
Abstract
Objectives
To compare the environmental health results in women trying to get pregnant or pregnant using a mobile health application (Green Page) through healthcare professionals or self-completed by women, and to explore the relationship between the subjective well-being of these women with their lifestyles and environmental factors.
Methods
A descriptive study with mixed methods was conducted in 2018. A mobile health survey was used in two phases. Phase 1 was a cross-sectional study through professionals (n = 1100) followed by phase 2, a convenience sampling through women's self-reporting (n = 3425). A personalized report was downloadable with health recommendations for the well-being of the mother and child.
Results
Of the 3205 participants (mean age = 33 years, SD = 0.2 years), 1840 were planning a pregnancy and 1365 were pregnant. One in five pregnant women had a low level of happiness. Globally, subjective well-being and happiness were found to be negatively associated with lack of contact with nature, sedentary lifestyle, excess weight, environmental exposure, and older age in pregnancy. Precisely 45%, 60%, and 14% of women were exposed to tobacco, alcohol, and illegal drugs, respectively. The women self-reported levels of risk factors higher than when the tool was used by or through professionals.
Conclusions
The use of mobile health interventions focused on environmental health during planning or pregnancy periods could help improve the quality of healthcare and foster greater involvement of women in their self-care process, thus promoting empowerment, healthier environments, and lifestyles. Ensuring equity of access and data protection are global challenges to be addressed.
Keywords
Introduction
The World Health Organization (WHO) and the European Union consider Children's Environmental Health to be one of the main sanitary challenges of the 21st century, and stimulate the development of strategies to approach these issues. 1 Environmental health risk factors during pregnancy include chemical, physical, biological, and psychosocial risk factors that impact pregnant women and infant health. The WHO and the American Obstetrician Society encourage healthcare professionals to conduct an environmental screening in order to assess exposure and risk to environmental health factors during the prenatal period.2,3 Following this advice, the Pediatric Environmental Health Specialty Unit in the Clinical University Hospital Virgen de la Arrixaca located in Murcia, Spain, developed Green Page, a clinical screening tool on reproductive environmental health.4–8 This questionnaire produces a standard clinical record of each pregnant woman and includes a series of basic questions by healthcare professionals to identify environmental exposures during or when planning a pregnancy. The Green Page approach is based on a comprehensive overview that assesses physical, chemical, biological, social, and psychosocial factors that affect the health of the pregnant woman and her child. Green Page is reproducible and has been adapted to the reality of different countries. 9 Despite efforts and the growing concern of pregnant women regarding environmental matters, the majority of physicians do not routinely screen for known environmental factors. 10
Mobile health is defined as a public health, medical, and clinical intervention based on digital devices such as computers, tablets, smartphones, or other mobile devices. 11 The Spanish health system is reported as one of the benchmarks of the digital revolution, including the use of mobile health, especially during the COVID-19 outbreak. 12
According to the European Union, mobile health applications may increase early diagnosis, promote health prevention, and enhance time management with 30% less effort required in data analysis, thereby reducing costs and expenses in both public as well as private health care and services throughout Europe by 99 billion euros annually. 13 Mobile health interventions offer a chance for the early detection of millions of cases of non-communicable diseases (such as asthma and diabetes) by means of remote diagnosis facilitated by health practitioners in a less expensive way and which can progressively extend their occupational capacity and work productivity.13,14 Other areas presenting opportunities include greater health coverage by enabling equity and inclusion; broadening the range of health promotion and education outreach, which increases patient skills and knowledge; strengthening global health; improving data science research; assisting in healthier aging; and enabling more encouraging strategies, focused on affordable self-care and self-management of people's health which, in general, succeeds in overcoming the patient's reluctance to seek healthcare.15–18
Meta-analyses show that electronic and mobile health-based treatments are effective public health interventions. 19 Efforts from both the patient and the health providers are essential for better well-being and health during pregnancy. Accordingly, mobile health explores self-management in patients relating to pregnancy care to reinforce positive health outcomes.19–22 The mobile health apps that are already in use have different functionalities: informative, educational, or healthcare-delivery intended to address social and environmental health in pregnant women. Although mobile health interventions have shown great potential to modify behavior, relatively few evaluations have assessed the effectiveness of mobile health interventions during pregnancy. Mental health during pregnancy is important for women's health and their offspring. Happiness is a psychological conception with several dimensions of well-being and is one of the most important concepts in the field of mental health, since it represents a protective factor. 23 Maternal stress has an impact not only on the mother but also harms birth outcomes, including low birth weight, preterm birth, lower gestational age, and intrauterine growth restriction.24,25 Examining positive psychology and its benefits on mental health and well-being among pregnant women is very important.26,27 Using mobile health apps may increase the physical, cognitive, and emotional health of women during pregnancy without significant risks or adverse effects. 28
The planning or pregnancy are critical periods for maternal and child health, it is therefore essential to develop and implement intervention strategies to reduce or eliminate environmental risk factors. Mobile health apps related to environmental health offer a potential and novel tool to empower families and communities about their health care. Thus, mobile health applications may contribute to improving the environment and lifestyles of women in the reproductive period and ensuring the normal development of the infant. Self-assessment interventions by apps are needed in order to help pregnant women or women planning a pregnancy.29,30 Accessibility must be created for women who are pregnant or planning a pregnancy so they can gather concise and valuable information concerning environmental health factors that may affect their pregnancy. Through this environmental health self-assessment, the participant received an automated, adapted, and personalized report containing healthcare recommendations for the well-being of the parents and future infants.
The main objective of this study is to compare the environmental health status of women trying to get pregnant or pregnant using a mobile health application (Green Page) by or through healthcare professionals or self-completed by women and to explore the relationship between the subjective well-being/happiness of these women and with their lifestyles and environmental factors.
Methods
Participants and data collection
The Region of Murcia is a Mediterranean region located in the southeast of Spain. It has a population of approximately 1.5 million inhabitants. The Murcian Public Health System assists and monitors more than 98% of pregnant women from the region across the nine Health Areas which it organizes. In 2014, there were 14,200 births in the five maternity hospitals in the Region of Murcia. 31 In the present study, we included women who were pregnant or planning to get pregnant in the Region of Murcia during 2018. We defined women planning to get pregnant as those who were seeking pregnancy. They completed a mobile health survey, and at the end of the questionnaire, respondents received a personalized report with recommendations for improving pregnancy outcomes. The study was conducted in two phases by mixed methods.
In Phase 1, a cross-sectional study was carried out by or through healthcare professionals of the Murcian Public Health System in the first semester of 2018. The mobile health survey was available to all women when they attended their first pregnancy check-up or during a preconception care visit if they were planning to become pregnant. The mobile health application was completed by healthcare providers. The midwives, obstetricians, and reproductive healthcare professionals received training (10 h contact course) about the mobile health version of the Green Page survey.
The sample size in phase 1 was calculated with a confidence level (
For the second period (phase 2), during the second half of 2018, a non-probabilistic sampling was carried out through the web and social networks such as Facebook and Twitter, and with the collaboration of the web portal Natalben Group (Italfarmaco Company). Information was also sent to pharmacies and other health departments (health centers and hospitals). The women accessed the surveys through a link (web format) or through a QR code (posters or brochures). The mobile health application was self-administered and completed by women who were pregnant or planning to get pregnant and who agreed to participate (Multimedia Appendix 1). The responses were limited to one answered survey per email or internet protocol (IP) address.
All responses were reviewed by two experts on environmental health, and participants were excluded from the analysis if they had duplicated information due to software error or with inappropriate or contradictory responses about age, alcohol intake, weight, and height (e.g. ages between 0 and 11 years old, 99 mixed drinks/week, contradictory weight or height). Disagreements were discussed in the research group, and the majority's decision was accepted. Finally, a total of 3205 participants during both phases of the study were considered for analysis.
Survey and report: mobile health green page
Green Page4–8,33 (on paper) is a screening questionnaire of environmental health for pregnancy and lactation periods that has been developed and used since 2009 in the Paediatric Environmental Health Unit of Murcia. Green Page for pregnancy and lactation is a clinical tool that provides a comprehensive picture of the pregnant woman and her partner. Training of the health professional is required prior to use, and it is carried out face-to-face with the pregnant couple within a motivational interview framework in 5 to 7 min. It is a very versatile instrument given that it can be used in preconception consultations, during pregnancy, and during lactation.
The Green Page mobile application was designed and adapted from paper to a web version in 2016 and became available in 2018. The purpose of the mobile application is to obtain valuable information regarding the user's health, detect environmental factors, and prevent, educate, and empower women to reduce or eliminate harmful exposures during pregnancy. It also serves to promote protective factors during pregnancy and to foster maternal and perinatal health outcomes.
This electronic format was grouped into 10 main spheres: (a) emotional state; (b) neighborhood (outdoor air quality by an air pollution annoyance scale and personal perception of environmental risks); (c) hobbies with environmental exposures; (d) medical x-ray exposure; (e) pesticides at home/garden; (f) alcohol, tobacco, and illegal drugs; (g) body mass index (BMI) information and food intake; (h) supplements intake, pharmaceutical products; (i) Occupational exposures; and (j) physical activity (PA)/interaction with nature. This mobile health web application consists of a self-administered survey by pregnant women or those planning to get pregnant. In the end, the toolkit provides each woman with a personalized report offering recommendations for improving the pregnancy outcome. In this automated and personalized report, for each of these spheres, the women received an outcome—emoji face, either red, yellow, or green color with a personalized report containing healthcare recommendations. A green smiley face indicates that current behavior in that category is conducive to a healthy pregnancy. A neutral yellow or sad red face indicates that there is a growing concern about the risk factors that may affect the pregnancy and includes the measures to be taken to decrease exposure and improve environmental health outcomes. Depending on the answers, a downloadable online report was self-generated by the participant. An example of the first page from a personalized report, with visual information (emoji) based on the answers to the questions, is available in Multimedia Appendix 2. Additionally, in the following pages of this report, each category has been expanded with specific recommendations generated from the algorithm based on the woman's responses.
The differences between the traditional and mobile health versions of Green Page are shown in Table 1.

*Only region and country.
Note: Digital version protects the user's identity.
The Ethical Committee and Institutional Review Board of the Clinical University Hospital Virgen de la Arrixaca approved Green Page (SAELCI Project, 18 July 2014). All participants electronically signed an informed consent.
Variables
The following variables were assessed to study their influence on subjective well-being.
Sociodemographic: Country, age (years), maternal main occupation (jobs related to chemical reproductive risk) 34 ; environmental factors of community or at home concern. Environmental and lifestyles: (a) height (m), weight (kg), and calculated BMI (kg/m2); (b) PA was evaluated according to an hour per week of sporting activity and measured by a categorical global self-perceived scale of overall PA—at home, sports activities and work—(sedentary, slightly active, moderately active, and very active); (c) consumption per serving/week of dried fruit, red meat, fresh tuna or shark; (d) illegal (yes/no) or legal drugs—women smoker (yes/no), secondhand smoke exposure (yes/no), grams of alcohol/day; (e) activities in contact with nature (defined as the frequency of activities in a natural environment; mountain, beach, forest, or urban park, or similar); (f) outdoor air quality as measured by an air pollution annoyance scale. This scale relates the perceived risk of families with outdoor air quality on an 11-point Likert scale and ranges from 0 (no disturbance at all) to 10 (intolerable disturbance). For analysis purposes, it was then divided into four categories: <2 good; 3–5 acceptable; 6–7 bad; and 8–10 very bad; (g) dragging chemical traces on job's clothes or shoes at home (yes/no), hobbies of chemical risk for pregnancy (yes/no), and use of pesticides at home/garden (yes/no). Other variables included were: medical ionizing radiation conducted or planned in the coming weeks; folic supplement intake (yes/no).
Outcomes: Emotional state/happiness
The emotional state/happiness was self-reported by a direct question: how happy and well-prepared emotionally do you feel for the pregnancy? It has been studied as a Likert variable where 1 represents “not at all emotionally prepared/unhappy” to 5 “A lot emotionally prepared for the pregnancy/happy” (1 = not at all; 2 = a little; 3 = somewhat; 4 = considerably; 5 = a lot). For analysis purposes, it was then divided into three categories: 1 to 2 not prepared emotionally; 3 somewhat emotionally prepared; and 4 to 5 fully prepared emotionally. From this, 4 and 5 were the variables that grouped the pregnancies considered emotionally prepared or quite, or very happy.
Statistical analysis
The answers to the self-administered survey using the mobile health app were analyzed with IBM Statistical Package for the Social Sciences version 21 (SPSS) statistical analysis software. Data were analyzed by descriptive statistics. An alpha level of significance of 0.05 was used for the statistical tests. The comparison tests aimed to analyze differences between both phases of the study. Furthermore, we undertook an association study between environmental health variables and the level of maternal happiness.
Results
Figure 1 shows the flowchart of the participant's selection. Overall, 77% of those who used the app completed the questionnaire and downloaded the auto-generated personalized report. A total of 3476 participants completed the environmental screening questionnaire in the mobile health application, of whom 7.79% were excluded. Finally, a total of 3205 participants were considered for the study. The mean time taken to complete the questionnaire was 6.5 min.
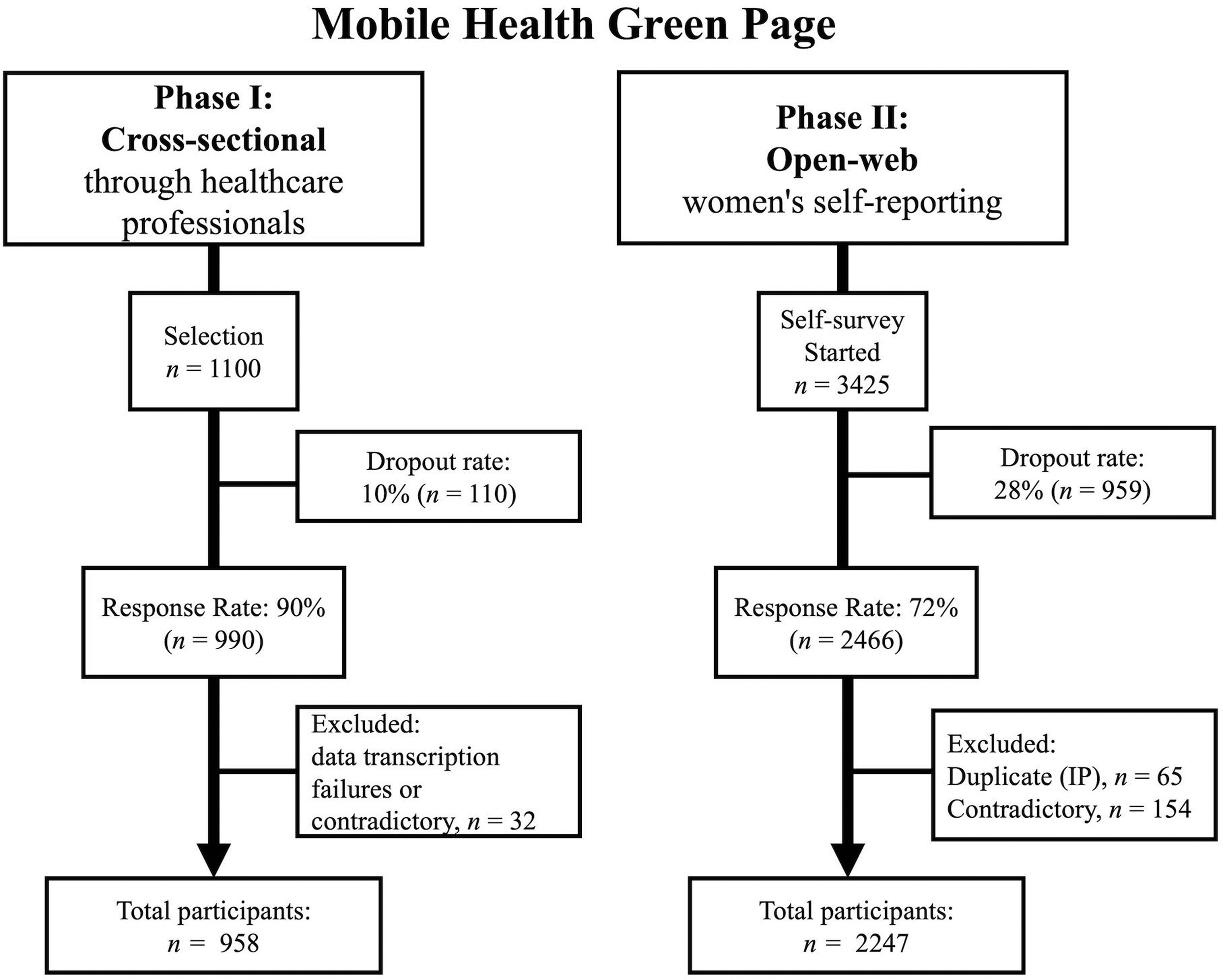
Flowchart detailing selection phases of mHealth green page.
The majority of the surveyed women were planning a pregnancy (n = 1840; 57%) compared to those currently pregnant (n = 1365; 43%). The reported age average of the sample was 33 years old.
Amongst the participants planning pregnancy, 36% had excess weight (26% overweight and 10% obesity). Regarding the geographical place of origin, the majority (
Among the women as a whole, no significant differences were observed in the study variables between phase 1 (mobile health by or through the professional) and phase 2 (self-completed). Nevertheless, the pregnant women self-reported levels of risk factors (alcohol, exposure to cannabis, risky hobbies in the family, air pollution perception scale, and medical x-ray radiation) higher than when the tool was used by or through professionals. The women who planned to have a pregnancy self-reported more alcohol exposure than in phase 1. Table 2 shows the sociodemographic results obtained with the use of mobile health in phase 1 (by professionals) and phase 2 (through women's self-reporting).
Sociodemographic results with mobile health green page in phase 1 (by professionals) and phase 2 (through women's self-reporting).

n: number; CI: confidence interval; BMI: body mass index.
Student t-test used.
Emotional health/happiness
Nearly 20% of the women in both groups considered themselves to not be happy and well-prepared emotionally for the pregnancy. Furthermore, 5% of all the women reported being not at all or little prepared in their emotional health and being unhappy. Lastly, differences by geographic origin were observed in the well-being and emotional health reported between the women planning pregnancy and pregnant women. Precisely 10% of the women planning a pregnancy from the rest of Europe and 11% of pregnant women from the Americas reported that they did not feel emotionally prepared for pregnancy. In phase 2 (self-reporting), pregnant women reported significantly lower levels of emotional health than in phase 1 (by professionals).
Illegal and legal drugs
Precisely 21% of women planning a pregnancy and 14% of those pregnant reported as active smokers and 45% of the women were exposed to any kind of tobacco smoke, including passive smoke. Cannabis or other illegal drug exposure (passive or active) amounted to 15% and 12%, respectively, for women planning a pregnancy and pregnant women. Precisely 36% to 47% of the total women reported being teetotalers.
Food/supplement consumption
For the women planning a pregnancy and the pregnant women, the consumption of any weekly servings of predatory sea fish was 44% and 29%, respectively. Precisely, 90% of both groups identified weekly consumption of more than one serving of red meat. In both groups, 16% of the women ate no fruit. More than half (60%) of the women planning pregnancy reported folic acid consumption in preparedness for the pregnancy, while 90% of the pregnant women reported consuming that supplement.
PA, contact with nature
Precisely 11% of the women lived sedentarily. Only 13% of the pregnant women carried out activities in contact with nature daily, while that percentage reached 19% in the women preparing for pregnancy. When comparing the data for emotional health and happiness, we found that for the most emotionally prepared subgroup, the results of the pregnant women who performed daily activities in natural environments presented a percentage difference of 7.7 points higher than that of women who reported not performing any activity in nature (<0.05). In the group of women who were preparing for a pregnancy, the differences between the same groups were 4.5 points (<0.05).
Occupational exposure
Precisely 60% of all the women had jobs related to chemical reproductive risk. In 16% of the families, some members of the household had clothing or shoes contaminated with chemical products from work to home.
Environmental risk perception
Around 33% of the women identified at least one environmental factor that concerned them in their neighborhood or community. The most frequent community environmental pollution factors identified by the total of this subgroup were air pollution (23%), home age (22%), exposure to pesticides in nearby areas at home (12%), and the lack of green areas (10%).
Outdoor air pollution/Chemical exposure at home
Precisely 29% of women planning pregnancy and 31% of pregnant women were exposed to pesticides in their home or gardening activities. Nealy 33% reported bad to very bad air quality in their neighborhood.
The demographic descriptions and differences in well-being and happiness (emotional health) outcomes between both groups are shown in Table 3.
Sociodemographic characteristics and emotional health outcomes.
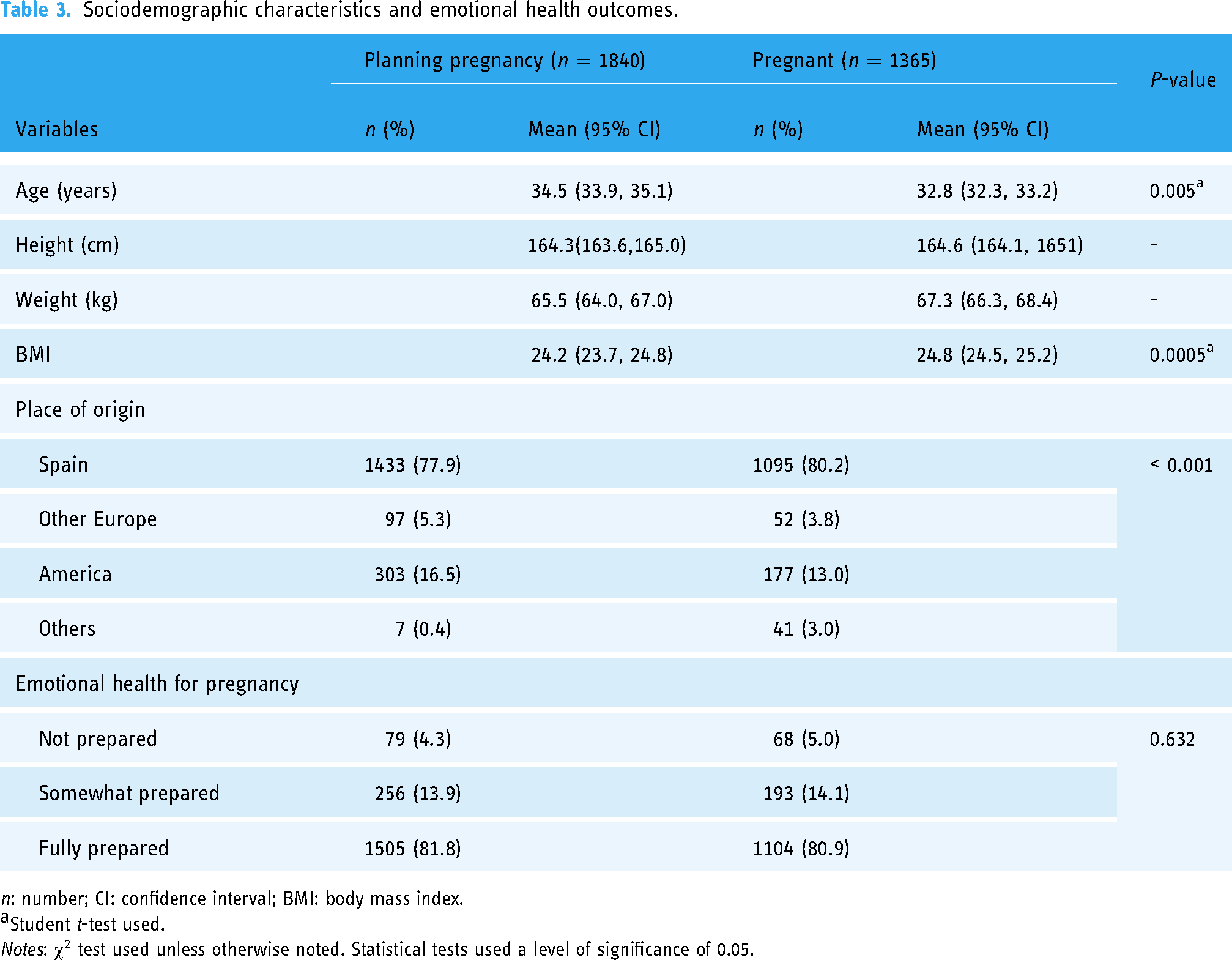
n: number; CI: confidence interval; BMI: body mass index.
Student t-test used.
Notes:
The lifestyles and exposure to legal and illegal drugs between the two groups of the sample are presented in Table 4.
Drugs and lifestyles.

n: number; CI: confidence interval; PA: physical activity.
Student t-test used.
Notes:
Table 5 shows the results of the chemical and ionizing radiation exposures.
Chemical and x-radiation exposure.
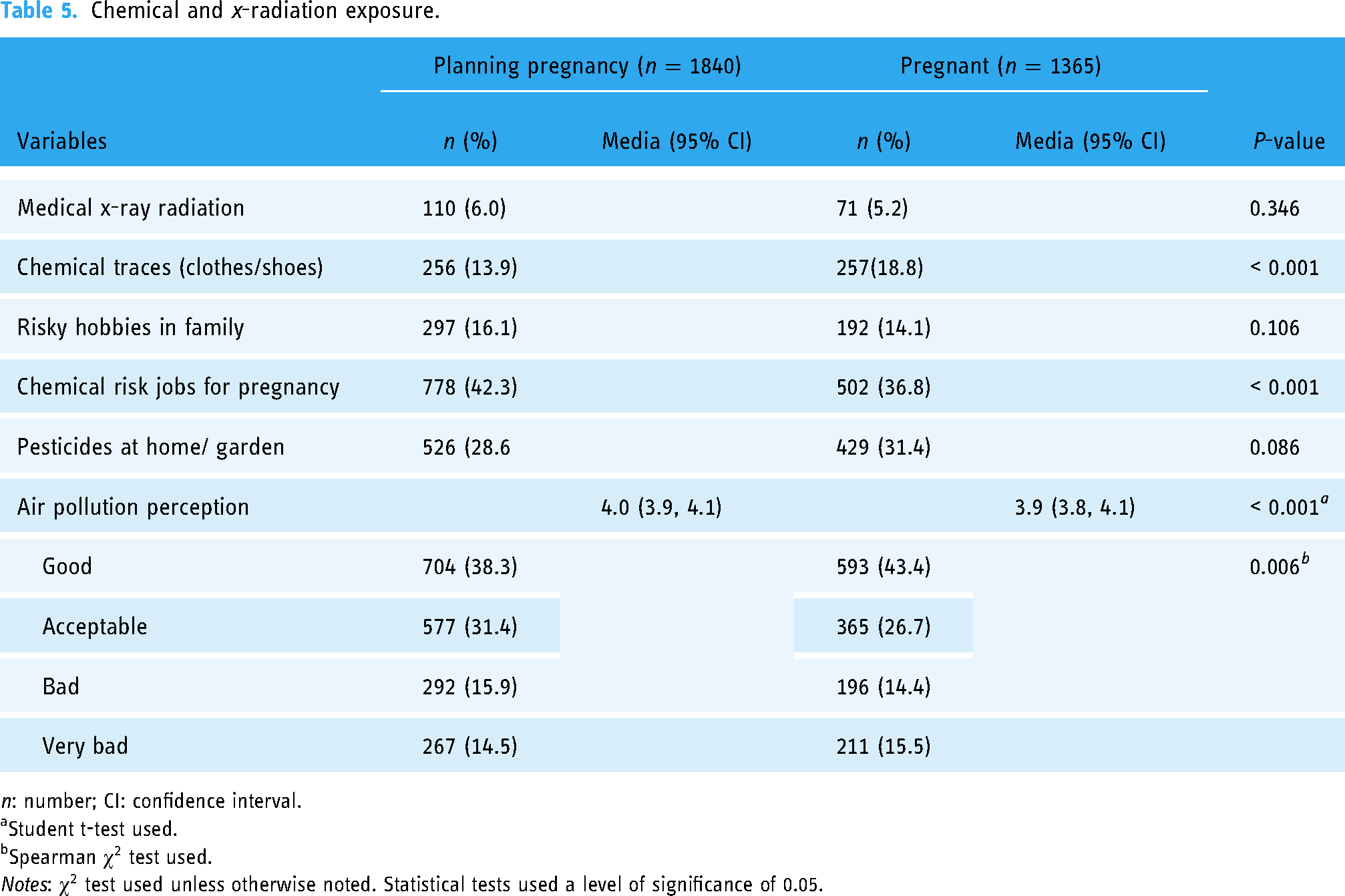
n: number; CI: confidence interval.
Student t-test used.
Spearman
Notes:
The distribution of the state of emotional health and happiness was studied for pregnancy associated with different environmental health risk factors in Tables 6 and 7. Different statistical tests, such as the Spearman correlation test and chi-square test, were run to assess various relationships between these variables.
Emotional health and happiness in preparedness for pregnancy in women planning pregnancy and pregnant in association with environmental health factors.

Notes:
Emotional health and happiness in preparedness for pregnancy in women planning pregnancy and pregnant, correlated to age, BMI, alcohol consumption, and outdoor air pollution perception.
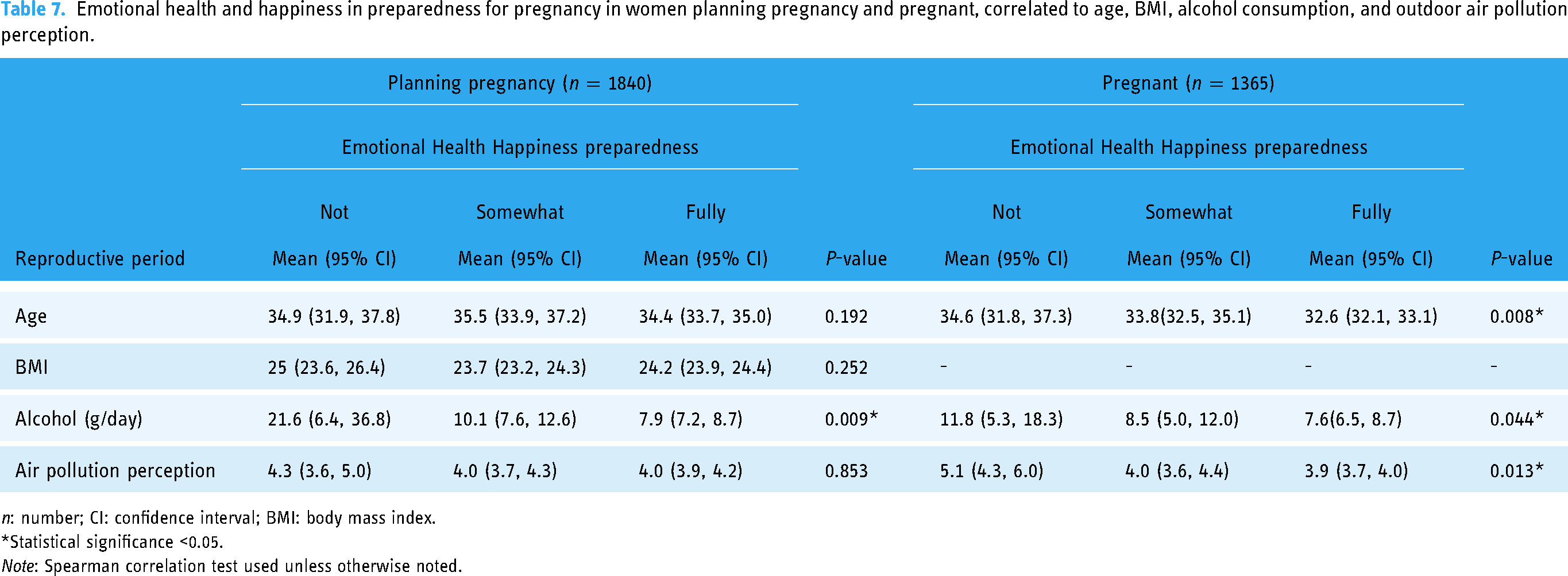
n: number; CI: confidence interval; BMI: body mass index.
*Statistical significance <0.05.
Note: Spearman correlation test used unless otherwise noted.
Discussion
The environmental health data reported in our study display an interesting profile to discover certain opportunities for public health strategies to benefit mothers and their infants.
The screening of environmental health reported similar results when women completed the mobile health (Green Page) by themselves to when it was done by or through the healthcare professional. These findings are important to us because these tools can help increase efficiency, reduce visits to the doctor, and also provide valuable guidance to pregnant women or women who want to get pregnant with the best recommendations through learning tools and artificial intelligence.
Precisely 80% of women of childbearing age and seeking pregnancy feel happy and emotionally prepared for the pregnancy. In our study, this indicator is associated with age, the geographical place of origin, and environmental factors such as exposure to drugs, contact with nature, or lifestyles related to reproductive health and pregnancy. Globally, the data reported by women about exposure to legal and illicit drugs is alarming. The national average maternal age estimated (32 years) by Spain's National Statistics Institute 31 is similar to that of our results (33 years). Overall, young pregnant women in our study refer to being happier and emotionally prepared. The distribution of the origin of mothers is that they are predominately from Spain, followed by Latin America and the Caribbean. It should be especially noted that among the geographical differences obtained in the outcome of subjective well-being, a relatively high frequency (11%) of women of American origin did not report feeling emotionally prepared for pregnancy. To explain these differences, cross-cultural and social aspects such as chauvinism, health inequities, and poverty, as well as the psychosocial approach of pregnant young women, should be addressed.35–37
According to the Centers for Disease Control and Prevention, 38 women preparing for pregnancy with a weight above average are more likely to experience adverse maternal and neonatal outcomes (e.g. cesarean delivery, macrosomia, stillbirth, and/or childhood obesity). 39 In our study, 35% of women planning pregnancy had a BMI above the recommended level, similar to the prevalence (31%) of overweight/obese women for the same age groups. 40 Body weight, diet, and PA may influence a healthy pregnancy; so this is clinically important in order to help improve women's and children's health outcomes.41–43 In our study, 10% of the pregnant women reported being sedentary, and 28% did no exercise per week. Increasing PA such as walking could help reduce premature deliveries, improve birth weight, and lead to a healthier child,44–46 also contributing to decreasing air pollution in cities, and diminishing the personal carbon footprint. 47 In our analysis, women with positive emotional health are more active physically and in contact with nature (Table 6a). Recommendations for pregnant women include a workout of at least 2.5 h weekly, together with a balanced diet that includes an intake of more fruits and vegetables, and less red meat, in order to maintain a healthy weight.38,48 According to the European Health Survey 2020 in Spain, 31 71% of women reported a daily intake of fruits which was similar to our findings. The intake of folic acid as a supplement in the analyzed women was high. 49 This might indicate that the respondents are taking measures to prepare for a healthy pregnancy.
Exposure to legal and illegal drugs is a growing global environmental health problem.
5
The prevalence of tobacco smoking during pregnancy in this study (14%) is higher than the estimated 10% in the European Perinatal Report,
50
but lower than the estimated 19.8% smokers in the general population of Spain.
51
However, similarly, 20% of the women planning a pregnancy in the present study were reported as active smokers. These differences are possibly due to those answers being given during the pregnancy, without the trimester or period of pregnancy being specified, and it is known that consumption decreases throughout.
5
Other researchers have reported that between 14% and 20% of pregnant women in their study were active smokers.
52
Spain is reportedly among the European countries where smoking (mostly tobacco) during pregnancy has a higher prevalence.
52
Alcohol intake in our survey exhibits a high daily consumption, with 64% of women planning pregnancy and 53% of pregnant women; this is concurrent with previous research.53–55 No amount of alcohol consumption is without effect.
5
Alcohol is a known neurotoxic substance, and such exposure might explain the estimated prevalence of 2.5% fetal alcohol spectrum disorder in Spain.
56
The binge intake model is very important to be screened for and detected during critical periods of pregnancy. We have observed geographical differences in exposure to legal and illegal drugs between Europe and America (

Emotional health (x-axis) in women planning pregnancy and pregnant in association with air pollution (y-axis), and alcohol consumption (y-axis), N = 3205. Note: One-way analysis of variance (ANOVA) test used with significance level 0.05.
Planned or exposure to ionizing radiation was only 5% of the women having an x-ray or body scan scheduled for the upcoming weeks at the time of completing the survey. Ionizing radiation exposure during pregnancy is potentially teratogenic and neurotoxic, and a risk factor for developing childhood cancer.5,61 It is important to consider that women of childbearing age who require an x-ray test should have it done in the second half of their menstrual cycle. 62
On average, our results show that air quality was perceived to be within an improbable range of levels, as evidenced by exposure to environmental air pollution (23% > 7 out of 10).63,64 A trend was observed of a higher proportion of women emotionally prepared for pregnancy who perceive the air in their environment as good and acceptable. This scale is related to air pollution levels of NO2, and particulate matter (PM10) in the neighborhood. 65 Exposure to urban air pollution is associated with decreased weight in infants, physical growth retardation in early life years, neurodevelopment alterations, and preterm birth.66–68
Non-occupational exposure to pesticides accounts for severe morbidities and mortality rates due to their frequency of usage and persistence in the environment. 69 Exposure to pesticides in the yard or residence was reported at 30%. Exposure to pesticides is associated with urogenital malformations and other alterations by hormonal disruption. It is therefore vital to improve the home environment's quality of life. 70
Precisely 40% of the females declared working in jobs with chemical risk for reproduction or pregnancy. Of that figure, healthcare professionals, along with the agricultural industry sectors (43% and 13%, respectively) were the most frequently exposed. It is essential to take appropriate occupational and personal measures to avoid and reduce exposure to chemicals and environmental substances that pose a risk to maternal and child health. These measures include changing out of work clothes and work shoes before leaving work. Para-occupational exposure to these substances may be a major source of exposure to endocrine disruptors.71,72
In terms of perceived environmental risk of concern in their neighborhood or community, air pollution and the age and condition of the residence were the predominant factors. The age of the home provides a valuable source of information about the quality of the construction materials and the quality of the air inside the house. According to the WHO, 47 housing conditions may affect human health and be attributable to many preventable morbidities.
Previous research suggests that women with a positive attitude toward pregnancy had a higher parental self-efficacy and well-being, and this may mean less risk for maternal and child adverse health outcomes.18,73,74 When determining the relationship between the emotional health of pregnant women and those planning a pregnancy with other environmental factors, statistical significance (p-value < 0.05) was reached when analyzing the following: age, BMI, binge drinking, cannabis, and illegal drug exposure; big fish servings per week; folic acid consumption; PA; geographical place of origin; air pollution perception; and contact with nature. Researchers in China 68 supported the implications of air pollution on the mental health of pregnant women; in our analyses, we can reaffirm this since we found a significant association between the emotional state when preparing for pregnancy in both women planning pregnancy and pregnant and the perception of air pollution. In our analysis, relating subjective well-being with contact with nature in the population studied suggests that an association exists, which could be explored in greater depth in a future approach. Spending time in nature helps to reduce maternal stress and exposure to air pollution. Exposure to air pollution during pregnancy and living in areas with little surrounding vegetation, or more than 1 km from urban parks have been related to adverse effects on the offspring, such as inadequate birth weight, premature births, or uterine growth retardation.75–78 Researchers have also previously found evidence regarding the effect of the proximity of urban parks on the blood pressure of 3416 women in the first trimester of pregnancy and suggested that the probability of having normal pressure increased when closer to green areas, 79 acted as a protective factor against preeclampsia. In another study, contact with nature in pregnancy or planning it promoted bonds with nature that allowed their future children to have a greater connection with nature, positively impacting their physical and mental health. 80 Moreover, lower levels of personal exposure to air pollution among pregnant women residing in greener areas were found in a study in Barcelona, Spain. 81 The results of our study show us alarming data that highlight the need to promote “nature prescription” initiatives in pregnant women and future pregnant women, as well as to communicate and disseminate the benefits of contact with nature for improved health for both them as well as their offspring. In the group of women planning to be pregnant, we found an association between the weekly consumption of fresh fruits and emotional health, compared to the other group of pregnant women. In addition, women planning for a pregnancy have significant associations between emotional health and chemical risks. No significant associations were found for tobacco exposure or red meat servings weekly in both cohorts. Any tobacco smoke exposure during preconception and pregnancy may be associated with an increased risk of mother morbidities, infant mortality, and other human health risks. 82
Furthermore, another noteworthy aspect of this study was the power to compare two samples that used different data collection methods (by or through healthcare professionals or self-completed by women). We found significant differences between the samples, especially among the pregnant women. It is likely that the legal, social, and psychological conditions (stigmas) that certain habits imply (alcohol, tobacco, or cannabis intake) may be one of the reasons why the results have differed. It is possible that the fact that the application issues a report may encourage women to be more candid in their responses because they were then provided with a report that assessed the real risks to which the fetus may be exposed.
Additionally, significant differences have been found in other spheres of the environment of pregnant women (hobbies, pesticides, and folic acid intake). Pregnant women who have completed the questionnaires on their own probably have a greater perception of risk that allows them to be more objective when it comes to knowing and being exposed to day-to-day environmental risks. Self-completed Green Page during pregnancy seems to better detect the risk factors such as alcohol or loss of happiness than when completed by professionals, possibly due to the anonymity and privacy provided by the mobile application.
The intervention of mobile health applications proves to be a novel and useful tool for the integrated management of women's health in pregnancy and its preparation. Risky behaviors and environmental risk exposures have enormous implications for maternal and child health, so it is imperative that these factors can be modified and thereby reduce potential harm through public health education and information acquired by this mobile application. 83 Additionally, with rising healthcare costs, particularly in underserved areas, mobile health applications could provide an affordable and accessible means of managing women's health during pregnancy and its preparation. Underserved communities must be guaranteed equitable access to health information provided by these technologies and ensure personal data protection in the face of a globalized information system. These challenges represent areas of focus that must be addressed in the future to fully harness the potential benefits of mobile health interventions for women's health. Future research could explore ways to maximize the effectiveness of mobile health applications in reaching underserved communities and reducing disparities in access to maternal and child health information and services.
Strengths and limitations
The present study faces some limitations. Firstly, sample validity, the sampling was not random, women were volunteer participants to answer the self-questionnaire using the digital tool, which does not allow inferring from the data. Secondly, the problem of non-response, following self-selection, or the automatic exclusion of those without Internet access. Human error, recall, and survey bias may have been incurred when answering the questionnaire. Nonetheless, the overall dropout rate was around 25% of those who started the questionnaire. The dropout rate was much lower in phase 1 of this study, in which the invitation to participate was made through trained healthcare professionals, thus offering the opportunity to provide trusted source information. Thirdly, it may happen that stakeholder bias in obtaining certain results contributes to the massive participation of people oriented toward one direction. To try to control this, the results were reviewed and limited to one response per email address or IP address of a device. In this part of the study, another limitation is unverified respondents. Survey responses were reviewed by two experts from the research group, and when responses were contradictory or incongruent, they were eliminated. Likewise, other important socioeconomic aspects such as educational level and income are not included in the questionnaire. This has been done intentionally to encourage participation, reduce time and avoid stigma, asking about aspects that could be important for professionals, but perhaps not so much so that they could be changed by the pregnant woman.
As strengths of the study, the results serve as a basis to describe the perception, challenges, and opportunities of physical and emotional health associated with environmental health factors in pregnant women or women planning a pregnancy. In phase I of the study, satisfaction with the tool was measured by means of a satisfaction questionnaire where 100% of health professionals and women participating gave a positive global assessment (average 7.7 out of 10), the most valued was the personalized report received and having the opportunity to contact a health professional. 84 In addition, our response rate was comparable to that reported in other studies.85,86 The percentage of women who completed the questionnaire, once started, suggests that it was well accepted by the participants. Moreover, downloading the report from the mobile application provides personalized information on environmental risks and how to improve them. In addition, this has the advantage that it effectively facilitates the work of clinical/medical staff, reducing the existential workload, and without requiring specially trained health professionals in environmental reproductive health.
This study did not implement the use of quality of life (QoL) scales to measure subjective well-being in women's pregnancy preparation. 87 However, it is the subjective nature of self-assessment by women through simply asking in our questionnaire, “How happy and emotionally prepared do you feel as a future mother?,” associations arise as a proxy for environmental risk factors for reproduction. For future studies, it is recommended to expand the information, and offer personalized health reports as a result of the mobile health application, to newborns, children, and adolescents, taking the offspring into account. Standardization of the format and systematized application of mobile health as a health intervention in pregnant women or preconception is necessary in order to ascertain its quality when educating, informing, and training in the self-care of women and their newborns. Finally, we conclude that more studies are needed to understand the magnitude and direction of the associations between the emotional health of women who are pregnant or planning to get pregnant and contact with nature; exposure to legal and illegal drugs; PA; among other environmental factors reported in the group studied.
Conclusion
A significant proportion of women who are pregnant or planning a pregnancy could improve their happiness and emotional preparedness to face being mothers-to-be. Emotional health indicators could serve as a proxy for identifying other environmental risks during pregnancy. Women's self-reported values of exposure to environmental contaminants and lifestyles seem higher than those obtained through professional surveys. Additionally, further analyzing the interactions between other variables might warrant exploration. Observational studies that allow the direction of the effects to be inferred will be needed.
Mobile health apps for environmental health provide valuable information on exposures to environmental risk factors in a way that is accessible to the general population, particularly in socially disadvantaged or remote settings. Additionally, they allow for self-assessment, which can help identify and implement effective intervention strategies to promote healthier lifestyles and environments during pregnancy. Future follow-up studies with a more experimental design may help clarify the hypotheses arising from this study.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231177146 - Supplemental material for Subjective well-being, happiness, and environmental health factors related to women planning a pregnancy or pregnant, using mobile health intervention
Supplemental material, sj-docx-1-dhj-10.1177_20552076231177146 for Subjective well-being, happiness, and environmental health factors related to women planning a pregnancy or pregnant, using mobile health intervention by Juan Antonio Ortega-García, Miguel Felipe Sánchez-Sauco, José Alberto Zafra-Rodríguez, Laura Teresa Cabrera-Rivera, Francisco Díaz-Martínez, Eduardo Manuel Llegus-Santiago, Juan Luis Delgado-Marín, Esteban Orenes-Piñero, Nicole Kloosterman, Albert Bach, Carlos Ojeda-Sánchez and Rebeca Ramis in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231177146 - Supplemental material for Subjective well-being, happiness, and environmental health factors related to women planning a pregnancy or pregnant, using mobile health intervention
Supplemental material, sj-docx-2-dhj-10.1177_20552076231177146 for Subjective well-being, happiness, and environmental health factors related to women planning a pregnancy or pregnant, using mobile health intervention by Juan Antonio Ortega-García, Miguel Felipe Sánchez-Sauco, José Alberto Zafra-Rodríguez, Laura Teresa Cabrera-Rivera, Francisco Díaz-Martínez, Eduardo Manuel Llegus-Santiago, Juan Luis Delgado-Marín, Esteban Orenes-Piñero, Nicole Kloosterman, Albert Bach, Carlos Ojeda-Sánchez and Rebeca Ramis in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors express gratitude to all members of the PEHSU at the Clinical University Hospital Virgen de la Arrixaca. The authors also acknowledge the contribution of all the volunteers of this project. Thanks go to the collaboration between the Italfarmaco Spain Company and PEHSU Murcia for joining forces to achieve the results.
Contributorship
JAO researched literature and conceived the study. JAO, JAZ, and MFS were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. JAO and JAZ contributed to the development of the application. NK and EML wrote the first draft of the manuscript, conducted statistical analyses, and interpreted the results under the supervision of JAO. JAO, FDM, and EML contributed to data visualization. RR, CO, AB, and LTC aided in statistical analysis, and interpreted the results and the discussion. All authors reviewed and edited the manuscript for intellectual content, and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The ethics committee of the Clinical University Hospital Virgen de la Arrixaca approved this study (Project SAELCI, 18 July 2014).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Foundation for Formation and Research (FFIS) from Murcia's Drug Commissioner Office (Ecosistema Saludable, Neurodesallorro Saludable), the National Plan on Drugs, Ministry of Health, Spain (ID8437); the Mount Sinai International Exchange Program for Minority Student (Grant MD001452) from the National Center on Minority Health and Health Disparities of the U.S. National Institutes of Health; and the Sociedad de Pediatría del Sureste de España and its contribution to the project “Profile of childhood and adolescence environmental health in the region of Murcia” (FFIS-DF-2022-36). EOP is supported by a postdoctoral contract from the Instituto Murciano de Investigaciones Biosanitarias Virgen de la Arrixaca (IMIB-Arrixaca, Murcia, Spain).
Guarantor
JAO.
Informed Consent
All participants electronically signed an informed consent.
Trial registration
Not applicable, because this article contains no clinical trials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.