
Abstract
Objective
To evaluate the role of a WeChat-based mobile platform in growth hormone therapy.
Method
Growth hormone therapy and health education information for height growth were embedded in a WeChat-based mobile platform, and the platform was evaluated through medical staff assessments, patient volunteer assessments and quantitative scoring criteria.
Results
In the medical staff evaluation, both clinicians and nurses had a positive attitude towards the mobile platform, believing that the design of the mobile platform was clearly visualized and easy to operate. In family volunteers’ evaluations, the summary of β-testing results showed that 90–100% of parents had a positive attitude towards the WeChat-based mobile platform. Parents of the patients and doctors and nurses assessed the mobile platform by reviewing quantitative scoring standards developed by professional researchers. All scores were >16 (the average score was 18–19.3). Children treated with growth hormone therapy were included for compliance tracking for one year, and patient adherence was described in this study.
Conclusion
The interaction based on the WeChat platform and the health education of the public have greatly increased the interaction between doctors and patients, and improved patient satisfaction and compliance.
Introduction
Mobile health (mHealth) is defined as the use of mobile devices for medical purposes or to support overall health and well-being.1,2 It can be used to perform tasks in areas such as wellness management, behaviour change, health data collection, disease management, self-diagnosis and rehabilitation as well as act as an electronic patient portal and medication reminder.3,4 In addition, a large number of studies support that well-designed mobile medical applications can empower patients, improve medication compliance and reduce medical costs.5,6
In modern society, the ubiquity of mobile phones has become the norm. It is estimated that 97.5% of the population had mobile phones in China in 2017. 7 Due to the large number of devices and easy access, the practicability of mHealth has never been so common. The study found that 31% of mobile phone owners use them to obtain health information. 8 WeChat conforms to the trend of information digitization and integrates various information modes, such as pictures, text, audio, video, etc., that are acceptable to almost all audiences so that users can view information anytime and anywhere. In China, more than 94% of smartphone users are actively using WeChat. 9 A study that collected 1636 WeChat customer questionnaires from 32 provinces pointed out that nearly one-third of users often receive and read health information through WeChat. 10 The role of mHealth in the field of child health care has attracted much attention. The improvement of children's immunization coverage in rural areas of China also benefited from mHealth. 11 Nutrition and diet applications are a hot area for mHealth and offer the possibility of providing behavioural change interventions for healthy eating and weight management in scalable and cost-effective ways. WeChat-based mHealth has contributed to improving the accessibility and intake of fruits and vegetables for young children 12 and increasing exclusive breastfeeding rates to support breastfeeding rates for neonates in intensive care.13–15 In addition, the accuracy of WeChat-based mHealth in collecting infant feeding data information is no less than that obtained by interviewing infant nurturers.16,17 WeChat-based mHealth can also reduce the occurrence of accidental injuries to children by improving parents’ skills, beliefs and behaviours. 18
Developing applications from the perspective of multidisciplinary experts and user-centred design makes it easier to integrate and utilize resources in primary and secondary nursing interventions.19,20 Therefore, we have added information on the health management of short-stature children to the WeChat mobile platform, and established relevant WeChat groups to strengthen doctor–patient interactions to improve compliance with the treatment of short stature. The details are as follows.
Methods
Introduction to relevant operations of the short stature health education mobile platform
The short stature health education mobile platform was developed with the technological support of a specialized information technology company, which was started during the treatment and ended. This platform included the following contents: weekly diet plan, weekly exercise plan, popular science knowledge related to children's health, physician's voice, growth guide and growth story. The first three items were displayed in the ‘message’ and updated once a week. The last three items were displayed in the drop-down list of ‘service’ for navigation within the platform, as shown in Figure 1(a). Physician's voice included three indices: expert lectures, online studies and bone age atlas; the growth guide included four indices, including parent class, growth encyclopaedia, 31 kinds of nutrition and growth assessment; and the growth story included three indices: summer/winter camp, growth club and growth sharing. Each index could be expanded with rich content, encouraging users to further browse related health education content to meet more needs, as shown in Figure 1(b). Each module displayed media elements in various forms, including text, pictures and videos.
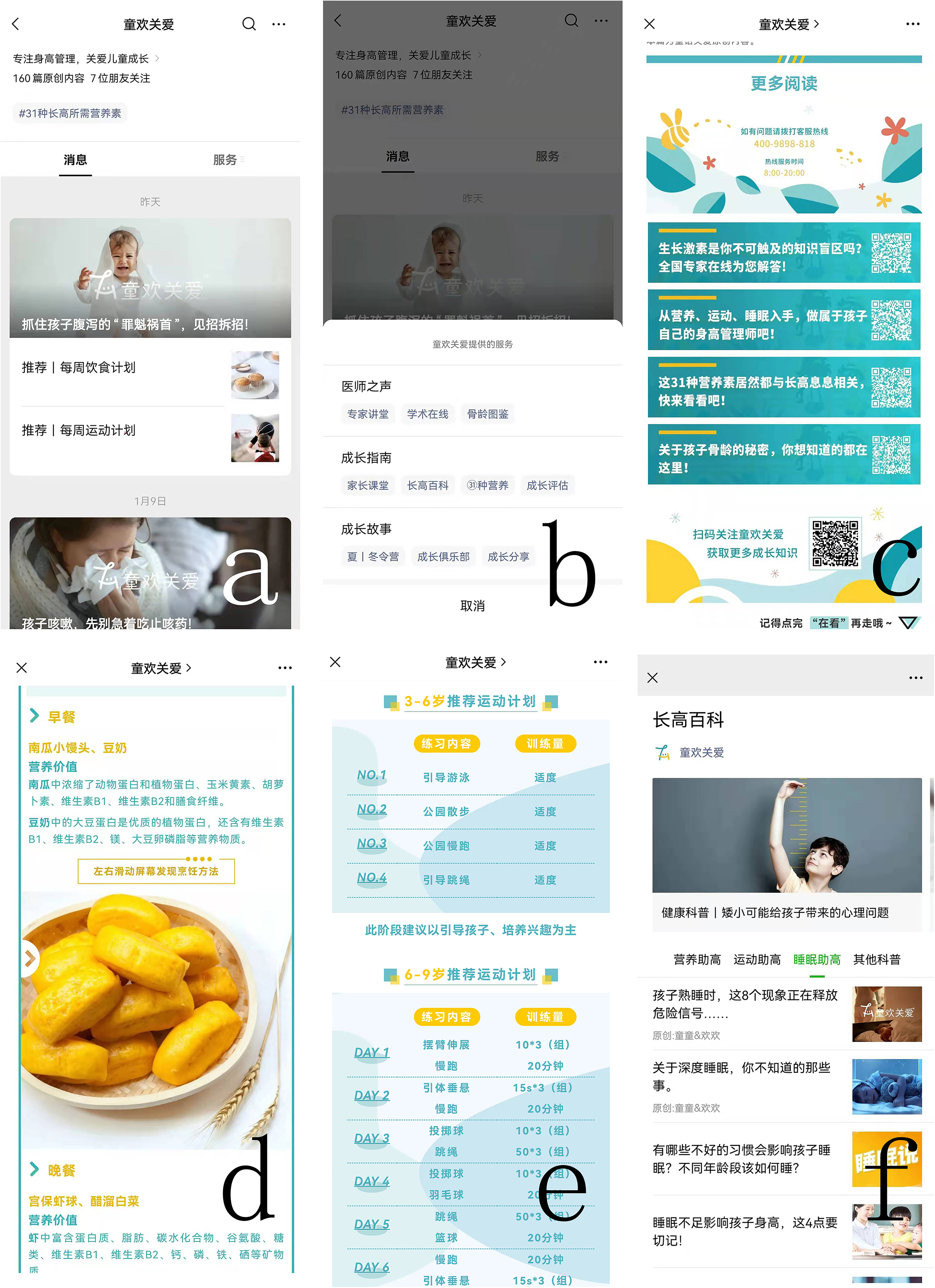
Short stature health education mobile platform (originally in Chinese). (a) The home page of the platform, showing ‘message’ and ‘service’; (b) the three major blocks of content included in the ‘service’, including physician's voice, growth guide, growth story. (c) a quick access QR code for growth related problems in the ‘service’; (d) the diet recommendations for each day of the week; (e) detailed exercise plans for children of different ages; (f) topics of ‘sleep helping height’.
When words and pictures are presented together, it is easier for learners to form a mental model of language and images and to establish a connection between the two, which is better than the presentation of words alone. 21 Therefore, the content in both ‘message’ and ‘service’ was displayed in videos or documents combining text and pictures. At the end of each article in the ‘message’, there was a quick access QR code for growth related problems in the ‘service’, which was convenient for parents to identify and consult, as shown in Figure 1(c).
In the ‘weekly diet plan’, the diet recommendations for each day of the week were listed, and the nutritional value of each recommended ingredient was explained, as shown in Figure 1(d). Proper nutrition is necessary for the healthy growth of children and adolescents. 22 Through the introduction of the nutritional value of ingredients, parents can strengthen their understanding of the nutrients needed by children and the differences in nutrients provided by different foods, which will help parents provide children and adolescents with a balanced diet. In addition, in the weekly diet plan, readers can also view the cooking methods of recommended ingredients.
In addition to a reasonable diet, proper physical exercise, muscle exercise, fresh air and personal body care are all conducive to the healthy growth of children and adolescents. 23 In the ‘weekly exercise plan’, detailed exercise plans for children of different ages were recommended, as well as different amounts of exercise for different intensities, as shown in Figure 1(e), which helps parents quickly grasp the daily needs of their children.
Although there is still some controversy about the correlation between sleep and height, the association between shorter sleep duration and the risk of overweight and obesity has been fully confirmed. 24 Developing good sleep habits among short stature children was encouraged. In the ‘Growth encyclopaedia’, the topic of ‘sleep to help’ for children's sleep was included to solve the various problems parents had regarding children's sleep, as shown in Figure 1(f).
Among children receiving growth hormone therapy, a nurse or doctor's assistant established a ‘diet check-in group’, and monthly material rewards were given to children and families who had a balanced diet every day, as shown in Figure 2(a) and (b).

WeChat interaction between medical staff and their families. (a and b) the ‘diet check-in group’ in WeChat groups; (c) the ‘exercise check-in groups’ in WeChat groups; (d–g) parents can feed back questions through WeChat private message to the nurse or doctor's assistant, and get their assistant; (h) nurses or doctor assistants encourage or affirm the good performance of children in the recent stage; (i) document bag for children in treatment, including a treatment informed consent form, a treatment follow-up notebook and an illustrated treatment guide.
Among children treated with growth hormone, nurses or doctor's assistants set up corresponding ‘exercise check-in groups’ and provided monthly material rewards to children and families who maintained sufficient exercise every day, as shown in Figure 2(c). To ensure the activity of check-in groups, check-in groups were usually established on a monthly basis, including injection punch-in groups, sports check-in groups, and diet check-in groups, and the number of people in the groups was limited to 25 people.
For some problems encountered during treatment, such as diet and exercise, but the time for the follow-up visit had not yet reached, parents could ask questions through WeChat private message to the nurse or doctor's assistant, contact their assistant and be referred to the doctor's clinic if necessary, as shown in Figure 2(d) to (g). The nurse or doctor's assistant would dynamically track the treated children and remind parents of the follow-up time two to three days in advance. Parents who were overdue to see the doctor were notified by WeChat voice again. Through a combination of voice and text, the family members were informed in advance of the inspection items and precautions that needed to be taken during the next follow-up visit and whether fasting was needed. In addition, nurses or doctor assistants could also encourage or affirm the good performance of children in the recent stage through WeChat private messages, as shown in Figure 2(h). Through reasonable doctor‒patient interaction, the anxiety of children and their families could be reduced, and the satisfaction of patients could be improved. Effective communication is essential to establish a good doctor‒patient relationship and practice high-quality medicine, 25 and to improve patient compliance with long-term treatment.
The value of online videos in medical education is increasingly recognized. The cognitive theory of multimedia learning and increasing evidence have confirmed that video enhances learning by activating visual and auditory pathways and presenting text and pictures in a consistent way 26 to help viewers consolidate their medical knowledge more effectively. Currently, with all kinds of video swarming, it is a major challenge to ensure that viewers can watch video content within a limited focus time. Studies have shown that people usually watch a video for a time of 3.9 min, 27 which provides a good suggestion for controlling the duration of popular science videos. The duration of each popular science video was controlled within 3 min in our mobile platform and each short video answers a small question to ensure the effective learning of patients and their parents. In addition, large videos load slowly and have poor quality on unstable networks, making it frustrating to watch and unable to wait. 28
Children's role-playing games provide opportunities for developing and improving children's cognitive skills and intellectual ability. 29 During the treatment, role-playing games and family interactive games were regularly provided to deepen the understanding and confidence of the treatment process and eliminate their fear. In the above interactive games, we have witnessed the whole process of the child's treatment from fear to acceptance.
At the beginning of treatment, we prepared a document bag for each parent, including a treatment informed consent form, a treatment follow-up notebook and an illustrated treatment guide, as shown in Figure 2(i). Parents were encouraged to record the follow-up time and height growth data and reduce the occurrence of lost or missed follow-up through the double reminder of medical staff and parents themselves. The paper version of the treatment guide contained the basic laws of growth and development, the calculation method of genetic height, the correct method and precautions for height measurement, the influencing factors of height, the height percentile comparison table for children and adolescents aged 0–18 in China (boys and girls), and the necessity of height management. Sex and science, nutrition, exercise and disease effects on height, five common diseases that cause short stature, introduction of growth hormone (including physiological effects, drug maintenance and injection, treatment precautions), treatment course, efficacy evaluation, FAQs, etc., which summarize the most concerning issues of parents and the precautions that must be understood to ensure that parents can easily read this basic knowledge even after watching and listening to video/audio popular science.
The evaluated variables and methods in the effectiveness of the WeChat platform
Interview
Before the official launch of the mobile platform, 60 clinicians (40 endocrinologists and child health doctors, 20 other paediatric physicians) and 60 clinical nurses were invited to evaluate the content and design of the mobile platform by interviews. Their opinions and suggestions were collected and sorted.
β-testing
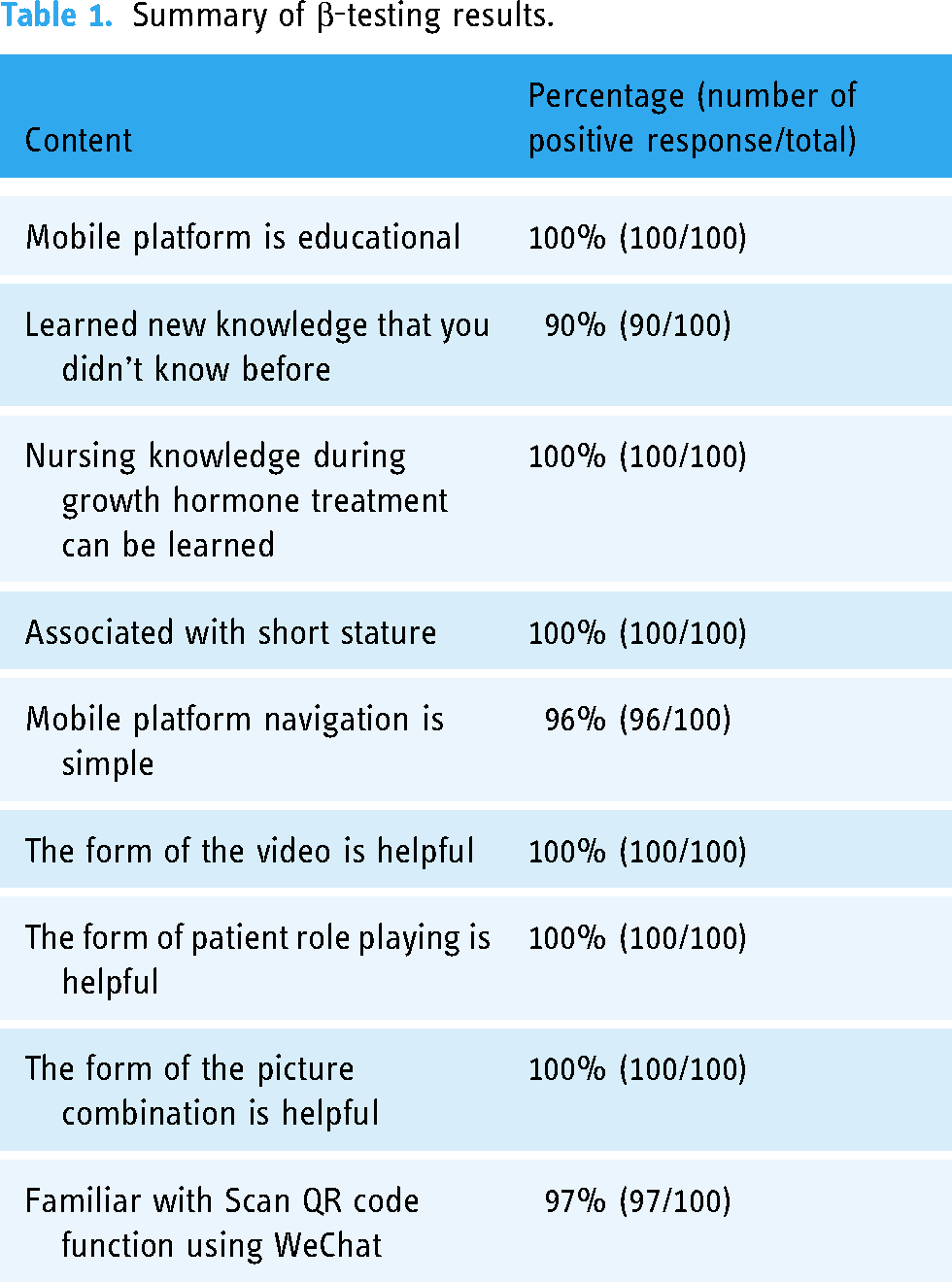
To understand the acceptance of the platform among parents, we recruited 100 parents, who volunteered and briefed them on the purpose and application scope of the platform. All volunteers’ children received growth hormone therapy. Participants were required to use the platform for more than 1 h or until they could provide feedback. 30 All participants received an electronic questionnaire survey with nine questions after using the mobile education platform, and a β-testing was performed (Table 1). Among the nine questions, four were related to whether parents received sufficient health education and nursing information during children's growth hormone treatment, and whether they learned new related topics; the remaining five questions evaluated whether the platform was easy to master and use. Participants answered the above nine questions with ‘yes’ or ‘no’. The above data were derived from the background operation of the system by the information staff.
Summary of β-testing results.
Quantitative scoring of the mobile platform
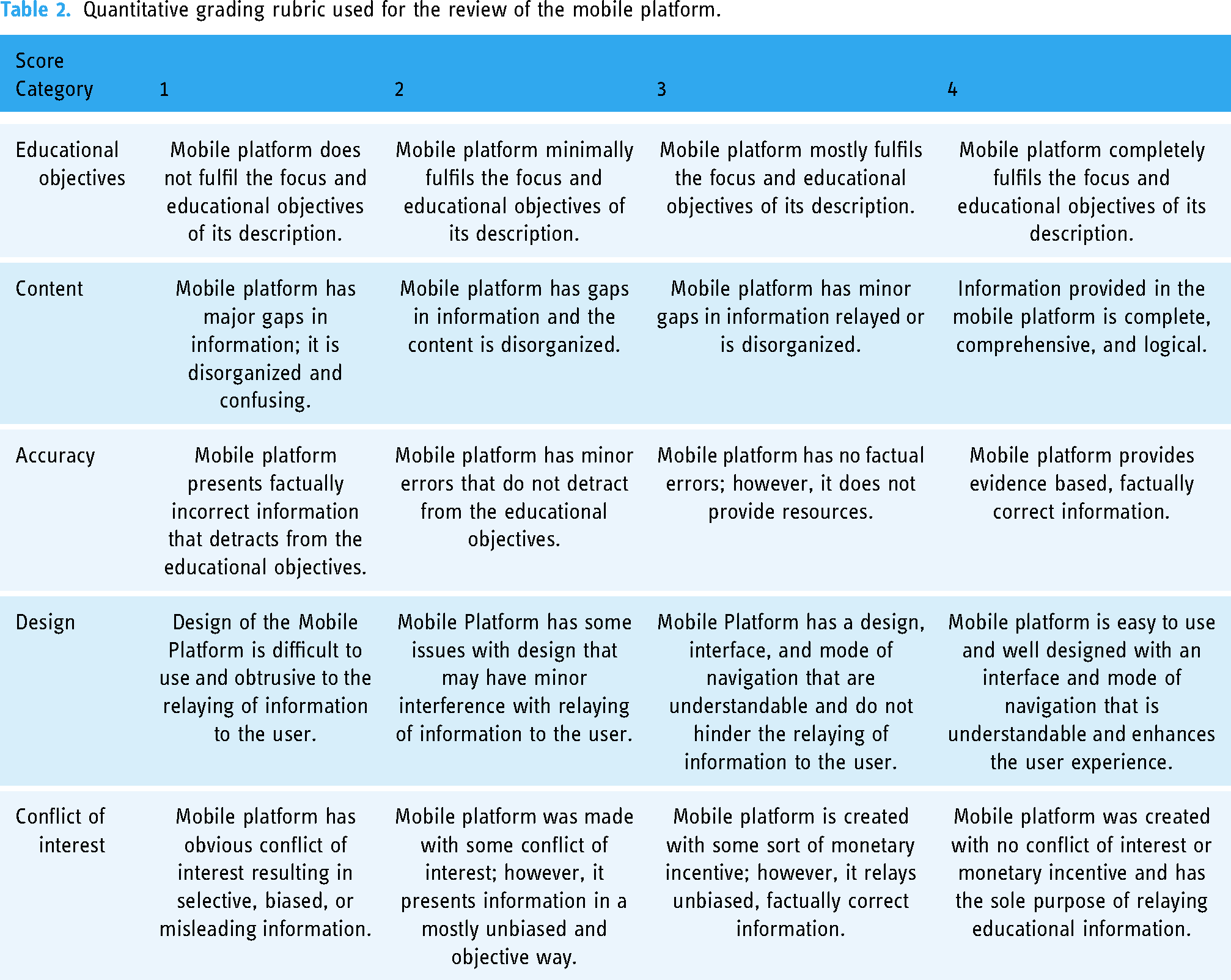
The mobile platform was reviewed by quantitative scoring standards developed by professional researchers.31,32 Combined with the purpose of this research, necessary adjustments and modifications were made to these standards, and a 4-point scale was adopted for each standard.
The final scoring items included (1) educational objectives, (2) content, (3) accuracy, (4) design, (5) conflict of interest. The total score was 5–20 points, and the evaluation was divided into three levels according to the scores: (1) 5–10 points: useless, and may even be harmful to patients; (2) 11–15 points: can be used for patient health education, but has certain limitations; and (3) 16–20 points: valuable and sufficient for patient health education. Quantitative scoring standards are shown in Table 2. 33 Parents of the patients, doctors and nurses (N = 100 each) assessed each of the above five dimensions.
Quantitative grading rubric used for the review of the mobile platform.
This study was not registered. It was approved by the hospital ethics committee, and family members gave informed consent.
Evaluation of patient adherence
A total of 100 children treated with growth hormone therapy were included for compliance tracking for 1 year, and a questionnaire survey on the treatment compliance was conducted by nurses. The survey included the following: (1) patient demographics such as age, education, and household income; (2) therapeutic dose of growth hormone; (3) questions regarding the skills needed to inject needles; (4) time and site of the injection; (5) number of missed injections; (6) causes of missed injections; (7) quality of the relationship with the follow-up physician; (8) medical fee; (9) patient confidence in treatment; and (10) the height difference between the last follow-up and the current visit.
Team composition
Our team was divided into three ranks. The first rank, composed of endocrinologists and nutritionists, was responsible for professional guidance when treating patients’ visits, as well as reviewing and guiding the content of our WeChat public account. The second group consisted of professional nurses and third-party medical consulting service companies. They were responsible for reviewing relevant literature and guidelines for growth hormone therapy and integrating the obtained information into health education content as simply and clearly as possible. In addition, they were responsible for instructing patients and their families to inject growth hormone, reminding parents to follow up, answering and guiding parents’ daily questions and coordinating the work of parents and doctors, as well as doctors, nutritionists and information technology personnel when necessary. Finally, they organized role-playing games and regularly established ‘diet check-in groups’ and ‘sports check-in groups’. The third was composed of information technology personnel, who were responsible for the compatibility of the content and the platform, the design of the mobile platform layout, the shooting of popular science videos, the maintenance of network connections, etc.
Results
Evaluation of the short-stature children's health education mobile platform
Medical staff evaluation
Doctors believed (N = 60) that the content of the platform was in line with current medical practice and clinical guidelines, easy to operate and conducive to fragmented learning. Nurses (N = 60) also expressed their support that the health education provided on the mobile platform helped parents to memorize and master, thereby reducing the need for nurses themselves to repeatedly provide health information. Both clinicians and nurses had a positive attitude towards the mobile platform, believing that the design of the mobile platform was clearly oriented and easy to operate; in addition, doctor‒patient interaction in WeChat groups effectively avoided duplication of work, strengthened doctor‒patient communication and enhanced patients’ trust in doctors.
Family volunteers’ evaluation
Among 100 parent volunteers we recruited, 40% were male and 60% were female, with an average age of 45 years (30–51 years). Volunteers came from Quanzhou city, counties and townships, and there were certain differences in economic income and educational level. All participants used the WeChat health education platform and completed the survey. Eighty percent of the participants used WeChat more than 20 times a day. Overall, parent volunteers believed that they had received enough health education and nursing information during children's growth hormone treatment, and in the contents of ‘Mobile platform is educational’, ‘Nursing knowledge during growth hormone treatment can be learned’, and ‘Associated with short stature’, parent volunteers gave 100% approval. Moreover, most parent volunteers believed that the platform was easy to master and use, and the three contents of ‘The form of the video is helpful’, ‘The form of patient role playing is helpful’ and ‘The form of the picture combination is helpful’ received 100% approval (Table 1).
Quantitative grading rubric
Patients’ parents (N = 100), nurses (N = 100) and doctors (N = 100) evaluated the mobile platform for health education. All scores were >16, suggesting that the mobile platform was valuable and sufficient for patients’ health education (Table 3).
Results of quantitative grading rubric evaluation.

Patient adherence
The general information of the patient is shown in Table 4. All parents and children who could inject themselves mastered the injection method and knew their own treatment dose (usually adjusted by the medical staff), injection site and injection time. Four children terminated the treatment early due to reaching the ideal height in advance, inability to keep up with the economy caused by family changes, children's resistance to injections and parents’ high subjective treatment expectations and dissatisfaction with the actual treatment effect. During the treatment, three people missed an injection once, one person missed an injection twice, and one person missed an injection three times. The reasons were vaccination against COVID-19 (two persons), hospitalization for pneumonia, parents unable to cooperate during injection time (one person), child living on campus and injection by himself (one person).
Main clinical characteristics of the children.

Discussion
The evaluation test provided us with the direction to improve the mobile education platform. In this study, parent volunteers said that during their children's growth hormone treatment, they were exposed to knowledge related to growth and development, and many of these, including diet, vitamin supplementation and calcium supplementation, were different from what they knew. Contrary to the traditional concept, by using this platform, their understanding of health education was updated. For example, it is traditionally believed that drinking bone broth can supplement calcium, but in fact the best foods for calcium supplementation are milk and other dairy products. Drinking bone broth is likely to cause fat accumulation and increase uric acid levels. Ten percent of parents were very concerned about children's height growth. Before using this mobile education platform, they clearly understood that nutrition, exercise and sleep can help children's height growth, but they said that it is difficult to implement these in daily life and look forward to getting help through a certain education platform. A small number of parents (4%) were very unfamiliar with the mobile education platform and could not quickly find the content they wanted when they used it for the first time, but they could master it after approximately half an hour to an hour of operation. Three percent of parents did not know how to scan the WeChat code at first, but with the help of their children, they were able to master it quickly. All in all, all parents said that the platform is easy to use and easy to master. Parents who are semiliterate or have a very low level of education can also obtain corresponding healthy content under the guidance of pictures or videos.
Quantitative scoring can help us better understand usage by different populations. In the educational objectives, some parents said that they had little understanding of the text health education content provided, but the corresponding video operations could help them understand well to guide their children. Some parents said that the video operation allows their children to learn while watching, reducing the pressure on parents to teach their children by themselves. In contrast, some parents suggested that the platform is so interesting that if their children are allowed to watch alone, they will often watch overtime (>1 h/times), which prolongs the child's sitting time and is not conducive to the health of eyesight. Other parents also suggested that in the ‘expert lectures’ of ‘physician's voice’, a brief text introduction can be attached to each expert in the video so that parents can have a quick understanding of the expert in the video. The score of ‘accuracy’ is higher than that of other dimensions, which is related to the perfect composition of our team members (doctors, masters and majors). However, the ‘design’ score is lower than other dimensions, which may be related to the fact that there is more professional content of short-stature, and the network speed is related to the instability of the region. In the later stage, the advocacy and education content will be continuously optimized and displayed in a more concise and easy-to-understand format with pictures and texts.
In sum, doctors and nurses agreed that this mobile education platform could convey professional knowledge in simple terms and was very friendly to parents without a medical background. The parents of the patients believed that the content provided by the educational platform was sufficient for them and played a very good role in guidance and education. The scores of the children's family members, doctors and nurses were all above 15 points, which highly affirmed the mobile education platform.
Up to 75% of young adults and adolescents impair the long-term efficacy of recombinant human growth hormone treatment due to poor adherence.34,35 A variety of factors, including low socioeconomic or educational status, difficulty in injection, lack of choice of injection devices, fear caused by traditional syringes, forgetting injection and injection discomfort, will reduce patient adherence. 36 Thus, this is a problem that must be solved. In some research, a wireless transmitter is installed on the injection pen to transmit the injection data (dose and time recorded in real time) to the doctor, allowing the doctor to remotely check the compliance of individual patients in the real-time setting. 34
The health education mobile platform can not only provide real-time online consultation, but also provide health education for short-stature treated children, including guidance before and during treatment such as healthy exercise, healthy diet and regular sleep, guidance on home injection of growth hormone, identification and treatment of complications, etc. It transforms traditional oral guidance into videos, pictures and texts, which reduces the trouble of doctors and nurses repeating instructions, solves the dilemma that patients have one ear in and one ear out, establishes doctor‒patient trust and improves patient compliance with treatment.
Some studies have proposed that considering the different preferences of patients for SMS and telephone delivery, the combination of SMS and telephone delivery can greatly improve the compliance of the target population. 37 In this study, the combination of pictures, text and popular science videos, and the real-time interaction and correlation of WeChat, enables the family members of the patients to obtain the corresponding answers at any time, build their trust in the doctor and improve the scientific ability of the family members to raise their children.
Combined with the doctor‒patient interaction of the WeChat group, it is very helpful in promoting healthy daily diet, reasonable exercise and timely follow-up of children's treatment. In addition, effective communication can improve patients’ confidence in treatment and make patients feel supported and encouraged 38 to help them take better care of themselves and adhere to treatment. 39
Inevitably, there are some limitations. First, the videos provided in this study are in standard Mandarin, without English or other local dialects. It is not suitable for people whose mother tongue is other languages, who are illiterate or who can only understand local dialects. Second, due to the long course of growth hormone therapy and the high cost, the included patient population was limited to families who received treatment, which may have a certain degree of selection bias. Last but not least, the observation period of treatment compliance in this study was short, lasting for one year. It did not represent treatment compliance for two years or even longer.
In conclusion, mHealth is readily available at low cost and can easily be used for interventions that improve established health outcomes. Based on the interaction on the WeChat platform and the health education of the public account, we greatly increased the interaction with doctors and patients, improved patient satisfaction, and improved patient compliance.
Footnotes
Acknowledgements
The authors thank Shengping YANG of Quanzhou Orthopedic-traumatological Hospital, the husband of Qingling ZHU, for providing assistance with comments on revising the manuscript. The authors thank Mingqing LI and Caimei ZHENG for providing continuous health counselling and height management services to the patients and their parents during the treatment and thank Senhua FENG for providing technical support in the mobile platform related design and network maintenance.
Contributorship
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: WL, QZ, LH. Drafting the article or revising it critically for important intellectual content: YS, QZ, YL. Final approval of the version to be published: WL, QZ, JL. All authors reviewed the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was not registered. And it was approved by the consent of the hospital ethics committee and the informed consent of family members.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Quanzhou city science and technology project (grant number 2022N031S), and Fujian provincial health technology project (grant number 2020QNB044).
Guarantor
WL