
Abstract
Objective
Mild cognitive impairment (MCI) due to Alzheimer's disease (AD), as an early stage of AD, is an important point for early warning of AD. Neuropathological studies have shown that AD pathology in pre-dementia patients involves the hippocampus and caudate nucleus, which are responsible for controlling cognitive mechanisms such as the spatial executive process (SEP). The aim of this study is to design a new method for early warning of MCI due to AD by dynamically evaluating SEP.
Methods
We designed fingertip interaction handwriting digital evaluation paradigms and analyzed the dynamic trajectory of fingertip interaction and image data during “clock drawing” and “repetitive writing” tasks. Extracted fingertip interaction digital biomarkers were used to assess participants’ SEP disorders, ultimately enabling intelligent diagnosis of MCI due to AD. A cross-sectional study demonstrated the predictive performance of this new method.
Results
We enrolled 30 normal cognitive (NC) elderly and 30 MCI due to AD patients, and clinical research results showed that there may be neurobehavioral differences between the two groups in digital biomarkers captured during SEP. The early warning performance for MCI due to AD of this new method (areas under the curve (AUC) = 0.880) is better than that of the Minimum Mental State Examination (MMSE) neuropsychological scale (AUC = 0.856) assessed by physicians.
Conclusion
Patients with MCI due to AD may have SEP disorders, and this new method based on dynamic evaluation of SEP will provide a novel human–computer interaction and intelligent early warning method for home and community screening of MCI due to AD.
Keywords
Introduction
Alzheimer's disease (AD) is one of the most common neurodegenerative diseases.1,2 A large number of patients, increasing prevalence with an aging population, high social costs, no effective cure, and other factors have made AD a major medical and social concern worldwide. 3 Mild cognitive impairment (MCI) due to AD is defined as the symptomatic predementia phase of AD. 4 Some studies have found that appropriate intervention at the MCI due to AD stage has the potential to halt or even reverse AD progression. 5 Therefore, MCI due to AD is an important point for early warning of AD.6,7 However, the onset of AD is insidious and the latent phase before the onset of clinical syndrome can last for decades. Accurate diagnosis and large-scale screening of MCI due to AD, as the symptomatic predementia phase of AD, is also a recognized challenge in the field of medical health. The current clinical screening methods with high diagnostic efficacy, such as cerebrospinal fluid screening (CSF), blood biomarker testing, positron emission computed tomography (PET), and magnetic resonance imaging (MRI), have the bottlenecks of being expensive and difficult to promote large-scale early screening in the community.8–11 In addition, neuropsychological scales such as the Minimum Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA), which are widely used in AD screening, have bottlenecks of relying on doctors’ on-the-spot evaluation, intense subjectivity, time-consuming, and insufficient early warning efficacy for early-stage patients with a highly educated background.12–14 Therefore, the above bottlenecks in clinical examination methods such as imaging, biology, and neuropsychological scales have led to a low diagnosis and a high underdiagnosis rate of MCI due to AD, resulting in many patients at this stage losing the best time to intervene. They also limit large-scale early screening for MCI due to AD at home and in the community, especially in developing countries, where medical resources are significantly inadequate. 15 Therefore, there is an urgent need to develop new intelligent early warning methods suitable for large-scale early detection of MCI due to AD at home and in the community.
Current neuropathological studies suggest that the hippocampus is the first site to be eroded by pathological changes in AD.16–18 The hippocampus, as the most important subcortical brain region involved in learning memory functions, plays an important role in spatial and episodic memory. Spatial and episodic memory impairments are also the most prominent manifestations of cognitive impairment in the early stages of AD. In addition, some studies have shown that the caudate nucleus, which plays a key role in supporting the planning and execution of behaviors needed to achieve goal-directed tasks, will also be involved in AD pathology.19,20 Executive function is defined as a cognitive mechanism, and impairments in executive processes resulting from damage to the caudate nucleus are also increasingly considered to have potential as a marker for early screening for AD.20,21 In addition to its memory function, the hippocampus also plays a guiding role. The ability to store and process spatial information involved in the hippocampus is crucial for humans to complete goal-oriented spatial execution tasks. And the core of many tests used to evaluate memory and learning ability is the evaluation of the spatial executive process (SEP).21–23
Handwriting is a complex act of spatial execution in humans that requires a complex mixture of cognitive, kinesthetic, and perceptual movements. 24 The characteristics of writing behavior during handwriting task execution can respond not only to participants’ executive functions but also to their higher-order neurocognitive decision making, information processing speed, memory, and other cognitive domain functions. 25 Tests related to “handwriting behavior pattern” have been shown to be sensitive to the cognitive abilities of patients with MCI due to AD.26,27 Several studies have also demonstrated the correlation between “handwriting behavior pattern” and hippocampal and caudate pathological changes through medical imaging.28–30 Moreover, because of its low cost, high acceptance, and short completion time,25,31 the “handwriting behavior pattern” has been widely used in rapid screening for major neurological disorders such as AD and Parkinson's disease (PD).24,32 Several studies have demonstrated the feasibility and effectiveness of handwriting tasks for cognitive detection based on human–computer interaction (HCI) early warning technology and digital devices.26,27,33,34 Physiologically and behaviorally relevant “digital biomarkers” captured by digital and intelligent devices are objective and quantifiable, and they can compensate for the shortcomings of traditional diagnostic methods that are clinician-dependent, subjective, and difficult to quantify diagnostic results.35–37 In addition, digital biomarkers have higher diagnostic accuracy and a lower rate of missed screening in the early diagnosis of neurological diseases such as AD, which are difficult to be early warned due to their insidious onset, and therefore have a good potential for clinical application.35–41
However, most of the current commonly used AD handwriting assessment methods require the use of digital writing tools (such as digital pens or electromagnetic pens) to write on the touch screen or digital board.42,43 These digital writing tool-based assessments increase the cost of screening equipment and have some unavoidable drawbacks. For example, handwriting evaluation results are influenced by individual differences in pencil grip and individual familiarity with electronic devices.43,44 What's more, many studies followed the traditional “brain partitioning” theory to rigidly divide individuals’ integrated information processing abilities into different modules in the cognitive process. Moreover, they did not reflect the entire cognitive assessment process in dynamic time series.45–47
Recently, Peter Stern presented a new idea in Science that brain neurons do not function in isolation but rather in connection and communication between different regions. The emergence of behavior and cognition also stems from the interaction between cortical areas. 48 The above views are in line with Villemagne et al., 49 who argued that AD pathology affects a wide range of brain functions.
In our previous research work, we found a comprehensive capability indicator that can dynamically measure the entire spatial task execution process: the spatial execution process. 50 It is related to both hippocampus-dependent memory and orientation abilities and executive processes deficit (including full-process optimal decision-making and fingertip executive dynamic abilities) controlled by the caudate nucleus.20,21,50–52 Based on this, the hypothesis that “there are neurobehavioral differences between normal cognitive (NC) elderly and MCI due to AD patients in digital biomarkers captured during the spatial execution” was proposed. And we designed a smart 2-min mobile alerting method for MCI due to AD in the community. This 2-min alerting method used a mobile tablet device to dynamically and intelligently assess participants’ SEP under a new spatial interaction task we designed, with the advantages of fast screening and low economic cost. However, we found that the paradigm in this method (control of the target sphere around obstacles by fingertip interaction to eliminate target squares) had poorer warning efficacy for low-education MCI due to the AD population with less than 9 years of educational experience. This may be due to the lower acceptance and operational proficiency of smart devices in the less educated elderly population.
Therefore, we have improved on our previous work and developed a new method for screening MCI due to AD patients with higher accuracy, age-friendly, and more generalizability. We continued to use the fingertip interaction format and designed a new early warning method for MCI due to AD based on dynamic evaluation of the SEP by incorporating two handwriting tasks, “clock drawing” and “repetitive writing.” These are more commonly used in neuropsychological tests and usually used in the clinical diagnosis of MCI due to AD. By intelligently capturing the task performance of MCI due to AD in fingertip HCI tasks, the new early warning method achieves objective quantitative analysis of the entire data, thus achieving effective intelligent early warning for MCI due to AD in the home, community, and other nonphysician environments.
Methods
HCI software design
Fingertip interaction handwriting digital evaluation paradigm design. Since “clock drawing” and “repetitive writing” are the two most common measures used to screen for MCI due to AD patients, we have designed the “fingertip interaction clock drawing paradigm” and “fingertip interaction repetitive writing paradigm” for MCI due to AD screening. Based on these two paradigms of fingertip interaction, we will collect spatial, temporal, and kinematic data on handwriting behavior patterns that can reflect MCI due to AD patients’ memory capacity, orientation ability, optimal decision-making, and fingertip executive dynamic abilities.16–23 We then used these data to assess participants’ SEP impairment during finger-writing tasks, enabling the assessment of cognitive function in MCI due to AD patients. The paradigms we have designed will replace the traditional “pen-holding writing” on paper media with “fingertip touch screen sensing.” And finger writing directly on the trackpad is in line with the concept of suitable aging and is more suitable for the intelligent assessment of the elderly (see Figure 1).

(a) Fingertip interaction capacitive touch screen, (b) fingertip interaction clock drawing paradigm, and (c) fingertip interaction repetitive writing paradigm.
Hardware and software architecture and data storage. We collect data through the capacitive touch screen of the fingertip interaction, the relevant parameters of which are shown in Figure 1(a). In designing the fingertip interaction software system, we used Visual Studio Code, Electron, and Vue front-end framework to build the desktop client. And the backend system was built based on the Fast API backend framework and scientific computing libraries such as NumPy and Pandas. We built a MySQL system database to store and manage the writing process data and the resulting image feature data (including finger position coordinates and corresponding time) of the finger interaction clock drawing paradigm and the repetitive finger interaction writing paradigm operated by the participants. We can draw paradigms’ “process-result” dynamic spatial trajectory maps based on the Echart mapping library (see Figure 2).
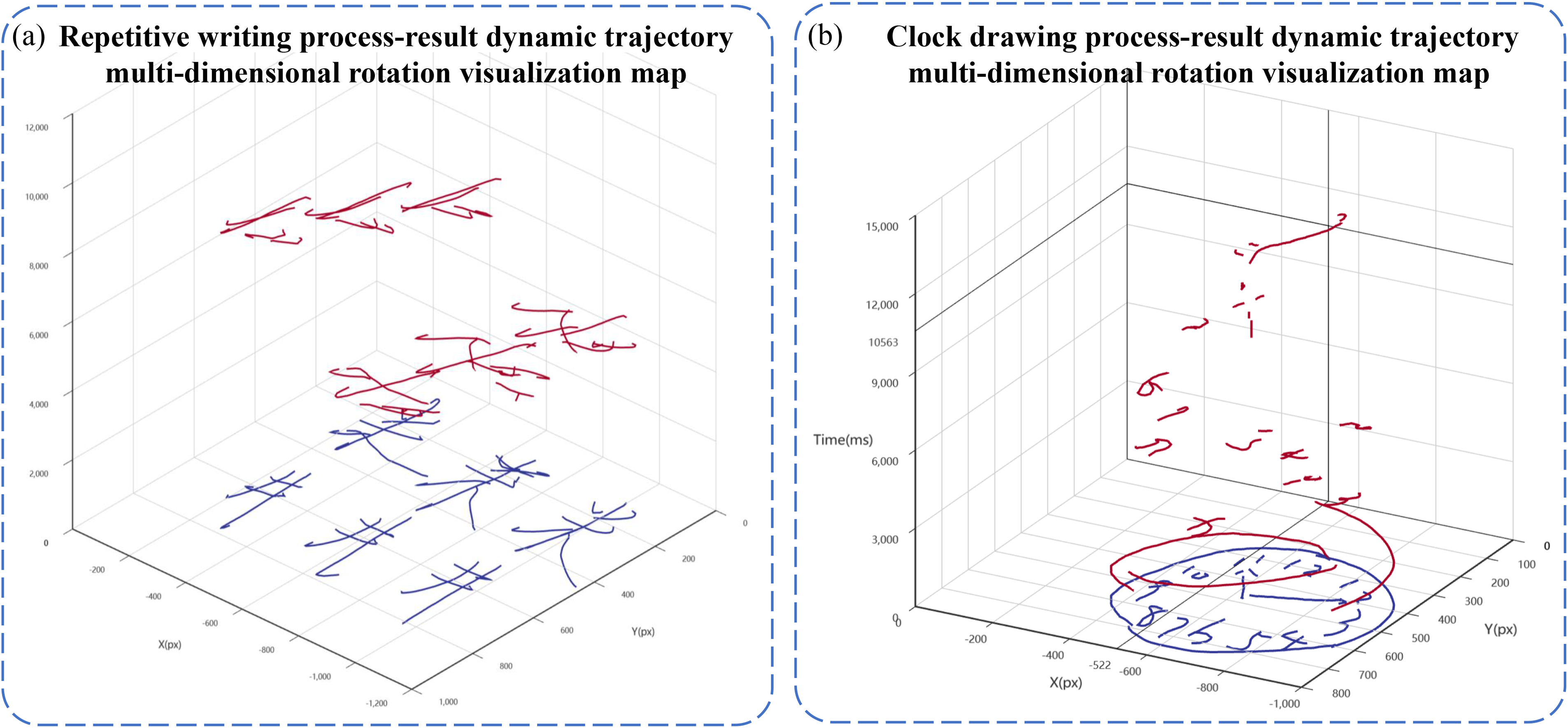
(a) Process-result dynamic trajectory multi-dimensional rotation visualization of repetitive writing, the black is the 2D trajectory, the grey is the 3D timing trajectory, the X and Y axes are the screen coordinates of the participant's handwriting, and the Z axis is the time, (b) Process-result dynamic trajectory multi-dimensional rotation visualization of clock drawing.
Fingertip interaction digital biomarkers extraction
With the use of digital biomarker extraction for fingertip interaction, we obtained data on drawing time, speed, and pause time during the two paradigms of finger interaction clock drawing evaluation and finger interaction repetitive writing evaluation via the finger interaction capacitive touch screen. In conjunction with the previous study, we set up three dimensions of digital biomarkers to provide intelligent warning to MCI due to AD patients from the perspective of spatial execution processes: (a) the digital biomarker dimension of execution speed signature and (b) the digital biomarker dimension of execution pause signature for evaluating optimal decision planning and fingertip execution dynamics dependent on the caudate nucleus19–21 and (c) the digital biomarker dimension of execution image signature for evaluating hippocampus-dependent memory capacity and orientation ability.16–18,22 Based on the above dimensions of digital biomarkers, we extracted fourteen digital biomarkers from two models of numerical fingerprint interaction handwriting evaluation, respectively.
Table 1 shows the digital biomarker dimension of execution speed signature, including four digital biomarkers: mean drawing speed (
The digital biomarker dimension of execution speed signature.

Table 2 shows the digital biomarker dimension of execution pause signature, including nine digital biomarkers: total task time (T), start writing time (
The digital biomarker dimension of execution pause signature.

Table 3 shows the digital biomarker dimension of execution image signature, including two digital biomarkers: the clock drawing process and resulting image feature score (
The digital biomarker dimension of execution image signature.

Intelligent analysis algorithms
We designed an intelligent analysis algorithm for fingertip interactive digital biomarkers analysis. It is suitable for analyzing the writing process and the resulting image features during the fingertip interaction clock drawing paradigm and the fingertip interaction repetitive writing paradigm. The following algorithms are general algorithms for digital biomarker analysis in two paradigms. We set the total task time as T, the start writing time as 



The drawing pause rate of clock is 




Second, we evaluated the resulting image features of the fingertip interaction clock drawing evaluation paradigm through the clock outline score, clock digit score, and clock hand score. The specific analysis method is as follows:
Based on the Open Source Computer Vision Library (OpenCV2), we realize the automatic preprocessing of the original clock image through the “open operation” in morphology. We “eroded” the clock images drawn by the participants to remove “burrs” and then “expanded” the clock images to prevent subsequent influence on the judgment of the closure of the outer contour of the clock. The formula for the “opening operation” is as follows:
We recorded binary clock profile scores based on contour edge detection techniques. If the clock profile is closed, the score is 1 or 0 otherwise. We used optical character recognition (OCR) and recorded the binary clock number score. If the clock numbers are complete and distributed clockwise, the score is 1 or 0 otherwise, as shown in Figure 3(a). We used a clock identification architecture from the space converter network (STN)
53
and recorded clock time scores in binary. If the clock time is recognized as 11:10, the score is 1 or 0 otherwise, as shown in Figure 3(b). The clock time reading formula is as follows:

Digital biomarker analysis algorithms: (a) the schematic diagram of the recognition of clock numbers, (b) the schematic diagram of clock time reading, and (c) the schematic diagram of Chinese character recognition of “repetitive writing.”
In the formula,
Third, we evaluated the resulting image features of the fingertip interaction repetitive writing paradigm. Based on the turtle library's handwriting restoration algorithm and OCR technology, we analyzed the stroke order of the participant and the resulting image during the repetitive writing process, as shown in Figure 3(c). If the participants’ stroke order and results are correct, the writing score will be 1 or 0 otherwise.
Experimental settings
In order to verify the clinical efficacy of the new early warning method for MCI due to AD based on dynamic evaluation of SEP, we conducted a cross-sectional study in the neurology department of a tertiary level A hospital in Zhejiang Province.
Participant recruitment
From June 2022 to September 2022, we enrolled 60 participants (27 males and 33 females) aged 55–80 in a hospital, including 30 NC elderly and 30 MCI due to AD patients. They were divided into the NC group and the MCI group. All recruited participants underwent clinical assessment and diagnosis by a neurologist (including laboratory tests, cognitive ability assessment, daily and general functional assessment, and psycho-behavioral assessment, and some patients underwent imaging tests such as MRI and PET). Individuals in the NC group were confirmed by clinical interviews not to show cognitive impairment or any signs of neurological or mental illness. The individual diagnosis of the MCI group met the clinical MCI diagnostic criteria developed by the National Institutes of Aging and Alzheimer's Disease Association in 2011, 4 including confirmed complaints of memory loss, objective memory impairment, retention of general cognitive function, complete daily activities, and no dementia.
Exclusion criteria included a history of mental illness such as schizophrenia, severe anxiety, and depression; meeting diagnostic criteria for PD, frontotemporal dementia, Lewy body dementia, or Huntington's disease; dementia caused by other causes, such as cerebrovascular disease and central nervous system trauma; aphasia, disturbance of consciousness, and other diseases affecting cognitive evaluation; severe arrhythmia; myocardial infarction occurring within 6 months; severe lung/liver/kidney dysfunction and severe gastrointestinal diseases; severe anemia; tumors; and a history of epilepsy or taking antiepileptic. In addition, participants in this study were right-handed.
The study design was approved by the Human Research Ethics Committee of Zhejiang Chinese Medical University (Approval Number: 20210806-1). All operations of this study were conducted in accordance with the relevant guidelines and regulations. After receiving a detailed description of the study, all signed informed consent. And all patient privacy data in this paper have been desensitized to protect patients’ privacy rights.
Experimental process
All participants were asked to sit at a table (see Figure 4(a) and (b)) and complete the digital evaluation of fingertip interaction handwriting with the index finger of the habitual hand in the blank area displayed on the touch screen according to the prompt of the fingertip HCI software system interface. In the fingertip interaction clock drawing paradigm, participants were prompted to draw an 11: 10 clock with their habitual hand index finger, including the contour, number, and pointer of the clock. Examples of drawing results are shown in Figure 4(c) and (d). In the fingertip interaction repetitive writing paradigm, participants were prompted to write two Chinese characters: “井” and “米” with their habitual hand and index finger. Each Chinese character must be written three times, as shown in Figure 4(e) and (f).

Evaluation scenarios and example results: (a) fingertip interaction clock drawing evaluation scene, (b) fingertip interaction repetitive writing evaluation scene, (c) examples of clock drawing result of NC, (d) examples of clock drawing result of MCI, (e) examples of repetitive writing result of NC, and (f) examples of repetitive writing result of MCI. MCI: mild cognitive impairment; NC: normal cognitive.
Fingertip interaction digital biomarker screening based on semistructured interviews
To enhance the scientific and clinical applicability of our new early warning method, we further used semistructured interviews to select digital biomarkers that are more credible, more consistent with commonly used clinical MCI due to AD screening, and easier to quantify digitally.
First, we developed interview profiles with different focuses for the two groups of interviewees based on previous literature reviews and the summary of the previous study.27,44,54–59 Interview Group A included 20 neuroscience experts with extensive experience in the assessment and diagnosis of cognitive impairment. Interview Group B included 20 information experts in the field of digital medicine. Then, we provided the interview outlines to interviewees 3 days before the formal interview, so that they could prepare in advance and thus improve the effectiveness and quality of the interview. In addition, we informed the interviewer of the interview process and explained the use of the information obtained before the interview was formally conducted, so that interviewees would have no worries. Tables 4 and 5 show the details of the interview outlines.
Interview outlines for clinical medicine specialists.

AD: Alzheimer's disease; MCI: mild cognitive impairment; NC: normal cognitive.
Interview outline for computer science experts.

AD: Alzheimer's disease; MCI: mild cognitive impairment; NC: normal cognitive.
Data analysis
All statistical analyses were performed using the general-purpose data analysis software SPSS 25.0. The homogeneity of variances was checked using Levene's test. Measures conforming to a normal distribution were expressed as `x ± s using independent t-test samples. While skewed distributions were expressed as M (interquartile range (IQR)) using the Mann–Whitney U test. The χ² test was used for the count data. Receiver operating characteristic (ROC) curves were generated and the areas under the curve (AUC) were compared for the performance of single fingertip interaction digital biomarkers in detection of MCI due to AD. For the joint analysis of multiple digital biomarkers, a binary logistic regression model was used for multivariate analysis. p values < 0.05 were considered statistically significant.
Results
We included a total of 60 participants aged 55–80, of whom 30 were NC elderly and 30 were MCI due to AD patients. They were divided into the NC group and the MCI group. First, we performed a differential analysis of baseline information between the two groups, and there were no significant differences in age, sex, and years of education between the two groups (p > 0.05), as shown in Figure 5(a) and (b). Detailed results are presented in Table 6. We organized senior physicians to score the participants on the MMSE neuropsychological scale (one of the commonly used clinical diagnostic tools for AD) at the time participants enrolled (MMSE score ≥ 27 considered NC function). We analyzed the differences between the two groups in the diagnostic results of the MMSE neuropsychological scale. Results showed that the MMSE score of the NC group was higher than that of the MCI group (p < 0.05), and there was a significant difference between the two groups, as shown in Figure 5(c).

Data distribution of (a) age of the NC group and the MCI group, (b) years of education of the NC group and the MCI group, and (c) MMSE score of the NC group and the MCI group. MCI: mild cognitive impairment; MMSE: minimum mental state examination; NC: normal cognitive.
Comparative results of demographic and clinical characteristics of the NC and MCI groups.
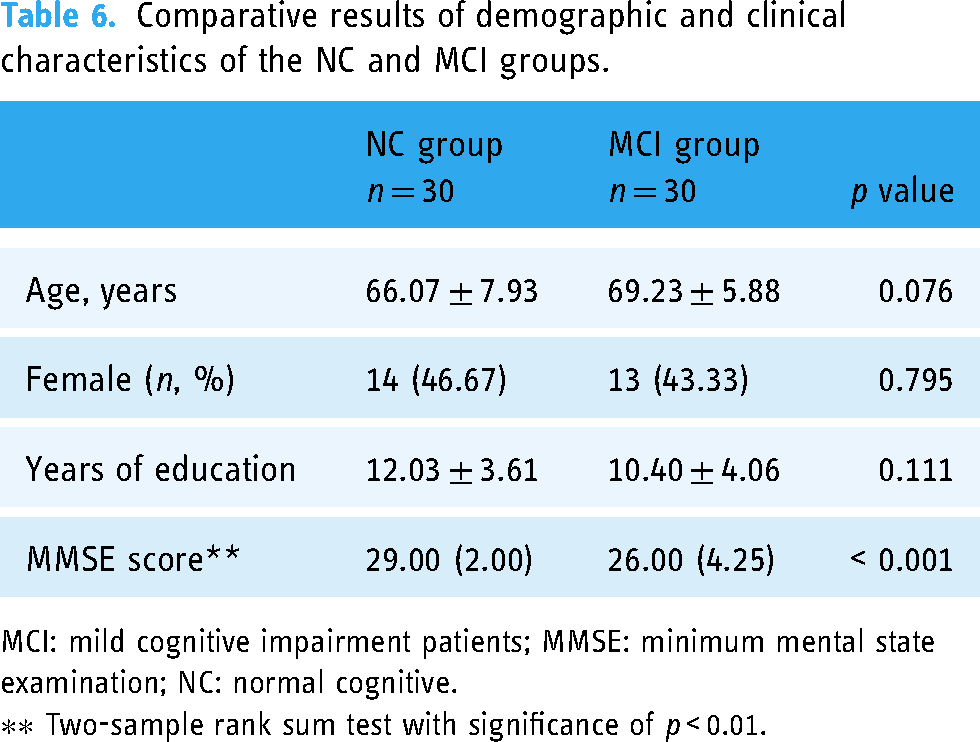
MCI: mild cognitive impairment patients; MMSE: minimum mental state examination; NC: normal cognitive.
∗∗ Two-sample rank sum test with significance of p < 0.01.
Second, we compared all digital biomarkers involved in completing the fingertip interaction clock drawing paradigm and the fingertip interaction repetitive writing paradigm between two groups. We found that a total of 19 digital biomarkers were different between the NC and MCI groups (p < 0.05). In the fingertip interaction clock drawing paradigm, T clock,

Digital biomarkers with intergroup variability p < 0.01 between the NC and MCI groups. ** indicates significant difference between the two groups, at p < 0.01. MCI: mild cognitive impairment; NC: normal cognitive;
Results of the test of variability between the NC and MCI groups for all fingertip interaction digital biomarkers.
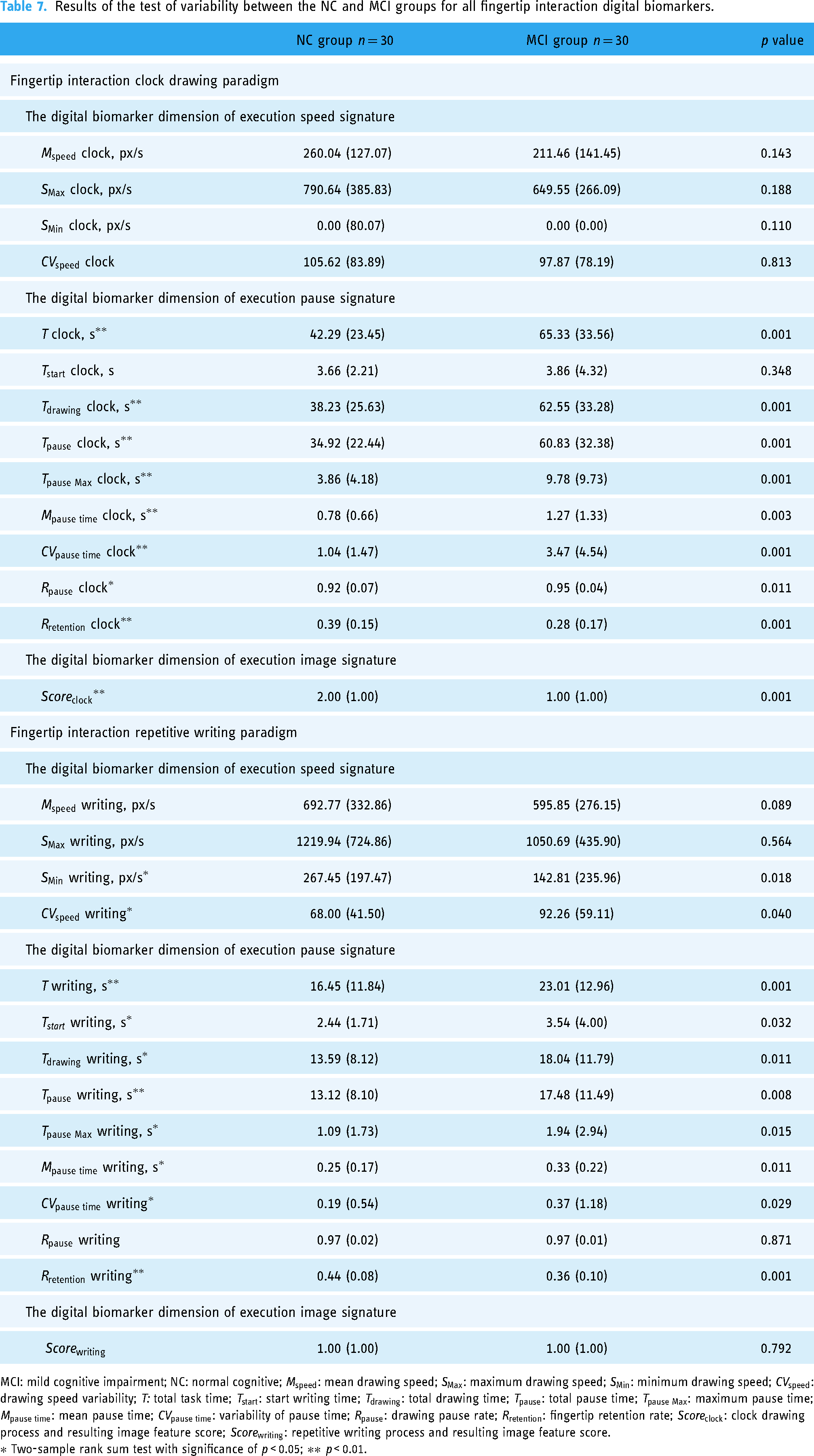
MCI: mild cognitive impairment; NC: normal cognitive;
∗ Two-sample rank sum test with significance of p < 0.05; ∗∗ p < 0.01.
Fingertip interaction digital biomarker screening results based on semistructured interviews
We conducted semistructured interviews with 20 clinical medicine experts and 20 computer science experts, and the results were as follows:
Conclusion 1. 75% of clinical medicine experts believe that the “fingertip interaction” model is more suitable for MCI due to AD early warning screening of the elderly population in clinical, home, and community settings; and all clinical medical and computer science experts from their professional fields affirmed the scientific, rational, and universal applicability of our new MCI due to AD early warning method;
Conclusion 2. In interview Group A, 60% of clinical medicine experts believed that the digital biomarkers extracted in this study were indicative of SEP impairment during interactive tasks in the MCI due to AD population; however, 70% of clinical medicine experts believe that
Conclusion 3. In interview Group B, 90% of computer science experts affirmed the ability of this new early warning method to dynamically capture the entire process of multidimensional fingertip interaction digital biomarkers; 80% of computer science experts believe that T clock,
Based on the results of the above semistructured interviews, we mapped the recommendation index radar of clinical medicine experts and computer science experts for 19 digital biomarkers with intergroup variability in the above two paradigms (see Figure 7).

Fingertip interactive digital biomarkers selection results.
Based on the above results, we downscaled the original digital biomarkers and screened six digital biomarkers. They may reflect MCI due to AD patients’ SEP barriers and are also commonly used for clinical screening and diagnosis of MCI due to AD. At the same time, these digital biomarkers have good performance in objective quantification and calculation. These digital biomarkers include
We then draw the combined ROC curve of MCI due to AD of these six preferred digital biomarkers and the AUC reached 0.880. Its early warning effectiveness exceeded that of the MMSE, a neuropsychological scale judged by clinicians (AUC = 0.856). The results demonstrate the clinical validity of this new early warning method for MCI due to AD based on dynamic evaluation of SEP (see Figure 8).

Receiver operating characteristic curves and the areas under the curve for MCI alerted by MMSE and six fingertip interaction digital biomarkers.
Exploring the cowarning efficacy of multidimensional fingertip interaction digital biomarkers analysis results
In addition to the early warning effectiveness analysis of the above six digital biomarkers, we also made an exploratory analysis of other digital biomarkers that were well evaluated by experts, although they did not show significant differences between NC and MCI groups (p > 0.05). The reason why there is no significant difference between groups may be due to insufficient sample size. We analyzed the dimensions of all digital biomarkers with intergroup differences. In the fingertip interaction clock drawing paradigm, they are aggregated in execution pause signature and execution image signature; in fingertip interaction repetitive writing paradigm, they are aggregated in execution speed signature and execution pause signature (see Figure 9).
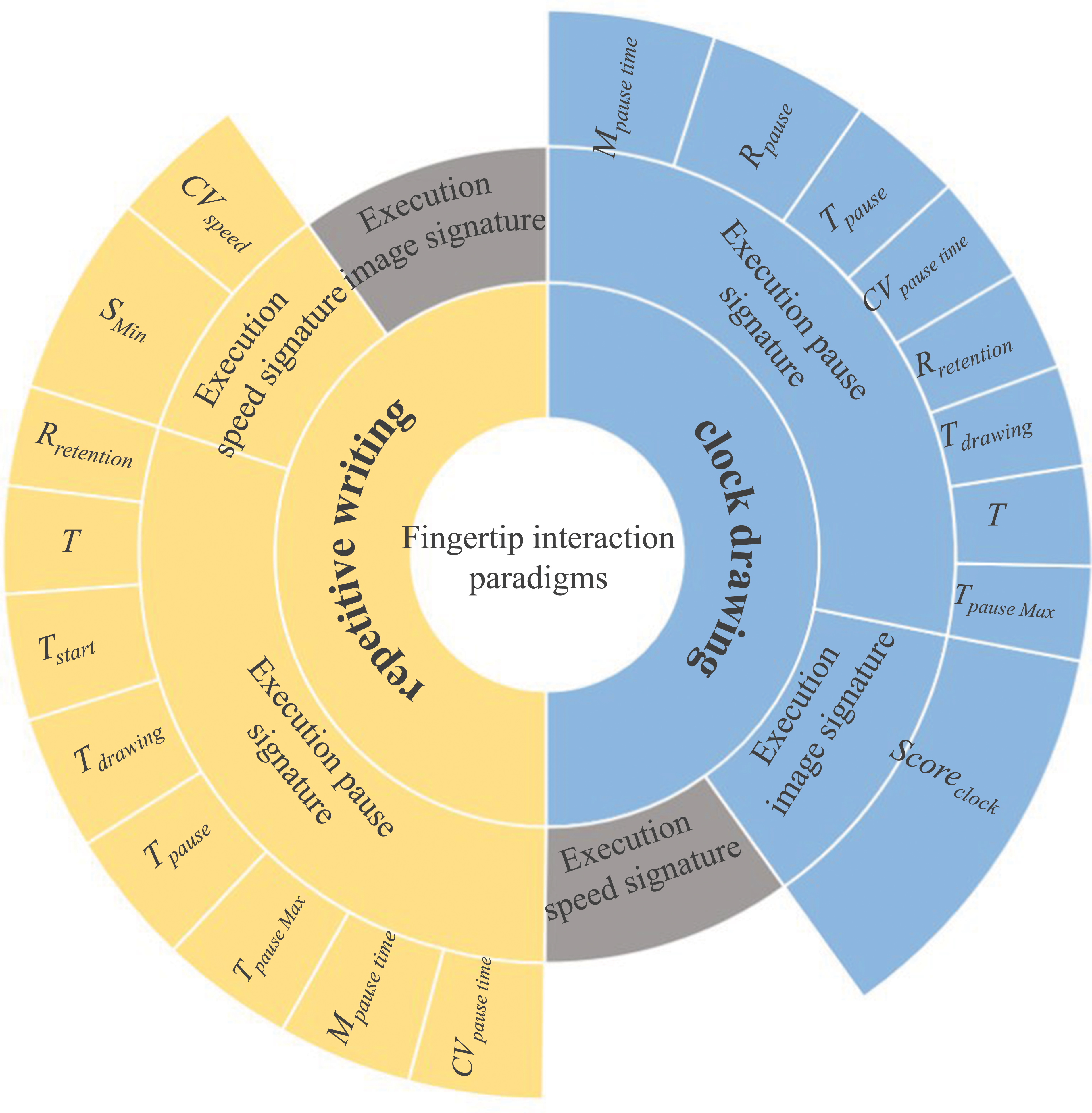
Dimension distribution of biomarkers with intergroup differences.
We included digital biomarkers that have not yet shown intergroup differences and explored the cowarning efficacy of multidimensional fingertip interaction digital biomarkers incorporating in execution pause, speed, and image signature digital biomarkers. Based on six previously screened digital biomarkers, we added an execution speed digital biomarker in fingertip interaction clock drawing paradigm (

The combined receiver operating characteristic curve and the area under the curve after adding two exploratory markers.
Discussion
Using the new early warning method for MCI due to AD based on dynamic evaluation of SEP, we extracted six digital biomarkers indicating spatial executive dysfunction in MCI due to AD patients. And the new method has an early warning performance of 0.880 for MCI due to AD patients.
First, compared to our previous 2.5-Minute Human-computer Interactive Rapid Digital Early Warning Technology, 34 we used fingertip interaction mode instead of eye tracking devices and gamepads. The use of fingertip interaction can minimize individual differences in familiarity with digital writing tools and pencil grip and avoid “writing anomalies” when participants change their usual writing style due to the writing tool. It not only reduces the cost of screening equipment and improves the mobility of the screening system but also improves the warning effectiveness of the screening method (the early warning effectiveness of eye-tracking device-based 2.5-min rapid digital early warning technology for MCI due to AD patients being 0.824). In addition to this, compared to our previous 2-min mobile screening method also based on fingertip interaction, 50 our new method takes into account differences in learning ability and acceptance of smart devices and digital assessment paradigms across older individuals. We chose the handwriting task paradigms of “drawing clocks” and “repetitive writing,” which are more commonly used in clinical settings and are more familiar to older adults, to minimize variability in individual familiarity with the paradigms and to reflect the interactive task performance characteristics of the subjects more objectively. Through the clinical research, our new method (AUC = 0.880) was found to be more sensitive than our previous 2-min mobile fingertip interaction-based screening method (AUC = 0.830). The above results suggested that this fingertip interactive handwriting assessment method based on “drawing clock” and “repetitive writing” is more suitable for large-scale initial screening of MCI due to AD in developing countries with uneven education and lack of medical resources due to uneven economic development, as well as for cognitive function assessment in home and community settings without physicians.
Second, according to the theory of neuropsychology, we interpreted the early warning mechanism of the new early warning method of screening MCI due to AD based on the dynamic evaluation of SEP at the medical level. Because the level of writing difficulties in patients with MCI due to AD is closely related to the severity of the disease and the level of concomitant cognitive impairment, indicators related to the handwriting of writing results and the process of performing interactive tasks in patients with MCI due to AD may reveal deficits in their ability to perform the process. The handwritten evaluation process is essentially a dynamic evaluation process based on a time series. And participants’ multidimensional characteristics such as touch-sensitive pressure, writing speed and acceleration, writing pause duration, and hand movements while performing interactive tasks can be used as MCI due to AD discriminators. Therefore, the fingertip interaction clock drawing paradigm and the fingertip interaction repetitive writing paradigm we designed could show participants’ SEP impairment in spatial interactive tasks in dynamic time series, which may reflect cognitive dysfunction in MCI due to AD.
Third, we explored the model of community-based intelligent primary screening for MCI due to AD in non-physical conditions. This new community-based early warning method for MCI due to AD could be used to achieve intelligent assessment across regions in developing countries where physicians are scarce and medical resources are unevenly distributed, using technologies such as the Internet and the Internet of Things. And it could also be repeated multiple times at different times and locations in various everyday life settings, such as home and community.
Finally, we explored the limitations of the study. Our relatively small sample size may result in insufficient test efficacy, and the actual warning efficacy of some digital biomarkers may not be demonstrated. In addition, the subjects of this study only include Chinese, so the features of “repetitive writing” may only be valid for individuals using Chinese characters. Furthermore, due to study conditions, we conducted only a cross-sectional study, not a longitudinal study, and only a comparative study with MMSE scores in the clinical applicability, lacking a comparison with more diagnostic imaging data. In the future, we will conduct longitudinal studies and explore the “repetitive writing” characteristics of individuals using different characters. And we will continue to test the clinical applicability and incorporate other clinical diagnostic data and further optimize the early warning system and evaluation paradigm based on large sample size data.
Conclusions
We believe that MCI due to AD patients has a SEP impairment during the execution of spatial interaction tasks. Therefore, we have developed a novel and innovative MCI due to AD screening method that can objectively and dynamically evaluate the whole process of SEP disorders in a nonphysician environment. Two digital evaluation paradigms of fingertip interaction, the fingertip interaction clock drawing paradigm and the fingertip interaction repetitive writing paradigm, were also designed. The method can intelligently extract and analyze the multidimensional digital biomarkers of fingertip interaction during the execution of the above two digital evaluation paradigms of fingertip interaction and realize effective early warning of MCI due to AD population by evaluating subjects’ ability to dynamically perform the whole process. After clinical research validation, our novel early warning method based on dynamic evaluation of SEP has a good warning performance for MCI due to AD (AUC = 0.880). And the new early warning method for MCI due to AD based on dynamic evaluation of SEP has the advantages of simple operation, high degree of aging suitability, high degree of intelligence, and high early warning effectiveness and will provide a reliable tool for early mass screening and warning of AD in a home environment without a doctor in developing countries with large populations, high demand for disease screening, uneven economic development, and varying levels of education.
Footnotes
Acknowledgments
The authors would like to thank all participants for enrollment in this study.
Contributorship
KL and RX: conceptualization and methodology. JX and SL: software. XM, TC, AO, BW, and YW: validation and formal analysis. SZ, YW, SH, ZC, and JL: investigation. KL, TC, and RX: resources; XM, YW, ZC, and CW: data curation. KL, XM, JX, and CW: writing—original draft preparation; KL RX, and TC: writing—review and editing; XM and CW: visualization; RX: supervision; KL: project administration and funding acquisition. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The experimental protocol was designed in accordance with the ethical guidelines of the Helsinki Declaration. Ethical permissions were granted by the Human Ethics Committee of the Zhejiang Chinese Medical University (Approval Number: 20210806-1). Written informed consents were obtained from patients or their guardians.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Province Key Research and Development Program of Zhejiang (grant numbers 2021C03116 and 2022C03064), and scientific research project of Zhejiang Chinese Medical University (grant number 2021JKZDZC04).
Guarantor
KL.