
Abstract
Objective
In an environment with an ageing population, elderly care has become a focus of social attention. The combination of smart medical care with elderly care and how to encourage the elderly to participate in the systems and enjoy a higher quality of life have become social priorities. We aimed to analyse the perceived risk and value associations of self-health management-conscious older adults regarding smart medical and elderly care systems (SMECS) and to explore the mechanisms of SMECS affecting them.
Methods
Using a Likert scale, we conducted a questionnaire-based survey and collected 387 valid responses. This was a cross-sectional study, and various key data were collected relating to the continued participation of older users in SMECS. Partial least squares structural equation modelling was used to explore the data.
Results
According to the data analysis, price, operability and personalisation all have significant correlations with perceived value and perceived risk. Perceptions of value and risk influence the continuous participation of the elderly, and this has a potentially positive effect on their mental and physical health.
Conclusions
Under the home-based care model, economic factors and technological accessibility were important factors affecting the elderly's continuous participation in SMECS. A personalised programme for the elderly warrants attention. In addition, the effect of perceived risk from the health-related systems was stronger than their perceived value. This research can help elderly users bridge the digital divide and enjoy smart health and medical care.
Introduction
The ageing trend in populations has far-reaching implications for the global economy, with significant shifts in consumer spending towards the elderly. 1 When the health consumption market is considered, it contradicts the public's stereotypes of the elderly, such as low levels of consumption and weak self-care ability. The 2030 Agenda for Sustainable Development released by the United Nations (UN) shows that paying attention to the health of older people is an important part of realising sustainable development goals. However, the extension of life expectancy is not inevitably equated with healthy living. The elderly still face many health-related problems, such as diminished physiological function and increased depression. In 2020, the UN pointed out in its ‘Policy Brief: The Impact of COVID-19 on Older Persons’ that isolation and distance during the pandemic had made many older people feel marginalized, leading to amplified age discrimination in society and making older people increasingly vulnerable. Considering economics, emotions, and realities, home care is a better choice for most elderly people. However, traditional models of care ignore crises, such as unexpected illnesses or sudden accidents, where there is no one to respond. In this context, achieving better self-health management for the elderly has become a challenge.
Therefore, the role of smart medical care has become increasingly significant. Smart medical care is one aspect of the smart city, 2 which refers to a combination of 5G, the internet of things (IoT) and other technologies that are combined with traditional medical models to achieve intelligent, humanized and personalised medical services. 3 The goal of combining smart healthcare with the home care model is to manage medical data coming through the smart devices so that they can provide detection, monitoring, social and other functions. This will enable the reasonable and efficient allocation of medical resources to achieve a sustainable ecosystem that combines medical with home-based care and supports a comprehensive assessment of health. The elderly can use physiological data collected through their smart medical devices to understand their own physical conditions better, to comply with nursing service instructions, to obtain simple online health consultations, and to adjust their dietary plans, rehabilitation treatments or other services. However, the UN's Sustainable Development Goals Report 2021 points out that the impact of the pandemic has eroded project reforms to implement digital health in several ways. Due to the digital divide and the problem of ‘getting old before getting rich’, the number of elderly people enjoying comprehensive smart medical service systems is less than expected. In addition, traditional elderly care has challenges in terms of medical security, such as limited medical resources for self-care. Furthermore, community and institutional healthcare resources are limited and generally expensive. Therefore, introducing smart medical care into the home care service system is an effective measure for solving home-based health problems.
Researchers have mainly explored the design and application of smart medicine in the fields of computer science, engineering, telecommunications and mathematical computational biology. For example, researchers have studied the architecture of smart medical systems as represented by smart monitoring systems. 4 Ermolina and Tiberius 5 conducted a study on voice-controlled intelligent personal assistants, which, although subject to errors and unable to replace manual care, have great potential for supporting older people. The existing literature on smart medicine mainly focuses on how smart technology can improve quality of life and optimise overall planning and design, with the aim of achieving sustainable development. 6 On further reviewing the literature, we found that most research discusses how to promote healthcare for the elderly through technological and systematic innovations in the face of practical challenges and considers the issue from the perspectives of the smart home,7–9 technical service suitability10,11 and so on. In China, there is little demand for smart home elderly care in the market. Zhang et al. 12 conclude that this is related to the poor social cognition of the needs of the elderly and the many stakeholders involved in the smart home market. Scholars emphasise that smart home development is mainly promoted by the government, and they provide guidance relating to all aspects. Hung 13 makes observations regarding technological innovation and policy development and provides an overview of research into the use of smart medical devices and their personalisation, advocating improvements in both areas for the elderly market. In this study, the smart home is considered in terms of its interactive environmental factors, such as intelligent lighting systems, video surveillance, burglar alarms, home networks, electric locks and access control. In this study, we explore self-health management for the elderly from the perspective of smart healthcare. Although smart elderly service systems are mainly driven by government policies and regulated by market participation, meeting the needs of the elderly is the core element of this study. The intellectualisation and systematisation of medicine combined with home care are not yet mature, and they face many problems in both theory and practice. 14 Although many researchers have promoted the popularisation and specific application of smart medicine, most of the achievements are still in the stage of theoretical discussion. In addition, there are still many gaps in the research into a combination of smart medical care and elderly care services.
Chen et al.
15
analysed some longitudinal data and concluded that smart medical services are beneficial to residents’ health and that the effects persist across regional differences. Although smart medicine has been shown to have many benefits for both the community and the public, its acceptance and use in elderly care service systems are low. The mechanisms of smart healthcare delivery are not verified, and many obstacles hinder the popularisation of their application. Du et al.
16
used a two-stage data envelopment analysis to analyse the service performance of elderly care institutions in China that had implemented a combination of medical and nursing care, and they pointed out that the coordination of medical resources in such a combination needed to be improved. Therefore, in this study, we refer to relevant medical services included in home care, in the course of which the elderly use various smart devices, as smart medical and elderly care systems (SMECS). This definition is based on the use of a variety of smart medical equipment and includes its extended functions and services, which form a complete ecosystem of smart medical services and provide multi-faceted elderly care services. The use of interactive smart medical devices, such as self-testing oximeters and smart bracelets, can detect, alert and warn seniors of their health conditions and safety. These smart medical devices can also be user-friendly and provide personalised medical and care services, such as issuing reminders to stand up and to take medication, and they can connect quickly with trusted caregivers of the older person's choice. This study focuses on the participation and feelings of elderly people regarding the continuous use of SMECS in their home settings. Hence, we propose the following research questions:
How does the stimulation provided by SMECS trigger psychological perceptions (of risk and value) in the elderly?
What is the relationship between the psychological changes prompted by the use of SMECS and the continued participation of older adults in the use of SMECS?
To answer these questions, the experiment was divided into two sections based on the stimuli–organism–response (SOR) model. First, the environmental stimuli were defined as price, operability and personalisation. Second, we explored the perceptual changes prompted by these three factors in the organism's state and, finally, their impact on the individual's continued participation. This research was carried out as an empirical analysis based on the demand for smart medical service systems. On the one hand, we were seeking to help improve the degree of acceptance of smart medical devices by the elderly group and, on the other hand, to provide a theoretical basis for the implementation of SMECS by institutions, governments and other organisations. Furthermore, we explained the impact mechanism of SMECS more comprehensively than before, which provides support for improving the quality of home-based medical care service systems and eliminating the digital divide.
Literature review
The degree of the ageing population is deepening, and the needs of the elderly are becoming more diverse. How to meet the needs of the elderly to achieve a better goal of old-age care has become a hot topic of social concern. According to the self-determination theory, Guo et al. 17 extracted the needs of all people, including autonomy, ability and kinship. Peine et al. 18 focused on the components of social life in old age and found that science and technology are closely related to ageing. Technology can meet the needs of the elderly to some extent. The government is also deeply concerned about the needs of the elderly. Due to the limited cognitive level and mobility of the elderly, the government has established a mobile digital government so that the elderly can equally and freely get information and enjoy services. 17 Under the guidance of UN policy, the whole society contributes to the elderly care service.
The combination of technology and the elderly care industry has resulted in the emergence of many smart home products. Many researchers have carried out research on the technology and equipment of smart healthcare. Regarding the elderly's use of smart technology, Golant 19 found that it was associated with the perceived effectiveness, availability and impairment of the technology. Smart devices, such as smart home speakers, can capture user interaction to analyse the data stream, which supports analysing the behaviour of elderly people at home and detecting health problems. 20 Sujith et al. 21 proposed that technological tools, such as 5G and deep learning, should be used to build smart health monitoring systems to better meet the needs of patients. Telemedicine systems assist older people get help at home in case of emergencies and shape a good environment. 22 Based on the private cloud, Hung and Lin 23 designed a smart system for home care, injecting advanced technology into the carriers of wearable devices to achieve real-time monitoring of the establishment of warning, tip, prevention and other functions. Personalised service design not only allows patients to feel the warmth of care but also reduces the cost of human resources and improves the efficiency and quality of medical services and systems.
Smart medical systems have gradually improved and proved necessary for the elderly. However, whether the elderly choose to use SMECS and how to better manage their medical treatment remains a question. Alavi et al. 24 focused on the elderly population in Asia and called for narrowing the gap between social and medical care, better care management for the elderly and a better quality of life for the elderly population as much as possible. Hussain et al. 25 built a model of a telemedicine system centred on the elderly and disabled to provide emergency services when health abnormalities are detected. Social networks are also used to provide services for vulnerable people with physical and mental health problems. The combination of smart systems and medical devices is a viable solution to healthy ageing. However, most of the existing literature focuses on the effect of a single technology or device on the independent living of the elderly. It separates the elderly from society and lacks attention to their life experiences. 26
The above research verified the inevitability of the development trend of smart medicine from different perspectives and confirmed the huge potential of SMECS. Most of the existing research has focused on the application of smart medical devices,20,21 but there has not been much involved in the field of the behavioural mechanism impact of SMECS. Exploring the elderly's continuous participation in SMECS can fill the research gap in this field. Therefore, based on the existing research, we elaborate on the behavioural mechanism of the elderly group's participation in SMECS.
Theoretical background and hypothesis development
SOR
The SOR model explores the process of people's mental state changes and reactions after being stimulated by the outside world. It has a wide range of applications and high explanations and can fully explain the changes in consumers’ mental states and behavioural choices caused by the external environment. SOR applies not only to the analysis of environmental biology 27 but also to the business domain, successfully explaining market incentives and cognitive factors that lead to differences in consumer behaviour. 28 The SOR model has good flexibility. 29 It is highly consistent with the theme of this research. This paper aims to explore how stimulation related to smart medical service systems triggers the psychological perception of the elderly and whether they are willing to continue participating. The SOR model starts with the three dimensions of stimulus, organism, and response. The stimulus perceptions of the technology and of the services provided by SMECS are outlined, and there is an exploration in progressive depth of the mechanisms at play in participants’ sustained engagement behaviours.
Based on the SOR, a model of home-based elderly people's continuous participation in smart medical services was constructed. Put the price, operability and personalisation as the stimulating factors (S), the perceived risk and perceived value as the organism (O), and the continuous participation behaviour as a response (R) and explore the correlation among the three. Furthermore, we will explore the influence of elderly users’ long-term participation in SMECS on their physical and mental health (see Figure 1).

The research model.
Perceived risk and perceived value
Decision making is the result of weighing pros and cons. 30 The most common approach is to consider risk and value as a whole. Due to internal and external uncertainties, the subject needs to consider potential hazards, namely perceived risk. 31 The perceived value is a comprehensive psychological evaluation formed by the comparison between the cost paid and the benefit gained in the whole process from purchase to after-sale. 32 Both play an important role in consumer behaviour, and the research on online shopping, 33 green consumption, 34 technology 35 and other fields is extensive. The existing literature has investigated perceived risk and value according to specific scenarios and has tested the hypothesis of a connection between customer perception and participation intention. Results show that perceived risk is negatively correlated with participation intention, while perceived value is positively correlated with participation intention.36,37
Based on the existing literature, the perceived risk and perceived value of the elderly group participating in SMECS will be defined as follows: Perceived risks include medical risks and financial risks. 38 Medical risk refers to the potential problems faced by the elderly after receiving smart medical services, such as inoperative equipment, improper diagnosis and privacy disclosure. Financial risk occurs when services require a considerable fee, and the elderly suffer from financial fraud and capital turnover problems. Perceived value is divided into two categories: utilitarian value and hedonic value. 39 Utilitarian value refers to the elderly's perception and evaluation of functional benefits obtained in time, information, efficiency and other aspects under rational circumstances. Hedonic value refers to the subjective happiness, relaxation and other emotions experienced by the elderly when they enjoy SMECS.
Hypothesis development
Prices are monetary representations of transactions. Price cognition directly impacts the perceived value of products and consumers’ purchase desires and is closely related to consumers’ purchase behaviour.
40
In this paper, price refers to the amount of money required for the various devices and related services used in SMECS. Price perception is the subjective judgement of different consumers on whether the price is suitable, expensive or cheap. For high-priced products and services, risks such as monetary losses and inconsistent expectations increase and the risk is related to consumer attitudes.
32
When consumers’ perceived risk increases, they make more cautious purchasing choices. Most older consumers tend to choose low- to medium-priced elderly care services over high-priced ones.
41
On the other hand, it has been pointed out that price is the determinant of perceived value, and the price of both services and products affects consumers’ perceived value.
42
Consumers are sensitive to price changes.
43
High prices will increase the perceived economic cost of consumers, thus increasing their perceived value.
44
High-priced items subjectively reflect a higher quality, and service quality significantly and positively affects consumers’ perceived utilitarian value.
45
With the relationship between price and quality, the elderly will have higher expectations for service and product quality, thus increasing their perceived value. As a result, the following hypotheses are proposed:
H1: Price is positively related to the perceived risk of older people. H2: Price is positively related to the perceived value of older people.
Operability is the functional description of a device in the technical field, which can positively affect purchasing behaviour.
40
Operability in this paper refers to the ease of operation of SMECS; that is, older people can conveniently use the equipment to access services. From a system-oriented point of view, the barriers to consumer acceptance are technology-based, where high-technology–level system quality leads to a better user experience.
45
In some studies, the use of smart devices brings convenience to life and effectively averts risks. For example, elderly people can use their voices to perform commands by interacting with smart home speakers.
20
Due to decreased behavioural, cognitive and memory ability, it is not easy for the elderly to strictly follow the doctor's advice, and the practical operation of drug treatment is poor. The smart pill box connects the Internet to the physical pill box to record and remind the elderly of their health data.
46
When smart devices are highly operable, the elderly can be better served by medical care and pension services. Smart devices have interactive features and are simpler to operate overall, allowing for an improved quality of service
45
and effectively reducing the perceived risk to older people. As the operational technology of smart healthcare matures, the perceived value increases when the consumer perceives that the benefits outweigh the costs.
47
Therefore, it is hypothesized that:
H3: Operability is effective in reducing perceived risk. H4: Operability is effective in increasing perceived value.
Personalisation generally means that providers offer services and products based on each person's different preferences, tastes, personal behaviour or geographical location.
48
In the field of health, personalisation refers to the provision of specialist healthcare services based on the consumer's health condition and health information.
49
Personalisation has a significant positive effect on trust,
3
while higher levels of trust reduce consumers’ perceived risk and increase their perceived usefulness and value.
48
Using big data to propose personalised medical plans can better treat patients with different conditions.
50
Many successful treatments will effectively reduce the perceived risk. In other words, when the level of personalisation is higher, the degree of product or service matching with consumers will be higher, thus reducing perceived risk and improving consumers’ satisfaction. As personalised SMECS innovatively infuse technology, consumers’ perceived costs and values will increase. The perceived value increases when consumers perceive that the benefits outweigh the costs,
47
increasing the perceived value of the service offered to older people. Hence, we propose the following hypotheses:
H5: Personalisation has a positive effect on reducing perceived risk. H6: Personalisation has a positive effect on increasing perceived value.
Customer participation is the resource or behaviour externalised by the customer's efforts and input at material and spiritual levels.
51
Customer participation is a mental, physical and emotional commitment based on a certain level of intention.
52
In this context, continuous participation is the intention to continue to use the function and participate in the activity.
53
In this paper, it refers to specific measures over an extended period where older people participate in SMECS with payments, learning skills, wearing devices, using a platform, etc. The predecessor of participation is intention, which is influenced by perceived risk and perceived value. Risk is a synonym for the possibility of adverse consequences, which all disciplines represented by investment and marketing science seek to eliminate, avoid and mitigate. Consumers’ perceptions of risk and their own risk-taking capacity directly influence their decisions. Perceived risk has a side effect on participation. The stronger the perceived risk, the greater the perceived chance that a crisis will be faced. Conversely, the greater the perceived value, the greater the perceived benefit, so perceived value is the main prerequisite for participation. Based on existing research, we propose the following hypotheses:
H7: Perceived risk has a negative influence on continuous participation. H8: Perceived value has a positive influence on continuous participation.
Research methods
Procedures
In order to achieve our research objectives of mapping, evaluation and prediction, we used a questionnaire due to its advantages of low costs and high levels of anonymity and efficiency. The questionnaire was designed and developed by combining previous findings identified in the literature with practical applications. First, the study population (i.e. the inclusion–exclusion criteria) was identified. Second, we created a research scope statement and pre-screening questions to enable later confirmation of the validity of the returned questionnaires. We then invited volunteers to be involved in a pilot survey and trial analysis so that we could make changes and adjustments to the scope. For the formal survey, the questionnaire was administered over a period of four months and was made available to participants in a range of activity venues frequented by older people. And the samples sizes following the 10-times rule in the partial least squares structural equation modelling (PLS-SEM) study. 54 Participation involved either filling out a physical questionnaire, distributed in person by the researcher, or scanning a QR code placed (with the permission of the person in charge) in retail outlets, residential areas, etc., and then completing the questionnaire online. The completed questionnaires were collected and checked for validity, and the data were analysed using the coding principle and SmartPLS 3.3.9 application. The results were discussed by the researchers, and the overall research was reviewed and the findings summarised, as shown in Figure 2.
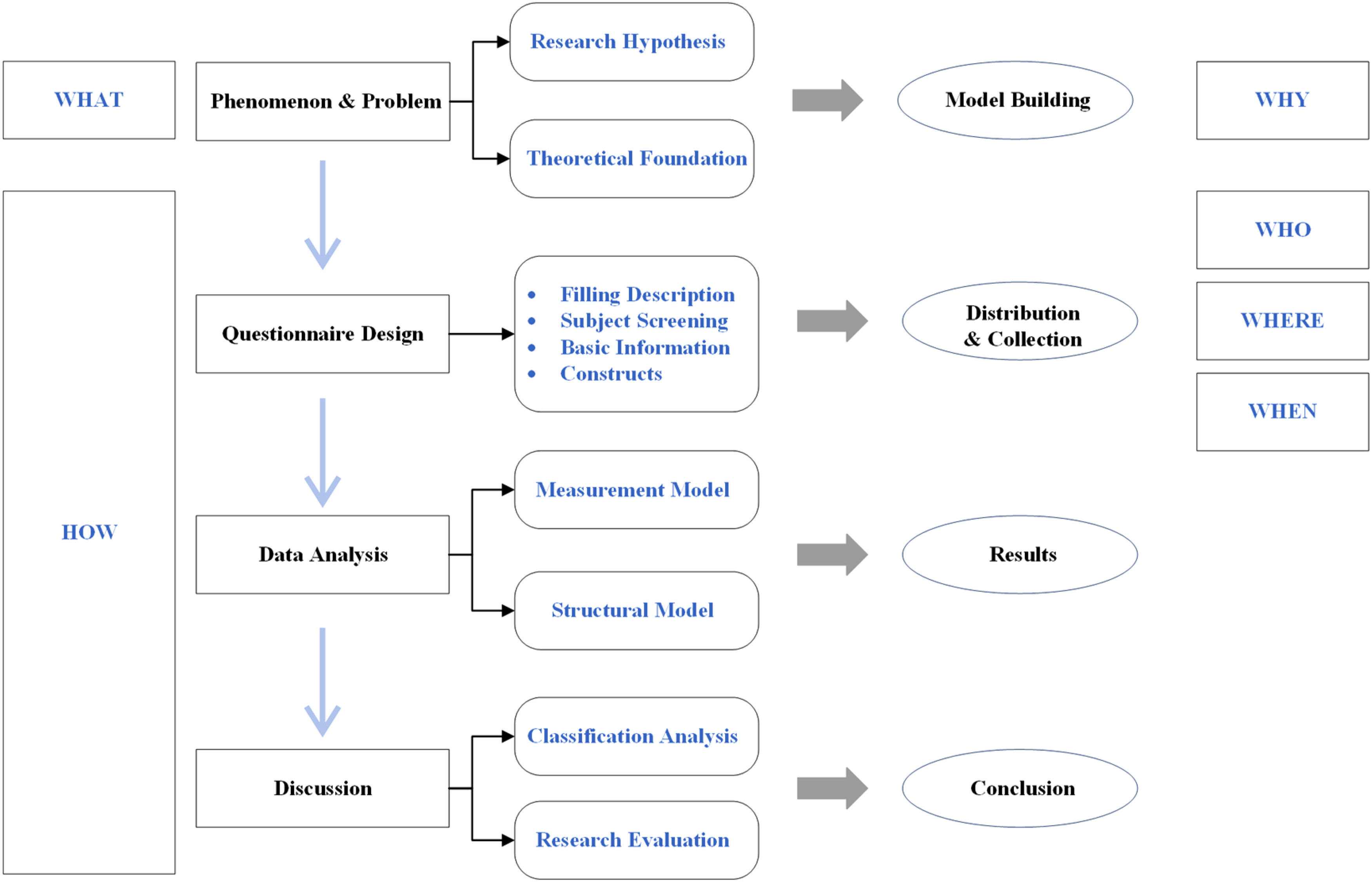
Research procedures.
Materials
The Likert scale was used to collect the responses of the participants and to test the above hypotheses. We constructed a structural model to explore the impact of the dependent variables on the healthy development of continuous participation in the SMECS based on six key variable elements. First, we conducted a small-scale pretest and recruited 35 elderly volunteers who met the inclusion criteria to complete the questionnaire. The research team then made adjustments based on issues that emerged from the pretest and from the feedback from the volunteers. Next, we invited experts to suggest ways of optimising the quality and effectiveness of the questionnaire. By implementing their suggestions, we arrived at the final version of the questionnaire (see Appendix).
The questionnaire consisted of three sections, and it began by clarifying the background and purpose of the research. First, we highlighted the study’s inclusion–exclusion criteria in relation to our definition of SMECS. In addition, we declared that the research data would remain confidential, and we encouraged the elderly participants to fill out the questionnaire based on their own situation and to provide a combination of subjective and objective responses. Part A collected basic demographic information about the respondents, such as gender, age and education level. Assuming that the participants were functioning in a home-based care environment, Part B collected the average time and range of use by quantity and functions of the smart devices used by the respondents, including whether they would call for help if they fell. Part C comprised of a scale designed to convert subjective elements into measurable indicators. In this part, the questionnaire explored operability variables and included options on the use of smart medical devices because the SMECS service is based on the use of a variety of devices. This included intelligent medical equipment, such as wearable devices for real-time heart rate recording and monitoring. This can provide a better service for elderly health reporting by providing warnings of abnormal signs and calling for help. It assists in supporting the data processing and analysis of the elderly's health records and improving service quality.
Samples and data analysis
This study focused on the factors that influence the elderly's continued use of SMECS and its impact on their health and resulting quality of life. SMECS is a smart device–based medical and aged care systems. The research emphasized the feelings and experiences of elderly participants who use multiple devices in intelligent medical service systems. The inclusion criteria for the subjects in this study were: (a) over 50 years of age, which matches the definition of later life by the World Health Organization (WHO) and the Mental Health Foundation; (b) living independently and living away from relatives and children; (c) having at least two smart medical devices in use at home; and (d) participation in smart health services for more than four weeks. Due to the inclusion criteria, elderly users with an educational level of junior high school or below were excluded, as the study focused on the self-health management of elderly people using smart medical product services. To ensure the accuracy of the study results, any elderly person who was receiving multiple medical programmes, such as continuous care in a hospital or nursing home, was excluded. The questionnaire was designed on the basis of existing research combined with practical experience. Questionnaires were distributed both online and offline in residential areas, parks, and health intelligent device retail stores, among other channels. We had set up a pre-screening mechanism and then investigated and tracked eligible subjects using a deeper survey. We collected questionnaire data from August to November 2022. A total of 625 questionnaires were distributed, 492 questionnaires were returned and 387 valid questionnaires were obtained after excluding invalid questionnaires (due to short answer times, overly concentrated selection options, omissions and failure of the questionnaire response validity tests).
We processed the collected data using the IBM SPSS Statistics application. We used PLS-SEM to further analyse the data. PLS-SEM is a variance-based path analysis method that can effectively estimate the structural paths of complex models. 55 It is a statistical analysis method used for estimating model structure through a combination of principal component analysis and ordinary least squares, enabling it to estimate internal consistency, discriminant validity, path coefficients and other model parameters. It also has strong statistical and explanatory power for research done with small samples. After obtaining 387 valid samples, PLS-SEM was used to analyse both the measurement model and the structural model. It was applied to exploring the mechanisms of continuous participation in SMECS and providing feedback on their use and effectiveness by home-based elderly participants.
Ethics
During the research, we strictly adhered to the following research ethics: (a) voluntary participation; (b) anonymous recording of relevant information; (c) adopting strict data protection and storage policies and not collecting the information of identifiable individuals; (d) respondents could terminate or withdraw at any time; (e) prior disclosure of research objectives; (f) no conflicting interests between subjects and researchers; (g) no data were recorded before the questionnaire was submitted and (h) information related to this research was stored on one computer, accessible only by related researchers authorized by the supervisor, and the computer's hard disk was encrypted to ensure the security and integrity of the data.
Results
General information
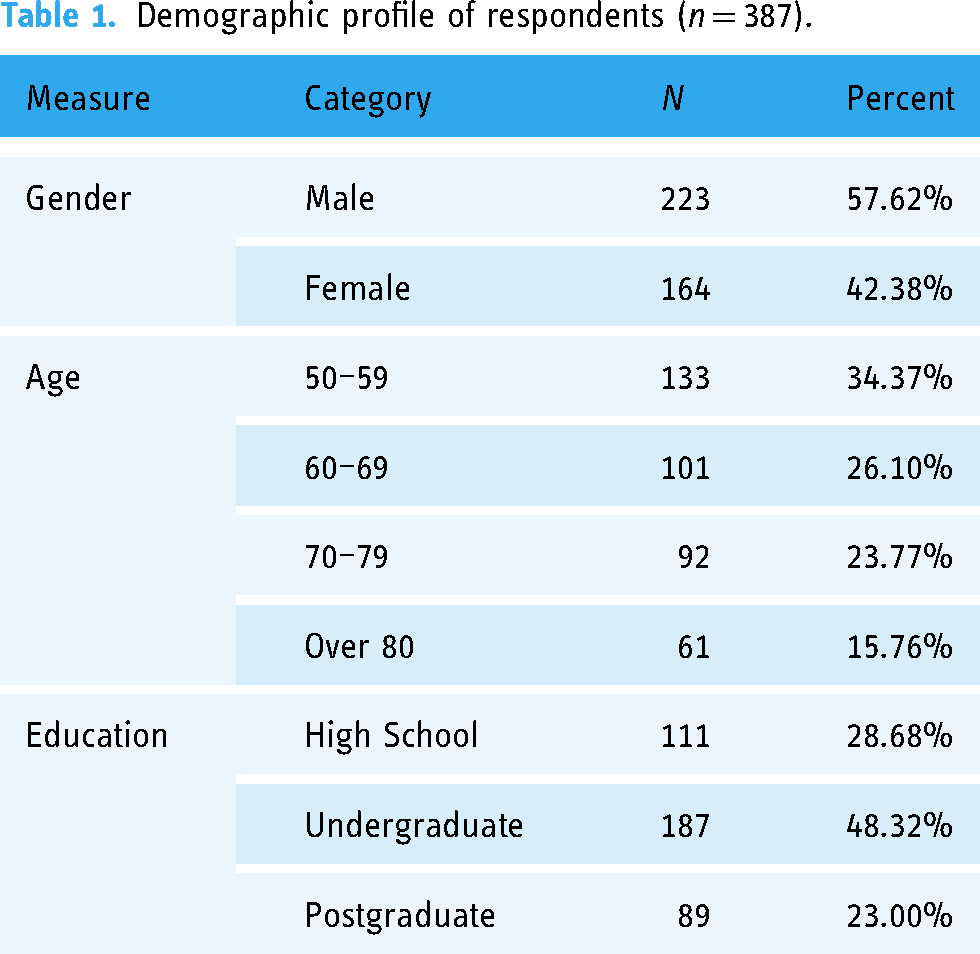
The research focused on collecting basic information about the sample in terms of gender, age and educational level. A total of 387 older people were included in the study. Of these, 223 were male and 164 were female. The participants were divided according to age ranges: 50–59, 60–69, 70–79, and over 80, with 133, 101, 92 and 61 participants, respectively. Regarding educational level, 111 (28.7%) had completed high school, 187 (48.3%) were undergraduates, and 89 (23.0%) were postgraduates (see Table 1).
Demographic profile of respondents (n = 387).
Measurement model assessment
To evaluate the reflective measurement models, we assessed the reliability and validity of all constructs. On the reliability indicators, we evaluated the model's internally consistent reliability through Cronbach's alpha (CA), composite reliability (CR), and rho_A.56,57 As shown in Table 2, the CA values were all greater than 0.883, CR was greater than 0.908 and rho_A were all greater than 0.848, all of which were greater than the minimum standard value required for the correlation,57,58 indicating that the structure had good internal consistency and passed the reliability test.
Descriptive statistics for the constructs.

In the validity assessment, we analysed convergent and discriminant validity. The average variance extracted (AVE) can test the convergent validity of a construct by squaring all indicators and calculating the mean value. The value of AVE above 50% indicates that the potential factors of the model explain more than 50% of the variance of the construct. 59 From the results in Table 2, all AVE values were significantly greater than 0.5, indicating that the model had good convergent validity. For discriminant validity, we used the Fornell–Larcker criterion and the cross-loading values to verify. The square root of the AVE of each structure was higher than the estimated correlation (as shown in Table 3), and the cross-loadings of each variable exceeded the loadings of their potential structures (as shown in Table 4), demonstrating that the model passed the test of discriminant validity. 60 Moreover, as shown in Table 4, the variance inflation factor is less than 3. Thus, there is no common method bias threat in this study. 61
Correlations among constructs and the square root of the AVE.

Note. Bold numbers represent the square roots of the AVEs.
Factor loadings, cross loadings and VIF.

Note. Bold numbers indicate outer loading on the assigned constructs.
Structural model assessment
In this paper, the analysis of the structural model was evaluated by the path coefficient (β), certainty coefficient (R2) and blindfolding-based cross-validated redundancy measure (Q2). The path coefficients (β) between the variables were obtained by estimating a series of regression equations (see Figure 3). Based on the data, the relationship between the variables and perceived risk: price (β = 0.520, p < 0.001), operability (β = −0.325, p < 0.001), and personalisation (β = −0.125, p < 0.01) and the relationship between the variables and perceived value: price (β = 0.357, p < 0.001), operability (β = 0.267, p < 0.001) and personalisation (β = 0.445, p < 0.001), supported hypotheses H1–H6. Perceived risk (β = −0.712, p < 0.001) and perceived value (β = 0.262, p < 0.001) support hypotheses H7 and H8. All the hypotheses proposed above are valid.

Statistical significance test results at research model.
The coefficient of determination (R2) is a good indication of the explanatory power of the model, with values ranging from 0 to 1.59,62 Larger values correspond to greater explanatory power. R2 for perceived risk was 0.596, R2 for perceived value was 0.396 and R2 for continuous participation was 0.535, indicating that the structure has good explanatory power. Finally, the prediction accuracy of the path model was assessed by calculating the Q2 value. The value of Q2 = 0.429, which is greater than 0.35, indicates that the model has good predictive accuracy and good predictive relevance.59,63
Results summary
We used a random sampling method to increase the sample size as far as experimental feasibility and funding allowed, and we encouraged eligible older people to participate in completing the questionnaire. A total of 492 questionnaires were returned, giving a return rate of over 75%. There were no significant differences in the demographic characteristics of the participants across the age ranges.
The regression analysis of the data obtained confirmed that the questionnaire had good reliability and validity and that the research model had good predictive power. Through PLS-SEM, the research results were verified, and they confirmed that all hypotheses were valid. Higher prices for smart devices stimulated an increase in perceived risk among older people, while operability and personalisation of the devices effectively reduced perceived risk. Perceived value was positively influenced by all three measures. While perceived risks had a negative effect on continued participation, perceived value had a positive effect. The results were categorised separately for the discussion and analysis.
Discussion
Principal findings
The findings reveal that price is positively related to perceived risk and value for older people. In contrast, Ye et al. 64 used data from online hotel reviews to find that price negatively impacts perceived value. This may be because our research focuses on multiple smart devices that require long-term use to obtain a more comprehensive evaluation. Subjectively, most people will consider a combination of price and quality. 42 As older people tend to attach more importance to product quality and utility, the higher the price, the greater their expectations. Objectively, higher-priced products have a clear superiority in brand effect, special features, after-sales services and other added value. In the results of this research, the impact of price increases fluctuates more significantly on perceived risk. As the smart product market grows, the products lack uniqueness, and there are more substitutes. Combined with prudence, older people are highly sensitive to price. High-priced products are exposed to risks such as payment overflow, difficulty distinguishing between genuine and fake products and difficulties in using them, increasing their psychological pressure and perceived risk. Therefore, the game of perceived risk versus value needs to be considered in the pricing of SMECS.
The findings demonstrate that operability effectively reduces perceived risk and positively increases perceived value. Compared with the research using the technology acceptance model (TAM), TAM studies perceived usefulness and perceived ease of use with intention,40,45 while we combined the two into usage (operability) as an external variable, which relates to continuous participation through perceived change. The elderly face the risk of being excluded by technology. Operability simplifies the process, reduces the difficulty of usage, weakens the perception risk for older people, brings a better user experience and further increases the perceived value. Smart devices, such as the smart pillbox and Apple Watch, enhance operability through voice reminders and data logging. 46 When the perceived difficulty of use is low, it will be easier and better to motivate the older group. 65 SMECS with better operability can be adopted faster by older groups, increasing their health awareness and the development of healthy habits.
The results show that personalisation has a negative effect on perceived risk, which in turn significantly increases perceived value. Similarly, Kang and Namkung 66 concluded that personalisation significantly influences perceived benefits and risks. They focused on brand apps for food services that share characteristics with smart devices. In reality, most smart devices and online health services do not satisfy the unique needs of older people, making them more difficult and risky to use and greatly hindering their use of online services. 65 The design of personalised features and operations, such as cameras with voice prompts for patients with reduced mobility and tailor-made care solutions, makes older people feel valued. 67 Meeting individual needs and being more adaptable and secure significantly reduces perceived medical risks and increases perceived value.
The empirical analysis data confirm that perceived risk and value have a significant negative and positive effect on continuous participation, respectively, which is similar to Chiu et al.. 68 We found the influence of perceived risk was greater than that of perceived value. Park et al. 69 found that mobile devices can help older people adhere to medication and perceive more value. The perceived use value of the elderly group through operability and personalisation leads to better experiences and satisfaction. Increased trust and loyalty will prompt them to continue participating in SMECS. However, along with information leakage, equipment failure and financial fraud, various potential risks sway the choices of older people. Out of caution and fear, they are more risk averse. Despite the increased perceived value, the relatively small perceived risk is still likely to cause older age groups to discontinue their use of SMECS.
Health is both an investment and a consumer good. 70 The impact of health on a person has a direct effect on his or her subjective well-being and creates undoubted fluctuations in life satisfaction. 71 There is diversity and inequality in healthy ageing. 72 People reaching old age will face many new risks, particularly medical risks. Illness in the elderly may cause serious consequences for their finances, emotions and family relationships. Health can be distinguished according to age, health status and other criteria. According to the WHO, health is divided into physical, mental and social health. 73 In view of the medical characteristics of SMECS, this paper examines the external stimulations of older people at the healthy development levels. 74 SMECS is a health investment based on the elderly's own medical needs. It is a technology-dependent management model that links the elderly, the doctor, the hospital and the living space in a close and effective way, enabling timely, rapid and efficient warning and management of health problems in the elderly. SMECS involve the elderly's continuous use of a variety of smart devices involving family medical services. This is based on intelligent medical equipment, which integrates a variety of medical resources with modern technology to break through the limitations of time and space, thereby joining the elderly to the main body of medical care, and providing a system that can enable the elderly to manage their health and, at the same time, help the elderly to cross the digital divide.
As for health development, the findings suggest that economic factors and technological accessibility were important factors affecting the elderly's continuous participation in SMECS, which is similar to Chen et al. 15 and Chan-Nguyen et al. 75 Chen et al. 15 measured smart healthcare services in terms of infrastructure, and Chan-Nguyen et al. 75 targeted virtual care using smart devices. Moreover, one study showed that continuous participation with a single smart device can effectively increase health performance in the elderly. 76 Instead, we focused on the overall SMECS with multiple smart medical devices. When elderly groups continuously participate in SMECS, they have more knowledge of their own body data information and improved health literacy, which is conducive to better health management. Meanwhile, most home-based groups crave companionship and perception. Interactive functions, such as dynamic voice and information updates in smart medical devices, enable the elderly to gain certain companionship and attention, effectively relieving psychological stress and positively impacting mental health.
Theoretical implications
This paper has some theoretical contributions. First, unlike previous research, this paper not only focuses on the behaviour of the elderly using a single smart device and is different from single decision-making research focusing on the intention to use trust or risk, but shifts the single factor into continuous participation. We focus on the mechanism by which elderly people who enjoy home care continuously participate in SMECS.
The home care model is both widespread and universal and is chosen by most older people in China. We constructed a home care scenario in which the elderly were in contact with their children from a distance. Various smart devices, such as smart bracelets and home cameras, monitor their health conditions and provide relevant smart medical services. The findings enrich the relevant research on home care and support further development and optimisation of the home care model. We aim to meet the real needs of the elderly and enable them to better enjoy the social conveniences brought about by digitalisation. We also deciphered the impact of continuous participation, which can help older people adapt to a healthy life over a long period. A complete continuous participation model was constructed to further track the effects of continuous participation, help improve the service system, and provide positive feedback.
Second, this research applies the SOR model to the field of smart healthcare and combines it with the elderly care model to further verify the validity and applicability of the SOR model, filling the research gap between the SOR model in the healthcare field and the elderly care model. The three important factors, which are representative, price, operability and personalisation of SMECS, were examined and thus enriched the research on smart healthcare. We conducted quantitative research on the healthcare model of smart ageing service systems using questionnaires. The study provides a preliminary discussion on how older people can better use smart medical devices to access their health information and enjoy the convenience of digital socialisation.
Practical implications
For elderly families, continuous participation in SMECS can be a good way to improve quality of life in old age and provide an additional guarantee of the safety and health of elderly people who are alone at home. Also, the results help older people better adapt to smart medical service systems in terms of decision-making regarding smart elderly services selection. From the perspective of the elderly, this paper can help them to measure and enjoy the convenience of socialisation when they are provided with information data and smart tools and to explore, initially, a smoother path for the elderly in the field of smart healthcare. From the results, the continued participation behaviour of the elderly is more influenced by the perceived risk, and how reducing the perceived risk of the elderly will be the key to the further advancement of smart healthcare for the elderly.
For organisations, age-appropriate product design is reflected in all aspects. In terms of price setting, they need to increase the perceived value of high-priced products through better quality, uniquely designed features, and good after-sales services to alleviate older people's distrust and riskiness of higher prices. In terms of design, consider customized design solutions to tailor the appropriate medical equipment to older people. In terms of operation, by simplifying the operational steps and fitting them with smart voice services, the elderly can use smart medical service systems conveniently and consistently. With the development of the IoT, organisations should upgrade their technology and work to make multiple smart devices interconnected to achieve real-time health data monitoring and analysis, creating a more convenient and efficient model of ageing in place.
For the government, this paper helps the government promote the integration of ‘medicine’ and ‘health’ and plays a role in guiding the market properly. It can set rules on the pricing of smart medical products to prevent serious price premiums and set technical standards for products and services to ensure product quality and standardize the service experience. Meanwhile, the government can also play a synergistic role in coordinating the allocation of medical resources, mobilising the enthusiasm of medical platforms, medical institutions and other relevant bodies through policy guidelines and encouraging corporate innovation. Adding safeguards to smart medical devices and strengthening the construction of a smart medical and healthcare system for the elderly.
The findings of this study confirm that SMECS can contribute to the physiological and psychological changing needs of elderly users. Elderly individuals with a certain level of digital awareness can enjoy convenient and intelligent medical service systems to assist in their self-health management. Compared to the current situation, all parties should pay careful and thorough attention to the physical and mental health of the elderly and improve their medical living conditions. When designing medical service systems, we need to focus on both the physiological and psychological aspects of health needs. For example, regarding physiological health, we can improve the design of physical index tests and the functioning of physical data monitoring and analysis. Regarding psychological health, we can add a module for interactive communication with the elderly and increase their psychological consultations.
Limitations and future study
There are several limitations to this study. First, the selection of variables regarding stimuli in the study selected only three prominent factors. Other factors regarding the elderly group's characteristics, such as age, income and education level, can also have an impact on the continuous participation of SMECS. A user portrait of the elderly group should be established to achieve better product design optimisation and user experience. Second, although the sample size of this study reached the minimum sample size required by the structural equation model, an increase in the sample size will further strengthen the accuracy and reliability of the results. Smart healthcare and elderly care for the elderly are complex compositions of multiple subjects and scenarios, and apart from home care, the applicability of the research model to other elderly care models still needs to be examined. Also, from the perspective of the smart healthcare ecosystem, the integration and enhancement of resource coherence are worthy of further study, given the discontinuity of medical resources among hospitals, institutions and the elderly. In future research, studies on health performance measurement can also be further improved to track continuously the effects of SMECS use by older people and to explore the mechanisms behind the reasons.
Conclusion
As the ageing process accelerates, more and more attention is being paid to a ‘combination of medical care and health care’ approach to ageing. The rapid development of technology has provided strong support for smart medical devices and services. This paper explores the mechanisms that encourage continuous participation in SMECS that would enable older people to adapt better to their old age while enjoying the convenience of a digital society.
This study explored the mechanisms of continued participation in SMECS by older people. Focusing on the scenario of home care, the SOR model was employed to define environmental stimuli (price, operability and personalisation) and to explore the impact of these factors on the psychological perceptions generated by continued participation. The results revealed that the three factors were associated with perceived value and risk and further influenced the continued participation of older people. In conclusion, this paper breaks through the limitations of a single behaviour and further refines the application of the SOR model to smart healthcare and elderly care models. In addition, it provides guidance and implications for all involved in SMECS, such as the elderly person, their family, the government, institutions, etc.
This study constructed a complete model for continuous participation. The results show that continuous participation in SMECS is associated with an awareness of self-health management in older adults. The elderly involved in SMECS need a certain economic foundation. Against a social background where digital is the default, they should be able to integrate digital health through self-improvement and enjoy certain digital privileges and benefits. A focus on physical and mental health is necessary for a comparison with the real-life challenges of older people. Although there are limitations to the study, in future research, we will continue to focus on the field of smart healthcare in ageing and consider factors related to the characteristics of older adults. In addition, we will continue to track the health-related performance of SMECS enjoyed by the elderly.
Footnotes
Acknowledgments
The authors thank all the respondents who participated in the study.
Contributorship
CC conceived the study. DL and HD researched literature. CC led the study design and planning of analyses, with all authors contributing. Data collection and formal analysis were conducted by HD. DL and HD wrote the first draft of the manuscript. CC reviewed and edited the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Review Board of School of Management, Zhejiang University of Technology, China.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the National Social Science Foundation of China, grant number 22BGJ037; the Zhejiang Provincial Federation of Social Sciences, grant number 2023N009; the Humanities and Social Sciences Research Project of Zhejiang Provincial Department of Education, grant number Y202248811; the Zhejiang Province University Students Science and Technology Innovation Activity Program (Xinmiao Talent Program), grant number 2022R403048; and the Zhejiang University of Technology Humanities and Social Sciences Pre-Research Fund Project, grant number SKY-ZX-20210175.
Guarantor
CC.
Informed consent
Participants gave informed consent via the statement ‘I am aware that my responses are confidential, and I agree to participate in this survey’ where an affirmative reply was required to enter the survey. They were able to decline to participate or withdraw their participation at any stage of the survey without giving a reason.
Appendix

| Construct and item | Reference |
|---|---|
|
|
Warganegara and Hendijani 40 Goldsmith et al. 43 |
| 1. The price of the smart medical and elderly care systems (SMECS) is a good indicator of its quality. | |
| 2. I think the high price SMECS matches its own value. | |
| 3. I don’t mind paying more for smart medical and elderly care equipment. | |
|
|
Warganegara and Hendijani 40 |
| 1. I can use smart medical equipment skillfully. | |
| 2. I can easily remember how to use smart medical devices. | |
| 3. I think I can use smart medical devices without the help of others. | |
|
|
Guo et al. 49 |
| 1. SMECS can understand the personalised needs of the elderly. | |
| 2. SMECS can collect and manage personal data of the elderly. | |
| 3. SMECS provides services based on the personal information of the elderly. | |
|
|
Chang and Tseng 33 Zhang et al. 35 |
| 1. SMECS may have system errors such as equipment and diagnosis. | |
| 2. I’m worried that SMECS will compromise my privacy. | |
| 3. SMECS may increase my medical care costs. | |
|
|
Chang and Tseng 33 Liu et al. 37 |
| 1. SMECS makes me feel more efficient. | |
| 2. SMECS can make me feel happy. | |
| 3. I think SMECS is a good deal and worthwhile. | |
|
|
Yang et al. 53 |
| 1. I will spend considerable time on the SMECS. | |
| 2. I am willing to use relevant resources and learn relevant skills. | |
| 3. I am willing to continue to use relevant services. |