
Abstract
Background
Medical alliance plays an important role in promoting resource sharing, optimizing the allocation of medical resources, establishing a hierarchical diagnosis and treatment system featuring primary diagnosis at the grassroots level, a two-way referral system, separated treatment for acute and chronic diseases, and dynamic cooperation. Thus, comprehensive performance evaluation for medical alliance is a necessary research that involves a multi-attribute group decision-making problem.
Objective
The aim of this paper is to develop a new multi-attribute group decision-making evaluation framework and new weight method to better efficaciously resolve the issues of evaluation for the medical alliance.
Methods
Firstly, Archimedean copula and co-copula operational rules, called Archimedean co-copula, and the form of q-rung orthopair fuzzy Hamy mean aggregation operator based on Archimedean co-copula operational rules are also developed. Secondly, an extended q-rung orthopair fuzzy extended best-worst method satisfying multiplicative consistency is developed to originate the weight information of the attributes. The new weight method can integrate the membership and non-membership of assessment information, improve constancy for group decision making and get an extremely reliable weight consequence. Finally, a novel multi-attribute group decision-making framework is presented based on the proposed q-rung orthopair fuzzy Archimedean copula and co-copula Hamy mean aggregation operator and q-rung orthopair fuzzy Euclidean best-worst method. Furthermore, the new multi-attribute group decision-making method is applied to comprehensive performance evaluation for medical alliance in Shanghai, and the effectiveness of the new method is also demonstrated.
Results
The results show that the proposed multi-attribute group decision-making method with Archimedean copulas-based Hamy operators and extended best-worst in this paper outperforms some existing methods and provides support for policymakers seeking the use of patient- and community-centered health evaluations to improve health services.
Conclusion
The proposed method is a theoretical guidance method and a good reference for the evaluation of medical alliances of other regions in China.
Keywords
Introduction
The distribution of medical resources in China has long been in an unbalanced state. In order to solve the problem, a medical alliance with a full-featured, hierarchical, and resource-sharing structure has been proposed. Medical alliance refers to the combination of tertiary hospitals, several secondary hospitals, and a number of community hospitals, as well as general and specialized hospitals by the integration of horizontal or vertical medical resources in the same region to a group of medical institutions or joint organizations. Medical alliance plays an important role in establishing a hierarchical diagnosis and treatment system featuring primary diagnosis at the grassroots level, a two-way referral system, separated treatment for acute and chronic diseases, and dynamic cooperation. At the same time, urban public hospitals also can make full use of the medical union to send quality resources to the grassroots level and guide patients to seek treatment. Obviously, the construction of a medical alliance is of great significance to alleviate the scarcity and uneven distribution of medical resources in China. In order to speed up the improvement of the medical alliance, fully leverage the intellectual support role of experts in promoting the construction of medical alliance, further improve the scientific decision-making and the high pertinency of policy measures, guide and assist in different regions to continuously promoting the construction of medical consortia during the 14th Five Year Plan period, the National Health Commission of the People's Republic of China decided to establish an expert group on promoting the construction of medical consortium, to assess and supervise the implementation and the construction of medical alliance across the country. Comprehensive performance evaluation for medical alliance as a feedback form of medical reform policy is conducive to mobilize the enthusiasm of all kinds of medical institutions at all levels to participate in the construction of medical commonwealth, and can help know the operating situation of medical alliance and find problems timely, formulate measures and targeted improvement. In this sense, it is of great significance to reasonably evaluate the comprehensive performance of medical alliance for solving the development difficulties, integrating medical resources, and constructing the hierarchical diagnosis and treatment system. Therefore, systematic evaluation of the operation effect of medical alliance can continuously improve the service quality of hierarchical diagnosis and treatment. When evaluating the operation effect of medical combination, multiple relevant factors will be considered comprehensively, which is a typical multi-attribute decision-making problem. The multi-attribute group decision-making (MAGDM) problem is the process of ranking alternatives and selecting the best one among a set of alternatives in line with multiple attributes, and it has been widely used in many fields in recent years. Due to DMs’ evaluations over alternatives are always imprecise and fuzzy, how to accurately express, manage and integrate expert attribute value of uncertain decision information is a key and fundamental question. To deal with it, quite a few fuzzy tools, such as intuitionistic fuzzy set (IFS), 1 Pythagorean fuzzy set (PFS), 2 complex IFS, 3 interval-valued IFSs, 4 interval-valued PFS 5 , and probabilistic linguistic term set 6 have been proposed. Yager generalized the IFS and PFS and proposed a new concept of q-rung orthopair fuzzys (q-ROFS) whose prominent feature is that the qth power of MD and the qth power of NMD is equal to or less than one. 7 Evidently, q-ROFS relaxes the constraints of both IFS and PFS, which makes it more powerful than IFS and PFS in the aspect of dealing with vagueness. Therefore, by adjusting the value of parameter q, q-ROFS allow DMs to independently assign values to MD and NMD. Due to its higher capacity of modeling the fuzziness, many studies on q-ROFS have been done, such as integrations of q-rung orthopair fuzzy continuous information, 8 continuities, derivatives and differentials of q-ROFS, 9 knowledge-based entropy measure, 10 logarithmic distance measure, 11 combination of q-ROFNs and other fuzzy sets,12,13 overview on q-ROFS, 14 etc.
Apart from that, more scholars focus on q-rung orthopair fuzzy MAGDM methods based on information fusion. As a basis of information fusion under different fuzzy context, aggregation operations play an important role in information fusion, and can aggregate a collection of individual evaluated values into one. In general, aggregation operations can be considered from the following two aspects, (a) Operations rules: many operational laws are based on the different t-norm and t-conorm family, such as Hamacher t-norm and t-conorm, Frank t-norm and t-conorm, Dombi t-norm and t-conorm, Archimedean t-conorm and t-norm. Especially, Archimedean t-conorm and t-norm are a generalization of various t-conorms and t-norms families and can generate different operational rules, such as algebraic operational laws, Einstein operational laws, Hamacher operational laws,
15
Frank operational laws, Dombi operational laws, and so on. (b) Aggregation functions: different aggregation functions are used to solve different decision problems. For example, PA operator proposed by Yager
16
can relieve the influences of unreasonable data given by DMs on the decision result. Bonferroni mean(BM)
17
and Heronian mean (HM),
18
can consider interrelationships of aggregated arguments. Based on the above operations rules and aggregation function, many researches about q-rung orthopair fuzzy MAGDM methods based on information fusion has been done. For example, Liu and Wang
19
proposed the basic algebraic operational laws and further develop a family of q-rung orthopair fuzzy weighted averaging and geometric operators. Peng et al.
20
proposed exponential operational law on q-ROFNs and then applied it to derive the q-rung orthopair fuzzy weighted exponential aggregation operator. Liu and Wang
21
proposed the Archimedean operational rules of q-ROFNs and further develop q-rung orthopair fuzzy weighted Archimedean BM operators. Based on novel Aczel-Alsina t-norm and t-conorm, Akram et al.
22
proposed q-rung orthopair fuzzy prioritized Aczel-Alsina averaging and geometric operators. Aydemir and Yilmazgündüz
23
proposed Dombi operational law and Dombi prioritized weighted averaging operator are also given. Further, Yang and Peng developed q-rung orthopair fuzzy weighted BM Dombi averaging operator. Darko and Liang
24
defined Hamacher operational rules and proposed weighted q-rung orthopair fuzzy Hamacher average and the weighted q-rung orthopair fuzzy Hamacher Maclaurin symmetric mean operator. Combined with classic arithmetic and geometric operators, Xing et al.
25
proposed a new family of q-rung orthopair fuzzy point weighted aggregation operators to control the uncertainty of decision data. Besides, Liu and Liu,
26
and Wei et al.
27
successively extended existing operators, such as BM, and HM to the q-ROFS. Meanwhile, Liu et al.
28
propose a new method based on the q-rung orthopair fuzzy extended BM operator and entropy measure for dealing with heterogeneous relationships among attributes. With the increasing complexity of realistic decision-making problems, aggregation operators with versatile functions also be further developed. For example, Liu et al.
29
put forward q-rung orthopair fuzzy power Maclaurin symmetric mean operator to solve the decision-making problems of attribute-related and unreasonable evaluating data. To deal with the situation where interrelationships of arguments exist in part of the argument but not in all the arguments, Yang and Pang
30
developed q
Obviously, the above-introduced MAGDM methods based on q-rung orthopair fuzzy aggregation operators are based on Archimedean t-conorm and t-norm, which makes them lack of flexibility in the process of aggregation. Is there any other way to build Archimedean t-conorm-like operational law that is based on a more general t-conorm? As far as we know, the copula functions proposed by Sklar 32 are the mathematical tool for describing probability distributions, while t-norms are the mathematical tool for combining membership functions of fuzzy sets. Thus, copula functions and Archimedean t-conorm are similar theoretically. The most commonly used copula function is the family of Archimedean coupla (AC). In fact, ACs are monotone non-decreasing and thus are aggregation functions, which have indeed been studied as a tool for aggregating information on certain sets. For example, Jouini and Clemen 33 used copula function to link the marginals for aggregating information from expert opinions. Grabisch et al. 34 focused on construction methods for copula functions. Han et al. 35 proposed a new computational model based on Archimedean copula (AC) and corresponding Archimedean co-copula (ACC) and apply to deal with probabilistic unbalanced linguistic multiple attribute group decision-making. Just as Archimedean t-norm and t-conorm, AC and ACC have the same advantages as they do, that is, copulas and co-copulas are more general and flexible as decision makes can choose different types of copula and co-copula to define the operational rules under fuzzy environment. More importantly, copula functions can reveal the dependence among variables and keep more original information in the process of aggregation. Therefore, it is meaningful to investigate AC and ACC operational rules and aggregation operators based on it. On the other hand, different q-rung orthopair fuzzy aggregation operators are used to solve different decision problems. For the aggregation functions aspect, HYM introduced by Hara et al. 36 is a useful aggregation function that can take into account of the interrelationships among multiple arguments. Due to this advantage, many scholars extended HYM to other fuzzy sets, such as cubic linguistic PFSs, 37 picture 2-tuple linguistic sets, 38 normal wiggly hesitant fuzzy linguistic term set, 39 etc. Thus, the study on the form of q-rung orthopair fuzzy Hamy aggregation operators based on the AC and ACC operational rules is also a key point of this paper.
Determining the weight of each attribute in the MAGDM process is also important, which can directly affect the reliability of results. AHP first introduced by Saaty 40 is one of the most popular methods to decide the criteria weights. However, the DMs need to do pairwise comparisons between all criteria in AHP method, which makes the calculation process more complicated. Recently, a novel best-worst method (BWM) as an enhancement of the traditional AHP method, has been provided by Rezaei. 41 BWM has the characteristics of simplicity, accuracy, and less redundancy. DMs only need to identify the best and worst desirable criteria, and then make pairwise comparisons between the best/worst criterion and the other criteria. Due to the ease of way and the reliability of the got consequences, plentiful studies have salaried care to use the BWM to originate apiece criterion weights. However, the traditional BWM method uses the form of 1–9 scales to express the pairwise comparisons of the BWM. With the complexity of information development, it is more appropriate if we use q-ROFS to express DM's preference degree, that is to say, the best-to-others vector and others-to-worst vector are all q-ROF vectors, then the obtained criteria weights also should be q-ROFs correspondingly. Unfortunately, how to solve such a type of q-ROF programing model is a problem. Some existing literatures 42 solve this problem by dividing the membership and non-membership parts separately to solve it, which may lose the essence of the q-ROF best-worst method (q-ROF-BWM) based on the membership part and non-membership part, and the derived weight vector may not be normalized. There is also some literature 43 that address it by using the division and subtraction operations laws of q-ROFS, midpoints 24 or score values 44 to transform it into a crisp mathematical programing model, which may get a nonlinear mathematical programing model and has no global optimal solution. Therefore, it is better to transform into a crisp programing model that can integrate the membership and non-membership functions, and get a normalized and global optimal solution. In this paper, we further modify the best-worst method (BWM) and develop an extended q-ROF-BWM to determine the weight information of the attributes.
The above analysis describes the motivation of this paper. Comprehensively considering the above aspects, it is very necessary to extend the HYM based on the AC and BWM method to further apply them to MAGDM problems under q-rung orthopair fuzzy environments. However, how to define copula operational rules under q-rung orthopair fuzzy environment? What is it the like the form of q-rung orthopair fuzzy aggregation operator based on the copula operational rules? How to define and solve the q-ROF extended best-worst method (EBWM) programing model without losing the original information? Therefore, the goal of this paper is to introduce AC and ACC operational rules of q-ROFNs, called ACC, q-ROF-EBWM weight determination programing model, then develops q-rung orthopair fuzzy HYM aggregation operators based on the AC and ACC, and finally provides a new train of thought for MAGDM problems with unknown weight information.
On the basis of discussed motivations, the paper is organized as in Figure 1. The “Preliminaries” section reviews basic concepts. New AC and ACC operational laws for q-ROFNs are also introduced in this section

Organization of the paper.
Preliminaries
In this section, basic concepts of q-ROFSs, the HYM and dual form of the HYM (DHYM) operators, Copula and Co-copula are briefly reviewed. Then, new operational rules of q-ROFNs on the basis of the AC and ACC that are important in the context of the paper are also proposed.
q-Rung orthopair fuzzy set and q-rung orthopair fuzzy preference relations

To compare two q-ROFNs, Liu and Wang 18 proposed a comparison method for q-ROFNs.
If If
If

Zhang et al.
46
also introduced the following multiplicative consistency concept of q-ROFPRs:



Copula and co-copula
if


If

if
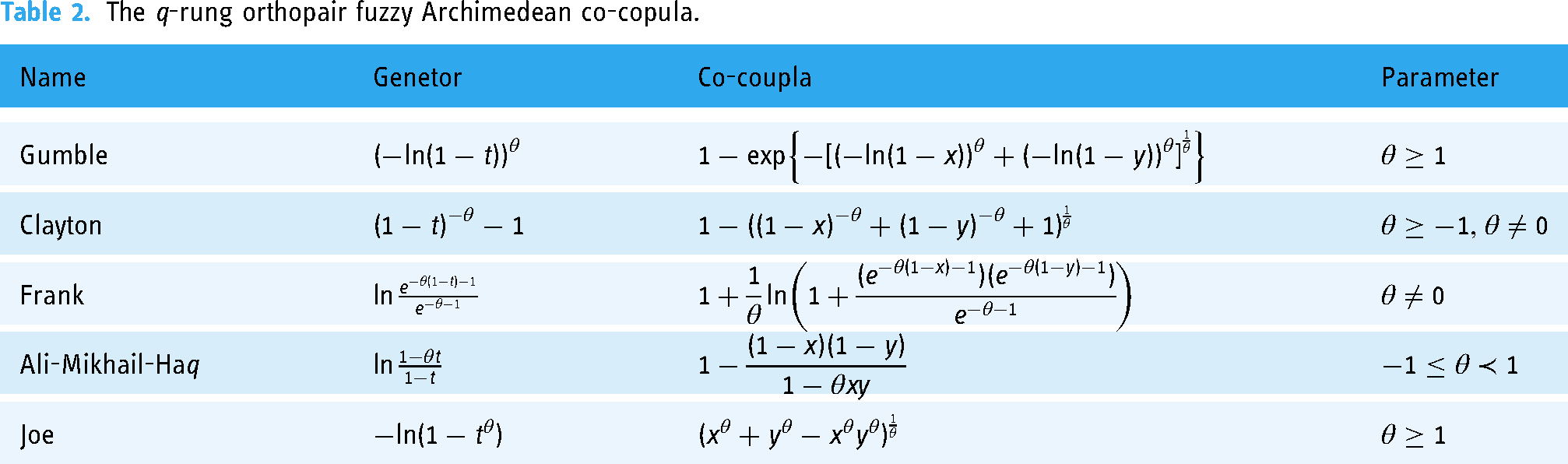
As described above, any generator of an AC is convex and strictly decreasing function. So, if a function satisfies the above properties, we can generate different families of AC. In Tables 1 and 2, we give some well-known families of AC and ACC corresponding to different generators

The q-rung orthopair fuzzy Archimedean copula.

The q-rung orthopair fuzzy Archimedean co-copula.
Operational laws of q-ROFNs based on ac and ACC
Based on the AC and ACC, we can propose a generalized intersection and a generalized union for q-ROFS. In the following, we will give the operational rules of q-ROFNs on the basis of the AC and ACC.
It should be noted the above equations (1)–(4) are the general expressions with functions
Moreover, desirable properties of the AC operational laws can be easily obtained.
The HYM was firstly proposed by Hara et al..
36
It can consider the interrelationships among arguments.

The HYM is a Schur-convex and monotonic function when aggregating numerical information. Based on the theory of majorization, Xing et al. 31 proposed the DHYM as follows:
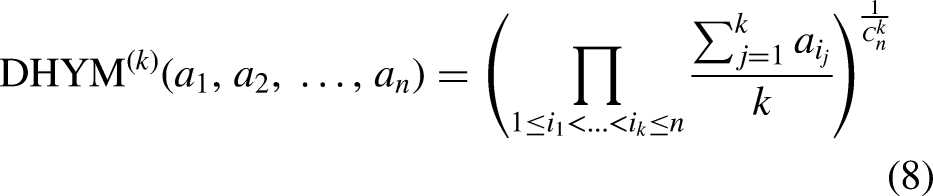
Especially, if k = 1, based on the definition of DHYM, the DHYM reduces to the geometric mean as follows:


Methods
This study aims to develop a performance evaluation model for medical alliance in China. In June 2021, in order to guide and assist local governments in accelerating the completion of the hierarchical diagnosis and treatment system, and continuously promoting the construction of medical alliance during the 14th Five-Year Plan period, the National Health Commission decided to establish expert group for promoting the construction of hierarchical diagnosis and treatment and medical alliance to evaluate and supervise the implementation of the construction of hierarchical diagnosis and treatment and medical alliance nationwide. In this section, According to the standard of “Medical Alliance Comprehensive Performance Evaluation Index System” in the working plan for comprehensive performance evaluation of medical cooperation (Trial) issued by the National Health Commission, based on the score of expert group, this is a theory-driven study conducted in five primary health care institutions in the medical alliance system of Shanghai. In this section, the steps that will carry out to achieve the aim are explained. New weight determination method satisfying multiplicative consistency by a crisp programing model, and q-rung orthopair fuzzy AC HYM aggregation operators are shown in the following sections.
Determining the criteria weights with multiplicative consistency based on the extend q-ROF-EBWM method
The important part of the BWM introduced by Rezaei 41 is the expression of preference information. Considering the hesitancy of the real decision-making problems, it is more suitable to adopt q-ROFS to express DM's preference degree. Zhang et al. 45 introduced the definition of q-ROFPR. It is a powerful tool for solving complicated MAGDM problems. Thus, in this section, we use the q-ROFPR R to describe DM's preferences.
The traditional BWM method uses the form of 1–9 scales to express the pairwise comparisons of the BWM, and then obtains optimal weight vector by constructing the following optimization model (M-1)
(M-1):


Next, on the basis of the multiplicative consistency of q-ROF preference relation, we propose extended q-ROF-BWM to determine the weights of the attributes and solve a mathematical programing problem, where the MD and NMD of the q-ROF assessment information on criteria weights are jointly considered. Detailed procedures are as follows:



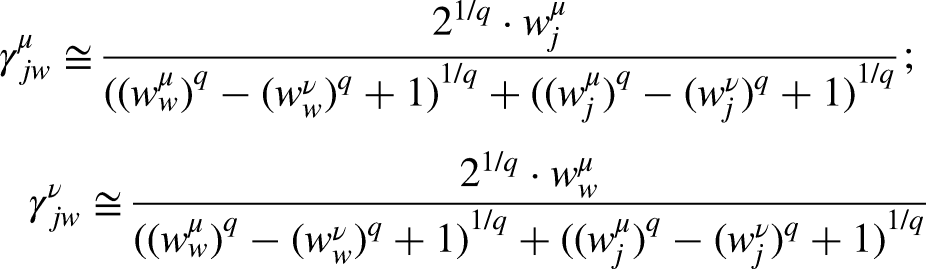




For convenience, 

According to Bellman and Zadeh's extension principle,
31
Wan and Dong's IFS extension principle, we view q-ROF decision R as a q-ROFPR R:




(M-2)


The q-rung orthopair fuzzy AC DHYM operator

Based on the new operational rules for q-ROFNs in the “Preliminaries” section, the following theorem can be obtained.
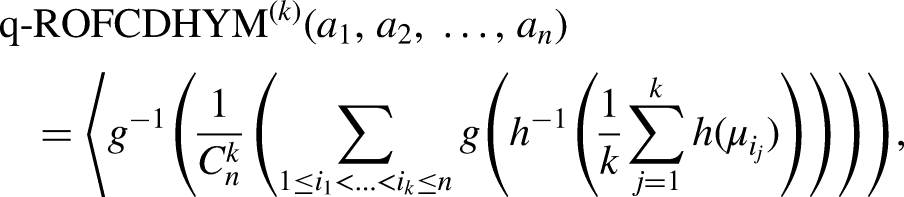















In the following, we can investigate some desirable properties of the q-ROFCDHYM operator.

The q-rung orthopair fuzzy weighted AC DHYM operator
The q-ROFCDHYM operator does not consider the importance of the input arguments. To overcome the limitation of the q-ROFCDHYM operator, we propose its weighted form (q-ROFWCDHYM).

Similarly, we can obtain the following theorem according to the interaction operational rules of q-ROFNs.

A new MAGDM algorithm with unknown weight information
In this section, we shall apply the proposed weighted determination method and aggregation operators to solve MAGDM problems under q-rung orthopair fuzzy environment.
A typical q-rung orthopair fuzzy MAGDM problem can be described as: Let X = (x1, x2, ..., xn) be a collection of alternatives, C = {C1, C2, ..., Cn} be n attributes and D = {D1, D2, ..., Ds} be a collection of decision makers. For attribute Cj (j = 1, 2, ..., n) of alternative xi (i = 1, 2, ..., n), decision maker Ds is required to utilize q-ROFN to express his/her evaluation value, which can be denoted as
For the sake of selecting the best alternative, a MAGDM algorithm based on q-ROFWCDHYM-EBWM can be developed and the key steps of the algorithm are provided as follows:

To clarify the MAGDM algorithm based on q-ROFWCDHYM-EBWM, we also plot a flowchart Figure 2.
Results
This section discusses the practical application and overall results of the proposed MAGDM based on q-ROFWCDHYM-EBWM for medical alliance comprehensive performance evaluation in China. In the first section, practical application is discussed. Next, the influence of different parameters k, q, and different types of generator on the decision results are also mentioned.

Flow chart of multi-attribute group decision-making (MAGDM) based on q-ROFWCDHYM-EBWM.
The practical application to medical alliance comprehensive performance evaluation in China
In April 2017, “Guiding Opinions on Promoting the Construction and Development of Medical Alliance” is issued by the General Office of the State Council, which once again triggered heated discussion on the medical alliance. Medical alliance is usually composed of a tertiary hospital, several secondary hospitals, and community health service centers. Although “medical alliance” and “hierarchical diagnosis and treatment” literally focus on “alliance” and “division” respectively, they share common ultimate goals, such as the effective sharing of quality medical resources, upward and downward flow of doctors, two-way referral of patients, and building an orderly medical treatment order. The construction of a medical alliance is an important measure for deepening the health system reform in China and plays an important role in promoting resource sharing, doctors’ flow up and down, two-way referral, and construction of ordered visits. China has experienced medical alliance exploration for nearly twenty years, but the siphon effect of large general hospitals on doctors, patients, and healthcare costs remains unchanged, and the establishment of a reasonable medical treatment is still difficult. One of the existing problems is that the importance of medical alliance evaluation is ignored, which leads to the shortage of related research, affecting the scientificity and efficiency of decision-making. In June 2021, in order to guide and assist local governments in accelerating the completion of the hierarchical diagnosis and treatment system, and continuously promoting the construction of medical alliance during the 14th Five-Year Plan period, the National Health Commission decided to establish an expert group for promoting the construction of hierarchical diagnosis and treatment and medical alliance to evaluate and supervise the implementation of the construction of hierarchical diagnosis and treatment and medical alliance nationwide. When evaluating the operation effect of the medical alliance, attributes will be considered comprehensively, which is a typical multi-attribute decision-making problem. The MAGDM algorithm based on q-ROFWCDHYM-EBWM proposed in the “Results” section is an effective way to solve this problem. Therefore, in the present case, we focus on evaluating the comprehensive performance of medical alliance to provide decision-making reference and experiences for the construction of medical alliance in other parts of China at the same time. The comprehensive performance evaluation for medical alliance can be viewed as a MAGDM problem described as follows:
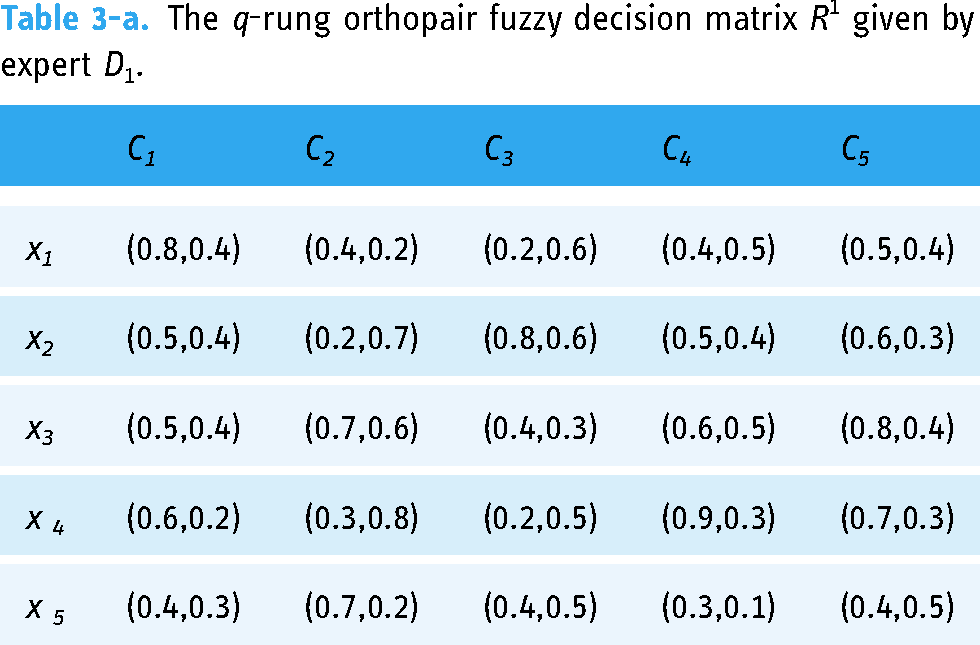
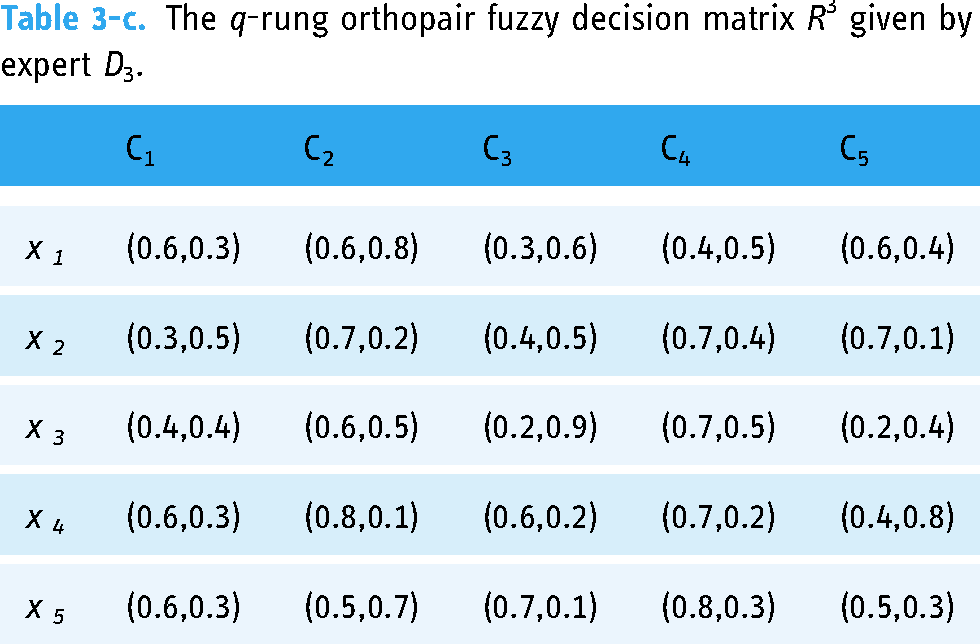
To explore and analyze the operating effect of medical alliance in Shanghai, five primary health care institutions in the medical alliance system, denoted by xi (i = 1, 2, 3, 4,5), need to be evaluated. According to the standard of “Medical Alliance Comprehensive Performance Evaluation Index System” in the working plan for comprehensive performance evaluation of medical cooperation (Trial) issued by the National Health Commission, 49 the operating effect of medical alliance of the five primary health care institutions are evaluated from the following four indicators (attributes). Satisfaction degree of patients and medical staffs (C1): describes the patients and medical staffs’ comprehensive attitudes to the service quality of the hospital and may be the most comprehensive indicator. The situation of organization and implementation (C2): Organization and implementation are very important in the medical alliance, including assessment and incentive mechanism for promoting medical resource integration and sinking in medical alliance, the implementation plan of medical alliance construction. Up and down connection of medical resources (C3): here we use the information platform construction and local shared resources to express the up-and-down connection of medical resources, for it is one of the comprehensive indicators for showing the input-output efficiency of the medical alliance. Division of labor and cooperation (C4) including continuity of medical care and establishment of cooperative system. Continuity of medical care means patients needed to be provided continuous services of diagnosis, treatment, rehabilitation, and long-term care for patients. Meanwhile, superior hospitals need to provide priority services for referral patients such as receiving, checking and hospitalization. Resource sinking and two-way referral C5: it can be viewed as the number and proportion of professional technical/management personnel dispatched to primary medical and health institutions by second-level or above medical institutions in the medical alliance. The proportion and growth rate of the number of diagnosis and treatment in primary medical and health institutions is also a typical indicator to evaluate the performance of the hospitals. Suppose that the expert group gives the rating values for the five primary health care institutions with respect to attributes Cj by the q-ROFNs, and the decision matrices are shown in Tables 3-a, 3-b, 3-c.
The q-rung orthopair fuzzy decision matrix R1 given by expert D1.
The q-rung orthopair fuzzy decision matrix R2 given by expert D2.

The q-rung orthopair fuzzy decision matrix R3 given by expert D3.
The decision making process
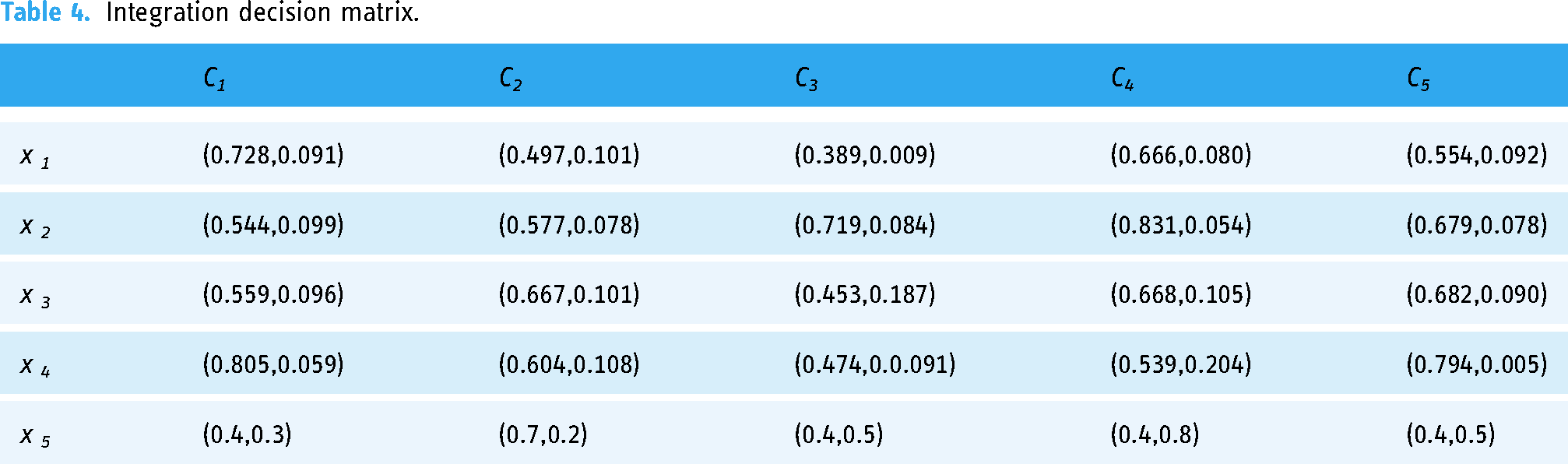
We apply the proposed algorithm based on q-ROFWCDHYM-EBWM in the “Results” section to address the problem:
Integration decision matrix.
Score values and ranking results obtained by q-ROFWCHYM-EBWM operator with diverse Archimedean copulas.

According to the Table 5, setting 





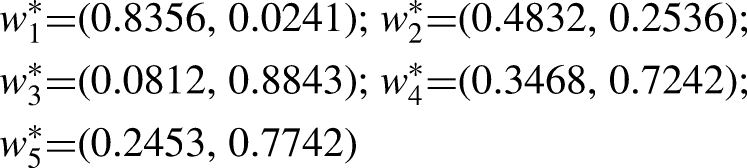
Then, we have

Comparison of all criteria with the best and worst criteria.
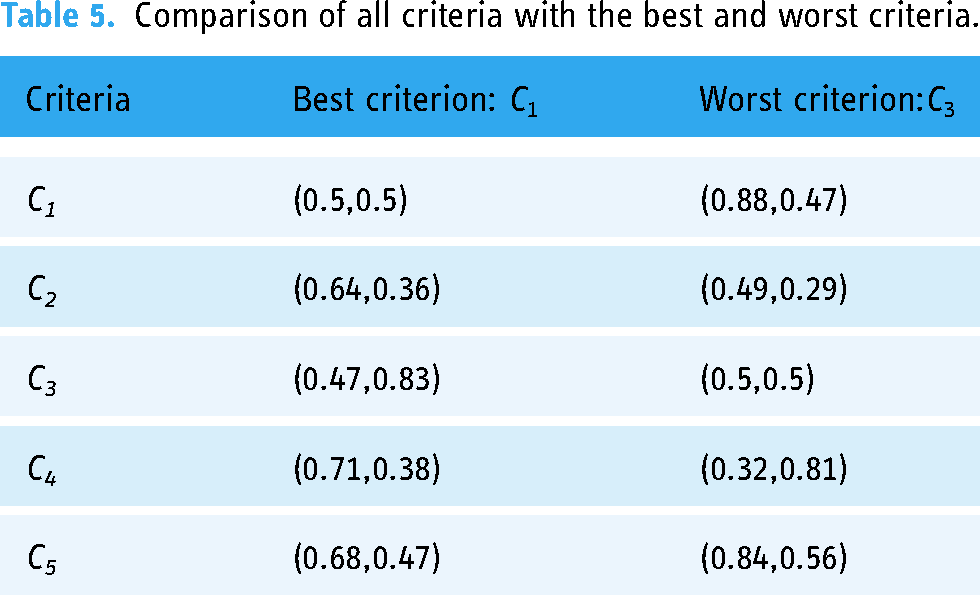
Then, a crisp mathematical programing model can be built by equation (37)









The influence of parameters k, and q on the results
There are accompanied parameters in the AC weighted DHYM operators, thus, in this section, we discuss the influences of different parameters k,

The variation tendency of score values of the five primary health care institutions when q
Ranking order of the five primary healthcare institutions for different parameters k.

Moreover, according to Table 6, it is easily found that the more the interrelationships s are taken into account, the smaller the score values of overall assessments will become, which is the difference between q-ROFWCHYM operator and q-ROFWCDHYM operator. The larger the value of the parameter k, the more the interrelationships among arguments are taken into account. Meanwhile, q-ROFWCDHYM operator can represent q-ROFWA operator by setting k = 1, which gives DMs flexibility in the decision process. In a word, an appropriate value of parameter k can not only capture the interrelationship among criteria, which definitely has an effect on the final ranking, but also further make the ranking result more objective and convincing.
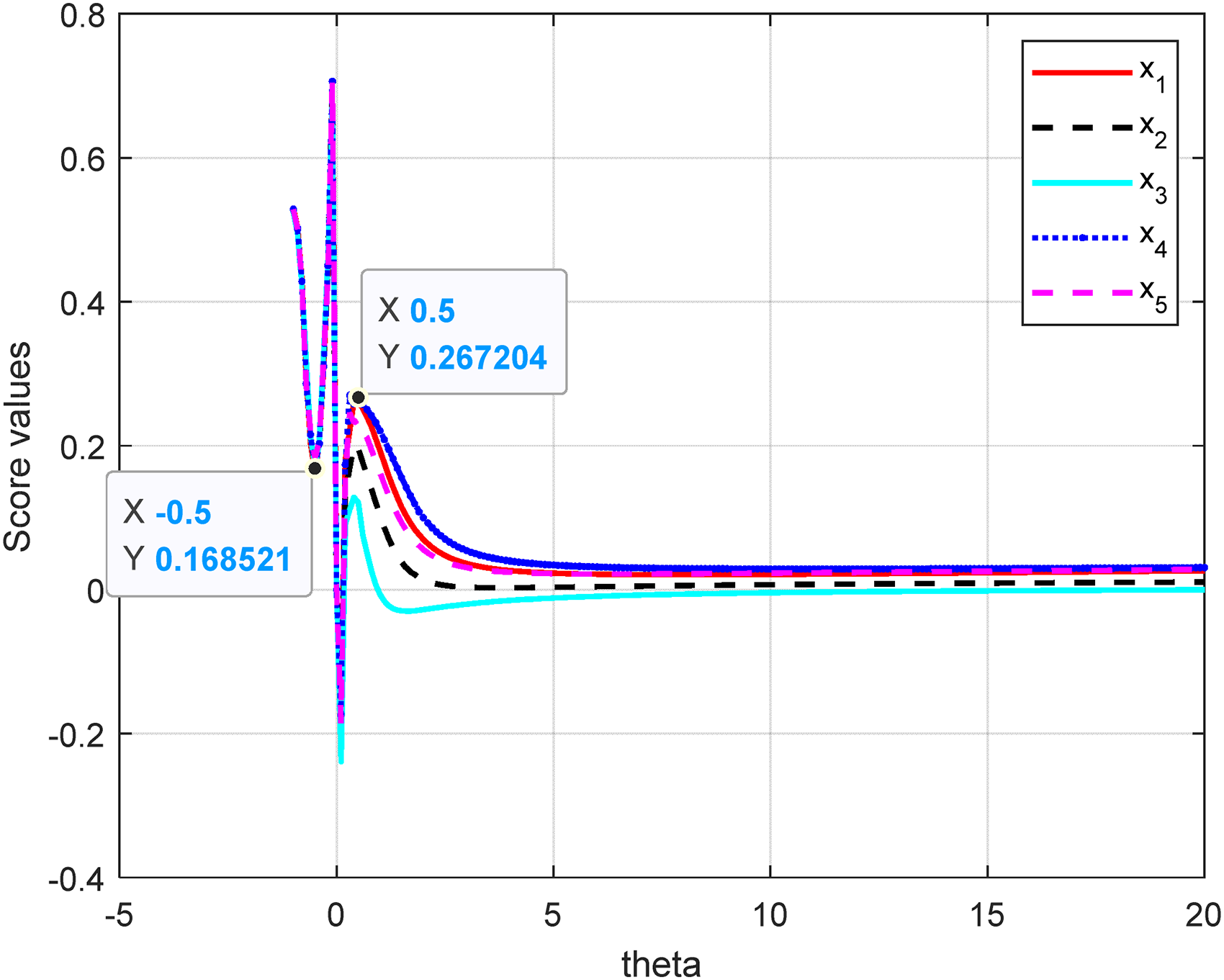
The variation tendency of score values of the five primary health care institutions with different parameters θ.
Figure 4 shows the variation tendency of score values of alternatives obtained by the q-ROFWCDHYM-EBWM operator with different parameters θ. As can be seen from the curve change in Figure 4, the parameter θ has significant effect on the score values of alternatives, but has negligible and slightly influence on the ranking results. The specific results are as follows: (a) When θ∈[−1, −0.5), the change of θ brings a sharply decrease in score values by q-ROFWCDHYM-EBWM, correspondingly, when θ∈[−0.5, 0), and [0, 0.5), the change of θ brings a sharply increase in score values by q-ROFWCDHYM-EBWM and the ranking result basically keep consistent. When θ∈(0. 5, 5], the ranking result is x4> x1> x5> x2> x3, and the score value decreases very sharply and then increase slowly accordantly with the parameter increasing. Then, the score values obtained by the q-ROFWCDHYM-EBWM operator increase smoothly and approaches stationary accordantly with the parameter increasing when θ∈[5, 20], and the influence of the parameter θ on score values is weaker with the increase of parameter θ, and finally the score values are very close to a fixed value, no matter the value of θ. The sensitivity analysis demonstrates how changes in the parameter θ affect the ranking result. Thus, we recommend the value range of the parameter θ reduce to a smaller interval within the definition domain, for example, [0.5, 5].
Decision results obtained by different types of generator produced by diverse ACs
In this section, we show the experimental result from different special forms on the basis of the different additive generators.
As we know, in the proposed AC, there are a family of AC with five different types. Therefore, we can use some special cases of the proposed five generalized operators to cope with the problem above. We suppose q = 4, k = 2 in the different ACs types, and the ranking results and order are listed in Table 7.
From Table 7, although the score values of alternatives generated by diverse operations from AC types, the final sorting relations are basically similar with slightly inconsistencies. The proposed q-ROFWCHYM-EBWM under different AC types is effective. From the above analysis, we can choose appropriate value of parameters and the suitable AC operator to meet the various actual requirements. Consequently, it is more feasible and flexible for decision making problem.
Management implications
Based on the above analysis results, we found that the medical alliance in Shanghai has differences in many dimensions, such as the ability organization and implementation, up and down connection of medical resources, and the realization of resource sinking and two-way referral. Among them, resource sinking and two-way referral are important factor for the construction of medical alliances. First, the sinking of resources in the medical union is limited. Although Shanghai came out the policy of “strengthening the grassroots,” the problem of brain drain’ has been improved in recent years. However, the salary of grassroots medical staff is not significantly improved, and the outflow of talent is still prominent. Second, the development of information connectivity within the medical alliance is slow and unsynchronized, and the level and scale of informatization are uneven. Medical institution in medical union cannot exchange and achieve adequately patient's information timely to communicate, which restrict the development of the medical alliance. These differences among primary health care institutions in the medical alliance system directly have an effect on its ability to optimize the allocation of medical resources, hierarchical diagnosis and treatment, and the service level of primary medical institutions. Thus, to optimize the governance pattern of medical consortium, Shanghai should learn from the successful experience of medical alliance, establish management committee of medical alliance to solve the problem of multi-management of the development of medical alliance, and promote the cooperation and resource sharing within the medical alliance.
Discussion
To further illustrate the reliability and superiority of the proposed methodology, a comparison discussion with the previous methods is carried out in this section. The comparison process is based on two aspects: Discussion of the existing BWM weight method towards different environments (i.e., crisp values, different fuzzy sets, and proposed q-ROF settings), and discussion of the relevant information aggregation operators. In addition, the limitations of this study are also discussed in this section.
Comparison with the existing fuzzy BWM weight method
We compare the results derived by the proposed BWM with those obtained by the existing BWM, including the crisp BWM, 41 intuitionistic fuzzy BWM (IFBWM), 42 q-ROF-BWM, 24 q-ROF score function-based BWM 44 and the developed q-ROF-EBWM, the final criteria weights generated by these approaches are displayed in Table 8.
Ranking results based on different weight methods.

q-ROF-EBWM: q-rung orthopair fuzzy Euclidean best-worst method; IFBWM: intuitionistic fuzzy best-worst method.
As Table 8 displays, the rankings positions of criteria weights generated by the five approaches are significant differences. Table 9 shows that the crisp BWM, the intuitionistic fuzzy BWM method cannot solve the above weight problem as the MD and NMD
Ranking results based on different MAGDM methods.
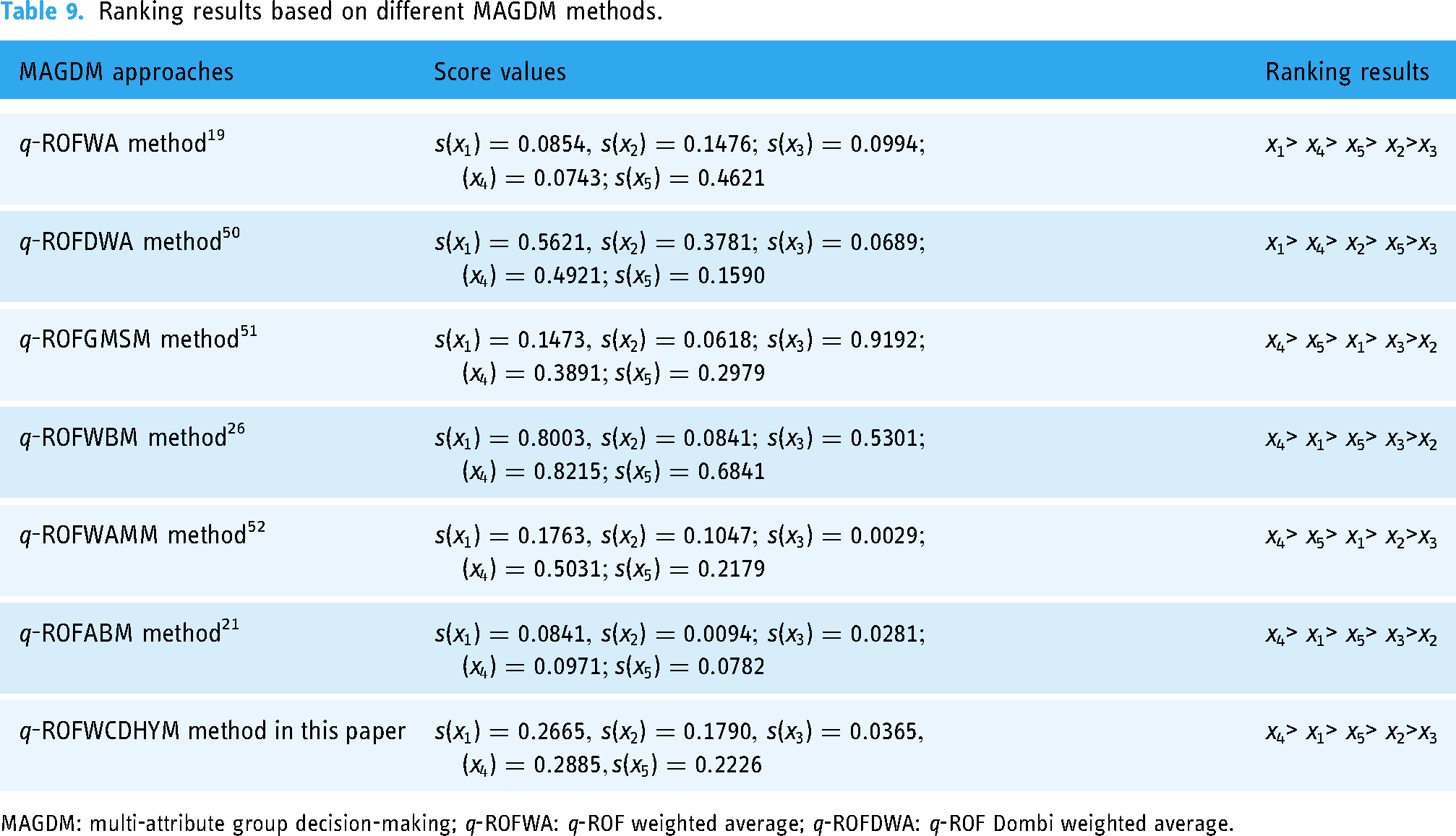
MAGDM: multi-attribute group decision-making; q-ROFWA: q-ROF weighted average; q-ROFDWA: q-ROF Dombi weighted average.
Thus, we can further draw the conclusion that the developed q-ROF-EBWM is superior to some existing BWM methods to some to some degree on the basis of multiplicative consistency and the normalization processing technique for weights. The developed q-ROF-EBWM not only studies the multiplicative consistency of the given q-ROF preference vectors but also gives an alternative for tackling q-ROF number using the BWM.
Comparison with the existing q-ROF aggregation operators
In this section, an analysis is conducted to explain the multiple advantages of the proposed approach. Considering the proposed approach is based on q-ROFCDHYM operator that combine copula and co-copula operational rules, and HM within q-ROFS environment, we choose the following as reference approaches to solve the above medical alliance comprehensive performance evaluation, i.e., q-ROFWA method proposed by Liu and Wang, 19 the q-ROF Dombi weighted average (q-ROFDWA) method proposed by Jana et al., 50 q-ROFGMSM method proposed by Liu and Wang, 51 q-ROFWBM method proposed by Liu and Liu, 26 q-ROFWAMM method proposed by Qin et al., 52 q-ROFABM method proposed by Liu et al.. 21 The ranking results yielded by the different approaches are shown in Table 9.
Table 9 shows the optimal primary health care institutions obtained by the proposed method is consistent with most of the other existing methods, except that the results obtained by the first two methods are different. These similarities and consistency of the results prove the validity of the proposed method. Although all approaches recognize that A1 or A4 are the best among the five primary health care institutions, only A1 is ranked first in the first two methods. As we can see from the Table 9, the rankings obtained by the first two methods are x1> x4> x5> x2> x3 while the rankings obtained by the last four methods and proposed method is x4> x1> x5> x2> x3, respectively. Clearly, by using the q-ROFWA and q-ROFDWA method, the optimal primary health care institution is A1, while the best is A4 using the proposed q-ROFWCDHYM-EBWM method. For the above results, the difference in results can be explained for two reasons. Firstly, the main reason is that the proposed method considers correlation among attributes in the process of information aggregation, while the q-ROFWA and q-ROFDWA method fail to consider it and neglect the relevance of dissimilar evaluation information. Through the q-ROFGMSM and q-ROFWBM method considers correlation among attributes, the ranking is x4> x5> x1> x3> x2, the west primary health care institutions obtained by q-ROFGMSM and q-ROFWBM methods is changed from x3 into x2 compared to the proposed method, but the same evaluation results regarding best primary health care institutions stay consistent. Secondly, the first four methods are all on the basis of algebraic operations or Dombi operations, and thus lacks generality. In comparison, the proposed q-ROFWCDHYM operator provides more general operations on the basis of ACs. Specially, when θ=1 in Gumbel-copula and Joe-copula, they will reduce into Algebraic operations, i.e., the q-ROFWCDHYM operator is more generalized compared with q-ROFGMSM method and q-ROFWBM method.
Next, we compare q-ROFWCDHYM-EBWM method with the q-ROFABM and q-ROFWAMM method. As we can see from the Table 9, the optimal primary health care institutions obtained by q-ROFABM and q-ROFWAMM method are in line with the results obtained by the proposed method, but the ranking are basically similar with slightly inconsistencies. For example, compared to q-ROFWCDHYM method, when the q-ROFAMM method is applied, the relationship between x1 and x5 is in the second and third position, respectively, and when the q-ROFABM method is applied, the relationship between x2 and x3 is in the fourth and fifth position through q-ROFAMM method respectively. It is due to that both of these methods are based on BM or MSM operators and thus consider the interrelationship of attributes. The reason for the slightly different results comes from that the q-ROFABM and q-ROFWAMM method are based on the AC generator while the proposed method is based on the copula generator. Moreover, criteria weights in the q-ROFABM and q-ROFWAMM method are predefined subjectively, while the proposed approach can obtain DMs’ preference and get the complete q-ROF rating matrix, further improve the effectiveness of BWM. Therefore, the ranking result obtained by the proposed method is more reasonable and more useful in determining weight than subjectively given weight.
In summary, the above comprehensive analysis shows the effectiveness of the proposed q-ROFWCDHYM method, and can solve medical alliance comprehensive performance problems.
Following the above analysis of the differences quantitatively, we further investigated the differences from a qualitative perspective. In Table 10, a comparison of the characteristics of these methods with our proposed method is presented.
Characteristics of different MAGDM methods.

MAGDM: multi-attribute group decision-making; q-ROF-EBWM: q-rung orthopair fuzzy Euclidean best-worst method; q-ROFDWA: q-ROF Dombi weighted average; q-ROFWA: q-ROF weighted average.
Table 10 demonstrates the summary results of the qualitative comparison analyses. Although all the above approaches are rooted in classical BM, MSM, HM, or WA, all have different from the classical methods. The merits of the developed method based upon q-ROFWCDHYM-EBWM during the course of information integration are listed below:
From the perspective of the weight method, most current studies on criteria weights are predefined subjectively, which leads to less comprehensive solutions and a biased view of the complex MAGDM problem. In the process of information aggregation, how to solve the weight of attributes is a key step, which can directly affect the reliability of results. In the proposed q-ROFWCDHYM-EBWM method, we employ a new BWM weight determining method. BWM is a widely used weight method and has the characteristics of simplicity, accuracy and less redundancy. DMs only need to identify the best and worst desirable criteria, and then make pairwise comparisons between the best/worst criterion and the other criteria. q-ROFS can describe the nature of uncertainty of objective things more flexibly and clearly and provides a new idea. Thus, utilization of q-ROFS, instead of crisp BWM, makes it easier for DMs to tackle uncertainties, and has been found more robust and useful in determining weight than subjectively given weight. From the perspective of fuzzy BWM expression: the existing q-ROFBWM and other fuzzy BWM are all based on the traditional BWM, so they have similar computational complexity. However, under q-ROF environment, the best-to-others vector and others-to-worst vector are all q-ROF vectors, the existing q-ROFBWM and other fuzzy BWM divide the MD and NMD separately to construct q-ROF programing model, or by using the division and subtraction operations laws of q-ROFs to transform it into a crisp programing model, which cannot consider jointly both MD and NMD and lose the essence of the BWM on the basis of the membership part and non-membership part. Our proposed extended q-ROFEBWM method solves the problem by constructing q-ROF equations satisfying multiplicative consistency to transform it into a crisp programing model that can integrate the MD and NMD of the q-ROF assessment information on criteria weights, and get a globally optimal solution. At the same time, the obtained q-ROF weight vector is normalized and satisfies multiplicative consistency of the q-ROFPR, respectively. Thus, the weights derived from the q-ROFEBWM are reliable because the approach is developed on the basis of definition of the consistent q-ROFMPRs. From the perspective of the operational laws and aggregation method, the proposed q-ROFWCDHYM-EBWM can capture correlation among attributes simultaneously in the process of information aggregation, and it also can handle case where the weight is unknown. However, the classical q-ROFWA and q-ROFDWA methods consider all pondered attributes are irrelevant and neglects the relevance of dissimilar evaluation information. Although the q-ROFWBM and q-ROFGMSM operators can deal with the correlation of attributes, they are based on the algebraic operational laws which lack flexibility and generalization for decision information integration. However, the proposed q-ROFWCDHYM-EBWM method can validly conquer these above-mentioned shortcomings which are illustrated as follows: It combines the concepts of q-ROFs and ACs normally used as tools to combine probability distributions, and constructs a general way by selecting different copula to obtain different aggregation operators and further obtain a general MAGDM method by choosing diverse flexible parameter adjustment copula generator. Moreover, it considers the relationship between the attributes in the decision analysis process with the help of the HYM operator and establishes a flexible parameter algorithm by different generators, which provides more choices for selecting appropriate parameters that meet DMs’ preferences. Thus, the parameters in each copula reflect the flexibility and robustness of the proposed q-ROFWCDHYM-EBWM method and it conquers the shortcomings of the most of pre-existing fuzzy operators. Especially, when θ=1 in Gumbel copula and Joe copula, they will reduce into Algebraic operations, i.e., the q-ROFWBM operator is a particular case of the q-ROFWCDHYM operator.
In summary, the proposed MAGDM approach provides general operations on the basis of ACs with q-ROF fuzzy set and BWM method, making the best of both the membership and non-membership information in the rating matrix to handle MAGDM problem with unknown weight information. Moreover, the comparison of the solution results obtained from three perspectives demonstrate the feasibility and the effectiveness of the q-ROFWCDHYM-EBWM method. Thus, the proposed method provides important theoretical guidance to help manager clearly find the current development status of e primary health care institutions in the medical alliance system.
Limitations
However, like other methods, the proposed method also has some limitations. The most important weakness of the method is that the decision matrix elements must belong to q-rung orthopair fuzzy sets. Thus, for future research, it is suggested that this issue be further generalized to other fuzzy sets, e.g., complex q-rung orthopair fuzzy sets and T-spherical fuzzy sets, 53 to study new MAGDM method by integrating different operational laws, such as neutrality operators, 54 Aczel-Alsina t-norm and t-conorm, 55 etc. In addition, it is recommended to integrate the proposed q-ROF-EBWM weight method with other MAGDM methods, combined compromise solution (CoCoSo) method, 56 ordinal priority approach. 57 Also, the application of the method proposed in this paper to large-scale group decision-making 58 and consistency adjustment of social networks 59 is worthy of further exploration and research.
Conclusion
In this paper, we develop a hybrid decision algorithm based on AC and ACC HYM aggregation operator under q-rung orthopair fuzzy environment and q-ROF-EBWM weight programing approach based on the multiplicative consistency to evaluate medical alliance comprehensive performance. This result shows the proposed MAGDM approach is applicable for government to evaluate the medical alliance comprehensive performance. Therefore, the proposed method provides recommendations for China's medical alliance reform by evaluating five primary health care institutions in the medical alliance system, and also provides case references for medical resource allocation in other regions. This result shows the proposed MAGDM approach is valuable for government to evaluate the medical alliance comprehensive performance.
The contribution of the work is briefly as follows: (a) The extended q-ROF-EBWM approach is proposed to derive the normalized optimal weight vector satisfying multiplicative consistency. (b) After determining the weights, in the second stage, new AC and ACC operational rules of q-ROFNs are defined, and q-rung orthopair fuzzy AC and ACC HYM aggregation operators are developed. (c) To evaluate medical alliance comprehensive performance, a new and general MAGDM algorithm based on the proposed q-ROFWCDHYM-EBWM is provided to solve the MAGDM problem with unknown weight information. The advantages of the proposed work are that the new MAGDM approach provides a general way and more choices that meet DMs’ preferences on the basis of ACs with q-ROF fuzzy set and BWM method, and can be applied to a more extensive range of information. Moreover, the new MAGDM approach not only can reveal the relationship among attributes and keep more original information in the process of aggregating information, but also avoid the irrationality of considering membership and non-membership functions separately when determining the weights.
Footnotes
Acknowledgments
We would like to express our gratitude and appreciation to all those participants who gave us suggestions to complete this study.
Consent for publication
All the authors approved the final version of the manuscript.
Contributorship
Y.X. proposed the idea and drafted the initial manuscript, contributed to the revised version of the manuscript in model selection, data processing and analysis. J.W. was involved in conception and design of the study, provided the study materials, finally revised and checked the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Shanghai Office of Philosophy and Social Science (2021EGL001), MOE (Ministry of Education in China) Project of Humanities and Social Sciences (22YJC630169), Shanghai Science and Technology Development Funds (Rising-Star Program-Sailing Program (22YF1401400), and Funds for First-class Discipline Construction in Beijing University of Chemical Technology (XK1802-5).
Guarantor
Y.X.