
Abstract
Personal recovery represents a paradigm shift in how individuals are seen to benefit from mental health interventions, from a narrow view of symptom reduction to a holistic, multi-dimensional view of well-being, functional gains and rehabilitation. Although there is a large body of evidence supporting the use of recovery-oriented care in adults, research on personal recovery amongst youth with mental health concerns is an emerging area of research. Efforts to promote youth mental health have also focussed on the use of digital applications and platforms as a means of overcoming barriers related to factors including stigma and lack of available services. This systematic review aims to review the literature on existing internet-based, youth mental health interventions with regard to (a) identifying elements of the programs that align with the personal recovery and (b) outcome measures utilised in assessing personal recovery. Eleven papers were identified that met the inclusion criteria. Five of the programs reviewed from these eleven papers showed efficacy for recovery processes. The results offer preliminary support and guidance for the use of internet-based mental health interventions in the promotion of personal recovery amongst youth. Future research and practice are suggested to further develop understanding in this area.
Keywords
Introduction
Background
There are growing concerns for the future mental health of young people around the world.1–4 Epidemiological studies highlight that increasing numbers of youth experience poor mental health.4,5 Young people diagnosed with mental disorders show prevalence rates between 20% and 25% with around 50% of adult mental health disorders originating during adolescence.6,7 The burden of mental health impacts is particularly pronounced amongst youth who are geographically and socially isolated and experience mental health problems in conjunction with multiple social vulnerabilities. 8 Concerns about the reach of mental health services for youth have led to innovations in interventions and service development as a way of engaging vulnerable youth and their families. Mental health interventions and services are increasingly looking to deliver services that move beyond symptom reduction and crisis management, to focus on de-stigmatisation, gains in general functioning and psychosocial rehabilitation. 9 Personal recovery (from here referred to as recovery) originates from the model of adult psychiatric rehabilitation and embodies a humanistic theme through the promotion of self-efficacy and maximising potential. 10 Recovery represents a paradigm shift in how individuals are seen to benefit from mental health interventions, from a narrow view of symptom reduction to a holistic, multi-dimensional view of well-being, functional gains and rehabilitation. 11
Conceptualisations of recovery
Concepts of recovery in mental health were introduced by Deegan 12 who described it as a unique, non-linear journey which is shaped by an individual's attitude and approach towards the challenges of daily life. Anthony 11 expanded the concept further, defining recovery as a personal process of change to one's way of thinking, feeling and being, to develop meaning and purpose outside the constraints of mental ill-health. The view challenges the dominant assumptions of mental health informed by the medical model, to support individuals to lead satisfying and productive lives, with or without the presence of concerns related to mental health. 11 Recovery-oriented care represents a person-centred approach to promoting recovery through a focus on individual strengths and goals. 13 Recovery-oriented care also incorporates mental health lived experience inspiring self-efficacy and hope and purpose, whilst diminishing long-term dependency on services.13,14
In doing so, recovery seeks to de-stigmatise mental illness and integrate individuals into the community supporting satisfying and meaningful lives.9,11 This multi-faceted approach has revolutionised mental health policy and service delivery around the world and has since become the best practice in adult mental health settings.15,16 With recovery-oriented practice gaining momentum around the world, numerous theories have sought to conceptualise the recovery process. Leamy et al. 17 have proposed a framework of recovery in adults emphasising five categories of individual recovery processes outlined in the CHIME model: connectedness, hope and optimism, identity, meaning in life and empowerment (see Figure 1). 17 With a growing body of literature supporting the model amongst adults with mental health concerns,17,18 emerging research has begun assessing the applicability of the model to younger persons.19–21
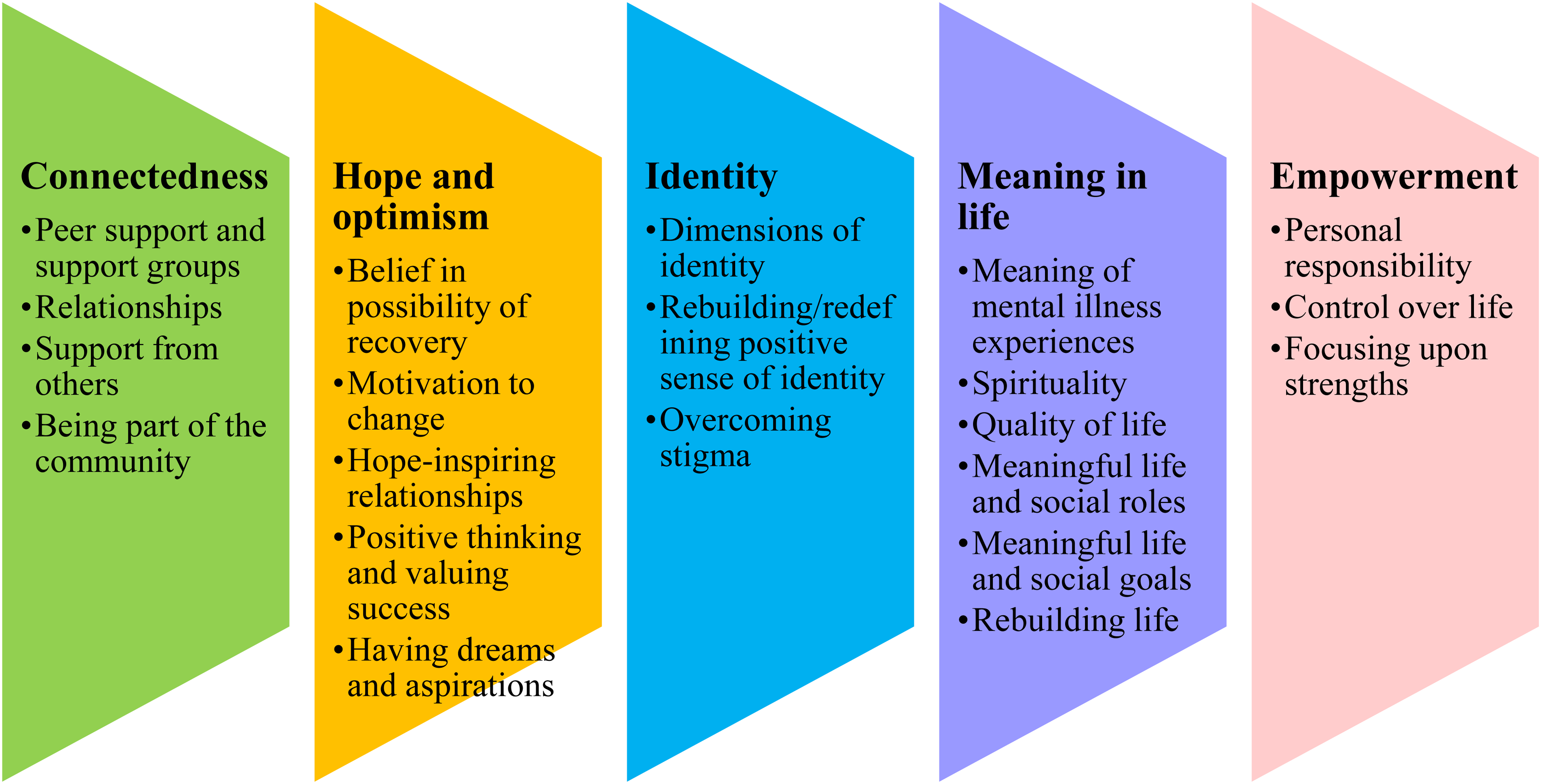
Processes of adult recovery (CHIME 17 ).
Mental health recovery in youth
Concepts of recovery are relevant to all youth and particularly important for vulnerable young people who have reduced capacity for self-management, who are less responsive to primary and secondary services, and who require more scaffolding to improve general functioning.4,7 The literature suggests that therapeutic relationships, system communication, community interventions, the inclusion of parents, families and supports and psychoeducation are imperative to the recovery journeys of young people. 19 While such elements can also promote clinical recovery, recovery-orientated interventions focus on improvement in functioning and engagement in normative activities and relationships across settings, rather than just a reduction of mental health symptoms.13,15,19 Additionally, appropriate measures for youth recovery are still emerging and as yet there are no dedicated measures to assess recovery that have been conceptually validated for youth. 16
Most recently, Naughton et al. 18 employed a scoping review to explore the literature on youth recovery in the context of mental health services. Eight papers met the criteria for inclusion, emphasising a significant lack of published literature in this area. Naughton et al. 18 noted that recovery for young people included themes consistent with the CHIME framework for adult recovery. 17 Additionally, Naughton et al. 18 noted the importance of including parents, families and support in recovery-orientated practice. Parents and systems play an imperative role in the recovery of youth, more so than in adulthood.13,18 It is also vital for parents and families to receive support themselves to assist with the distress that may be experienced from having a child or family member with mental health issues. John et al. 16 noted the importance of evaluating both the young person’s and the parent's perceptions of personal recovery.
Potential of internet interventions to promote recovery
There has been increased interest in delivering mental health interventions through internet-based platforms.6,22,23 Several growing youth are turning to websites and social media platforms for social and emotional support and reports indicate that the medium of online interventions offers a key incentive for young users.24,25 Digital mental health services and applications have been found to overcome several barriers to access, including geographical restrictions limiting access, high costs and concerns regarding stigma.22,26 Numerous reviews indicate that digital interventions are feasible and acceptable for young people with mental health concerns, with promising signs of their efficacy. 27 The internet also provides a medium for direct delivery of interventions to a wide population of individuals, as well as a link to other online or face-to-face health services and resources and represents a unique opportunity to promote recovery and recovery-oriented care to youth. 23 However, relatively few applications have employed a recovery-oriented co-design and co-delivery methodology in the design and development of internet-based interventions. 27 Current online interventions are typically more clinical in orientation, focusing on problems and dysfunctions and placing the expertise with the professional. 28 The current review aims to understand the elements of existing internet-based applications that include recovery-oriented interventions and measures to identify recovery intervention efficacy.
Summary
Recovery interventions for youth provide an opportunity to reduce the burden of mental illness on young people while also reducing the potential impact of mental illness into adulthood. Internet-based applications offer the potential to support recovery for youth, providing greater reach and engagement. This review is, to our knowledge, the first systematic attempt to synthesis the evidence on the effectiveness of internet-based interventions in promoting recovery for this population. Given the potential for internet-based interventions to enhance mental health services, it is worth noting that many existing internet interventions may also possess elements of recovery-oriented practice. Utilising the CHIME recovery framework, 17 this review examines recovery-oriented application in existing internet-based interventions for youth to answer the following question: What specific interventions and outcome measures have been utilised and what are the characteristics of internet-based interventions that promote recovery amongst youth aged 13 to 18 years with mental health concerns?
Methods
A systematic review attempts to collate all pertinent evidence that meets pre-determined eligibility criteria to answer a particular research question. It uses specific systematic methods to reduce bias in the identification, selection, synthesis and summary of previous findings. The key characteristics of a systematic review are defined objectives with reproducible methodology; identification of all studies meeting eligibility criteria; assessment of the validity of the findings of selected studies; systematic presentation and synthesis of the characteristics and findings of the included studies. 29
Search strategy
The search was conducted between March and April 2020 with searches limited to publications between 2006 and 2020. The initial search strategy included the term (Recovery OR Personal Recovery) and resulted in only one article. The search was revised with the intent to increase the number of search items. The revised search strategy included (Adolescen’) AND (mental health OR mental illness’ OR mental disorder’ OR mental disease’ OR mental problem) AND (online OR internet OR computer’ OR web’) AND (intervention OR program OR therapy OR treatment OR psychoeducation) and combinations of these search criteria. The search was run on six databases (EBSCOhost, PsycINFO, Ovid, Scopus, JSTOR and JMIR), and a limited keyword search was performed on Google Scholar and Semantic Scholar search platforms. Additional searches included hand-searching of population-specific clinical journals and citation tracking of relevant literature. Reference lists of sourced literature were hand-searched for additional publications.
Study selection
The review follows the guidelines set out by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2009 checklist. Eligible studies included an internet-based platform for intervention, included at least one outcome related to a process of the CHIME model, and focussed on reducing mental health issues in participants aged 13 to 18 years. This age range was selected to support the focus of a larger research project that encompasses this review. Experimental study designs included randomised control trials (RCT) or pre-post designs without a control comparison. Only literature published in English was included to avoid translation and publications prior to 2006 were excluded as the majority of searched literature commenced in 2006.
A total of 2199 publications were assessed through two phases detailed in Figure 2. Exclusion criteria were: (a) age groups outside the population under review, (b) not written in English, (c) not published in a peer-reviewed journal, (d) internet-based interventions that are not self-directed, (e) studies that do not include measures corresponding in some way to the five CHIME processes, (f) studies that were not experimental quantitative designs or (g) research before 2006.
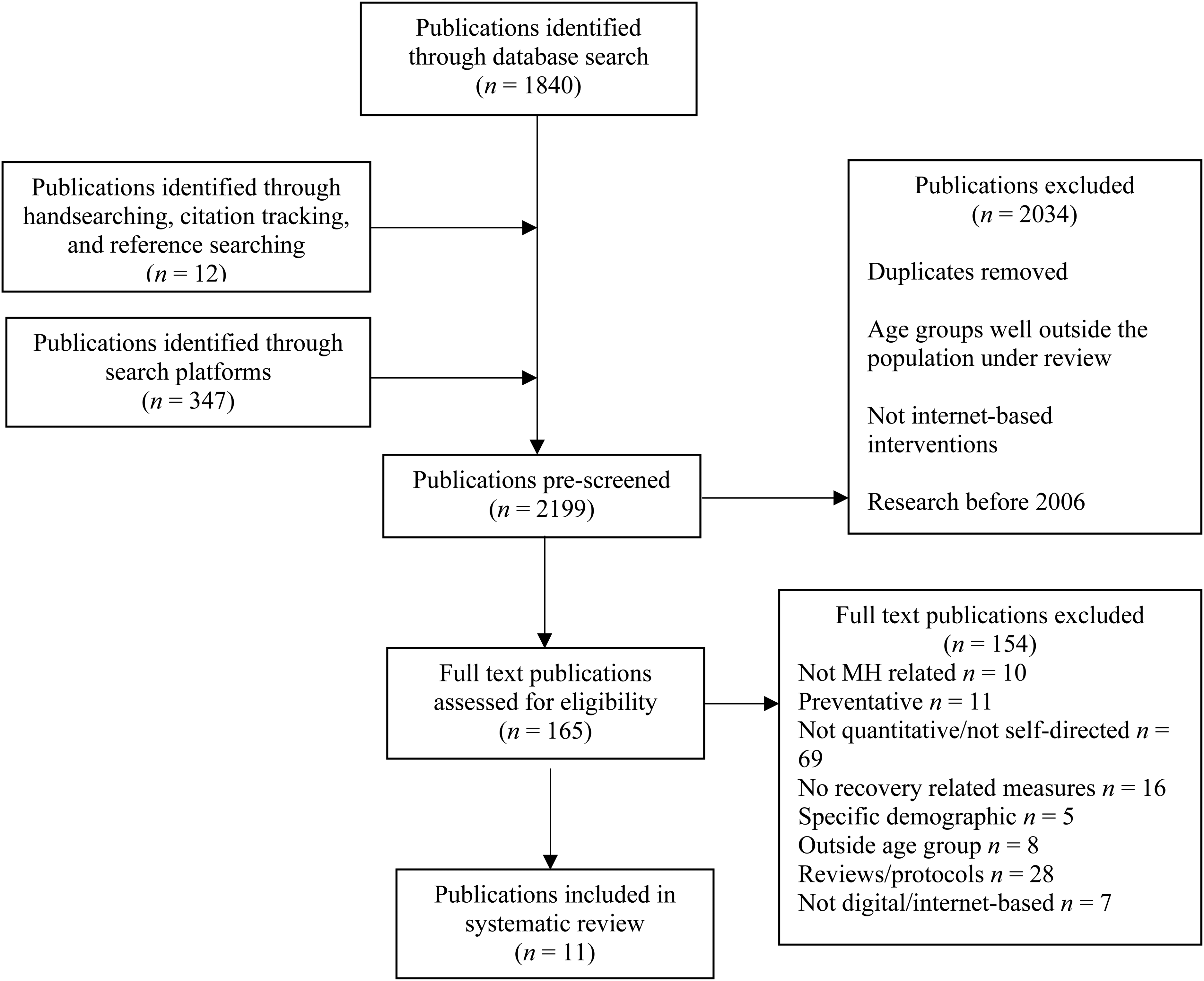
PRISMA flow diagram for the study selection process.
Data extraction and synthesis
A narrative synthesis was employed to accommodate the diversity of the publications reviewed and deemed more appropriate than thematic analysis in exploring the recovery-related outcomes of these studies that were designed to observe and report on symptomatic outcomes. The initial selection was compiled by one researcher and full-text publications were reviewed by both first and second authors to ensure relevant criteria were met within included articles. Any discrepancies in meeting criteria were resolved with the removal of related article/s.
A quality assessment of each of the final articles was completed using the Effective Public Health Practice Project Quality Assessment tool for Quantitative Studies. This assessment tool was developed for use in public health and can be applied to articles on any public health topic area.30,31 It includes the following criteria in the assessment of the quality of quantitative research: (a) selection bias, (b) study design, (c) confounders, (d) blinding, (e) data collection methods and (f) withdrawals and dropouts. Table 1 details the quality assessment results for the publications evaluated within this review.
Quality assessment results.
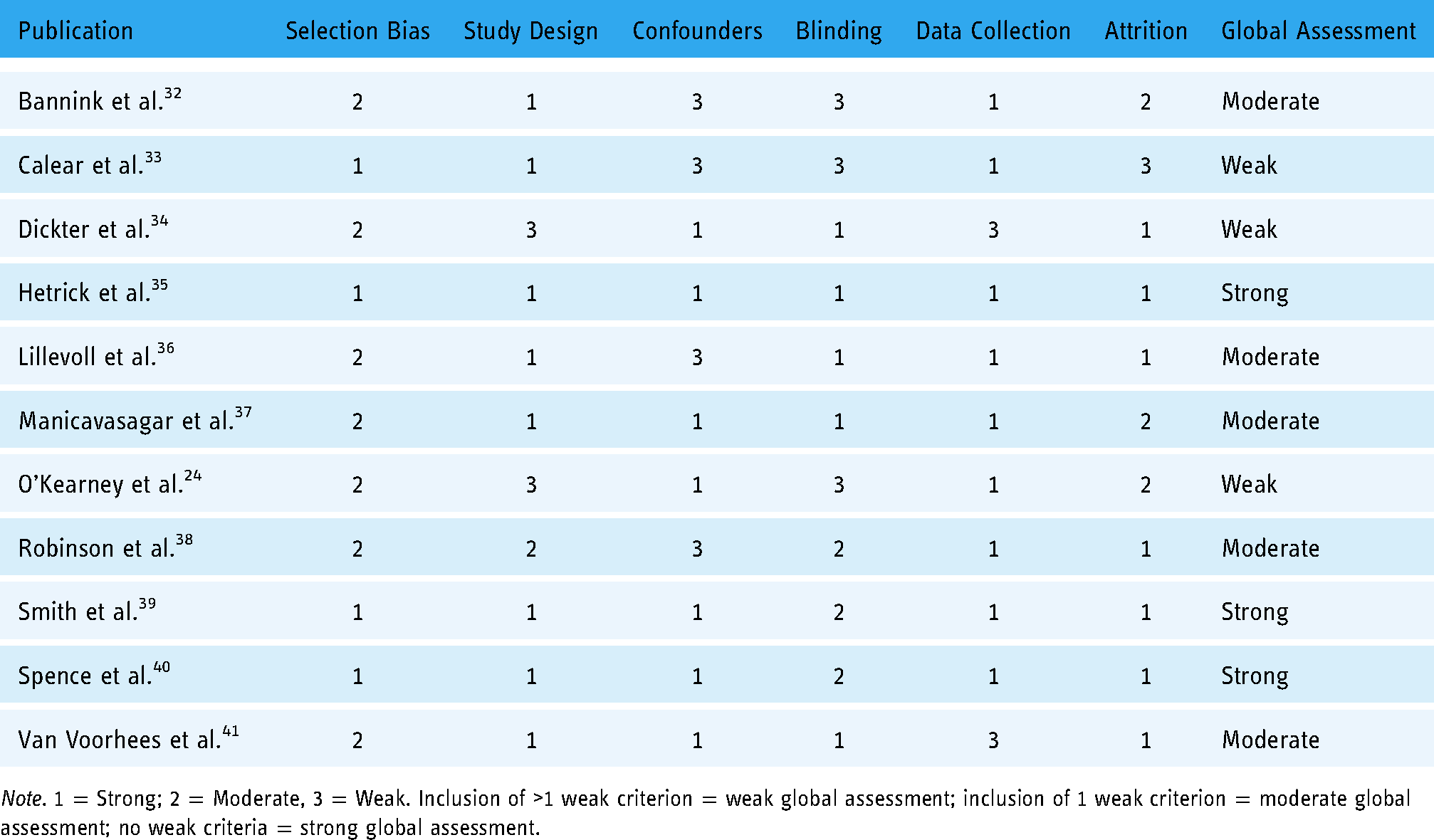
Note. 1 = Strong; 2 = Moderate, 3 = Weak. Inclusion of >1 weak criterion = weak global assessment; inclusion of 1 weak criterion = moderate global assessment; no weak criteria = strong global assessment.
Results
A total of 11 publications meeting the criteria were included in the systematic review. Results from these publications are presented in the below tables. All included studies incorporated measures that could be applied to the CHIME model.
Intervention characteristics and how they aligned to recovery processes
Study characteristics, designs, effect size and effectiveness outcomes of the interventions are detailed in Table 2.
Study characteristics.
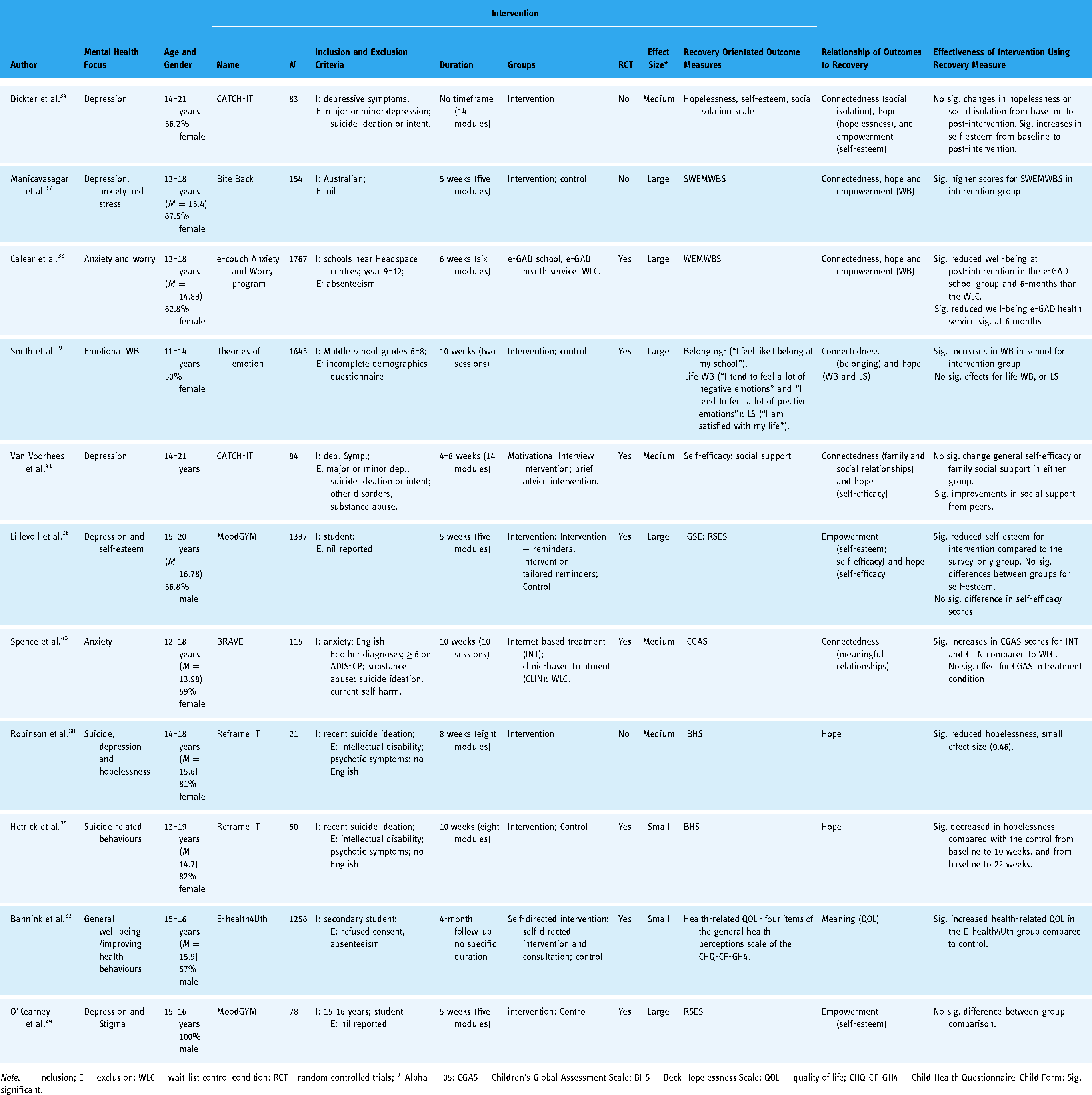
Note. I = inclusion; E = exclusion; WLC = wait-list control condition; RCT – random controlled trials; * Alpha = .05; CGAS = Children's Global Assessment Scale; BHS = Beck Hopelessness Scale; QOL = quality of life; CHQ-CF-GH4 = Child Health Questionnaire-Child Form; Sig. = significant.
Table 3 details the specific intervention characteristics and how they align with the CHIME recovery processes. 17 Not all processes were assessable or shown to be efficacious using the measures employed in these studies. Seven of the eight interventions embodied characteristics associated with the process of connectedness. Providing resources was the common intervention characteristic that aligned with the recovery process of connectedness and was found in three of the eight interventions. Other characteristics included the support of professionals and parents while accessing the intervention and education on relationship building and coping strategies.
How intervention characteristics aligned with recovery according to CHIME. 17

Note. ToE = Theories of Emotion; * = measured; ** = measured and showed significant benefit pertaining to this process.
Study characteristics
Intervention characteristics, a relationship of the interventions to recovery, and facilitators and barriers to the interventions are detailed in Table 4.
Intervention characteristics and relationship to recovery.

Note. * = see Gladstone et al. 42 for further detail on intervention structure and content; CHIME = connectedness, hope, identity, meaning and empowerment; CBT = cognitive behaviour therapy; IPT = interpersonal psychotherapy; WEMWBS = Warwick–Edinburgh mental well-being scale;
CHIME = connectedness, hope, identity, meaning and empowerment; CBT = cognitive behaviour therapy; WEMWBS = Warwick–Edinburgh mental well-being scale;
CBT = cognitive behaviour therapy.
How personal recovery was operationalised
Outcome measures were analysed for items that encapsulated characteristics aligning with the CHIME framework. None of the studies included outcomes that were relevant to all processes within the CHIME framework. Outcomes for each process are discussed in the acronym order.
Connectedness
Six studies included measures identifying connectedness such as the Children's Global Assessment Scale (CGAS 44 ) and Warwick–Edinburgh Mental Well-being Scale (WEMWBS33,37,45). The CGAS assesses overall levels of social functioning while the WEMWBS includes items “I’ve been interested in other people,” “I’ve been feeling close to other people” and “I’ve been feeling loved.” 45 Dickter et al., 34 Voorhees et al. 41 and Smith et al. 39 compiled items to develop their own social isolation and belonging scales (Table 1).
Hope and optimism
Eight of the studies reviewed included measures assessing hope or included items that aligned with the hope process defined by the CHIME framework.33–37,39,41,43 Smith et al. 39 included items assessing life well-being and satisfaction which has been linked to hope in numerous studies46,47 (Table 1). Dickter et al. 34 compiled items to form a hopelessness scale. Studies by Calear et al. 33 and Manicavasagar et al. 37 both assessed outcomes using the WEMWBS which contains items “I’ve been feeling optimistic about the future,” “I’ve been feeling useful,” “I’ve been dealing with problems well” and I’ve been feeling cheerful.” 45
The Beck hopelessness scale (BHS) was used by Hetrick et al. 35 and Robinson et al. 43 to assess outcomes. The general self-efficacy scale (GSE) used by Lillevoll et al., 36 and Voorhees et al.’s 41 self-efficacy scale were also aligned with hope and optimism as self-efficacy is associated with increased levels of hope. 48
Identity
According to the CHIME personal recovery framework, the identity process includes the following characteristics: dimensions of identity, rebuilding/redefining a positive sense of identity and overcoming stigma. 17 None of the studies in this review included outcomes aligned with this process.
Meaning and purpose
Bannink et al. 32 included outcomes associated with quality of life. This study utilised four items from the Child Health Questionnaire-Child Form (CHQ-CF-GH4). While they did not detail which four items they included in the outcome measure they did report these items were associated with general health perceptions which can be associated with the meaning of mental illness experiences.
Empowerment
Six of the studies reviewed included outcome measures that were associated with the process of empowerment.24,33,34,36,37,41 These measures assessed outcomes for self-efficacy and self-esteem and while they were different constructs of empowerment, both were considered elements of empowerment.49,50 Dickter et al. assessed outcomes using a self-developed self-esteem scale 34 and Voorhees et al. assessed outcomes using a self-developed self-efficacy scale. 41 Calear et al. 33 and Manicavasagar et al. 37 both assessed outcomes using the WEMWBS that contains items associated with empowerment such as “I’ve been feeling good about myself,” “I’ve been feeling confident” and “I’ve been able to make up my own mind about things.” 45 Lillevoll et al. 36 utilised both the GSE and the Rosenberg self-esteem scale (RSES) to assess outcomes, while O’Kearney et al. 24 also used the RSES.
Discussion
The ongoing burden of mental health concerns for youth is of prominent interest in the provision of services that are looking to reduce ongoing reliance on resources and promote well-being in this population. Particularly for youth with more severe mental health concerns, the goal of symptom cure is not always a realistic one and research has shown that quality of life is not dependent on being symptom-free. Recovery for youth is an emerging construct and research on interventions and recovery-orientated practice for this period of development is still in its infancy. This review provides the first overview of research pertaining to internet-based interventions designed to support mental health in youth and those that may indirectly support recovery in this population. It is worth noting that there are currently no internet-based interventions specifically designed to promote recovery in young people and that the interventions discussed in this review have a primary objective of symptom and behaviour reduction. The lack of evidence-based efficacious internet interventions for youth recovery may be directly related to the early stages of research in this area.13,19 It may also be related to controversies around the application of recovery to youth with some reporting that the concept of recovery is developmentally inappropriate for young people. 13 However, this review has shown that while some internet interventions are not designed to target recovery, they do indirectly promote it.
The studies identified in this review comprised measured outcomes that could theoretically support at least one of the CHIME recovery processes outlined by Leamy et al. 17 It was found that while each of these interventions held different objectives related to either behaviour change or symptom reduction, each could be aligned in theory with the concept of recovery. Of interest were the common intervention characteristics that supported recovery outcomes. These were psychoeducation, linking to external supports, sharing the experience with family or professionals, skill-building activities, peer narratives and teaching problem-solving skills. It was also noted that most of the various outcome measures employed could be aligned with at least one of the CHIME processes. 17 This demonstrated that while there are currently no internet interventions solely dedicated to youth recovery, there is efficacy in the use of existing internet interventions in support of recovery. Further research exploring the efficacy and characteristics of these interventions offers the opportunity to provide additional support to these findings. Additionally, this review highlighted the need for dedicated personal recovery measures for youth and that some existing youth mental health measures offer a potentially effective assessment of individual personal recovery processes.
Support for the use of internet interventions to promote recovery in youth
Interventions were assessed according to how their characteristics aligned with the CHIME model. 17 Of the eight interventions reviewed through 11 publications, the Bite Back and Reframe-IT interventions held characteristics that aligned with all five of the CHIME processes.35,37,38 Both interventions also showed efficacy for recovery through measures aligned with these processes.
For the interventions BRAVE, CATCH-IT and eHealth4U, each held characteristics that aligned with four of the CHIME processes.32,34,40,41 All other interventions held characteristics that aligned with three or fewer of the CHIME processes. Except for the MoodGYM intervention, all interventions showed efficacy for recovery processes through measures aligned to recovery processes. Of those interventions that showed efficacy, the Reframe-IT, BRAVE and CATCH-IT interventions included participants with mental health symptomology.34,35,38,40,41 These findings suggest that while existing interventions largely had the primary objective of symptom reduction, they also demonstrated the ability to support recovery for young people. Characteristics identified offer a platform for future recovery targeted inventions.
Youth recovery outcomes in internet interventions
All interventions except for Bite Back had at least one study utilising an RCT in this review. Publications for the CATCH-IT and Reframe-IT interventions included an RCT and a pre–post method of design. While the Reframe-IT studies employed the same measures and reported consistent results across both research methodologies, the CATCH-IT studies reported inconsistent results across both methodologies. This may have been a result of the different study designs used and may have limited the validity and reliability of the measures used within the CATCH-IT research as relevant to recovery. Measures from both studies aligned with connectedness, hope and optimism processes and intervention characteristics aligned with four of the five CHIME processes. Both CATCH-IT studies failed to demonstrate any benefits to hope and optimism; one CATCH-IT study showed some benefit to connectedness, 41 while the other was linked to empowerment. 34 Both studies utilised ratings from standard assessments of importance to assess research questions. The research question proposed by Dickter et al. 34 aimed to examine the effectiveness of the CATCH-IT program on suicide risk factors and therefore outcomes were assessed using different compilations of the data to represent relevant risk factors. This may have been attributed to the variance in results between the studies.
Several outcome measures were used in the studies examined. None of the measures used within the studies provided outcomes for all five recovery processes. In fact, none of the measures examined in this review aligned with the process of identity. The majority of measures aligned with CHIME processes connectedness, hope and optimism and empowerment, respectively. This may reflect the fact that most of these measures were designed to assess well-being, hopelessness and/or self-efficacy. Only one measure could be aligned to the process of meaning and purpose (CHQ-CF) and this relationship could be deemed as weak because the study using the measure provided no detail regarding the items used within the quality-of-life scale assessed. Other measures, such as the WEMWBS, GSE, RSES and BHS, have stronger theoretical alignment to the processes of connectedness, hope and optimism and empowerment and therefore provided more reliable outcomes for recovery. No measures specifically designed to assess recovery for youth were used within any of the studies for reasons previously mentioned.
Five of the eight interventions examined showed beneficial outcomes for recovery-aligned processes. The Bite Back program assessed well-being using the WEMWBS and found benefits of this program to all three CHIME processes aligned to well-being (connectedness, hope and optimism and empowerment). The BRAVE program showed promise for increased levels of connectedness (CGAS) and intervention characteristics aligned with four of the five processes. The Reframe-IT program showed improvements in hope (RSES) and intervention characteristics aligned with all five processes. The eHealth4U program induced a greater sense of meaning for health-related quality of life (CHQ-CF) and held intervention characteristics aligned with four of the five CHIME processes. As previously discussed, the CATCH-IT studies showed inconsistent but efficacious results for connectedness and empowerment.
The e-Couch anxiety and worry (WEMWBS), theories of emotion (self-developed measures related to connectedness and hope), and MoodGYM (GSE; RSES) interventions showed no benefits to recovery-aligned outcomes. All of these interventions aligned to a lesser extent with CHIME processes. While some programs did not show efficacy in those measures aligned to recovery, this did not mean they did not show efficacy in symptom reduction.
Limitations
It is difficult to be conclusive regarding internet recovery-orientated interventions for youth when there were so few studies available for review. Further research is required to determine the effectiveness of the characteristics and length of these online interventions, and appropriate outcome measures supporting recovery are needed. Due to the variability among the interventions, it was not possible to assess specific strategies and methods that supported recovery outcomes through this review.
Ethnicity of the populations explored within this review was varied with three publications based in the US, one from Norway, one from The Netherlands, one with mixed Westernised representation and five based on Australian youth. While this may increase the generalisability of these results for Western and euro-centric populations this review is limited in its representation of a more global perspective.
A systematic search of grey literature was not included, nor were studies that were written in languages other than English. The possibility of publication bias should also be considered as there may have been other research available through unpublished studies that have not shown positive outcomes for support of youth recovery. Additionally, the data reviewed from these publications were summarised and analysed using a narrative synthesis and not statistically combined, limiting the strength of the derived conclusions.
Future research
Further research exploring the efficacy of these interventions and their characteristics offers the opportunity to provide additional support to these findings. The construct of youth recovery is still in its infancy and this research highlights several research gaps in this area including the use of online interventions to support young people during recovery. There is a particular need for further research to identify the key internet-based program elements required to support youth recovery. While this research has found several common intervention characteristics consistent with recovery for young people, further research should focus on other recovery-aligned characteristics and their efficacy within new and existing online interventions supporting youth recovery. Additional research is also needed to explore other existing measures that align with recovery processes and their efficacy for measuring these processes for this population. Furthermore, there is also a capacity for the development and validation of a youth recovery measure that assesses all five recovery processes according to the CHIME framework.
Conclusion
Although there are currently no dedicated internet-based interventions supporting recovery for youth, this review has shown efficacy in supporting recovery within existing internet-based interventions for this population. While these results should be interpreted with caution, they hold promise for the benefit of further research in this area. Youth mental illness is a growing concern for the well-being and future of our younger generation and leads to an increased burden on families and health services. Recovery for young people is a relatively new construct and research is still emerging to support the efficacy of recovery-orientated interventions and recovery-orientated digital interventions for youth. This review has demonstrated that while research dedicated to online recovery-orientated interventions and measures of recovery for youth are largely non-existent, the benefits of existing internet-based mental health interventions and youth measures hold hope for future success in this area.
Footnotes
Author contributions
VCD and GK researched literature and conceived the study. VCD wrote the first draft of the manuscript. GK, LB, CdP, APS and AA reviewed, added to, and edited the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Guarantor
L.B.