
Abstract
Objective
Digital health has been gaining widespread attention but has not been fully integrated into the existing healthcare system. However, it remains unclear whether the new digital health solutions align with users’ needs and wants. This study examines how citizens perceive the functionalities of digital health and how different health risks influence their perception.
Methods
Using an online survey, data are collected from over 4000 Danish citizens. The data are analysed using linear regression models.
Results
The results show how users’ perceptions of digital health differ significantly. Users are highly interested in data sharing across different healthcare stakeholders but less interested in online health communities. The results also show that the support for digital health is correlated with various health risks, including age, smoking and social network. However, health risks do not have uniform relationship with the perceived value of digital health.
Conclusions
While developing and implementing new digital health solutions, it is important to consider the perceptions of people who are expected to benefit from such solutions. This study contributes to the literature by deepening the knowledge of how citizens with different risk profiles perceive the multitude of digital health tools being introduced in the healthcare sector.
Introduction
In recent decades, healthcare organisations have become increasingly interested in digital health as a digitalised infrastructure that creates, delivers and captures value in the healthcare sector. Digital health covers a diverse set of solutions ranging from telemedicine to online communities 1 and is fast gaining prominence. For instance, citizens these days use digital self-monitoring tools to manage their health conditions and patient portals to communicate with healthcare personnel online.1,2 This explosive development is driven by the challenges the healthcare sector faces, which call for new solutions or approaches, and the opportunities new technologies offer. 3
Despite the popularity of digitalisation, the healthcare sector remains largely analogue, comprising brick-and-mortar organisations and face-to-face interactions between citizens and clinicians. 4 Several financial, organisational and regulatory barriers make developing, testing and augmenting digital health challenging. One example is the ‘plague’ of trials and pilot project, wherein digital solutions are introduced, but few are integrated in day-to-day activities and mainstreamed across healthcare organisations.5,6 Moreover, discussions on new digital health solutions have predominantly focused on the technology and the healthcare professionals involved in these innovations, whereas there has been comparatively less emphasis on the perspectives of citizens who will often be the end users of these solutions.7–9
This study examines how citizens perceive the functionalities of new digital health solutions. It focuses on modern information and communications technology solutions related to citizens’ interactions with the healthcare sector. Digital health solutions that improve healthcare organisations’ internal operations (such as logistics systems and data banks) do not fall within the scope of this study. New consumer-oriented digital health solutions can change citizens’ relationship with the healthcare sector. However, this is possible only if they perceive such solutions favourably. Failure to adapt digital healthcare (such as telemedicine, health apps and online health communities) to citizens’ needs and wants will create a gap between the supply and demand of these solutions. Knowledge of citizens’ perception of digital health functionalities can help improve existing healthcare offerings, inspire innovation and generate market intelligence.10–12
This study also examines the relationship between citizens’ health risks and the support for digital health. More knowledge is needed regarding the relationship between the perceived value of digital health and a broad set of health risks. While the health risks of citizens are likely to shape the perceptions of digital health, the verdict is still out on the relative importance of the individual risk factors and the direction of the relationship. On the one hand, deteriorating health of high-risk citizens may make them more likely to seek new solutions and make trade-offs (for example, between online health monitoring and the need for privacy), inducing them to accept digital health solutions. On the other hand, high-risk citizens may not always have the competencies necessary to reap the benefits of digital health. For example, the most frequent users of healthcare services are elderly citizens with multiple health conditions who generally have less experience with digitalisation than younger citizens, who, in contrast, have less interaction with the healthcare sector. 2 This study provides new insights into the relationship between the perceived value of digital health and the underlying health risks of citizens. Previous research has examined how various factors influence citizens’ engagement with digital health, 1 but the influence of their health risks remains underexplored.
Empirically, the study is based on survey responses from 4022 Danish citizens. Denmark is a small, modern society which is consistently at the top of international rankings of digitalisation, including the European Digital Economy and Society Index and the UN E-Government Survey.13,14 However, not all citizens benefit from digitalisation. The Danish Agency for Digital Government estimates that approximately one in five citizens are disadvantaged and lack the competences to take part in the digital society.15,16 In terms of health, Denmark has a comparatively advanced public healthcare system, which has also been on the forefront when it comes to digital health (e.g. electronic health records). 17 However, Denmark also struggles with a number of structural challenges, including rising costs, lack of personnel, an aging population, and a rapid increase in citizens with chronic conditions. 18 Moreover, Denmark experiences inequality when it comes to the health of citizens and their interaction with the healthcare sector.19,20 Lastly, while digital health comes with many benefits, it is also a barrier for citizens who are not comfortable with digital technologies (booking appointments, accessing health information, etc.).
Digital health from citizens’ perspective
The digital revolution has sparked interest in healthcare solutions linked to Artificial Intelligence (AI), 21 robots, 22 blockchain 23 and telehealth. 24 We use digital health as an umbrella term for a new digitalised infrastructure that creates, delivers and captures value in the healthcare sector. Digital health solutions offer many opportunities to create value for citizens and innovate healthcare systems. For instance, they improve patient safety, enable better access to healthcare services, reduce unnecessary transportation, provide faster care, inspire healthy lifestyles, slow disease progression, provide access to healthcare information and healthcare professionals, reduce admissions/readmissions and improve health outcomes.21,25–27 To give a few examples, is has been suggested that telehealth solutions can detect health deteriorations at an early stage, whereas wearables and apps can inspire citizens to adopt a healthier lifestyle.21,25,26 Moreover, big data solutions and AI have made it easier to make early diagnoses and detect healthcare needs.21,27,28 This plethora of benefits makes it difficult to understand why digital health is not fully integrated into existing healthcare offerings. For instance, the uptake of telehealth has been slow even though the technology has been around for decades.2,19,27 Studies show that the successful adoption (or lack thereof) of a new digital health solution can be influenced by a variety of factors, including the functionalities of the technology, the actors involved in the use, and the organisational and institutional context in which it is introduced.6,29,30 A distinction has been made between practice-related and patient-related determinants of digital health adoption. 2 Practice-related determinants concern the healthcare providers and the professional users of digital health (e.g. physicians and nurses), and cover for instance reimbursement, quality issues, and digital competences. 2 Patient-related determinants cover the individuals with diseases and include issues like access to technology, digital literacy, personal lifestyle, and motivation.1,2,29
This study focuses on the value citizens in general ascribe to new digital health offerings. Citizens serve as customers and co-producers of digital health when they, for instance, use new technology to manage their health, interact with healthcare personnel and share information about their conditions. In some cases, citizens use their competencies and resources to provide health services and develop new innovations. 31 For instance, online health communities have emerged which bring citizens with similar diagnoses together for sharing information, providing peer feedback, and collaborating with partners on better solutions. 32 However, digital health solutions are sometimes introduced without heeding to citizens’ voices and complex needs. This happens when greater emphasis is placed on ‘technology push’ rather than ‘demand pull’. 6 The prioritisation of technology comes with risks since organisational assumptions about user value may be biased.
The value of digital health can be perceived in multiple ways by the citizens, who have different needs and hold different ideas about what creates value for them.33,34 This study draws attention to health risks as salient factors in understanding citizens’ perceptions of digital health. Some health risks are behavioural (smoking, drinking, physical activity), whereas others are linked to demographics (such as age and sex), physiology (such as hypertension and cholesterol), biology/genetics, and the environment. 24 Either way, health risks possibly influence the perceived value of different digital health solutions, albeit not always in the direction one would normally expect. On the one hand, it is reasonable to expect high-risk citizens to value digital health solutions that enable them to manage their own conditions and improve their interactions with healthcare professionals. However, citizens’ digital competences may not be aligned with their health risks. In fact, digital health may deepen the digital divide between citizens with digital competences and those without them. 10 Evidence indicates that health risks linked to age, income, education, and health conditions influence the use of digital health solutions. 2
The digital divide may result in the paradox that high-risk citizens who could potentially benefit the most from digital health are also the ones who are least likely to make use of them. According to OECD: ‘The challenge is that the patients that most stand to benefit from digital technologies like telemedicine are also those who are most likely to face difficulties in accessing and using it’. 19(p32) The phenomenon has also been labelled the digital inverse care law. 35 For instance, a new telehealth solution may arguably help high-risk elderly citizens with chronic conditions to live a more independent and meaningful life. However, older, poorer, and less-educated citizens with multiple health conditions are less likely to use digital technologies compared with younger, well-educated citizens with fewer diagnosis. 10 Scholars talk specifically about a ‘grey’ digital divide because elderly citizens are less familiar with the use of digital technologies. 36 In consequence, citizens who value digital health the most may have a different risk profile than citizens, who stand to gain the most benefit from them.
Method and dataset
The researchers designed the survey which was carried out by an external data provider (Norstat). The data provider contacted 9621 participants from a citizen panel by email or a survey app. A total of 4022 citizens fully completed the survey (347 were incomplete) which equal a response rate of 42%. The survey aimed to maximise the responses of those citizens who were interacting with the healthcare sector because this segment is in a better position to assess existing healthcare services and the need for new digital health solutions. The survey revealed that 2643 respondents (65.7%) had one or more diagnoses within the last 12 months. Hypertension was the most common diagnosis (29.3%), followed by osteoarthritis (19.4%) and diabetes (9%). Table 1 presents the characteristics of respondents. The survey was conducted in the local language, and all texts were subsequently translated to English. The survey was part of a large, externally funded research consortium aimed at promoting a more patient-centric and digitally driven healthcare sector.
Respondents’ characteristics.

Measurement of variables
The respondents were asked several questions regarding socioeconomic factors (housing, education), health conditions (diagnoses, well-being), use of healthcare services (general practitioners, hospitals) and the perceived value of digital health.
Measuring digital health from a citizen perspective is not easy. Generally, citizens do not have experience with different health solutions; thus, they cannot compare alternatives.
37
Moreover, they are unlikely to be aware of, and have access to, a number of technologies which support the healthcare infrastructure, for example, health management information systems and logistics management information systems.
38
Instead, we focused our research on the functionalities of digital health rather than on specific technologies (such as 3D printing, wearable devices, AI and genetic testing technologies). We emphasised solutions directly influencing citizens’ interactions with the healthcare sector. An inspiration for the categories was existing information about digital health initiatives in Denmark.
39
The focus was on the interface between the citizens and the healthcare sector rather than functionalities intended to benefit actors within the healthcare sector.
39
More specifically, citizens were asked to indicate whether better digital opportunities were needed for the following functions (1 = Completely agree and 5 = Completely disagree).
Gather all health data in one place (such as doctors, municipalities, hospitals and pharmacies). Get a second opinion on test results, diagnoses and treatment. Get private alternatives if the waiting time is long. Share health data with others (relatives or insurance companies). Get virtual consultations, follow-up meetings and test results. Book and cancel appointments for consultations and examinations. Monitor health (e.g. pulse and blood pressure) and share results with health personnel. Start treatment (e.g. take medicine) after consulting with health personnel online. Share private health data (e.g. from mobile phone) with health personnel. Participate in online groups where members have the same diagnosis. Follow progress of one's examination and treatment process. Get online training and education tailored to one's health condition.
There are numerous potential health risks and a single survey cannot contain all of them. An individual's long-term health can be linked to genetics, lifestyle (e.g. smoking and drinking) and various contextual factors, including education, occupation and housing.40,41 In our survey, we limit the risk factors to those that affect citizens’ health according to the literature (e.g. smoking, alcohol, obesity).40–43 It is noteworthy that these risk factors may be interrelated. For instance, education level may be related to physical activity, whereas age may be linked to smoking habits.
44
Table 2 summarises the health risks included in the survey where respondents were asked to assess their perceived health.
Health Risk Categories.

We derived the number of Conditions from a list of 19 common diagnoses and ‘other’ (followed by an open-ended question on what the diagnosis was). Then, we summed up the diagnoses for each citizen. Only five citizens had more than nine diagnoses. The number of Channels was derived from a list of 14 different healthcare services and ranked from ‘no contact’ to ‘more than 50 contacts annually’. We only considered the number of different healthcare channels used, not the frequency of their use. Citizens with contacts to multiple healthcare services (e.g. patients with polychronic diseases) were expected to face more coordination challenges across functional, professional, and organisational boundaries.
All independent variables were standardised because interaction terms were also included. The dependent variables were not standardised, so the constant represented an average interest in a particular functionality. Using IBM SPSS 27, we conducted linear regressions to analyse the impact of risk factors on the 12 digital solutions (see Table 3). Variance inflation factor (VIF) was used to assess collinearity.
Regression coefficients.
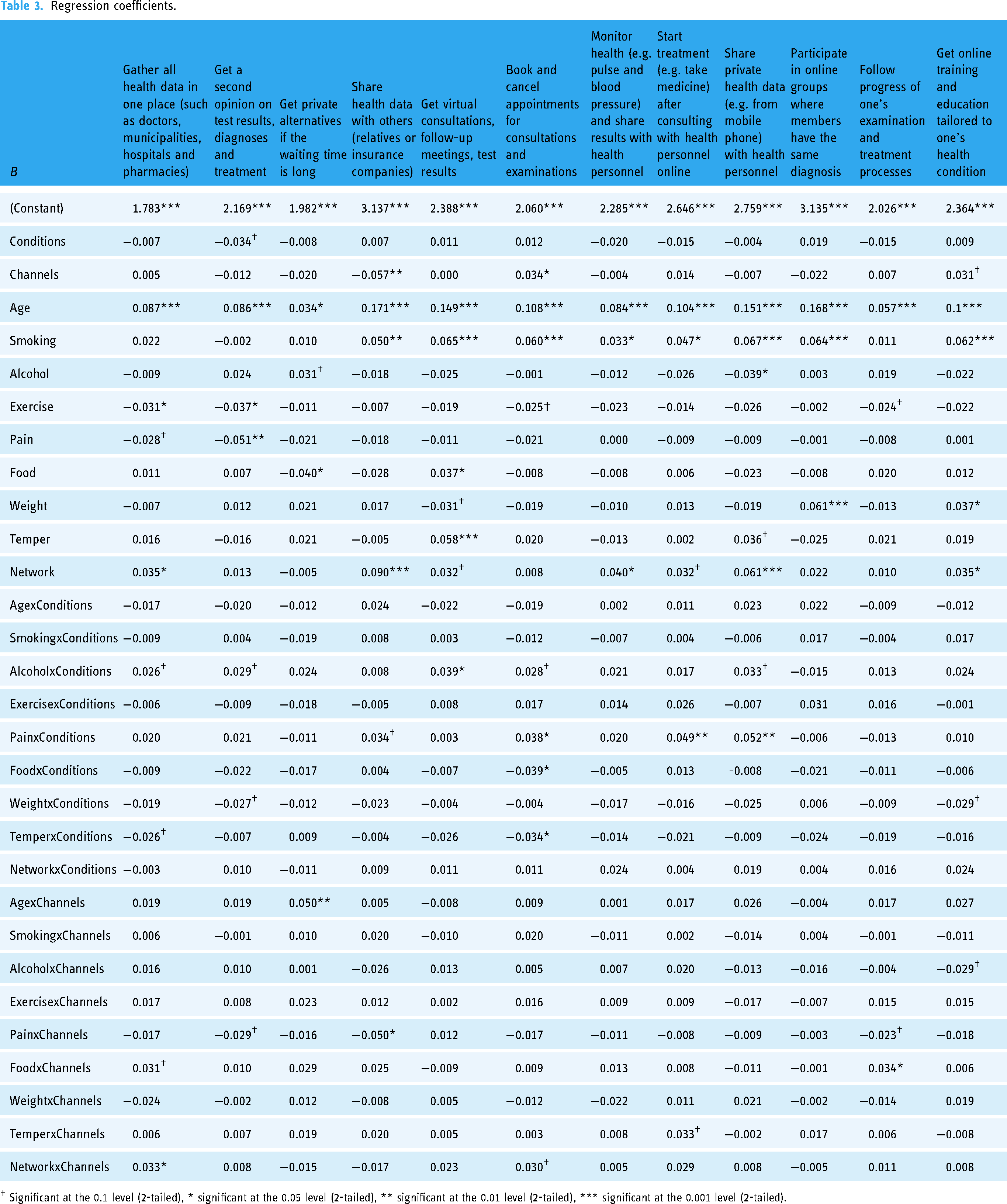
† Significant at the 0.1 level (2-tailed), * significant at the 0.05 level (2-tailed), ** significant at the 0.01 level (2-tailed), *** significant at the 0.001 level (2-tailed).
Results
Figure 1 shows how citizens view digitalisation in the healthcare sector. Evidently, citizens are concerned about data silos in the healthcare sector, and health data are not shared among healthcare professionals across different units. They have few concerns about sharing data with health professionals but are less supportive of external actors accessing their health data. This perception resonates with concerns raised in the literature; health data can enable better diagnoses and treatment but insurance companies and employers can misuse it to discriminate against specific citizens. 25 Furthermore, the citizens are in support of better tools for choosing private healthcare providers. In certain cases, Danish patients have the right to choose private alternatives if the waiting time for examination and treatment in the public healthcare system exceeds nationally defined limits. Citizens also call for better tools to manage the logistics of their interaction with the healthcare sector, for example, making appointments and following the progress of tests and treatment. Finally, citizens do not consider online patient groups a high priority, raising concern over the potential of such communities.25,32,49

How citizens view digitalisation in healthcare.
Table 3 presents the regression coefficients of the relationship between risk factors, including their interaction with the number of conditions and the number of health channels, and the support for digital health. To present all 12 regression models side by side, we only state the regression coefficients, and significance is denoted using asterisks. Results are presented at a significance level of 0.05. All VIFs were less than two, while the upper threshold provided in the literature ranges from 3 to 10. Thus, collinearity was not an issue in any of the models. The impact of the independent variables will be interpreted in relation to the support of digital health, that is, opposite to the sign of the regression coefficient. The results indicate that several digital health solutions are sensitive to the risk profiles of citizens.
Age (as a direct effect) is consistently and negatively correlated with interest in digital health since all 12 coefficients are significant at the 0.05 level. This result is not surprising; elderly citizens generally have low digital competency, which may translate into limited support for digital health solutions. It supports those findings that indicate an age-based digital divide between generations when it comes to digital health. 35 Smoking (as a direct effect) was negatively correlated with 8 out of 12 digital health solutions, suggesting that smokers are less likely to value the benefits of digital health solutions. This result is surprising because smokers are expected to have poor health, which would increase the likelihood of them using healthcare services. A possible explanation is that stigmatisation affect smokers’ perception of the interaction with healthcare professionals. Where health authorities attempt to de-stigmatise other types of drug use to facilitate early contact to healthcare, anti-tobacco campaigns and policies actively try to denormalise and stigmatise smoking. 50 Citizens’ social network (as a direct effect) is positively correlated with the support for 5 out of 12 digital health solutions. We coded a large social network as 1 and no social network as 4. Therefore, citizens with a large social network had a lower interest in digital health. This may be because they have sufficient social support to cope with their conditions. In contrast, citizens without much social network will be more dependent on the services of healthcare workers or digital health solutions. Another possible explanation is that social support boosts neurotransmitter (such as serotonin and dopamine) levels, making citizens more confident in their health and the existing healthcare services. A final explanation is that a strong social network induces a cushion effect, making citizens with stable and safe relationships more willing to take risks. 51 Interaction terms were included to check for a moderating effect of the number of conditions and the number of healthcare channels in the relationship between risk factors and digital health solution. However, the coefficients of most interaction terms were not significant, even at the 0.1 significance level.
Discussion
Digital health shapes interactions between healthcare professionals and citizens. However, the value of digital health solutions ultimately depends on how the users perceive them. Our findings demonstrate that citizens perceive the value of digital health solutions differently. Solutions that improve data sharing and logistics and provide access to private alternatives receive high support, whereas interest is low for those that involve non-healthcare stakeholders (e.g. employers, insurance companies and patient organisations). These results suggest that new digital health technologies should focus on improving data sharing, patient flow and process times (of tracing, tracking, measurement, etc.) within the existing healthcare system. The results resonate with the idea that citizens have relatively simple healthcare needs: efficiency, access, integration and availability. 52 The support for better orchestration of healthcare activities also echoes previous findings, which indicated room for improvements in organisational collaboration in the healthcare sector. 53
Regarding the relationship between citizens’ health risks and the perceived value of digital health solutions, the health risks were expected to exclude some citizens from accessing healthcare services. Digital health can be a double-edged sword which can remove barriers for healthcare provision as well as contributing to the digital divide. 2 Our findings indicate that digital health solutions are not always aligned with users’ interests. Some citizens have health risks which make them reluctant to use digital health solutions. For instance, age was found to be consistently, negatively correlated with digital health solutions, even though the elderly use healthcare services the most. Such findings confirm those of other studies on telehealth adoption.2,54 Clearly, there is opportunities for developing digital health solutions which are better adapted to the needs and wants of elderly people, who take up a significant proportion of capacity and costs in the healthcare sector. Moreover, blended health solutions combining digital technologies with consultation from healthcare professionals could potentially increase the adoption among this group of citizens.
Social network is another factor which seems to shape citizen perceptions of digital health. The findings tap into the discussion of whether digital health can help reducing social isolation among especially elderly citizens. 55 In this study, citizens with limited social network seem to have more positive perceptions of digital health compared to citizens with sufficient support from family and friends. The findings may call for more segmentation of digital health technologies depending on the needs and wants of the citizen population. Well-designed digital health solutions may therefore hold potentials beyond the technical functionalities by improving the social wellbeing of citizens with limited social support. This is not a trivial benefit, as social isolation among especially older adults are expected to grow significantly in the future. 55
Another revelation is that that citizens’ health risks do not have a uniform relationship with the perceived value of digital health. The heterogeneity of health risks and digital health solutions makes the relationship between the variables complex. Categorising citizens based on generic health risks has limitations in explaining their needs and wants. Age, smoking and social network seem to be health risks which more generally call for attention when developing digital health solutions. However, other health risks may be important to take into account when it comes to specific technologies (e.g. virtual consultations). Knowledge of health risks can facilitate the design of better digital health solutions, which are aligned with the needs and wants of the citizens who are supposed to benefit from them. Regarding the functionalities of digital health, different modes of data sharing seem to be most closely linked to health risks. The findings provide inspiration for the future development of digital health solutions, which emphasise innovations overcoming data silos and improving the logistics of healthcare provision. New digital health tools can potentially be important boundary objects which help permeating existing healthcare silos between, for example, professions, functions and organisations.
Overall, the findings highlight the need to include citizens’ perception in discussions on digital health. All attempts to introduce patient-centric approaches (‘What matters to you?’ and not only ‘What is the matter?’) in discussions of healthcare transformation presuppose an interest in citizen values and preferences, something the technology push approach often suppresses.3,56 A citizen-oriented approach also aligns with the World Health Organization, which suggests that people should be: ‘(…) at the centre of digital health through the appropriate health data ownership, adoption and use of digital health technologies and development of appropriate literacy’. 57(p27) Digital health solutions promoted by technology providers and healthcare professionals may not always meet the needs and wants of the citizens who are expected to use them. Such solutions will be of little value because users may not adopt them. Deepening the knowledge of the value citizens ascribe to digital health solutions is important for designing solutions that can gain traction and be successfully implemented in the healthcare sector.
In the future, it will be relevant to examine the dynamic relationship between individual, organisational and institutional factors that shape the perceptions of digital health solutions. Poor uptake of digital technologies can be the result of poorly designed solutions for users, inadequate regulation, limited financial incentives and organisational resistance.4,27 Moreover, external environmental events, such as the COVID-19 pandemic, can dramatically influence the adoption of digital health solutions. 2 For instance, in February 2021, the use of virtual care was 38 times higher than its use before the pandemic. 58 In other words, the future of digital health will depend on the complex relationship between citizens, healthcare organisations and the external environment.
Conclusion
Digitalisation is a cornerstone of the healthcare sector's transformation, yet it remains unclear whether the new digital health solutions align with users’ needs and wants. Evidence indicates that solutions improving the flow and efficiency of healthcare interactions are valued, but those expanding the boundaries to non-healthcare parties are not. Our results highlight the need to adapt the development and implementation of new digital health solutions to the needs and wants of target groups. However, our findings also indicate that some digital health solutions gain support across all citizen groups and risk profiles. These include solutions that facilitate better data sharing across different healthcare stakeholders. Overall, this study fills a gap in the literature by exploring how citizens’ perceptions of digital health are shaped by a broad set of health risks.
Limitations
This study is subject to some limitations. First, there is a need to develop better scales to measure digital health from the perspective of different stakeholders. The literature on digital health remains nascent and calls for further conceptual and empirical research. Moreover, there is a lack of consensus on the meaning and measurement of concepts such as health technology and digital transformation. 59 Second, the survey yielded mixed results, which is not surprising, because the 12 digital health solutions vary significantly (ranging from data sharing to online training). However, meaningful progress has been made in developing health technology typologies, which can help create better scales and measures. 60 As for health risks, the inclusion and exclusion of risk factors can be debated. Moreover, some of the questions may be influenced by a social desirability bias (e.g. smoking and alcohol), where some citizens will overreport desirable activities and/or underreport undesirable ones. 61
Third, data were collected from only one country. Therefore, findings from the Danish healthcare sector cannot be directly applied to the healthcare sector in other countries. For instance, there may be limited interest in privacy and data protection only in countries with high levels of trust and healthcare institutionalisation. Moreover, the degree of maturity of digital health may influence users’ perception. The perceptions of citizens belonging to countries with high levels of digitalisation may differ from those of citizens living in countries with less advanced digital infrastructure. The digital divide can also be a significant issue, even in digitalised societies. In Denmark, approximately 20% of the adult population is digitally excluded, and this percentage is higher in specific groups. 15
Footnotes
Acknowledgements
We would like to thank Innovation Fund Denmark for support of the study. We would also like to thank the data provider Norstat for carrying out the data collection.
Contributorship
ERGP designed the survey and prepared the main manuscript. FS conducted the statistical analysis and contributed to the interpretation and writing of the findings. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Innovation Fund Denmark (Danish: Innovationsfonden).
Guarantor
ERGP.