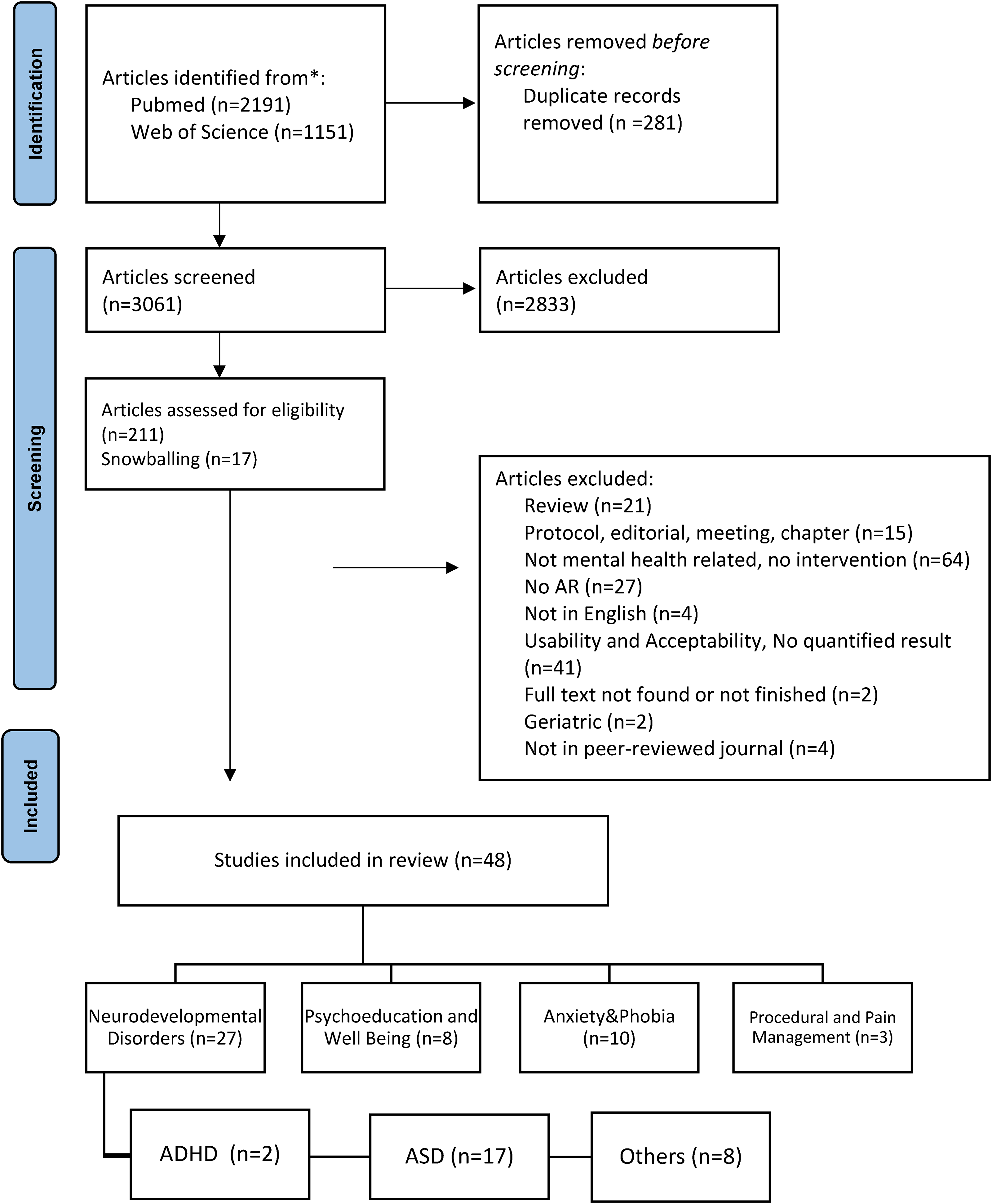
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart of the study selection process for this systematic review.

Number of studies that found AR effective and not effective.
Summary of the main study results
Figure 2 demonstrates the number of studies that found AR interventions effective. The studies on ASD focused on increasing socio-emotional skills, the ability to function independently, and joint attention. Most studies that investigate the effectiveness of ASD have experimental study designs with small sample sizes (Table 1). All studies demonstrated AR as an effective tool; one study by Lorenzo et al. found no difference compared to the control group. 31 AR was less studied in ADHD than in ASD (Table 2). One of the two studies found AR to be attention tasks, 37 and one study did not find improvement in reading abilities 38 (Table 2). Besides ASD and ADHD, AR was mainly studied in ID in neurodevelopmental disorders; eight studies were included in this paper (Table 3). These studies primarily focused on improving the ability of individuals with ID to function independently, thus increasing their quality of life (Table 3). Studies found AR as an effective tool that enabled individuals with ID independent performance in daily tasks and provided a better learning environment (Table 3).
Characteristics of the studies investigating the effect of AR on other neurodevelopmental disorders.
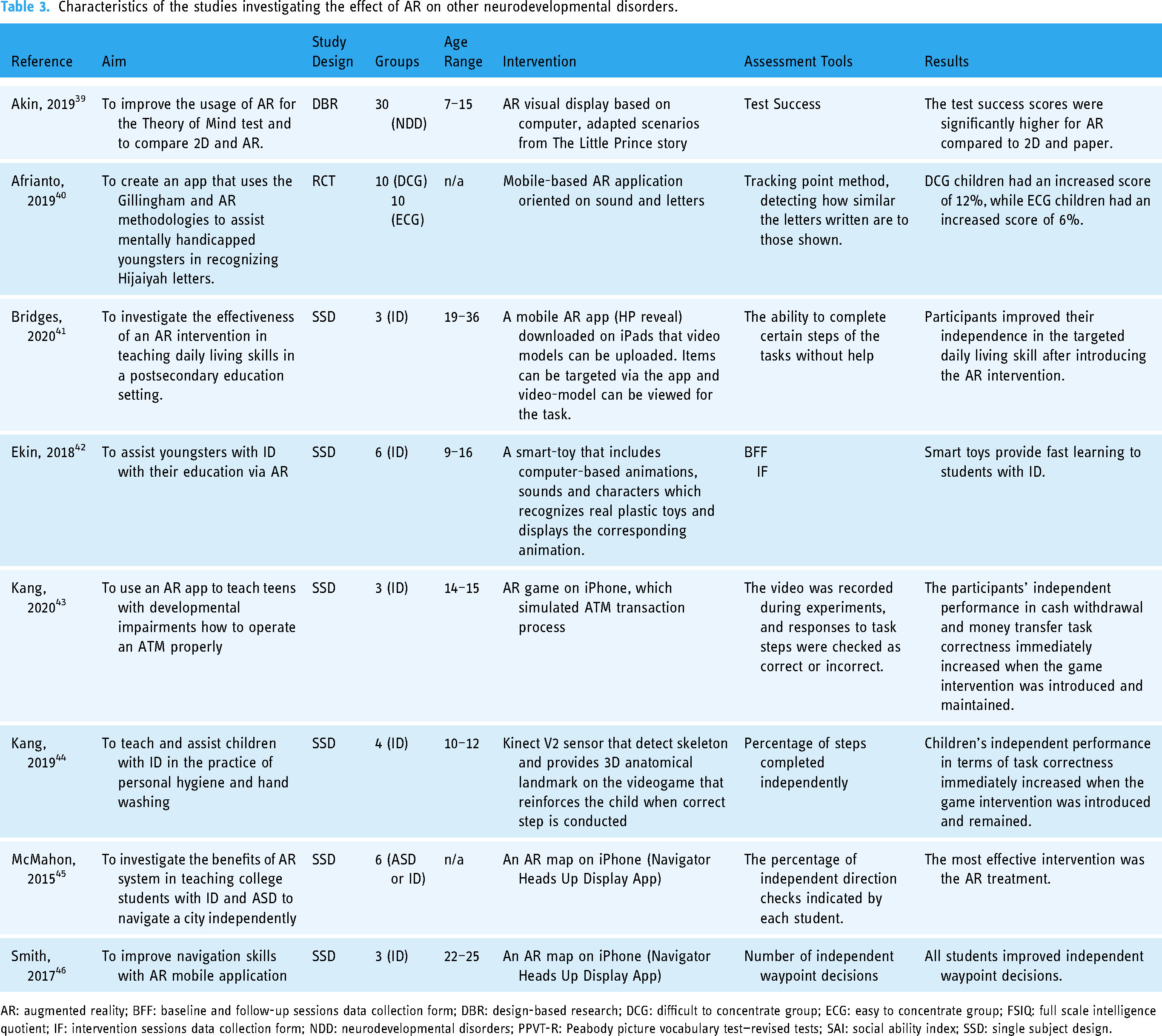
AR: augmented reality; BFF: baseline and follow-up sessions data collection form; DBR: design-based research; DCG: difficult to concentrate group; ECG: easy to concentrate group; FSIQ: full scale intelligence quotient; IF: intervention sessions data collection form; NDD: neurodevelopmental disorders; PPVT-R: Peabody picture vocabulary test—revised tests; SAI: social ability index; SSD: single subject design.
Research on anxiety & phobia included studies with relatively larger sample sizes and qualified research designs as randomized controlled trials (Table 4). Nine of the 10 studies integrated exposure therapy to AR and found satisfying results similar to in vitro therapy but with higher user acceptability (Table 4). The other study focused on anxiety and did not find any effect. 47 In psychoeducation and well-being, we included the nine studies that use AR to improve physical health, emotional well-being, and cognitive performance (Table 5). Except for one study that used an AR book, 48 all studies used online video games as the intervention tool; AR effectively increased physical activity, cognitive performance, and emotional well-being. One study that took place in the office reported the number of patients lost due to patients’ refusal to come or the researcher being unable to reach the patient. 49 The number of patients lost during the intervention in the AR group was similar to the in vivo treatment group. 49 The adherence data could not be collected from other studies. Only three studies were included in procedural & pain management; two were conducted in the pediatric group (Table 6). AR tools decreased anxiety, increased procedural knowledge, and improved pain management (Table 6).
Characteristics of the studies investigating the effect of AR on anxiety & phobia.

AR: augmented reality; ARET: augmented reality exposure therapy; BAT: behavioral avoidance test; CG: control group; CP: cockroach phobia; ECS: experimental case study; ECT: experimental clinical trial; FSQ: fear of spiders questionnaire; HMD: IVET: in vitro exposure therapy; SUDS: the subjective units of discomfort scale; SBQ: spider phobia beliefs questionnaire; SG: study group; STAI: state-trait anxiety inventory; TT: traditional treatment.
Characteristics of the studies investigating the effect of AR on psychoeducation & well-being.

AR: augmented reality; BHS: beck hopelessness scale; BRS: brief resilience scale; CG: control group; GP: game players; DES: differential emotions scale; MVPA: moderate to vigorous physical activity; PANAS: the positive and negative affect schedule; PHQ-4: patient health questionnaire-4; SWEMWBS: short Warwick-Edinburgh mental well-being scale; SWLS: satisfaction with life scale; TEIQue-SF: the trait and emotional intelligence questionnaire short form; SPIN: social phobia inventory; SG: study group; TILS: three item loneliness scale; WMS: Wechsler memory scale.
Characteristics of the studies investigating the effect of AR on procedural & pain management.

AR-TG: augmented reality treated group; CG: control group; ECS: experimental case study; FLACC: faces, legs, activity, cry, and consolability; FPS-R: faces pain scale-revised; SG: study group; VAS: visual analog scale.
The tables below provide details of the study characteristics. (Tables 1–6).
Discussion
In this systematic review, we extracted studies that investigate the efficacy of AR in a wide range of mental health conditions. We demonstrated that the research focused on specific areas, guiding us in this review. We found that AR research in mental health focuses on four domains: neurodevelopmental disorders, anxiety & phobia, psychoeducation & well-being, and procedural & pain management. To our knowledge, there is no systematic review or meta-analysis this comprehensive; nevertheless, we found complementary results with other systematic reviews on specific areas.6,68 After examining numerous studies, we have found a wide range of variables, including study design, sample size, age range, and assessment methods. Our research revealed that AR can be a valuable intervention tool when used in conjunction with evidence-based practices, particularly in cases of autism and phobias. However, we cannot generalize these findings due to the variety of diagnosis and management approaches. As a result, we discussed each group separately to provide more insightful conclusions for our readers.
Neurodevelopmental disorders
According to the DSM-5, Neurodevelopmental Disorders are a category of conditions that start during the developmental stage and cause deficiencies that result in functional limitations. Neurodevelopmental Disorders include ID, communication disorders, ASD, ADHD, and neurodevelopmental motor disorder. 69 The management of neurodevelopmental disorders is difficult due to the complexity of the disorders, which include conditions that affect each other. 70 The evidence-based treatment of autism is based on CBT, focusing on improving social skills, language use, and managing challenging behaviors. 71
Most of these studies that investigated the use of AR in ASD had low sample sizes with experimental case designs. Since these studies investigated a newly developed technological device, they focused on both feasibility and efficacy (Table 1). Due to the investigation of new perception-altering technology in such a diverse population, an experimental case design is acceptable. In contrast, double-blind, randomized controlled trials are challenging to apply. 36 Studies focused on facial emotional recognition, daily life skills, attention, social interaction, and functional and motor abilities. Most of the studies indicated an enjoyable experience that can be individualized (crucial in a wide-spectrum condition) and effective in the long term.21,24,27–29,33 Studies demonstrate that AR provides an intervention that can be implemented in many environments delivered by people other than therapists increasing ecological validity and cost-effectiveness. 33 Besides, it benefits instructors and parents by collecting quantifiable data, increasing quality time spent on tasks, and demonstrating advances in real-world abilities at home. 34 AR tools can be utilized to attract attention to the area that is intended to improve and restrict it there. For instance, one study where AR and video modeling technologies are combined to teach, recognize, and understand facial emotions gave augmented cues for facial expressions. 24 Therefore, children gave attention to expressions instead of unnecessary details, increasing their correct facial expression assessment rate afterward. 24 Similarly, with augmented cues that increase children's attention, AR gamification improves children's reaction time with ASD related to higher cognitive and motor performance. 25
Many studies focused on social interaction. Lee et al. have developed a system that combined AR and Kinect Skeletal Tracking that allowed therapists to control the movements and expressions of the virtual characters in real time. 27 This enables children to interact with virtual characters, which gives them appropriate emotional and verbal responses helping them to comprehend the situation they are observing. 27 Vahabzadeh et al. designed a computerized smartglasses intervention as behavioral and socioemotional support for students with ASD resulting in improved irritability, hyperactivity, and social withdrawal. 35 Chung et al., while studying the effect of active videogame play on the social behaviors of children with ASD, found consistent improvements when AR is added. 22 Considering that difficulty in social interactions impacts the daily functioning of children with ASD, these studies are valuable and can be life-changing. Overall, similar to a previous systematic review conducted in 2020, we demonstrated that the majority of the studies enhance a variety of cognitive and emotional processes, social communication, and theory of mind skills, including facial emotion recognition and attention, as well as functional and motor abilities. 6 Since AR technology has various implementations with different applications and software, the studies that use AR for children with ASD must be replicated and standardized with evidence-based therapies with proven superiorities.
AR is less frequently studied in ADHD compared to other neurodevelopmental disorders. Tosto et al. investigated the effect of a web-based AR learning environment on reading and spelling performances. 38 They found no significant difference between the already-proven approach and AR adjoined. 38 Kim et al. also worked on a game that helps children with ADHD to pay attention and sustain interest in the treatment. 37 Children’s attention and impulsivity improved based on the advanced test of attention and interactive metronome. 37 Although the number of studies on ADHD is small, the results are promising.
The studies that could not be evaluated under ASD and ADHD were investigated in the “others” group, which included eight studies. Studies are composed mainly of people with ID and improving their daily life skills such as navigation, cash withdrawal, and personal hygiene (Table 3). All studies have found that AR is a useful tool for individuals with ID to help them practice daily life more independently.39–46 Parents and teachers of intellectually disabled children express that they recommend AR and find it beneficial. 44 Because the samples are diverse and generalizability is problematic due to the small sample sizes of experimental case designs, more studies are needed for these promising AR tools to overcome the barriers to the independent living of individuals with ID. 41
The research of AR on neurodevelopmental disorders mainly consists of preliminary studies, and the results are promising. Individualized experiences for individuals with special needs renders AR a useful tool.
Anxiety and phobia
According to our review results, it is seen that “Anxiety Disorders” is the area where AR is most commonly integrated and research is conducted. Regarding Anxiety Disorder subtypes, it is seen that the treatment of phobic conditions is the most frequently investigated (Table 4). When used in vitro, exposure therapy has proven efficacy for treating specific phobias. Its adaptability to new technologies, such as VR and AR, rendered it a research focus. A previous systematic review that included VR and AR in phobia exposure therapy stated that VR was widely used in treating various phobias. 68
In contrast, the research on AR is somewhat restricted to animal phobia, and there are few studies. 68 All the studies we included have significantly improved symptoms of phobia with AR exposure therapy. However, the studies which compared in vivo and AR exposure therapies did not find any significant differences in outcomes.51,57 Although studies found no advantages in treatment efficacy, AR has many advantages, including the ability to apply a wide range of situations, enjoyment of exposure therapy games, and a less aversive option.51,57
One of the studies utilized AR to orient nursing students to the clinical environment, investigating the effect of AR on anxiety. 47 Although they found no effectiveness compared to routine orientation, they indicated other advantages, such as saving faculty time and conventional standardized content. 47
Overall, AR interventions offer a safe and controlled environment for exposure-based treatments, which may be more practical and agreeable for some patients than in vivo exposure therapy.
Psychoeducation and well-being
AR is not only valuable for specific mental health disorders but also for physical and emotional well-being. The potential of AR for general well-being was recognized with the emergence of “Pokémon Go,” in which players use their cell phones to search for virtual Pokémon characters. 59 It required players to walk through neighborhoods, increase social interactions, and create new friendships. 59 Its potential for increment in well-being was enhanced during the COVID-19 pandemic and lockdown. It was demonstrated that adolescents had increased cognitive performance in addition to increased physical exercise and socialization. 64 During this period, video games provided people with an escape from the depressing COVID-19 news, entertained them by keeping them busy, relieved their stress, and strengthened their social connections. 61 Studies showed that AR was related to increased physical wellness and self-reported physical activity.59–61 One study using a built-in mobile phone accelerometer did show a trend for increased daily physical activity following the use of Pokémon Go; however, the differences did not reach statistical significance. 63 AR was found effective in mental well-being for the domains of increased positive mood, social connectedness, friendship formation, decreased hopelessness, and reduced emotional stress.8,60 Alarcon-Yaquetto et al. compared the effect of a regular book with an AR book on emotional stress and salivary cortisol levels of hospitalized children and showed that the AR book was more effective than the regular book for reducing self-reported emotional stress in children, but the salivary cortisol difference between groups was not significant. 48
The AR games were effective on cognition, memory, and attention when assessed by validated tests.62,64 The sample sizes of studies using physiological measures were relatively small.48,63 There were no studies investigating the long-term effects of AR on physical and mental well-being. Improving well-being is a public health approach with a preventive potential, and AR was consistently found effective in well-being. However, there is a need for studies investigating the effect of AR on well-being using objective physiological measures on large samples.
Procedural and pain management
Two of the three studies on procedural and pain management focus on children with increased anxiety in hospital conditions.65,67 Mott et al. conducted an RCT for children undergoing burn dressing where they all were administered usual analgesics but randomized into the AR group and basic multidimensional cognitive techniques. 67 They have demonstrated a significant decrease in pain for burning dressing time over 30 min, reported by children and perceived by parents. 67 They have also mentioned a reduced association with negative emotions compared to the control group. 67 Another study to increase the procedural knowledge of children was conducted with a digital therapeutic program called Xploro, which administered information through gamification and AR avatar. 65 Children's trait anxiety and self-reported procedural anxiety decreased while their knowledge about the procedure and satisfaction increased through the intervention. 65
AR devices are demonstrated to attract children's attention, decrease hospital anxiety, and improve procedural knowledge. AR devices are easy to use, entertaining, and portable, and they have great potential for procedural and pain management, although the number of studies is small, and there is an extensive research gap.
Limitations
In this study, we tried to gather studies from many disciplines that complicated the overview of AR in mental health. The quality of the studies, sample characteristics, and interventions are diverse, which handicapped the conclusion. The small sample sizes of most studies and newly developed devices created a challenge in the generalizability of the effectiveness. Another limitation of the studies is the various study designs that could not be grouped. The number of studies that used both a scale and behavioral analysis was limited. We could not include studies that are not English, not in the Web of Science, or Pubmed index (if not referenced in a review article), which are missed for results. Additionally, adherence to AR applications is not discussed in detail in the studies, which is an important issue that could affect the results considering that delivery method and place of the intervention can impact adherence. 72
Conclusion
Our results demonstrate heterogeneity in terms of study designs, intervention tools, and sample sizes among studies investigating the effectiveness of AR in mental health conditions. The heterogeneity is incredibly high among neurodevelopmental disorders with different sample sizes, study designs, and scales, and many studies have low quality. AR has shown to be efficacious for anxiety and phobia, whereas comparison with traditional treatment has no significant advantage for treatment response. The research gap is significantly high in psychoeducation and well-being studies (focusing primarily on Pokémon Go) and procedural and pain management (the number of studies is minimal).
Most studies point out promising results regarding integrating AR in treating mental health conditions. AR, which is easy for gamification, increases children’s enthusiasm to enhance treatment engagement. Although AR is a new technology still in development, the devices are portable, cost-effective, and easy to use. AR provides a personalized intervention tool that enables patients to enhance treatment options for time and environment, allowing them to continue at their own pace. We need further studies with high sample sizes, complete demographic information, and validated questionnaires with high diagnostic values to integrate AR to present evidence-based treatments. Additionally, it is essential to ascertain the extent to which the connection between using AR applications and intervention outcomes is influenced by adherence and whether this adherence persists over time. Studying what increases participants’ adherence can help researchers design easily applicable follow-up studies. We believe that investing more to create engaging and user-friendly content can help people's willingness to participate in more longitudinal studies.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231203649 - Supplemental material for Use of augmented reality in mental health-related conditions: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076231203649 for Use of augmented reality in mental health-related conditions: A systematic review by Çiçek Nur Bakır, Sharif Omar Abbas, Egemen Sever and Aslıhan Özcan Morey, Herdem Aslan Genç, Tuba Mutluer in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231203649 - Supplemental material for Use of augmented reality in mental health-related conditions: A systematic review
Supplemental material, sj-docx-2-dhj-10.1177_20552076231203649 for Use of augmented reality in mental health-related conditions: A systematic review by Çiçek Nur Bakır, Sharif Omar Abbas, Egemen Sever and Aslıhan Özcan Morey, Herdem Aslan Genç, Tuba Mutluer in DIGITAL HEALTH
Footnotes
Acknowledgment
Special thanks to everyone who helped throughout the study. Thanks to Belgin Konakci, who contributed to the quality assessment. Thanks to Mehtap Bekhan, who contributed to the introduction, discussion feedback, and proofreading. Thanks to Asım Evren Yantac, who introduced us to AR. Thanks to Arda Cayci and Mercan Beyazit for their contributions to the literature search and data extraction.
Contributorship
TM, HAG, and AOM conceptualized and designed the study. ÇB and SA conducted systematic literature review and article screening, with TM, HAG, and ES as reviewers. ÇB, SA, ES, HAG, and TM conducted data extraction. SA, ES, and ÇB conducted quality assessment. HAG, TM, and AOM contributed to critical revision. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
TM
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.