
Abstract
Background
Virtual care has emerged as an adjunctive response to challenges in rural health care, including maternity care, and use has accelerated during the coronavirus disease 2019 (COVID-19) pandemic. This gives rise to the need for a strategic plan for post-COVID-19 virtual maternity care in rural communities. To date, no provincial initiative has focused on understanding and documenting the needs of maternity care practitioners to provide virtual care.
Methods
Qualitative study, including virtual interviews and focus groups with rural primary maternity care providers and urban and rural specialists on perceptions of the utility of virtual maternity care pre- and post-COVID-19, and benefits and barriers of virtual care. Data were thematically analysed.
Results
In total, 82 health care providers participated in the study. Health care provider responses fell into three categories: Attributes of virtual care, barriers to virtual care and system interventions needed to optimize the provision of virtual perinatal care. Participants expressed a desire for use of virtual communication tools post-COVID-19, continued ability to use fee codes for virtual care and a need for more secure texting options. The benefits of tripartite consultations were noted by many participants; impacts of the transition to virtual care included additional workload and interrupted workflow. Concerns over the lack of physical examinations and challenges in building relationships with patients when providing virtual care were frequently noted.
Conclusion
Adapting the current implementation of virtual maternity care in British Columbia may be enhanced through several provider- and evidence-derived strategies, many of which are currently underway in BC. The results from this provincial survey will be used to focus further discussion on the characteristics of an optimal system to meet patient and provider needs within a rural context.
Keywords
Author summary
During the coronavirus disease 2019 (COVID-19) pandemic, many health care providers offered virtual patient appointments. While this shift from in-person to virtual care has many benefits, it has also created challenges. This study was done to understand and document the needs, preferences, and experiences of maternity care providers using virtual care. Health care provider responses fell into three categories: Attributes of virtual care, barriers to virtual care, and system interventions needed to optimize provision of virtual perinatal care. Most participants preferred the use of phone calls over video appointments. Video virtual consultations were described as time consuming and frustrating because of technical difficulties related to poor internet or cell phone coverage, low internet speed, lack of access to equipment, and unfamiliarity with digital platforms. This may increase the workload of the care providers, impact workflow, and is not appropriately reflected in the fees that care providers can charge for such consultations. Additionally, the lack of physical examinations raised concerns about the quality of care provided because they might miss important information during virtual visits. The participants reported that a reliable internet connection, access to technological support and resources, along with real-time assistance would improve their overall experience of providing virtual care.
Introduction
Like many jurisdictions across Canada and internationally, British Columbia has seen a contraction of rural maternity services due to difficulty recruiting and retaining care providers and the centralization of specialist services in larger centres. 1 Attrition of local services has led to adverse health outcomes2,3 and psycho-social costs for birthers and their families 4 as well as unintended consequences for communities. 5 Primary maternity care is offered by registered midwives and physicians in British Columbia, sometimes through a collaborative practice model. Specialist back-up is available in some larger communities or in associated regional referral centres, although in many communities caesarean section is offered by Family Physicians with Enhanced Surgical Skills (ESS). 6 The availability of local care, with or without ESS, is essential in communities with enough procedural volume to support this care due to inclement weather and challenging geography that often makes transfer to other care centres challenging.
When a patient requires complex care that exceeds the scope of primary care practitioners, however, referral or transfer is the only option. In obstetrics, this means that birthers with ‘high risk’ pregnancies must travel to the nearest specialist centre to receive care, even for non-emergent situations. In some instances, patients are unable or choose not to travel due to a combination of financial and/or family constraints or due to significant challenges associated with remote geographical locations. A solution to enhancing access to specialist care for rural and remote populations has been the development, refinement and implementation of virtual care strategies. ‘Virtual care’ broadly refers to ways in which health care providers can remotely interact with patients – or other providers – through the use of telephone, text messaging, or video communication.
As an early contributor to virtual maternity care in BC, the Mobile Maternity Care project (MOM) was funded by the Specialist Services Committee in 2015 as a proof of concept to assess the efficacy of linking primary maternity care providers with a regional obstetrical specialist for urgent and routine consultative support at a distance. This connection allowed for improved shared care of high-risk pregnancies to reduce patient travel to see a specialist It was also available as a ‘safety net’ for precipitous deliveries in communities without supportive local resources and facilitated real-time educational opportunities between specialists and primary care providers through direct consult for clinical conditions. Most importantly, the MOM project pioneered a system for tri-partite visits, i.e., clinical encounters that included the specialist, the local primary care provider and the birther and family.
As antenatal health care in many jurisdictions is retaining the COVID-inspired shift to virtual care, emerging research is addressing the experience of patients receiving such care.7–9 However, there has been a gap in understanding the experience and preferences of antenatal care providers. These data are best suited to a qualitative research design due to the lack of existing data on the topic and to capture the nuances of experience. This paper is a tentative first step in consolidating this essential evidence to inform further health system planning.
Background
Recently, necessity has spurred the diffusion of antenatal virtual care in the context of COVID-19. Health Canada (2021) notes that since COVID-19, ‘adoption of virtual care has dramatically increased with approximately 86% of BC patients connecting with a physician virtually (phone, video, email, etc.) between April and September 2020 alone’. 10 A Canadian survey conducted pre-COVID showed 41% of Canadian residents wanted the option of video consultations with their physicians, yet only 4% of family doctors offered this option. 11 The rapid move to virtual care occurred in a setting not well equipped for such a transition. While Canada was an early adopter of virtual care via telephone in remote regions of the country in the 1970's, other countries have surpassed Canada in terms of the planned expansion of virtual care. Australia, France and England released digital health transformation strategies in 2018, including access to ‘digital first’ primary care options within 5 years (in England) and improved access to virtual healthcare options among rural and remote dwelling patients in Australia. 11
As with all health care transformation, improved patient experience remains the north star, and international evidence suggests high levels of satisfaction both with the quality of virtual care appointments and the attendant reduction in the need for travel with all of the associated actual and social costs.11,12 This has led to increased follow-up with specialists where otherwise such care would not be sought. 7 However, there has been scant evidence regarding the preferences of care providers in Canada, a key element of the Institute for Health Care Improvements’ Quadruple Aim. 13
Hofman et al. 14 surveyed physicians, nurse-practitioners, and midwives in Colorado to assess the feasibility of barriers to virtual maternity care. Data were collected twice during the early months of COVID-19, three months apart. The feasibility of using telehealth to provide perinatal care was perceived as very high: 94% of participants deemed it feasible at baseline and 92% at follow-up. Virtual postpartum care was deemed more appropriate than virtual prenatal care. The most commonly reported barriers to provision of virtual maternity care at baseline and follow-up were: patient and provider lack of access to essential tools for virtual care, inadequate clinic support, patients preferring in-person visits, poor image/sound quality, quality of care not as good as in-person visits, inadequate training and IT support and reimbursement/financial concerns. 14
Flaherty et al. published a qualitative evidence synthesis of 48 studies across 14 countries describing the experiences of maternity care providers and childbearing people during COVID-19. None of the studies described the experiences of Canadian providers. The synthesis revealed five themes reflecting women's experiences and three themes describing maternity care providers’ experiences, including the following: Altered care structure and provision, professional and personal impact, and broader structural impacts. Care providers described how the move to telehealth required them to be adaptive and innovative and how they often felt abandoned by management because changes in protocols were not communicated well and their needs were not considered. The personal impact of increased workloads because of staff shortages and new care practices was a prominent subtheme. Care providers in some of the included studies described that the chaos and uncertainty during the pandemic strengthened relationships between team members. In some settings the opposite was observed, i.e., interprofessional relationships between midwives and doctors worsened. While maternity care providers mostly described the negative impact of COVID on maternity care provision, some saw it as an opportunity to effect positive change, including expansion of virtual care options and enhanced access to care for under-served groups of childbearing people. 15
Current context of virtual care: the influence of the COVID-19 pandemic
This investigation into care providers experiences with the use of virtual modalities to support rural maternity care occurred during the second wave of COVID-19. During this time, health care providers were conducting most clinical visits virtually as per public health guidelines. Maternity care providers were guided by the (changing) best available evidence for in-person prenatal visits which set minimum targets for in-person visits but, as summarized by the BC Centre for Disease Control, emphasized ‘where appropriate Virtual visits (instead of in-person visits) should continue, to minimize the chance of exposure to COVID-19’. 16 Given this context, we also asked participants in this study which tools they adopted directly due to COVID-19, whether this altered their communication with patients and other providers and which virtual practices they intended to maintain post-pandemic.
The goal of this study was to understand and document the virtual care needs, preferences and experiences of specialist and primary rural maternity care providers in British Columbia.
Specifically, we set out to (a) understand health care providers’ perspectives and experiences with virtual maternity care (rural general practitioners, midwives and obstetricians) and the utility of virtual tripartite visits; (b) identify barriers and challenges of providing virtual maternity care in BC; (c) outline systems level needs desired by rural providers for virtual maternity care in BC and (4) provide recommendations to guide the implementation of virtual maternity care post-COVID. Findings from this study are transferable to rural communities in other high-income countries.
Methods
Definition of virtual care
Virtual care has been defined as any interaction between patients and/or their social supports, ‘occurring remotely, using any forms of communication or information technologies with the aim of facilitating or maximizing the quality and effectiveness of patient care’. 17 For the purpose of this study, virtual care means patient care consults by video conferencing, digital communications between team members and/or patients such as text messaging email, and video consults between providers.
Theoretical orientation
The project was grounded in the recognized importance of partnerships in affecting health system change through the inclusion of key stakeholder groups as described in Charles Boelen's paper, 18 “Challenges and Opportunities for Partnership in Health Development”. In this work for the World Health Organization, he described the “Partnership Pentagon” that underscores health system transformation. The partners include policy-makers, health professionals, academic institutions, communities, and health managers (see figure 1, below), each with discrete frames of reference, strengths and insights.

Partnership pentagon 18 .
Ironically, in the rapid proliferation of virtual health care due to COVID-19, the voices of care providers have been notably absent from many discussions on models of care despite their recognized ‘indispensable’ contributions. 18 This primary research sought to capture these experiences, embedded in practice ‘at the coal face’, recognizing the importance of both lived experience in health care design and of the synergistic benefit of multiple viewpoints. Core values underscoring this work include inclusivity and recognition of the necessity of divergent experiences.
The methodological approach of in-depth, open-ended interviews and focus groups and thematic coding were used to reflect both the pragmatic nature of the project and the need for practical outputs for care providers and policy-makers: we were not developing theory as much as capturing and cataloguing experiences.
Recruitment
We invited all self-determined rural primary care providers (Family Physicians and Midwives) and rural and urban specialist Obstetricians and sub-specialist Maternal-fetal medicine providers who practiced in BC to participate. Invitations to participate were sent through care provider-focused list serves and newsletters with a provincial reach including through UBC's Department of Family Practice, the Midwives Association of BC and Divisions of Family Practice/Doctors of BC.
Data collection
Data was collected via 11 virtual focus groups and 6 interviews (n = 82) between April and July 2021. Focus groups ranged in size from 3 to 8 people; data was only collected once from each participant. Semi-structured interviews and focus groups, based on key themes from existing literature, were all held over Zoom to abide by public health guidelines and reduce the transmission of COVID-19. Each took between 45 and 90 min with the average time being approximately 60 min. With participants’ permission, all focus groups and interviews were audio recorded and transcribed verbatim for accuracy in analysis. Typed interview notes were also taken by the project research assistant to capture any non-verbal cues. Interviews were continued post-data saturation to honour commitments to participants who volunteered to participate. The transcripts were quality checked by one research assistant to ensure digital accuracy. The interview questions covered demographics, perceptions and utility of virtual maternity care pre- and post-COVID-19, benefits and barriers of virtual care, and the utility of virtual tripartite visits. See Appendix 1 for the complete interview guide.
Analysis
The data collected from the interviews and focus groups was analysed using a thematic analysis framework outlined by Braun and Clarke. 19 The principal investigator and research assistant engaged in-depth reading of the transcripts and made notes of preliminary codes, derived from the data. A codebook was independently developed by both to organize the initial codes and ensure consistency in interpretation. When compared, there was a high level of congruency between the code books. Qualitative data analytic software, Nvivo, 20 was used to sort the transcripts and related codes were grouped together into themes. The themes were then reviewed, defined, and written up. Ethics approval was granted by the University of British Columbia's Behavioural Research Ethics Board. This study was approved by the Behavioral Research Ethics Board, University of British Columbia (H15-03048).
Research team reflexivity
The primary author (JK) conducted the interviews. As an Associate Professor (PhD) in the Department of Family Practice and co-Director of the Centre for Rural Health Research, she built on 20 years of primary research including the development of metrics to determine appropriate levels of care to meet population level need for services and system interventions to sustain such services. Through previous work, she has gained a deep understanding of the conditions of rural practice. As a result of this work, the principle investigator established many connections with care providers across rural BC and involvement in this study was part of a longitudinal commitment to develop rigorous evidence for rural health planning. Other members of the research team were likewise engaged longitudinally in rural healthcare, two as specialist obstetrical care providers (SM and RJ) and one as a project manager for a diversity of project grants (MM). Where there was the potential for a conflict of interest (e.g., interviews with primary care providers who refer to one of the project team specialists), the affected team member would not participate in the interviews.
Results
Analysis of focus group and interview transcripts revealed three overarching themes: Attributes of Virtual Care, Barriers to Virtual Care and Systems Interventions needed to optimize the provision of virtual perinatal care, each with subthemes. Each theme is explicated below and summarized in Figure 2.
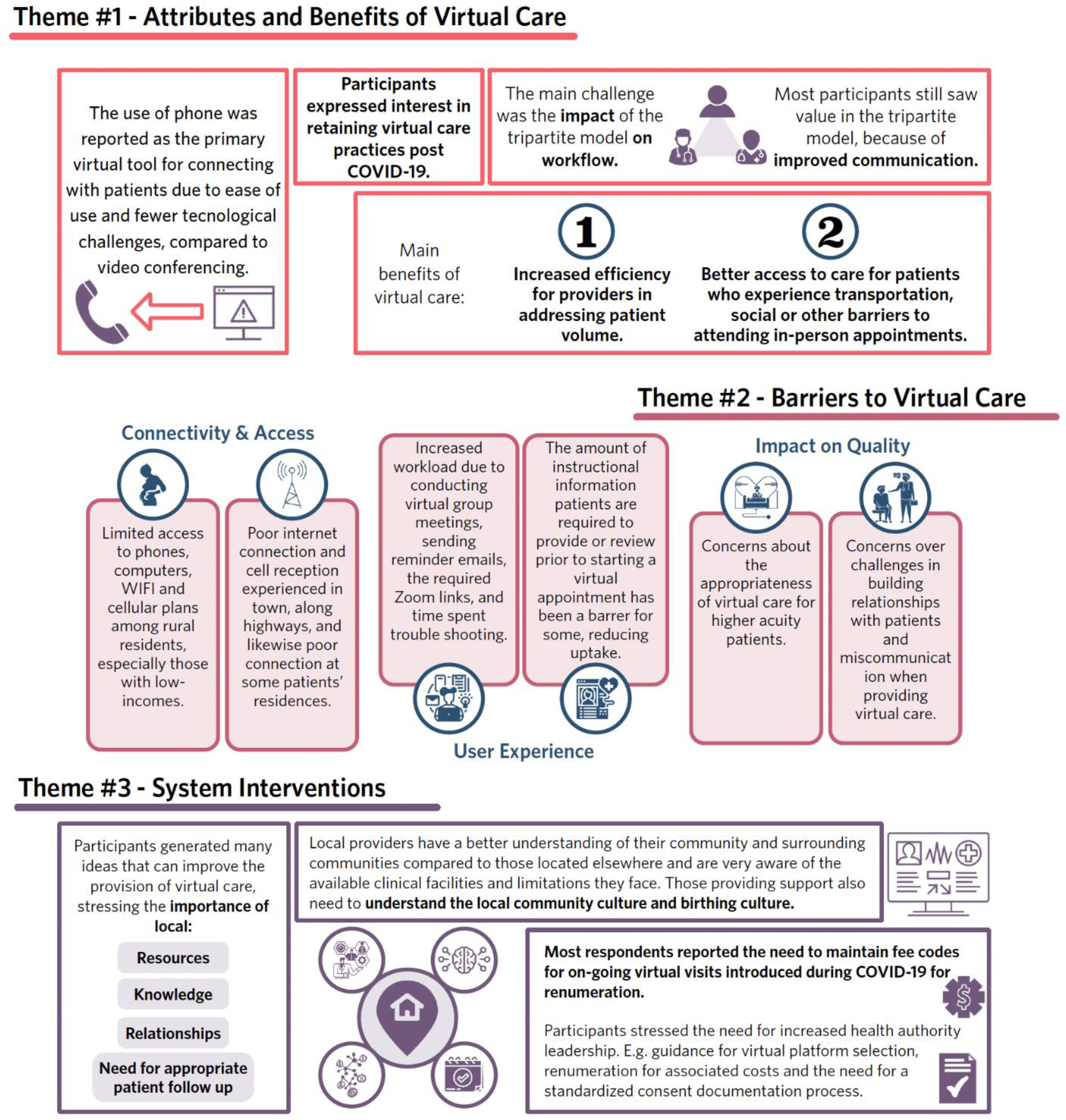
Summary of main themes.
Theme 1 – attributes of virtual care
Usage
The use of the phone was reported as the primary virtual tool for connecting with patients due to its ease of use and fewer technological challenges, compared to video conferencing. Texting was common but respondents expressed concerns with security and setting personal boundaries. Several participants reported the value of combined phone – in-person visits allowing them to achieve ‘a bit of a balance’. In-person visits were seen as important to assess the fetal heart rate, weight, and other ‘hands on’ aspects of care, but many found it to be ‘quite reasonable, to do telehealth [phone] for every second visit or so…’ (OB_28). Another participant commented that they utilized the phone for counselling related to breach or VBAC but their patients would attend an appointment in-person to confirm BMI or weight distributions prior to a procedure (OB_28). Despite the clear value of telephone visits, however, most participants stressed preferring in-person visits in the antenatal period (‘there's just certain aspects of physical care that can't be replaced over the video or telephone’). This was due mostly to the tactile advantage of the physical exam in pregnancy: I really like to look at the belly and I like to lay hands on the belly, I’m a very tactile and visual kind of doctor, so I always do my Leopold's and my hands on the belly and I estimate fetal weights and you know, I look at people's faces to see if they’re puffy or they’re getting pre-eclampsia and I can see it before the blood pressure goes up, so you can get some of that over tele-health because I do have tele-health but it's, I mean medicine is all the senses right? Like we use all our sense and so when you take away one or two of my senses, I’ll do the best I can and it's really hard to compensate for that, but it's not the same as having all our tools in our toolbox. (OB_16).
When connecting with other health care providers, participants expressed a preference for speaking on the phone or, more commonly, texting due to the convenience of asynchronous communication. Although some participants expressed concerns about the lack of secure texting, many noted that secure options were too challenging to use.
Tripartite model
A tripartite clinical consultation involves the family physician or midwife in addition to the patient and specialist. When discussing attributes of virtual care, participants often mentioned the tripartite model and attendant improved communication between all parties, due to reduced reliance on patient recall. Participants in this study also noted the value they provided in the tripartite visit by translating technical information. One participant noted that this model allows all care team members to ‘validate care plans’, be on the same page, and reduce the potential for misunderstandings. (PCP_10).
One specialist participant mentioned that it is particularly helpful to have three-way conversations for complicated cases as ‘the patient doesn't have to remember what you say and go back and talk to the other one, we can just put everyone in the same virtual room’. (OB_19). Another participant noted their concerns about how information was discussed with a specialist: …you send them to see the OB with these concerns and then the OB said no, no this is fine and you almost wonder did they talk about that? Did that come up? Like how clear was the consult? So, it can be really frustrating when it's things like you know, consenting for trial of labour after caesarean or they have these comorbidities or other things are going on. Did they really get into that?… (PCP_06).
Challenges and solutions to achieving tripartite care
The main challenge to tripartite care was the impact on workflow, namely scheduling challenges and the logistics of coordinating two providers and a patient. Some participants were not convinced that the efforts would be worthwhile. Other participants acknowledged the scheduling issues but still considered it a valuable endeavour: ‘guaranteed it's going to be a headache, [but] there are just some things that are worth it.’ (PCP_21).
Participants also reported that tripartite care would improve communication between care providers by reducing the need to contact other providers directly or endure a potentially long wait to receive a formal consultation letter. One participant stated that it would ‘remove a step’ of reaching out to a provider after seeing a patient as they ‘can all just talk together’. (OB_22). Other participants noted that they ‘might not get a consult [letter] for days’ (PCP_17) and the wait for recommendations can delay when action can be taken.
As the tripartite model facilitates providers with varied levels of training and experience to attend an appointment at the same time, many reported another benefit being the opportunity to learn from one another as well as be supported and reassured by their colleagues. One participant commented that they ‘learn so much’ and that a specialist offering ‘clear and explicit direction’ would make them ‘feel more comfortable in providing care’ (PCP_11). Another participant mentioned the value of the primary care provider being involved because ‘you can reinforce what was discussed or clarify anything that is unclear’ (PCP_18).
Benefits of virtual care for patients
Participants were asked about the benefits of virtual care for their patients and resoundingly noted a reduction in travel and increased access to care. Namely, virtual care increased access to patients who may not come into a clinic due either to geographic or social reasons and enabled providers to connect with patients’ in-between appointments if needed. As one participant noted, ‘[it is] very helpful for patients who have difficulty accessing transportation or [who] have mobility issues’. Convenience was also highlighted by participants who noted patients could attend visits during their workday or during their lunch hour. Another participant commented that the expectations for travel on rural patients are often unfair: ‘it seems cruel that someone has to come to me and … drive however many hours and sit for half an hour in my waiting room and I spend like 20 min with them …’ (OB_16). Due to the counselling aspects of their work and understanding that in-person appointments can be a barrier, one participant echoed previous comments that virtual care offers greater “accessibility”, to the point that “people can do it [take a phone call] when they’re driving home from work…”.
Benefits of virtual care for providers
The main benefit of virtual care for participants in this study was increased efficiency in addressing patient volume, which resulted in better waitlist management and using scheduling gaps to advantage. As one participant said, I think the main benefit that I’ve found is, because we always try to judge and keep our wait lists across different communities more or less equal, now if I see I fall behind in [one town], I just book an extra virtual day. If the OR is cancelled, I can leverage that time to do an outreach clinic and do a bunch of consults, decide who I need to see in person … (OB_25)
Many participants also noted the benefit of being able to fit appointments into gaps in their schedule: … if you have a free day or a free morning … it is really expeditious and effective to book a day of consults over the phone and that can be really very very helpful and useful. Having the flexibility to do that is brilliant, especially doing what we do because there's so many variables all the time (OB_25).
Other participants described attending virtual appointments specifically during labour or between operative procedures ([I]‘can just go to a back room and do a couple phone calls’). This was generally facilitated at a scheduling level by maintaining a list of patients amenable to unscheduled appointments, allowing them to ‘hit the list’ when time permits. Most mentioned that unscheduled visits cannot be done for in-person appointments due to travel time logistics and that ‘if you have to change [an in-person visit] it's an absolute disaster in the office’. The same participant noted that when changes in the schedule do occur the ‘consequences of changes are much less’ as patients did not have to travel or take time off work in order to attend the appointment.
Retention of virtual tools post-COVID-19
Some respondents expressed a desire to maintain the (increased) use of phone, texting and video for connecting with patients post-COVID. One respondent stated: I think there's a place for it, especially for patients that can't come to your office because they live remotely and access to specialist care is a barrier for them. I think there certainly is a place for telehealth and virtual visits because of its ease and its flexibility for a lot of patients in my perspective and I think I would probably continue adapting it into my practice (OB_29).
Other participants commented that they would also continue to use virtual tools as long as appropriate billing of the service was maintained. One respondent stated that post-COVID-19, their preference ‘would be to use video for new consults with patients rather than telephone’ (OB_07), while another respondent stated that they would likely run their practice with ‘at least half virtual, [and] half in-person’ (OB_25).
A minority of participants in this study expressed a lack of desire to continue to use virtual care post-COVID-19.
Theme 2 – barriers to virtual care/challenges with virtual care
Participants described several barriers to provision of virtual care. Logistical barriers fell into two main categories: Connectivity and access and user experience.
Connectivity and access
Participants described patient challenges, provider challenges and infrastructure challenges to connectivity and access. Common challenges included limited access to devices (e.g., phones or computers) as well as inconsistent access or lack of phone minutes, WIFI access, and cellular plans. These challenges are exacerbated among rural low-income patients.
Provider challenges described included issues with a poor internet connection, which lead to changes in how providers conduct virtual care. For many, unreliable internet required switching to phone calls during video calls to ensure consistency with the quality of communication. Some participants noted that they altered their workflows to avoid high internet traffic times. The reliance on older forms of technology was also noted by one respondent who mentioned their use of pagers: Midwives, we still carry a pager. I’m not kidding because there are places even within [our town] where if someone was calling a phone, say we had a cell phone that was specific for the person on call they wouldn't get through. So those little analog pagers work 99 percent of the time. Versus about 87 to 90 percent of the time with a cell that would be designated as the on-call cell (PCP_04).
User experience
Participants discussed various challenges with workflow and the time required to deliver virtual care, including issues with the set-up or facilitation of the virtual appointment, along with audio or visual problems. Some described time wasted trouble-shooting, causing delays in workflow and issues with maintaining set appointment times.
Another barrier noted was the increase in workload due to virtual care, specifically the extra time and work required in order to conduct virtual group meetings and send reminder emails, zoom links and information hand-outs to those attending. Many participants noted that the shift to virtual care came about quickly and with limited support during the COVID-19 pandemic, placing technical demand on providers as well as increasing the overall number of daily tasks.
Patient information
Several respondents also highlighted that the amount of instructional information patients are required to provide or review prior to starting a virtual appointment has been a barrier for some. One respondent noted ‘70% of patients couldn't get on’ one popular platform and that the overall process was ‘really cumbersome’ (OB_16). Another respondent expressed apprehension at the need to read through ‘ten pages of instructions’ and the lack of willingness for most patients to do this.
Virtual care challenges
Although virtual care was viewed by most participants in this study as enhancing patient care, concerns such as the implications of the lack of physical exam, changes to the patient-provider dynamic and the inefficiency of virtual care when higher acuity care is needed were noted.
Several participants noted that in obstetrical care particularly, the lack of in-person contact was problematic: ‘…to diagnose and understand women in their overall health and well-being I need to see them … I need to see how they walk in the door, how they sit down, how they look at me … this is very important’ (PCP_06). Specialist participants expressed concern that some primary care providers had not physically seen patients prior to them being in their care, one stating, ‘primary care practitioners have been saying, “I haven't actually seen this patient, can you examine them?” Which I find a bit problematic with virtual care’ (OB_14). As one participant summarily noted, ‘so much of medicine is still… hands-on; you need to have that art of medicine and we can replace some of it with technology but I don't think that any of us will say that it's better care without seeing people’. (OB_28).
Virtual triage
Although ‘efficiency’ was noted as an overall benefit of virtual care by most participants, many also reported inefficiencies due to duplicating virtual visits with in-person visit when a physical exam was necessary. As one participant noted,’[some days there are] four or five people that you’re re-booking next day or you’re bringing in that afternoon because you actually do have to see them physically in person, not just on Zoom’ (PCP_06). Concerns regarding inefficiency as well as the overall appropriateness of virtual care options for certain patients gave rise to the need for increased adeptness with triage for in-person appointments. Illustratively, one participant commented that it has been ‘tricky to know who needs to be seen in person and who can be seen virtually’ and that they think that things are being missed. Some participants described techniques they used in triage including reviewing clinic visit schedules in advance, noting reasons for the visit and then evaluating whether or not a phone call would be appropriate. Others conveyed pre-appointment assessments with patients themselves. One participant noted: …now I’m just adding in that filter of ‘is that likely to be appropriate for a phone visit and I might get my staff to call them and just say no, you should come in’, or I might call them myself quickly and just say I just want to make sure that we’re using this time properly, let me ask you a couple questions and then we might change it to in person or vice versa (PCP_06).
Patient-provider dynamics
Many participants commented on both positive and negative patient-provider dynamics due to the use of virtual care. Negative impressions included a lack of prioritization of the virtual visit, feelings of reduced patient connection, and misinterpretations of information provided. Positive aspects included increased levels of connection and comfort for patients, opportunities for teaching, and the potential of ‘seeing’ more of a patient's life than before.
Specifically, although virtual tools have contributed to increased accessibility for patients to attend appointments or receive follow-up communication from wherever they are located and at various times throughout the day, participants reported that this has led to increased multitasking and diminished focus from patients during virtual visits. One participant commented that, in their experience, ‘patients don't have as much respect for our time, they don't really pay attention, they’re busy with a screaming toddler in the background, they make no effort to dedicate themselves to the appointment’. (OB_12). Another participant echoed the concern, noting ‘they’re just squeezing it into their day’ and felt it was hard to know if the information being provided is ‘registering at all’ (PCP_23). Some patients’ more ‘casual’ approach to virtual appointments may not be ideal but one participant noted that there is a ‘learning curve’ and that patients will have to adjust ‘if they can't hear what the doctor is saying, its's them losing out on care. They have to do their due diligence as well, so I think we’ll all get better at managing it’. (OB_25).
Lack of connection was also a concern, as one noted, ‘we’re really missing that kind of connection with the clients and not feeling like it's the same level of care or level of knowing each other’. (PCP_23). Another participant echoed this sentiment by stating that not being in the same room as someone impacts the ability ‘for building trust and for really establishing that connection’. There were also concerns about privacy with some participants noting they are usually unaware if a patient is alone or in a safe space, which can make it difficult to assesses intimate partner violence.
Theme 3- systems interventions
Participants in this study suggested many ways to improve virtual care, stressing the importance of local resources, knowledge, and relationships and the need for appropriate patient follow-up. There was consensus that visits with regional or local care providers are favoured over visits with providers in distant, larger urban centres, however, the latter would be helpful for more general advice. Participants felt local providers have a better understanding of their community and practice context compared to those located elsewhere and are better able to understand the community and birthing culture.
Other respondents noted that unless the case they are managing is complicated and in need of sub-specialist care, contact with regional providers would be best as it increases ‘inter-professional relationships in your sort of core local group’ (PCP_17). The most productive relationships were underscored by a sense of trust that comes from shoulder-to-shoulder work on the part of both specialists and generalists. As one participant noted: … I think in general, it's way easier to like trust the specialist … that they’re hearing you and that they understand the geography that plays into the decision making, … especially around like ‘do we need to transfer this patient?’, when they’re your home specialist … I think I would way rather like [to] have a relationship [with a regional specialist], have a sense of how things are going to go, know that they know where I am, and where we’re talking about this patient ending up. (PCP_27).
Fee code adaptation
Most respondents reported the need to maintain fee codes introduced during COVID-19 for remuneration for ongoing virtual visits. As one said, … the billing codes need to stay and not be taken away because you can't spend your time doing consults if you’re not going to get paid for them … I think if they want us to do that kind of thing [virtual care] then the codes have to stay… (OB_05).
Almost all respondents noted this was essential if the virtual health care gains achieved during COVID-19 were to remain post-pandemic. However, some respondents critiqued the current payment structures for virtual visits, one noting, ‘[remuneration for] virtual maternity care is paid, for family practice, significantly less than any other virtual visit for any other segments of the population’. They added that pay structures need to be more comprehensive: ‘these aren't simply maternity visits, they’re also counselling visits, infectious disease lessons, and sometimes you have grandma on the line too, and dad and all those things’. (PCP_04). Exacerbating the increased load of individual calls, a few participants noted an increase in seemingly trivial patient calls due to easy availability: … people call me for the silliest stuff now, that they never would’ve called me before and they never would’ve come in [for], and now they have access to me and I think the billing codes are going to have to change, or something's going to happen here because I don't see how the government can sustain paying us for these visits that are really you know [are] not whole visits …. from a governmental health systems perspective, I think that's just silly (PCP_24).
Health authority leadership
A few respondents noted the need for increased health authority leadership to navigate changing and challenging virtual care modalities, specifically, guidance for platform selection, remuneration for associated costs and the need for a standardized consent documentation process. Many participants pointed to the underutilization of secure messaging services and attributed this to a lack of system-level promotion and education. Others appealed to the need for guidelines on handling patient complaints arising in the virtual encounter and clearer guidance on what platforms are acceptable. Funding support for the use of virtual care platforms like Zoom was reported to be limited, particularly for midwives, and one respondent noted that free Zoom accounts only allow for a maximum 40-min call and the providers must pay for accounts that offer more features: if we’re doing like other meetings or different things, we’re still paying for our Zoom account, right? And so, you know like again it's kind of money and time off our backs that we don't get compensated for which is just starting to get old, personally. (PCP_18).
Networks of virtual care
Many participants in this study recognized the value of virtual technologies in facilitating administrative and clinical relationships with colleagues in other communities.
Respondents noted that the use of virtual platforms would help connect providers that are geographically far apart and increase provider awareness of regional services and support. Many participants felt that the expansion of a virtual infrastructure for connectivity, in addition to clinical support, would enable more participation in administrative and social events for rural providers. Most participants valued the idea of peer support, one person noting that ‘sometimes people take their frustrations out on this e-mail group and it ends up being … a horrible way to let out your woes. I think it would be really good to have some access to actual care, as opposed to ranting on a group e-mail’. (PCP_18). Another respondent noted that a ‘mentorship component would be great’ to help develop connections with more senior colleagues (PCP_11).
Required supports
Respondents were encouraged to describe the support that would help them practice rural obstetrics and optimize delivery of virtual care. This ‘blue sky’ discussion resulted in various recommendations described below (see Table 1). Systems level suggestions included more support for midwives, health stations in the community for participating in virtual appointments and increased access to virtual reproductive mental health services. Specific recommendations included having everything integrated to the Electronic Medical Record – EMR (video, phone, resources, etc.), and implementing one provincial EMR. Ideally, the EMR would be embedded within a single health platform that everyone is using and provides province wide access to information.
Supports and strategies to optimize rural obstetric practice, described by participants

Discussion
Participants in the current study described several barriers to provision of perinatal virtual care, including lack of wireless infrastructure and lack of access to reliable connectivity in many rural communities. Some participants reported modest improvements in rural connectivity due to COVID-19 but many noted that some patient populations lack access to technology and infrastructure due to costs. Texting was seen as a common solution in low-income communities. Other researchers who interviewed patients about their experiences with using virtual health services during COVID 19 found similar themes. In one interview study with 74 vulnerable patients in Finland (older adults, migrants, the unemployed, users of mental health services and those using health services frequently) patients voiced concerns over the security of digital platforms and reported problems accessing digital health services (because of insufficient computer skills or lack of identification documents needed to access virtual care platforms). Patients often found virtual appointments impersonal, and reported more misunderstandings during virtual care encounters, compared to in-person visits. 21 Researchers recommended several strategies to enhance digital health equity, including different remote options for different patient populations, plain language instructions, targeted advertising about virtual care services so more vulnerable populations are aware of this option, and access to secure and private spaces in public facilities (like libraries) where patients can use digital health services. 21
Health care providers in the current study described how virtual care benefited patients but also noted how it affected the quality of care and challenges with providing person-centred care (because of lack of physical examinations and care provider inability to see the whole person). A qualitative evidence synthesis of 48 articles describing the experiences of childbearing people and maternity care providers during COVID supports these findings. Childbearing people described similar benefits of Telehealth as respondents in the current study: Avoidance of long waiting times at clinics, reduced need to travel for antenatal or postnatal appointments, having appointments in the comfort of their homes and not being exposed to COVID-19 infection. Similar to health care providers in the current study, childbearing people noted that it was difficult to establish rapport with maternity providers during virtual appointments. 15
Other jurisdictions have attempted to solve this problem by implementing technology-supported, person-centred health care strategies, operating from the assumption that technology can aid the provision of person-centred care (PCC). For example, in western Norway virtual PCC for COPD patients was implemented to enable patients to receive care in their homes rather than having to travel for follow-up appointments. This telemedicine initiative included remote monitoring of COPD indicators and daily videoconferencing with patients for 2 weeks after hospital discharge, to support self-management at home. The programme is led by nurses, but also included a physiotherapist, occupational therapist and nutritionist 22
A recent scoping review about how to implement telemedicine services showed that successful implementation requires significant organizational and practice change. 23 Several change management (CM) strategies can support the implementation of virtual care, including assessment of organizational/clinic readiness, and the needs of providers and patients so this can be taken into account when designing the virtual care service. Other CM strategies include gaining leadership support, identifying champions and engaging key stakeholder, to design and plan telemedicine services. It is also important to articulate a simple but clear vision for how the virtual service will operate, ensure adequate resources, seek buy in, coordinate roles, provide education and training, develop new work processes and protocols, and monitor and evaluate change while maintaining flexibility. 23
Rural and remote health care includes, by definition, lower procedural volume due to lower population densities. This creates challenges for sustainable specialist practice, particularly for services that require continuous availability and a robust call rota of providers. Within this context, the planning imperative to centralize highly specialized care is reasonable; it is more difficult, however, to plan specialist care in a way that creates a balance between meeting local population needs and provider sustainability. This tension was clearly identified by participants through their discussion of the preference for regional or provincially centralized virtual consultation.
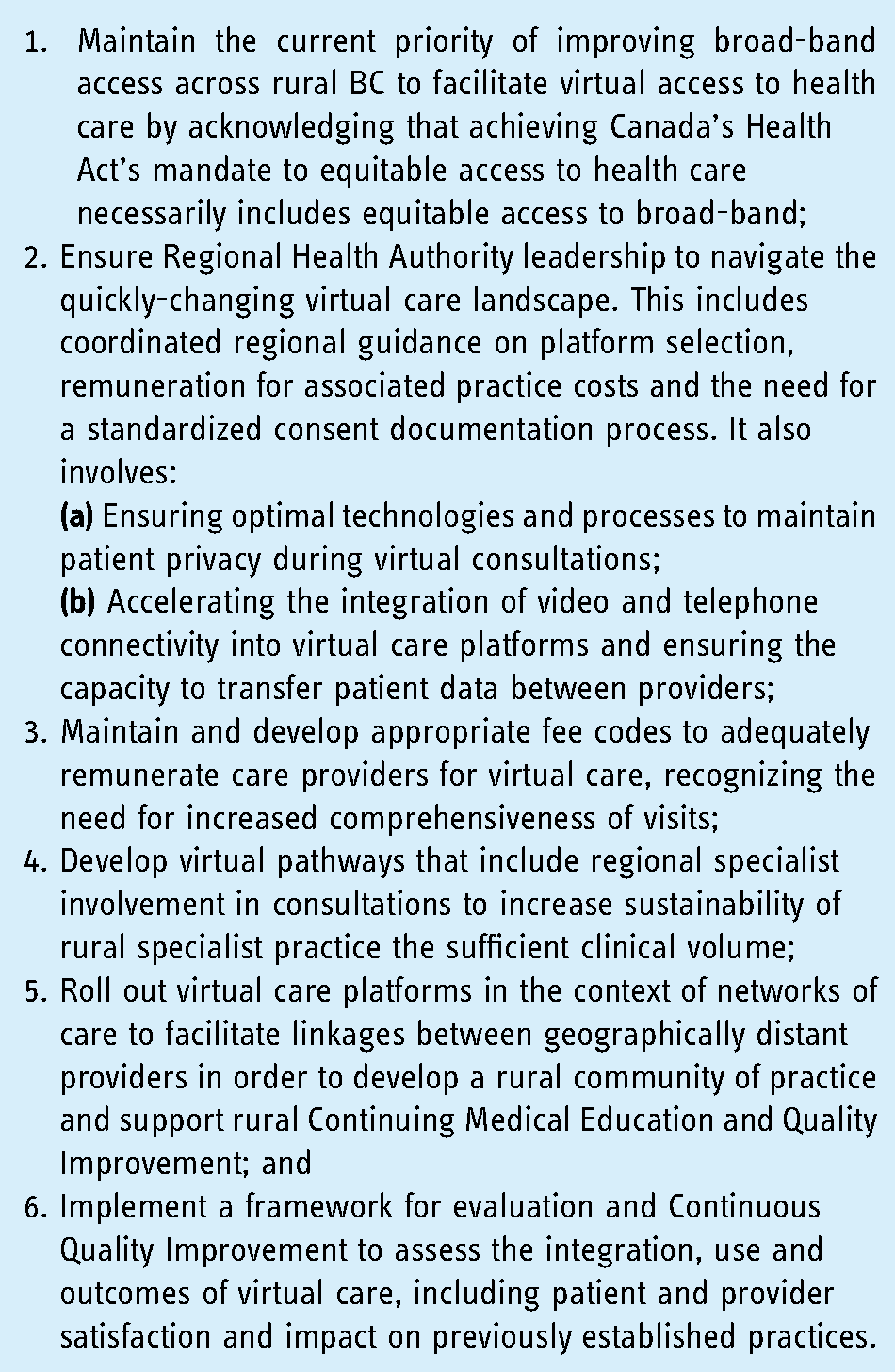
Based on results from this qualitative study, we identified several system enablers of virtual care. Adapting the current implementation of virtual maternity care in British Columbia may be enhanced through several provider-and evidence-derived strategies, many of which are currently underway in BC (see Table 2).
It should also be noted that the Federation of Medical Regulatory Authorities of Canada (FMRAC) published a framework for virtual care in 2022 24 that serves as a good foundation for improving the provision of virtual care in Canada. In addition, FMRAC is working on addressing barriers to provision of virtual care. This includes allowing physicians to use their licence in any province or territory for the purpose of delivering telemedicine, enabling fast-track licences ‘to expedite the issuance of licensure for physicians who hold full registration in another province/territory and who are considering moving to another part of the country (or obtaining a second licence)’ (p.9) and a licence portability agreement ‘to enable physicians to work for a maximum number of days in another jurisdiction solely on the basis of licensure in their “home” jurisdiction’ (11, p.9).
Some healthcare teams have embarked on a formal process of evidence-based and patient-informed re-design of prenatal care pathways to incorporate more virtual care options. 25 These and similar models offer promising examples of building back better after COVID.
When the MOM project began in 2015, uptake of virtual maternity care was primarily embraced by ‘early adopters’ with slow spread to the ‘early majority’ of users. Gradually, in the ensuing years, other platforms have been added to the provincial landscape such as the Rural Coordination Centre of BC's Real Time Virtual Support programme for peer-to-peer support for both urgent and non-urgent cases for Emergency care (RUDi), Paediatrics (CHARLiE), and Maternity and Newborn (MaBAL). 26 There has also been the emergence of direct pathways for patients including the First Nations Virtual Doctor of the Day, a direct-contact line for patients in rural, remote and Indigenous communities and HEiDi (HealthLink BC Emergency iDoctor-in-assistance) pathway when they call HealthLink BC (8-1-1), among others.
Limitations
This study was undertaken during an active phase of the COVID-19 pandemic which saw the precipitous, enforced shift to virtual care. The uncertainty of the pandemic itself, the stress incurred by care providers and the lack of administrative infrastructure for virtual care was significant factor influencing experiences. However, the influence was not unidirectional: there were positive and negative experiences of virtual care precipitated by the pandemic. Ultimately, however, the backdrop of the pandemic brought to light issues surrounding the uptake of virtual care that would not have been as pronounced or would have been more difficult to articulate if this study was done in a different context. Further, as with all studies that rely on voluntary participation, those who respond tend to be either positively or negatively predisposed to the topic at hand and those with less pronounced views tend not to participate. This may exaggerate the magnitude of the response.
Conclusion
The COVID-19 pandemic created the conditions for a natural experiment in scaling up the use of virtual care in obstetrics and maternity care by providing opportunities to document the insight and reflection of health care providers on the shift in care modality. These reflections and experience-based recommendations are the building blocks for a robust infrastructure for virtual care that can meet the needs of rural and vulnerable populations in an ongoing way post-pandemic. Data from this study provides an essential starting point for a deliberate and inclusive discussion on how to create a sustainable system of virtual care that meets both population health and care provider needs.
System enablers of virtual care.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Doctor of BC Specialist Services Committee for funding support for this work and to the rural maternity care providers who contributed their time and expertise to the discussion. Additionally, we express appreciation to Kathrin Stoll and Olivia Klaassen and Simrat Dial for their assistance with manuscript preparation. All authors have authorized the submission of their manuscript by a third party and approved any statements or declarations.
Contributorship
All authors contributed to the development of this paper
Ethical approval
This study was approved by the Behavioral Research Ethics Board, University of British Columbia (H15-03048).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Doctors of BC Specialist Services Committee
Guarantor
JK
Appendix 1
Draft Focus Group questions for Care Providers’ Virtual Care preferences/10 March 2021
Demographic Information
Where is your practice location? What is your provider designation: (e.g., Family Physician, OBGYN, Nurse Practitioner, Midwife)? Would you describe your practice as rural or urban? What is the volume of maternity patients you see annually? What is the distance to your referral centre? If there is no local Obstetrician, does your community have visiting Obstetrical specialists? If yes, how many days, on average, per month? Does inclement weather influence transportation type/time to referral centre? Have your incorporated virtual care into your regular practice due to COVID-19? What proportion of all visits? Will you maintain the option for virtual care post-COVID? What are the benefits of virtual care in your practice?
[If NOT OB/GYN]
Virtual Maternity Care: Practitioner values
Prompts may include:
Patient access to appropriate consultant and knowledge to make informed choices Continuity of care and carer Rural practitioner support Consultant understanding of context of rural maternity care Patient access to comprehensive, culturally safe health care Patient access to optimal care What are the main advantages of virtual consultations?
Virtual Maternity Care: Benefits and barriers
Are there any system constraints that would challenge the use of virtual tools with patients in your practice? Please describe.
Prompts may include:
Internet accessibility Speed of internet provider services in area Lack of access to required equipment (ie: computer, tablet) Unreliable cell phone service coverage Patient distance to a provider clinic to access virtual services Equipment storage and security Unfamiliarity with medical technology/digital platforms and apps What are the benefits to using digital tools to provide virtual care in your practice?
Virtual Maternity Care: Clinic impact
How did/does providing virtual care to patients impact your clinic?
Virtual Maternity Care: Practitioner use
During COVID, approximately how many virtual calls did you do a week? Pre-COVID? What would be your preferred system for the following consult scenarios:
Emergent care with patient and care team present Scheduled care consults with patient present Provider to provider decision support consults eConsults between providers When connecting for clinical decision support in a non-emergent situation, which would you prefer to connect with specialist in your regional referral centre or a provincial resource who can guide the immediate care and connect with regional teams later? What are your preferences in an emergent situation? When connecting for clinical decision support, what type of device would you prefer? In which situations would you use video conferencing? Do you have any additional comments regarding your experience with and/or preference for technology and virtual care in your maternity care practice?