
Abstract
Objective
The ongoing pandemic has accentuated the use of telecare services; however, only limited progress has been made in understanding the barriers and facilitators to using these services. In order to move towards sustaining such essential services, the present study aimed to ascertain the experiences of stroke survivors and healthcare providers regarding the utilization of a post-stroke telecare service in Hong Kong.
Methods
Interpretive description was employed for this study. Semi-structured discussions and interviews were undertaken with nine stroke survivors and four stroke nurses who delivered the telecare services. The principles of thematic analysis were inductively followed to analyse the data. The Standards for Reporting Qualitative Research checklist was used to guide the reporting of the data.
Results
Three themes emerged: (a) pre-existing post-discharge service pathways; (b) push factors/facilitators for telecare usage; and (c) barriers to telecare usage. Overall, the telecare service was considered a significant alternative and one that complements conventional face-to-face follow-ups. Stroke survivors were motivated to use the service because it was convenient and flexible. However, significant barriers exist, including technical issues and a lack of guidelines and training opportunities for healthcare providers.
Conclusions
Although telecare is still evolving, several factors drive stroke survivors to use the service. Attention needs to be paid to the emerging barriers to improve long-term usage of the service. Clear guidelines are needed to underpin the development and implementation of telecare services.
Introduction
A stroke is a life-threatening situation that happens when the blood supply to the brain is interrupted and can be broadly categorized as haemorrhagic (bleeding) and ischemic (thrombotic). Stroke affects ∼17 million people every year and has been one of the leading causes of death globally. 1 Persons recovering from stroke require life-long care to prevent the recurrence of stroke and to manage their functional deficits. The evidence suggests that about half of stroke patients experience recurrent strokes within a few days or weeks of the initial event, with the greatest risk occurring during the first week.2,3 Recurrent stroke not only impairs once-recovered physical and cognitive functions, but also leads to prolonged hospitalization, worsened mental well-being, and increased mortality. 4 Considering the seriousness of the aftermath of the first stroke, it is crucial to institute continued efforts to improve the effectiveness of secondary prevention strategies.
Current gap in care and telecare
Following discharge, post-stroke patients are usually referred to nurse-led post-acute stroke clinics operated by stroke advanced practice nurses for continued observation and follow-up. 5 These nurse-led clinics generally provide secondary care services, such as a comprehensive stroke assessment, risk factors and healthy lifestyle education, medication reminders, and caregiving support to facilitate the survivors’ rehabilitation progress. 5 Stroke nurses often also coordinate with multidisciplinary teams to provide integrated care to survivors. Over the years, studies have proven the clinical effectiveness of these nurse-led clinics in reducing depressive symptoms, 5 hospital readmission rates and recurrent stroke rates, 6 and in improving blood pressure control. 7 However, the emergence of COVID-19 disrupted face-to-face services which made continuity of care rather challenging, especially for stroke survivors who live in rural areas or have difficulty in leaving home due to physical disabilities. 8 Meeting in person is in fact unfavourable for infection control as it further increases the risk of disease transmission. 9
The development of telecare in the past few years has helped to improve the service delivery of the clinics and increased the satisfaction of both nurses and stroke survivors. Telecare, through which healthcare professionals utilize telecommunication technologies such as telephone modality, Zoom, and Skype to remotely diagnose and provide treatments to patients, has been adopted globally in the past few years. 10 In fact, telecare services came to be regarded as an alternative as the pandemic evolved, and are still expected to be used after the pandemic. 11 Given the significant quantifiable and qualifiable advantages as supported by a growing body of literature, telecare has the potential to be further sustained in the clinic beyond the pandemic and to enhance the quality of the care delivered to post-stroke patients. Previous investigations have shown that when compared to conventional face-to-face consultations, telecare could lead to significant improvements in blood pressure due to ongoing monitoring, medical adherence, activities of daily living, executive function, and memory rehabilitation in patients.12–14 Several qualitative studies also showed that stroke survivors found telecare convenient and user-friendly because they could connect with their healthcare team anywhere and at any time when nurses were available.15,16
The increased use of telecare services has become more pronounced recently due to the ongoing COVID-19 pandemic. Social distancing measures and a fear of becoming infected have deterred patients from returning to use available services on a face-to-face basis. 17 However, there may be various barriers to the continuous use of telecare services in clinics. For example, patients might experience difficulties in setting up the telecare system, 18 while providers might not be able to conduct physical examinations such as assessing the patients’ limb power to evaluate their recovery status. 18 There are also issues to be concerned about, such as administrative licensing, financial sustainability, 19 technical support for managing updates and new developments, 20 and the establishment of proper telecare guidelines and policies. 21
In Hong Kong, just like in other parts of the world, the use of telehealth and telemedicine is not a new phenomenon. In fact, in 2002, the feasibility of implementing telehealth services among older adults was examined and was observed to be cheaper than providing conventional care and to be well accepted by healthcare providers as well as clients. 22 However, the growth thereafter has been rather slow, although the impact of the ongoing pandemic has awakened calls to push for the wider implementation of telehealth not just in Hong Kong but across the globe as a strategy to reach more patients and their families in their homes and communities.23,24 The ongoing pandemic has demonstrated that it is possible to deliver some form of care virtually via telehealth. However, as the world recovers from the pandemic and prepares for a post-pandemic era in which the use of telehealth has been forecasted to further escalate, it is important to examine the experiences of people who delivered and received care via telehealth, as these can offer insights into the facilitators and barriers that favoured or hindered the process. 24 Although some forms of barriers and facilitators have previously been highlighted in the literature, these have mostly been from the perspective of healthcare providers. 25 In addition, the added aspect of living through the pandemic may give rise to new issues worth exploring to inform strategies and policies that seek to promote the use of telehealth. This creates a critical gap, and it is argued that by uncovering the experiences of both care providers and stroke survivors, it will be possible to identify potential barriers, facilitators, and strategies to improve telehealth usage in the long term. This may provide insights for the continued adoption of telecare as a usual healthcare delivery mode for post-acute stroke follow-ups in a nurse-led clinic setting. To this end, in this study, the experiences of stroke survivors and healthcare providers were examined in relation to their utilization of a telecare stroke service in Hong Kong.
Methods
Study design
Standards for Reporting Qualitative Research checklist guided the reporting of the results. Interpretive description (ID) was employed for this study. 26 ID is a non-categorical approach grounded in the epistemological mandate of generating findings that can feed into healthcare practices along the continuum of care. 27 The inductive stance of ID to understand phenomena that translate to healthcare practices makes it particularly helpful for this study. In addition, the aspect of capturing shared realities is particularly essential, as it will permit both patients and healthcare providers to be included in one study.
Setting and participants
The present study was conducted in collaboration with a Neurological Medical Ward in one of the largest hospitals in Hong Kong. The ward was assigned to be a pioneer in the hospital in the implementation of telecare. Telecare in this study was applied in order to streamline the hospital's systems to limit the need for stroke survivors to come to the hospital. Stroke survivors could use either a smartphone, a tablet, or a computer to interact with a nurse in a pre-assigned schedule. The study employed a convenience sampling method and targeted stroke patients who had been discharged from the ward and who had at least one risk factor, either diabetes or hypertension, or both. They were included in the study when they: (a) were diagnosed with stroke within 1 month before enrolment; (b) were referred to a nurse-led post-acute stroke clinic; (c) aged 18 or above; (d) were cognitively competent with a score ≥22 in the Montreal Cognitive Assessment Hong Kong version 28 ; and (e) lived at home before being admitted to hospital and after being discharged. Patients were excluded when they: (a) had hearing or visual problems; (b) could not be reached by phone; (c) were bedbound; and (d) required physical contact during a consultation, for example, wound dressing. Stroke advanced practice nurses with at least a postgraduate qualification in nursing and had provided the telecare service in the stroke clinic for a minimum of 6 months were invited to take part in this study by commenting on their supportiveness and willingness to sustain this innovative delivery model. The nurses were fluent in both Cantonese and English and adept at technology.
Facilitation of technology and education
The telecare service was delivered via Zoom and telephone modalities. Patients and their families were educated on the use of telecare modalities as part of discharge preparation and reinforced at the time of discharge. The stroke nurses were also oriented to the modalities and had been using these even before the commencement of the study. The stroke nurses were further trained in basic troubleshooting skills. The training delivered to the stroke nurses, patients, and their families was well received. The goal was to use the Zoom platform, with the telephone modality used as a backup plan. The hospital Wi-Fi connection, which was secured, was used for the program. Appointments were scheduled at the time of discharge albeit with flexibility. An emergency contingent plan was maintained, and this comprised scheduling a physician appointment if required. Privacy was maintained by ensuring that each telecare consultation was with a designated stroke nurse only.
Recruitment
A research assistant identified the potential subjects (patients) using the Management System in the hospital and approached them at their bedside one day before they were discharged. She screened potential subjects (both patients and stroke advanced practice nurses), explained the purpose and procedures of the study, and sought their written consent once they agreed to take part in the study. The subjects were contacted by the research assistant after they had completed two monthly telecare consultations. During the two consultations, the patients received a comprehensive stroke assessment, symptom monitoring, and stroke disease management education from the advanced practice nurses as usual, but in an online mode. To ensure that the patients could use Zoom without difficulties, the nurses conducted a trial run with the patients in the clinic before holding the first online consultation. The research assistant who was involved in recruitment also trained and provided the patients with a user manual, which included information on the workflow of the study and guidance on the use of the software.
Data collection and procedure
Four semi-structured group interview sessions were conducted with nine patients, while three semi-structured interview sessions were held with four stroke advanced practice nurses due to their busy schedules in the ward and difficulty in getting together to be interviewed in a one-time slot. A focus group interview format was employed to allow the research team to understand multiple points and perspectives on the process, which are dynamically connected to its effective implementation. 29 Online sessions were conducted due to the prevailing social distancing measures that were enforced at a time when the pandemic was at its peak in Hong Kong. All interviews were conducted using a topic guide that had been developed and piloted by the research team. The interview sessions were facilitated by three researchers (AW, FW, RC) with experience and advanced training in conducting qualitative research. The guide included several open-ended questions such as: (a) What are some environmental factors that make it easier or more difficult to use telecare services? (b) How can resources or policies help to facilitate the sustained use of telecare services? The two researchers used prompts such as, ‘Can you tell me more about…?’ to solicit details from the participants. The interviews took place between July 2022 and October 2022. The interview sessions lasted from 45 to 60 min and were digitally recorded. A trained part-time research assistant, who had signed a non-disclosure agreement, transcribed the interview data verbatim. All interviews were completed in Cantonese.
Data analysis
All interviews were transcribed verbatim in the original language (Cantonese). The original transcribed files were translated to English using the Trint Automated Software. Both Cantonese and English files were reviewed by the lead author to ensure completeness. The transcribed and translated files were imported to NVivo 12 to manage the data. The data were analysed inductively using thematic analysis to discover, understand, and report patterns in the data. The paper followed the analytical steps proposed by Braun and Clarke. 30 The data were analysed using the following steps: becoming familiar with the data, generating initial codes, searching for themes, reviewing themes, and defining themes. Both Cantonese and English transcripts were analysed independently by members of the research team who were fluent in both languages. All interview transcripts were read several times to gain an initial understanding of the participants’ experiences. The authors then undertook line-by-line coding independently to formulate an initial coding frame. The coding frame was applied to two transcripts selected at random, with ongoing discussion with the team. The coding frame was refined iteratively and applied to all of the interview transcripts. Following the completion of the coding process, all codes were populated. They were reviewed and similar codes aggregated to generate subthemes. These were also reviewed iteratively with a re-reading of the transcripts, after which similar subthemes were grouped to formulate higher-order themes.
Methodological rigour/trustworthiness
Lincoln and Guba's framework for establishing rigour was used to attain trustworthiness. 31 Their framework is comprised of four constructs: credibility, confirmability, transferability, and dependability. All interviews were completed by members of the research team with advanced training in qualitative methods, which helped when probing and uncovering the participants’ experiences. Additionally, these persons were knowledgeable about the context of the study and fluent in both Cantonese and English. The process of analysing the data was undertaken in both Cantonese and English to enhance credibility, confirmability, and dependability. Once the data were analysed, participants who agreed to undergo member checking were sent a copy of the summarized results for review and asked to provide clarification or feedback on the analysis. Maintaining an audit trail and providing a detailed description of the study process were conducted to achieve transferability of the study.
Ethical considerations
The study was conducted under the standards and ethical criteria of the Helsinki declaration and approved by the ethics committee of the study university (HSEARS20211207003). All eligible subjects were assured that they had the right to refuse participation and had the full autonomy to withdraw from the study at any time without the need to give an explanation. The information provided by the participants was kept confidential and anonymous. For privacy, the name of each participant was replaced by a subject code. All the information was stored in a password-secured file, accessible only to members of the research team. The file was deleted after the completion of the study. The participants and stroke advanced practice nurses each signed a written consent form.
Results
Socio-demographic characteristics
Nine patients (females = 2) and four nurses were invited to participate, none refused or dropped out, and all completed the interviews. The interviewees ranged in age from 40 to 75 years. Eight out of nine patients suffered from ischaemic stroke and one from haemorrhagic stroke. More than half of them (n = 5) claimed that they were confident in utilizing telecare in consultations with nurses. The four nurses held the title of advanced practice nurse or above and each had more than 20 years of working experience. Table 1 provides details about the interviewees.
Demographic data of the interviewees.

*1 = not confident at all; 2 = slightly confident; 3 = somewhat confident; 4 = quite confident; 5 = very confident.
Themes and subthemes
Four themes and nine subthemes emerged from the data (see Table 2).
Themes and subthemes.
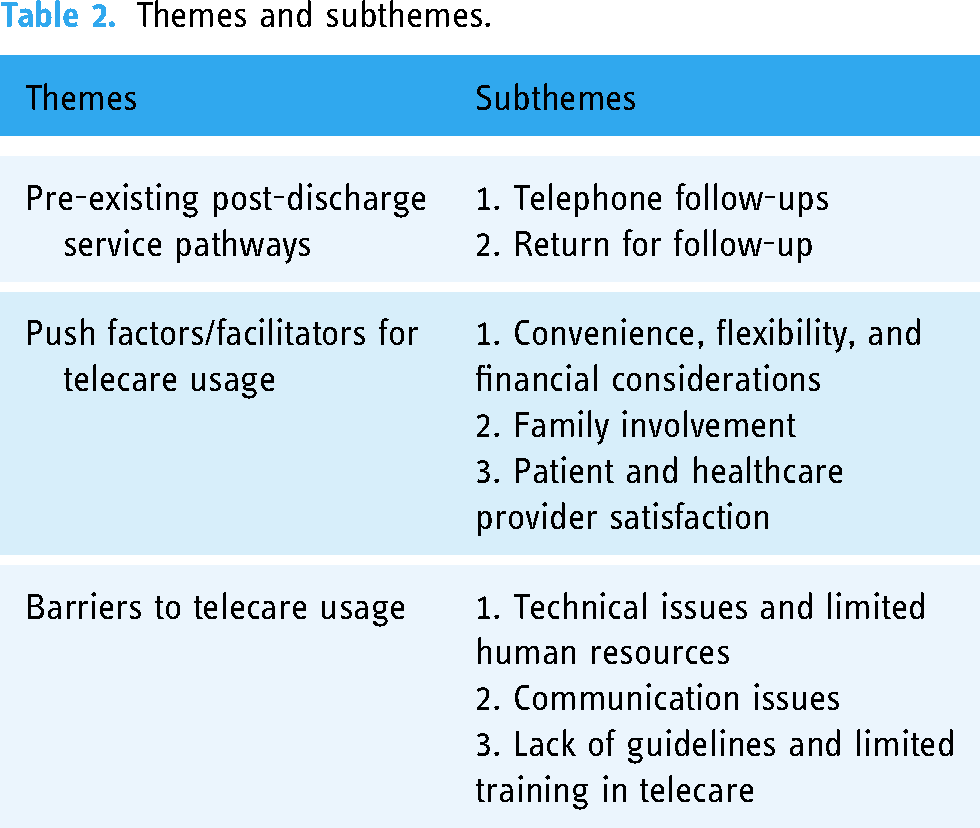
Theme 1: Pre-existing post-discharge service pathways
The theme describes the pre-existing service following discharge prior to and during the pandemic, that is, before the launching of the nurse telecare service. Two forms of service pathways were noted from the data: (a) telephone follow-up and (b) return for follow-up.
Telephone follow-up
Both healthcare providers and stroke survivors mentioned the availability of a telephone follow-up service following hospital discharge. It took the form of the healthcare providers actively reaching out to the stroke survivors following their discharge. Usually, a fixed schedule would be communicated to the patient prior to their discharge. In one instance, one patient participant noted the number that they were expected to call so as not to miss the call. The content of the telephone follow-up involved finding out about the patient's general condition, the vital signs if recorded at home, medication reminders, and reminders regarding in-person consultations in the hospital if required: Before, we used the telephone and didn't use telecare because in those days we needed the patient to come back for a visit. The patients at first would think it was strange to pay money and go back to visit the nurse. (HCP Group 2) In the past, we would not have regarded telephone calls as a visit. For stroke patients, we wouldn’t be able to determine many things about them over a telephone call. (HCP Group 2)
Return for follow-up
This form of follow-up was described as consisting of an in-person consultation with physicians in the hospital. It was observed to be for patients who were required to undergo various forms of follow-up diagnostic investigations or to see a physician: Actually, in the past, we mostly used face-to-face consultations, but because of the pandemic, we have been using telecare. But in the future, we think both can be used. (HCP Group 1)
Originally, if there had been no pandemic, our former practice was that the first, second, or even the third visit if the patient needs it, would be face-to-face. (HCP Group 2)
Theme 2: Push factors/facilitators for telecare usage
The theme describes those factors that motivated the use of telecare services from the perspectives of both healthcare providers and stroke survivors. The factors have been categorized as follows: (a) convenience, flexibility, and financial considerations; (b) family involvement; and (c) patient and healthcare provider satisfaction.
Convenience, flexibility, and financial considerations
The telecare service, although novel in the current Hong Kong healthcare system, was generally perceived by both the healthcare providers and the stroke survivors as offering a much-needed option for delivering continuous care. This was certainly the case during the pandemic when face-to-face visits were not allowed. The service was also described as being very helpful for people with mobility issues: There's lots of traffic. When someone is wheelchair bound or does not find it convenient to walk, the service is a convenience. If someone has a phone at home, we can see the patient more easily. I think that if people need to come for a follow-up, they would need to book a car, and those in a wheelchair would face lots of restrictions. Now, it would not be necessary. It would be okay for the patient to stay at home. I think those are the kinds of people who would benefit most. (HCP Group 1)
Of course, it did help me. Take people like me as an example – when I was just discharged from the hospital, my hands and feet were not good… I had trouble walking. (SS Group 2)
Although different from the face-to-face service, nurse participants felt that the video option associated with Zoom helped them to see the patient, evaluate the patient's progress as far as practically possible, scan the patient's environment, and engage with the patient and available family members. Healthcare providers reiterated that this enhanced option was unavailable in the previous telephone follow-up service. This feature was described as helpful in examining adherence to medications and observing for potential side effects: They [patients] can show their faces. Some serious problems, such as whether or not he took his blood pressure or completed the blood pressure chart can be shown by telecare. (HCP Group 1)
If, when using the video call, patients can have the drug shown directly to them as we place it in front of us, which would mean higher accuracy, so some additional information can be supplied via telecare, for example some stroke patients may have some of the medications like anti-coagulants, they may have bruises on their body, etc., so additional information, some real information, can be provided via telecare. The telephone is not that good. For example, maybe the patient complains of loss of strength, but what is the extent of the loss of strength? Sometimes the description given via the phone is not as full as what can be obtained via a video call. (HCP Group 1)
The telecare service was generally perceived as a time saver, as it was not necessary to spend time travelling to the hospital. Also, there was no need to wait a protracted time to see the doctor: This is simpler. For example, I observed that the patient had high blood pressure. We want to see progress every time, but there is no reason to ask the patient to come back only for some simple tasks like taking blood pressure. But telecare is different. I tell them to stay at home, they don’t need to come back, and they can appear every time. I think that's easier. That means that if there is a simple situation, it may easier for us to follow up, which means that time is saved. (HCP Group 1)
Normally they need to wait for an hour to see the nurses and doctors for only 15 minutes. The transportation time both ways may be up to 4–5 hours. It is exhausting for them. A face-to-face consultation may not be the best for them. In my opinion, if the telecare mode is beneficial, I hope it becomes more formal in the future so that more patients can benefit. (HCP Group 2)
Everyone has time issues. So much time is spent meeting face-to-face. So just use this service and it's okay; it's more flexible. (SS Group 4)
I don't need to travel. I am always fatigued by the long journey to see the doctor. I don’t need to go to the hospital every time. (SS Group 2)
Another aspect of convenience regarding the telecare service relates to the fact that patients can receive the service in any location as long as they have an Internet connection and can access the Zoom platform. The stroke survivors felt that they were still being cared for by the healthcare providers even at the peak of the pandemic when social distancing was in full force. Although they would have preferred a face-to-face service with the healthcare providers, they felt that they did not have any other alternative in this pandemic situation and, as such, the opportunity to receive care in the comfort of their home was a relief for them: In the past, when they come back to the clinic, they may tell us that they have nothing to do at home. If we are on Zoom, I can see how they stay at home. I can suggest that they try putting things beside them. It feels more down to earth, that we can tell them to do something in their daily life. (HCP Group 2)
They make a phone call, and I listen to the phone and talk to them. I tell them to turn on the video, everyone, press out, let's see what you are doing. (SS Group 2)
The telecare service was also considered helpful for patients who needed to continue active employment, as the service could be delivered right in their office. Despite this flexibility, both the healthcare providers and patient participants cautioned that it is possible that not all stroke survivors will survive, as survival may depend on the severity of their stroke and on the post-stroke recovery process: For those patients who cannot come by themselves, or those who need to be accompanied by their family to visit the hospital, telecare can help them. In addition, some patients need to work, and applying for sick leave for their follow-up will cause them financial trouble. But we need to be cautious about the target groups that we choose. The investigations and assessments of some patients must be done face-to-face or in the clinic, and not through telecare. Yes, they would need to come back. (HCP Group 2)
Their tongue can't turn around, they can't breathe, so if it's serious, you must call a doctor, and you must go to the A&E department. (SS Group 4)
Both healthcare providers and stroke survivors highlighted the point that the telecare service also helped to cut healthcare costs. This was observed to be associated with the fact that when patients received care at home, they did not need to travel to the hospital and pay for the services there: But I guess most patients could benefit from doing the follow-up through a video call mode. If they can use this service, we could offer them one more option. So they can save on costs, both time and money. (HCP Group 2) In fact, we can broaden our reach; even if the patient's condition is very poor, we can still reach them. On the issue of payment, it is unclear how we will deal with this later. For now it's free of charge, so all patients are very welcome. (HCP Group 3)
Family involvement
Delivering telecare also offered an opportunity to actively engage available family members in the care of their relative. Family members were involved in the technical aspects of delivering telecare, such as by assisting with setting up the Zoom call, helping to troubleshoot in the case of technical hitches, and supporting their relative during the telecare sessions: They are having lessons on Zoom. So, in the beginning, I had one of the cases in which the grandson was helping his grandparents to use the Internet, and to join this clinic. (HCP Group 2)
He is capable of using the Internet, but he cannot speak… And we are having video calls… What I mean is that we need to check the personal information of the patient. Like his name, etc. So his wife can help. Also, our clinic always encourages family members to join, so his wife will participate in the visit with him at home. (HCP Group 2)
With old age and stroke, their memory is sometimes not good. So it could be difficult for them to use this new format. It is better to have help from the family. (HCP Group 1)
In addition, family members were involved in the education sessions, to enable them to better support their relative: It is my experience that the sons and daughters… are very nice. If you make a reservation with them, they will be willing to take a day off for it. I once saw six people in the patient's family all take a day off. They came home to accompany their mother and attended the video call follow-up together. They took turns asking questions. It was heartwarming. We got to know each other's opinions, so we knew how to help their mother. (HCP Group 2)
With their permission, I will Zoom with them. Even before they go to work, or while they go to work, meeting me for 10–15 minutes can have an effect. We can reach them even if they are busy at work or have mobility issues after being discharged. The most important thing is that we will welcome all their relatives if they want. But most of the time, we want to share some information with the patients and their families. For example, the examination report on the patient's admission to the hospital. Honestly, we can only briefly talk about it. As for the family members, we can also interact with them through Zoom. (HCP Group 3)
Patient and healthcare provider satisfaction
Overall, both patients and healthcare providers expressed satisfaction with the telecare service. Although there were instances of technical or Internet challenges, they were generally satisfied that continued care could be delivered and received using the telecare service: Patients are 80% to 90% satisfied with this service. The data proves this. We review the operations of the clinic from time to time. We also review areas where we can improve. By doing an assessment, we can discover what the patients think we are not doing well and what we need to improve on. If we continue to do things in a traditional way, this would be a waste of time and would cause stress for the patient. If patients need to go to the hospital frequently, it would be very troublesome and tiring for them. Because the current clinic does not need money, there is no reason for the level of satisfaction to be low. (HCP Group 3)
Theme 3: Barriers to telecare usage
In this theme, obstacles to the use of the telecare service are described. This can provide insights into the strategies that can be employed to sustain the service over the long term. The subthemes are (a) technical issues and limited human resources; (b) communication issues; and (c) lack of guidelines and limited training in telecare.
Technical issues and limited human resources
From the perspectives of both healthcare providers and stroke survivors, it was noted that technical issues that served as barriers to telecare included challenges with joining Zoom meetings and troubleshooting. Also, some stroke survivors mentioned that their phones could not support the Zoom functionality, which made it difficult and sometimes impossible to access the telecare platform: I think we find technical problems in about 20–30% of cases because lots of older people do not have a phone that can be connected to the Internet. Actually, we already provide Wi-Fi to them, because we have the Wi-Fi egg, which they can use there, and can purchase Zoom, but sometimes they don’t have Wi-Fi at home and can’t use Zoom. In this case, these patients cannot be recruited to have video calls. (HCP Group 1)
When we go to meet the patients, the patients need some time to connect with us. Sometimes, they cannot open their microphone during calls. When they can open the microphone, they can’t switch on the camera. When they can switch on the camera, they can’t open the microphone. It takes time for them to do so. If it is you and me, we are used to video calls, we can complete everything immediately. But they need a lot of time. So, there will be support staff to assist them. Time management is also difficult. Let's say I may have a meeting at 11, but the previous meeting is still going on. (HCP Group 2)
When I had not been discharged from the hospital, the nurse asked me if I wanted to participate in the service. The nurse helped me, so I took the Wi-Fi egg. As soon as I paid the medical charges and left the hospital, they called me, but the Wi-Fi egg was not working. (SS Group 1)
Other stroke survivors found that their main challenge was Internet connectivity, which was unavailable or limited at their location: Basically his home does not have the system, or cannot connect to the Internet, so we cannot choose these cases…. A lot of families have Wi-Fi, but unfortunately, some of those living in village houses have no Wi-Fi, so we cannot provide the telecare service to them. (HCP Group 1)
If these issues persisted, the healthcare providers reverted to using telephone follow-ups to reach out to the affected patient until the issues were resolved: I have never used it. So the nurse uses video, but I don't know how to use that; therefore they sometimes give me phone calls. I talked about how I was doing. He asked me if I take my blood pressure, take my medicine on time, things like that. (SS Group 1)
Although the healthcare staff reiterated that they educated the survivors on how to use and navigate through the Zoom platform, some stroke survivors felt that they were incapable of operating the telecare virtual platform: I was able to Zoom with them once when I was in the hospital, so when the patients go home to Zoom, they just need to repeat it once. Because, for example, if they don't know how to use apps like Zoom, they won't know how to use them when they get home. (HCP Group 3)
Because of the poor reception ability of Zoom, I switched to telephone access. (SS Group 2)
As the telecare service is new and still evolving in the Hong Kong context, healthcare staff felt that more human resources need to be allocated to develop and continue to deliver the service in a timely manner and to be able to reach more patients and their families: With more manpower, we can have more time, and we can do telecare. (HCP Group 3)
Another notable challenge that emerged was the impossibility of undertaking physical examinations within the virtual telecare space, which was mentioned by both categories of participants: It would be better to have a face-to-face examination in the hospital because the doctor is there. (SS Group 1)
Communication issues
Although the participants highlighted the convenience and flexibility associated with the telecare service, the stroke survivors felt that the atmosphere associated with the face-to-face mode of follow-up was lacking. In the presence of options, the stroke survivors would still prefer the face-to-face approach as they felt that they could express themselves more in the presence of a healthcare provider. The stroke survivors said that communication issues affected how often they wished to have utilized the service. Although the stroke survivors appreciated the efforts of the telecare team, they found that the monotony of the service and the questioning hindered their continued usage of it: The nurse gave me phone calls to remind me of the follow-up from time to time, that's it. He doesn't know how to communicate well. He asked me if I take the medicine on time, I said yes. Then we had a few words. Then he occasionally makes a phone call to remind me when and where I have a follow-up. (SS Group 1)
The nurse reminds you to take your medicine, to get your blood pressure measured, to take the medicine on time, and when, what time, and where to go for the follow-up. Other than that, you don't really talk about anything else. For example, will he care about you or check how are you doing? If he asks me whether I feel better and how the consultation is going, I would say a few more words in the telecare consultation. (SS Group 3)
Lack of guidelines and limited training in telecare
The healthcare providers stated that there was a general lack of guidelines on operating a telecare service, and limited training was provided. Perhaps the sudden outbreak of the pandemic meant that there had been limited time to prepare for such a service. This implied that healthcare staff had little to no institutional guidance to support the process and had to take personal initiative to become familiar with the telecare services: In the beginning, when we were going to implement (telecare), it was quite vague, because in Hong Kong, no one has ever tried this in a nurse clinic. Even most of the doctors haven't formally done this. I know some nursing homes have tried, but the results weren't great. The efforts were also informal. Therefore, when I first started to do (telecare), I had nothing to follow. I attempted to search on the Internet, only to find things such as under what conditions we will use telecare, and the mode, but there was nothing more for me to refer to. However, the pandemic has pushed us to try many things. For example, we can't visit the patients. Our hospital has been kind enough to prepare a Zoom link for the patients, so the patients and their families can use the service at home. (HCP Group 2)
Discussion
The aim of the study was to shed light on the experiences of stroke survivors and neurology nurses regarding the use of a novel telecare service, with the goal of uncovering potential barriers and facilitators, in order to formulate strategies to sustain the long-term utilization of the program of care. The findings highlight the potential of the stroke telecare service to be an add-on program to complement ongoing face-to-face services. This is particularly important because even though the stroke survivors generally appreciated the service and reiterated the benefits associated with it, they still felt that they occasionally needed the face-to-face service and to have a real person with whom to communicate. Besides, the service might not be appropriate for people with severe deficits associated with their stroke. Overall, telecare is still in a stage of infancy stage in Hong Kong. The findings of the study point towards the desirability of integrating the telecare service in the delivery of mainstream healthcare services, and to an urgent need for guidelines and further training to enable healthcare providers deliver the program as needed.
Even before the genesis of the pandemic, the study findings suggest the utilisation of telephone modality in the study setting. This was used as a strategy to reach out to stroke survivors following discharge. Telephone follow-up remains a simple, cost-effective strategy of following up on patients to facilitate post-discharge care. Aside from stroke survivors as noted in this study, the use of telephone follow-up has been reported among frail older adults 32 and persons with osteoarthritis. 33
Although telecare services have been in existence for several decades, their use escalated following the outbreak of the COVID-19 pandemic. In the post-pandemic era, its use is predicted to escalate further to overcome healthcare disparities. 34 For stroke survivors, a recent systematic review has reported that telecare services are effective at improving their ability to carry out their activities of daily living, which warrants its inclusion in routine services, including post-discharge support. 35 In addition, existing studies have highlighted facilitators associated with sustained telecare usage such as including increased social support, the convenience of the telecare service, timeliness, faster initiation of treatment, and decreased cost.36–38 Although increased connectedness with healthcare providers has been mentioned as a potential facilitator,36,38 this was not evident in the current study. Stroke survivors in the current study still felt that something was missing, although they appreciated the efforts of the nurses in supporting them via the telecare service. The difference in the findings may be related to the fact that the telecare service emerged as an alternative during the pandemic and people may need some time to get used to the system. In fact, telecare may have been viewed as ‘foreign’ in relation to the conventional/traditional approach of face-to-face services. In this current study, the telecare service was delivered via Zoom. However, as the service expands, more state-of-the-art technology can be introduced to improve interactions between patients and healthcare providers. Moreover, in the current study, only nurses were involved in delivering the telecare. Thus, there is a need for collaboration with other healthcare providers engaged in stroke care to ensure that their services are also available via telecare. Finally, the telecare service should not replace the conventional face-to-face approach but should be considered as an add-on, with patients having the option to select which approach fits their situation, with the assistance of the healthcare providers.
An interesting finding on barriers is the lack of guidelines and limited training opportunities. Following the emergence of COVID-19 and the global trend of extending telecare services to various areas of healthcare, the Hospital Authority in Hong Kong has expanded the application of telecare services to several patient groups requiring follow-up consultations. Despite this critical move, Hong Kong, as with other parts of the world, lacks a framework to govern or guide the use of an emerging, innovative technology for delivering healthcare services. While the current Hong Kong Government advocates a broader application of telecare services in patient care, comprehensive telecare service delivery frameworks grounded in the experiences of patients and practitioners are generally lacking. This may make it challenging to develop and implement telecare services. This gap points to a critical need for more research and collaboration to establish clear guidelines and strategies to support the growth and implementation of telecare services where applicable, such as for stroke survivors.
Further to the above is a critical need to improve the communication skills of healthcare providers while delivering care in a virtual mode. Although the telecare virtual interface may appear to be like a face-to-face interaction because of the video component, it is an established fact that healthcare providers who deliver care via telecare need to have advanced communication skills to interact and understand both verbal and non-verbal cues. 39 The telecare virtual environment adds further complexities to this experience, with one study noting that patients may forget 40% to 80% of the information that was delivered. 39 This critical area therefore requires further attention, as the nature of communication can either hinder or facilitate sustained usage of the telecare service. Forgetfulness can also adversely impact patient outcomes in the long term.
Strengths and limitations
The current study presents interesting findings on the use of a stroke telecare service. A notable strength of this study was the inclusion of both healthcare providers and stroke survivors in one study, which is innovative and helped to generate nuanced, yet shared realities and can inform healthcare practice. Despite this strength, some limitations are noteworthy. First, the study included stroke survivors. Their illness and recovery trajectory may differ significantly from those with other diseases and may have caused them to experience the telecare service in a unique way. Second, the study was completed in a setting with a unique socio-cultural context and, as such, some findings may be unique to the site.
Conclusion
The use of telecare is evolving across the globe. The emerging evidence suggests that telecare is still at a stage of infancy in Hong Kong and that more work will be required to develop guidelines to underpin the development of telecare and to increase training opportunities for staff. Also, telecare services may offer a wide range of benefits and can serve as add-on services to complement existing post-discharge services.
Supplemental Material
sj-doc-1-dhj-10.1177_20552076231176163 - Supplemental material for Sustaining telecare consultations in nurse-led clinics: Perceptions of stroke patients and advanced practice nurses: A qualitative study
Supplemental material, sj-doc-1-dhj-10.1177_20552076231176163 for Sustaining telecare consultations in nurse-led clinics: Perceptions of stroke patients and advanced practice nurses: A qualitative study by Arkers Kwan Ching Wong, Jonathan Bayuo, Frances Kam Yuet Wong, Vivian Wai Yan Kwok, Danny Wah Kun Tong, Man King Kwong, Bernard Man Kam Yuen, Ching Sing Fong, Shun Tim Chan and Rinis Sin Yi Chan, Wah Chun Li in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank the nurses and stroke survivors who willingly agreed to participate in this study.
Contributorship
AKWC and FKYW conceptualised the study; AKWC and FKYW researched literature and conceived the study. AKWC, JB, VWYK, DWKT, MKK, BMKY, CSF, STC, RSYC, and WCL were involved in protocol development, gaining ethical approval, patient recruitment, data collection and data analysis. AKWC and JB wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Health and Medical Research Fund (Ref: 19200241).
Ethical approval
The ethics committee of the Hong Kong Polytechnic University approved this study (HSEARS20211207003).
Guarantor
AKCW.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.