
Abstract
Objective
This study examined the feasibility of an activity tracker and app intervention to increase physical activity in whole families.
Methods
This was a single-arm feasibility study with pre–post-intervention measures. Between 2017 and 2018, 40 families (58 children aged 6–10 years, 39 mothers, 33 fathers) participated in the 6-week Step it Up Family programme in Queensland, Australia. It was delivered using Garmin activity trackers and apps, weekly motivational text messages and an introductory session. Online surveys and semi-structured interviews conducted with parents assessed intervention usage, acceptability, usability, perceived usefulness, use of physical activity self-management strategies and programme influence. Analyses included descriptive statistics, Wilcoxon signed-rank test and qualitative content analysis.
Results
Overall, 38 families completed the post-intervention survey (95% family retention; 90% children, 95% mothers, 88% fathers). Garmin activity tracker usage was high (i.e. nearly 24/7 during the 6 weeks intervention). Families also used the Garmin apps regularly (i.e. mostly 2–6 times per week). Further, 80% of mothers and 52% of fathers read the motivational mobile text messages. Usability and perceived usefulness of the Garmin activity trackers and apps were rated high. Both parents significantly increased their use of physical activity self-management strategies from pre to post-intervention. Parents expressed that the intervention had increased awareness of physical (in)activity in the family, encouraged to be active and promoted outdoor family activities.
Conclusions
Using activity trackers and apps to increase physical activity in the whole family was well received by children and parents which suggests that this intervention approach is feasible. However, further testing is needed amongst more diverse family populations. These early findings support the implementation of a randomised controlled trial to examine intervention efficacy.
Keywords
Introduction
In Australia, more than 80% of children aged 5–17 years do not get the recommended 60 minutes of moderate-to-vigorous physical activity per day. 1 Further, 55% of adults do not achieve the recommended 150 minutes of moderate-to-vigorous physical activity per week. 2 Physical inactivity significantly contributes to Australia's high prevalence of overweight and obesity in children (25%) and adults (67%). 3 Moreover, physical inactivity significantly contributes to major chronic diseases such as cardiovascular disease, diabetes and cancer. 4
Physical inactivity starts in childhood and often runs in the family.5,6 Within the family unit, children and parents influence each other's physical activity behaviours through mutual support and role modelling.6–9 Therefore, family-based physical activity interventions that actively involve the whole family are needed. However, previous family-based physical activity interventions have typically involved parents (mainly the mother) as supporters, rather than as participants, with the primary aim to increase physical activity in the children.10,11 A whole family approach where the intervention aims to increase physical activity in both children and parents has been attempted in very few studies.12,13 A common difficulty in family-based interventions is engaging both parents when they need to attend sessions face to face. 14 Key barriers for attending face-to-face sessions are families’ busy schedules and their limited time during the after-school/work hours. 14 An online delivered activity tracker and app intervention can address these barriers as the whole family can participate in the intervention conveniently from their home environment. Further, when using activity trackers and apps to monitor progress, both parents can easily be involved in a family-based physical activity intervention.
Activity trackers combined with a smartphone app are widely used and popular motivators for becoming more physically active.15–17 In 2021, one in five Australian adults used a wearable activity tracker that comes with an app (e.g. Fitbit and Garmin). 18 Latest activity tracker and app brands (e.g. Garmin Vivofit Junior and Fitbit Ace series) are also designed age-appropriately for young children. Recent meta-analyses19–21 and our own systematic review 22 have shown that activity tracker and app interventions can effectively increase physical activity in children and adults but testing in whole families is lacking. The popularity of wearable activity trackers and apps in the general population, and their proven efficacy in both children and adults, suggests that this technology has great potential to promote physical activity in families. However, to our knowledge, no physical activity intervention has yet used the latest commercial activity trackers and apps to increase physical activity in whole families. The few existing family-based interventions in this area have utilised an older generation activity tracker (i.e. pedometer) 12 or a researcher-developed smartphone app. 13
To address the research gaps, this study aimed to examine the feasibility of using activity trackers and apps in an intervention to increase physical activity in whole families. Intervention feasibility was examined in terms of usage, acceptability, usability, perceived usefulness, the use of physical activity self-management strategies and programme influence.
Methods
Study design
The Step it Up Family programme was a single-arm feasibility study with pre–post-intervention measures conducted between 2017 and 2018 at the Central Queensland University in Rockhampton, Australia. The study examined the active involvement of children and parents (mothers and fathers) in a family-based physical activity intervention. Ethical approval for the study was received from the Central Queensland University Human Ethics Committee in May 2017 (H17/03-041). Written informed participant consent was obtained online from both mothers and fathers, and one parent provided consent on behalf of the participating children. 23
Participants
In 2017/2018, 40 families living in Central and South East Queensland (mostly in the Rockhampton and Yeppoon areas), Australia were recruited into the Step it Up Family programme. Recruitment was paused during the Australian summer school holiday period from December 2017 to January 2018. Eligibility to participate in the study required that mothers and fathers (including step-mothers/fathers and female/male guardians) were older than 18 years, and at least one of their children were aged 6–10 years. Children aged 6–10 years were targeted as this age range is crucial for forming physical activity behaviours, spending time with parents and being influenced by parental social support and role modelling. 24 Children younger than 5 years were not enrolled due to limited ability to comprehend activity tracker and app features. Children older than 10 years were not enrolled as (pre)adolescents are more influenced by physical activity role modelling and support from peers rather than parents. 25 Non-enrolled siblings still received an activity tracker to ensure that no child in the family was left out and that positive family dynamics targeted in the intervention (e.g. family step challenges) were not undermined. Since the study focused on active involvement of both mothers and fathers in a family-based intervention, single-parent and same-sex parent families were initially excluded. However, family eligibility was later relaxed to expedite recruitment and reach the target sample of 40 families. Other study inclusion criteria included: all family members could speak and read English; all family members lived together in one household; all enrolled parents had access to the Internet, and a smartphone or tablet; the child had not previously used an activity tracker (e.g. pedometer, Garmin, Fitbit and Apple Watch) to increase physical activity, and all family members could safely increase physical activity. Further, children and parents had to be ‘insufficiently active’ at baseline, defined as not meeting Australia's Physical Activity Guidelines (children: <60 daily minutes of moderate to vigorous physical activity; adults: <150 weekly minutes of moderate to vigorous physical activity). 26 Finally, to be eligible, the mother could not be pregnant at the time of recruitment, as pregnancy can affect physical activity levels and motivation. 27
The Step it Up Family intervention
The intervention components of the Step it Up Family programme are presented in detail in the Supplemental material and.23 in a previously published paper on this study. 23 Briefly, the Step it Up Family programme was designed to motivate the whole family (children aged 6–10 years, mothers and fathers) to become more physically active. The intervention incorporated evidence-based health behaviour change techniques (e.g. goal setting, self-monitoring, performance feedback, social support and role modelling)28,29 tailored to physical activity behaviour. Further, the intervention targeted core constructs of social cognitive theory (e.g. self-efficacy and modelling, reinforcement) 30 and self-determination theory (i.e. autonomy, competence and relatedness). 31 Overall, the 6-week intervention included an introductory session (delivered to each family face to face or via telephone; ∼60 minutes duration), wearable activity trackers and apps, other family resources (i.e. family step challenge log poster, informational leaflets) and motivational and educational text messages (sent 3 × per week to parents). Primarily, the Step it Up Family programme was an activity tracker and app intervention. Children, mothers and fathers received age-appropriate activity trackers combined with apps (Children: Garmin Vivofit Jr activity tracker including Vivofit Jr app, Parents: Vivofit 3 activity tracker including Garmin Connect app). The activity trackers and apps aimed to motivate all family members to increase steps and active minutes daily and weekly. The detailed design and features of the wrist-worn activity trackers and smartphone apps used in the intervention have been presented elsewhere. 23 Briefly, the Garmin Vivofit Jr activity tracker had a child-friendly design as it displayed children's steps and progress to reaching the recommended 60 minutes of physical activity. Further, it was waterproof and its battery lasted 1 year. The corresponding Vivofit Jr app (installed and controlled via parents’ smartphone/tablet) displayed the steps of all enrolled family members on a family leaderboard. Additionally, the Garmin Vivofit Jr activity tracker and app had other engaging features children could opt to use (e.g. bright colour band, watch, personal name and animal images on display, virtual coins as rewards and virtual adventure trail). Using the activity trackers and apps daily for 6 weeks, both children and parents were instructed to set individual and family-level graded step goals, self-monitor steps and active minutes individually and as a family, conduct family step challenges and use the family leaderboard shown in the app to monitor individual and family progress (Table 1). All enrolled family members attended the introductory session together to actively involve the whole family from the start. In the introductory session, the family members were asked to become physical activity role models and support each other in becoming more physically active individuals and as a family. For this, both children and parents were given examples of goal setting and physical activity social support (e.g. encouragement to be active, praise for reaching step goals) and modelling (e.g. co-participation in physical activity).
Sociodemographic characteristics of Step it Up Families.

M: mean; SD: standard deviation.
Procedures
Research personnel
Recruitment, intervention delivery and data collection were carried out by a trained research officer who was experienced with family-based intervention research. Another research assistant helped with the recruitment process.
Recruitment
The families were recruited through multiple channels: (1) 1 Facebook advertisement, (2) 11 Facebook groups (e.g. Yeppoon and Rockhampton Regional Councils and Yeppoon Families), (3) 78 local organisations (e.g. schools, kindergartens, youth and community organisations, sporting facilities, businesses and politicians’ office), (4) six local media (newspaper, radio) and (5) word of mouth. An online screening survey was used to determine families’ eligibility for the Step it Up Family programme. One parent (91% mothers) completed the screening survey for the family, and if potentially eligible, further confirmation was sought via a telephone interview. After family eligibility was confirmed, parents received an email with a link to an online participant consent form and baseline survey. The participant consent form and all online survey assessments (baseline, post-intervention) were completed by both mothers and fathers. In addition, one parent (93% mothers) completed the participant consent and survey questions on behalf of the participating children (as children younger than 10 years do not provide reliable and valid survey data).
Intervention delivery
Upon completion of consent forms and baseline surveys by both parents, the researchers arranged the introductory session (60 minutes duration) with families in accordance with families’ schedules. During the introductory session, families received the intervention resources (i.e. activity trackers and apps, family step challenge log poster, informational leaflets). To further accommodate families’ schedules, the delivery mode of the introductory session was organised conveniently for each family: via telephone (35% of families) or face to face (65% of families) at the Central Queensland University Rockhampton Campus, a public playground or the family home. When the introductory session was delivered via telephone, families were posted the intervention resources including instructions on how to download the apps to their smartphones/tablets. Families received up to five shopping vouchers (3 × $20 AUD voucher, 2 × $30 AUD voucher) as a compensation for their time, and to encourage retention and minimise Garmin activity tracker and data loss. The first two $20 vouchers were provided at the face-to-face introductory session (or posted with the intervention resources if the introductory session was delivered via telephone), provided both parents attended. If one parent attended, one voucher was provided. The third voucher was posted mid-intervention if all family members had recorded steps and active minutes via the Garmin apps (daily and weekly recordings were downloaded by research staff during the intervention through the access of participant’s app accounts). The fourth voucher ($30 AUD voucher) was posted at the end of the intervention, upon completion of the post-intervention survey and return of the Garmin activity trackers. The fifth voucher ($30) was posted to families that completed a semi-structured telephone interview post-intervention.
Data collection
The screening, baseline and post-intervention survey data were collected online using SurveyMonkey software. Families received up to three reminder emails/text messages and two reminder phone calls if they did not complete the baseline or post-intervention survey. Throughout the 6-week intervention, families were required to regularly sync their activity tracker data on the Garmin Vivofit Jr (child) app and Garmin Connect (parent) app. Once a week, the research officer logged into the child and parent app accounts to extract daily/weekly step counts and active minutes (i.e. objective activity tracker and app usage data). Post-intervention, a sub-sample of the families participated in a semi-structured telephone interview (15–20 minutes duration) to collect qualitative data on families’ engagement, satisfaction, perceived usefulness and experience with intervention components. The telephone interviews were audio-recorded using an iPhone and transcribed verbatim by a professional transcription service.
Measures
Intervention feasibility was assessed using mixed-methods process evaluation measures. These included online surveys (pre/post-intervention) and semi-structured telephone interviews (at post-intervention) completed by parents. This article reports intervention feasibility in relation to parent/self-reported intervention usage, acceptability, usability, perceived usefulness, use of physical activity self-management strategies and programme influence. The previous article 23 presented data on intervention delivery and fidelity, intervention engagement measured objectively through activity tracker and app usage, as well as intervention effects on moderate-to-vigorous physical activity levels in children and parents.
Usage
Parent-reported usage of Garmin activity trackers and apps was measured in the post-intervention online survey. The parent-reported usage data provided important details on activity tracker wear time (i.e. hours per day, days and weeks), as well as families’ weekly app usage and synching of activity tracker data to the apps. It complements the previously published objective Garmin activity tracker data of active minutes and step counts. 23 Mothers and fathers reported their activity tracker and app usage respectively. In addition, one parent reported the app usage data on behalf of the child(ren). The usage questions (see Supplementary material) were similar to those applied in previous online-delivered physical activity interventions.32–34 For example, parents were asked ‘For how many weeks have you worn the Garmin activity tracker?’ with response options ranging from 1 to 6 weeks. Further, parents were asked ‘On weeks where you wore the Garmin activity tracker, on average how many days per week were you wearing the Garmin activity tracker?’ Response options ranged from 1 to 7 days.
Acceptability
Acceptability of the introductory session was measured in the post-intervention online survey using questions (see Supplementary material) adapted from those used in previous online-delivered physical activity interventions.34–36 Acceptability was assessed using 11 statements rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Rated statements included, for example, ‘The physical activity information was interesting’, ‘The physical activity information was personally relevant’ and ‘Too much physical activity information was provided’. Response options 4 (agree) and 5 (strongly agree) were grouped into a percentage of parents agreeing. In addition, parents were asked: ‘Overall, how much of the physical activity advice sent via text messages did you read?’ using an 8-point Likert scale (1 = all of it, 2 = most of it, 3 = more than half, 4 = about half, 5 = less than half, 6 = not much of it, 7 = nearly nothing, 8 = nothing). Based on data distribution, the response options were grouped into ‘read most’, ‘read about half’ and ‘read less than half’.
Usability
Usability of the Garmin activity tracker and app for parents was measured in the post-intervention online survey using a modified version of the standardised System Usability Scale (SUS). 37 Thirteen usability statements related to the activity tracker and 11 statements concerned the app (see Supplementary material). Statements included, for example, ‘I thought the Garmin activity tracker was easy to use’, ‘I would like to continue to use the Garmin activity tracker frequently in the future’ and ‘I found the Garmin activity Connect app too complex’. Response options included a 4-point Likert scale (0 = strongly disagree to 4 = strongly agree). Response options ‘agree’ and ‘strongly agree’ were collapsed into a percentage of parents agreeing. The standardised SUS has shown high reliability (α = 0.91) when assessed through Cronbach's alpha, 38 and acceptable construct validity (r = 0.70) when measured through Spearman rank correlation. 39
Perceived usefulness
Perceived usefulness of intervention components was assessed in the post-intervention online survey using questions (see Supplementary material) derived from previous online-delivered physical activity interventions.34,40 Parents were asked: ‘How useful were the following programme components in helping you to increase your physical activity over the past 6 weeks?’ Programme components rated included the introductory session, mobile text messages, Garmin Vivofit 3 activity tracker for parents, Garmin Vivofit Jr activity tracker for children, Garmin Connect app for parents, Garmin Vivofit Jr app for children and the family steps challenge log poster. Perceived usefulness was rated by all parents, mothers and fathers using a 5-point Likert scale (1 = not at all useful to 5 = very useful). Based on data distribution, response options were grouped into very/quite useful, somewhat useful and not/little useful.
Use of physical activity self-management strategies
The use of self-management strategies for increasing physical activity was assessed in the pre- and post-intervention online surveys using questions (see Supplementary material) adapted from Saelens et al. 41 Parents were asked ‘How often have you done the following?’ and presented with 16 self-management strategies. Examples included ‘Evaluate how active you are’, ‘Attempting to get family members to be active instead of sedentary’ and ‘Set aside a special time to be active’. Response options for each self-management strategy were 1 = never, 2 = rarely, 3 = occasionally and 4 = often.
Programme influence
Programme influence was examined qualitatively in the semi-structured telephone interviews (15–20 minutes duration) conducted with parents at post-intervention. Prior to each telephone interview, parents were assured that all responses are valued and that their feedback will help improve the Step it Up Family intervention. Recurring themes, categories and sub-categories relating to programme influence were derived from two questions: (1) ‘How do you think the programme has influenced your families’ physical activity levels?’ and (2) ‘Which aspects of the programme did you find helpful to increase your physical activity?’
Sociodemographic data
Sociodemographic data collected in the parent surveys included sex, age (in years), employment status (employed: full-time, part-time and casual; unemployed: home duties, student and retired), education (high: 13 + years, low: 0–12 years), ethnicity (Caucasian, African, Asian; Aboriginal, Torres Strait Islanders and Pacific Islanders; Other) and families’ geographic location (major city, regional, remote and very remote).
Sample size
This was a small-scale, single-arm feasibility study. Based on pragmatic considerations of the feasibility of recruiting whole families and available resources, no formal sample size calculation was performed prospectively. We aimed for a convenience sample of 40 families participating in the intervention to examine the feasibility of delivering this intervention approach in ‘whole families’ (i.e. at least one child aged 6–10 years, mothers and fathers). At post-intervention (6 weeks), 38 families (38 mothers, 33 fathers) completed the online survey which provided the sample size for the quantitative analyses conducted in this study. Of these, a sub-sample of 19 families (17 mothers, 2 fathers) agreed to complete the semi-structured telephone interviews at post-intervention. This convenient sub-sample was used for the qualitative analyses.
Data analyses
Most previous family-based physical activity interventions have predominantly involved mothers as the parent representative,10,11 whilst few interventions have also involved fathers.12,13 A novelty of the Step it Up Family programme was that it actively targeted and implemented the intervention in whole families including mothers and fathers. To identify valuable insights and contributions from both parents, the feasibility findings were analysed separately for mothers and fathers. For the quantitative analyses, categorical data were presented using counts and percentages, and continuous data were presented using means and SDs. Chi-square tests and independent t-tests were used to assess gender differences in sociodemographic characteristics. Chi-square tests were also used to assess parental differences in intervention acceptability, usability and perceived usefulness. Wilcoxon signed-rank test was used to compare pre–post-intervention differences in mothers’ and fathers in relation to the use of physical activity self-management strategies. The quantitative analyses were performed in IBM SPSS Statistics (version 26.0). For the qualitative analysis of the Step it Up Family programme influence, audio recordings of the semi-structured telephone interviews with 19 families were analysed using qualitative content analysis 42 to identify emergent themes, categories and sub-categories. The qualitative analyses were carried out in Microsoft Excel (version 2201). A pen profile, which is an increasingly utilised technique to present analysed text data in a diagram, 16 was constructed based on themes identified in relation to programme influence (Figure 1).

Participants flow.
Results
Participant flow
The participant flow is shown in Figure 1. Eighty-one families completed the screening survey and were assessed for eligibility. Of these, one family was excluded because they did not meet the eligibility criteria. Four families were excluded because they did not provide written parental and child consent to participate in the study. Furthermore, 36 families were excluded because they either did not complete the baseline survey, did not set up their activity trackers and app software or withdrew from the study prior to intervention commencement. Overall, 40 families including 58 children (50% girls), 39 (98%) mothers and 33 (83%) fathers participated in the Step it Up Family programme. 23 Of these, 38 families completed the post-intervention survey (95% family retention) and 19 families completed the post-intervention telephone interview.
Baseline data
Sociodemographic characteristics of Step it Up Families at baseline is presented in Table 1. Most families (80%) lived in a regional area; the remainder (20%) lived in a major city. Over half of the families (58%) had one child enrolled in the programme, other families (40%) had two children enrolled and one family had three children enrolled. The mean (SD) ages of children, mothers and fathers were 8.0 (1.5) years, 37.8 (4.3) years and 41.2 (6.1) years, respectively. Of the parents, 71% had 13 + years of education, 82% were employed and 99% were Caucasian. There were no significant differences in baseline characteristics between those lost to follow-up and those retained (all p > 0.05).
Usage
During the 6-week intervention period, the mean (SD) number of self-reported weeks the Garmin activity tracker was worn was 5.8 (0.7) in mothers and 5.7 (0.9) in fathers. The mean (SD) number of days per week the Garmin activity tracker was worn was 6.9 (0.4) in mothers and 6.9 (0.4) in fathers. Further, the mean (SD) number of hours per day the Garmin activity tracker was worn was 21.1 (5.2) in mothers and 22.6 (4.1) in fathers. Mostly, family members used the Garmin apps 2–6 times per week (57% mothers, 52% fathers, children 42%). The majority of parents (66%) synched Garmin activity tracker data to the Garmin apps 2–6 times per week. In contrast, fewer parents (17%) synched the activity tracker data daily.
Acceptability
Acceptability of intervention components reported by parents is presented in Table 2. Most parents found the physical activity information received during the introductory session interesting (80% mothers, 76% fathers), credible (83% mothers, 86% fathers), easy to understand (83% mothers, 90% fathers) and personally relevant (69% mothers, 69% fathers). Most mothers (69%) and about half of the fathers (52%) agreed that they have used the physical activity information to become more active. Most mothers (80%) and about half of fathers (52% said they read most of the motivational and educational text messages received during the 6-week intervention.
Acceptability and usability of intervention components and resources reported by parents.

Parents responded on a 5-point Likert scale for each statement ranging from 1 = strongly disagree to 5 = strongly agree. The response options ‘4 = agree’ and ‘5 = strongly agree’ were grouped into a percentage of parents agreeing (% agreeing).
Usability
Usability of intervention components reported by parents is presented in Table 2. Most parents (91% mothers, 93% fathers) thought the Garmin Vivofit 3 activity tracker was easy to use, and they found its various features were well-integrated). Further, most parents (91% mothers, 82% fathers) felt very confident using the activity tracker. The majority of mothers (87%) and nearly two-thirds of fathers (62%) stated they would like to continue to use the Garmin activity tracker frequently in the future. Most mothers (80%) and two-thirds of fathers (66%) found the Garmin activity comfortable to wear. Also, most mothers (83%) and two-thirds of fathers (66%) agreed that the activity tracker helped them to increase their physical activity.
In terms of the Garmin Connect app, most parents (87% mothers, 93% fathers) thought the app was easy to use. Furthermore, most parents (89% mothers, 83% fathers) liked the presentation and layout of the app. Most mothers (77%) but fewer fathers (55%) stated they would like to continue using the Garmin Connect app frequently in the future.
Perceived usefulness
Table 3 presents the perceived usefulness of intervention components for increasing physical activity reported by parents. Most mothers (87%) and two-thirds of fathers (66%) found the Garmin Vivofit 3 activity tracker for parents very/quite useful for increasing physical activity. Furthermore, most parents (91% mothers, 79% fathers) found the Garmin Vivofit Jr activity tracker worn by their children very/quite useful for increasing physical activity. Moreover, most parents found the Garmin Connect app for the parents as well as the Garmin Vivofit Jr app for the children very/quite useful for increasing physical activity. However, few parents (11% mothers, 7% fathers) considered the family steps challenge log poster very/quite useful. Also, less than a third of parents (29% mothers, 21% fathers) found the educational and motivational mobile text messages very/quite useful for increasing physical activity. About half of mothers (49%) and a third of fathers (35%) considered the introductory session very/quite useful for increasing physical activity.
Perceived usefulness of intervention components for increasing physical activity reported by parentsa.

Parents responded on a 5-point Likert scale for each program component ranging from 1 = not at all useful to 5 = very useful. The response options were collapsed into ‘1 = Not/little useful’, ‘2 = Somewhat useful’ and 3 = Very/quite useful’.
Use of physical activity self-management strategies
Pre–post-intervention differences in the use of physical activity self-management strategies by mothers and fathers are presented in Table 4. The physical activity self-management strategies assessed included behavioural and cognitive strategies. At post-intervention, both parents had significantly increased the use of behavioural strategies such as ‘Evaluate how active you are’, ‘Attempt to get family members to be active instead of sedentary’ and, ‘Schedule physical activity into your daily plan’. Fathers (but not mothers) also increased the strategies ‘Post cues for being active’ and ‘Reward yourself for being active’. In addition, both parents had significantly increased the use of cognitive strategies such as ‘Set physical activity goals’, ‘Praise your child for doing physical activity’ and ‘Choose convenient physical activities’. Mothers (but not fathers) also increased the strategies ‘Set aside a special time to be active’ and ‘Say positive things to yourself about physical activity’.
Pre–post-intervention differences in physical activity self-management strategies used by mothers and fathers.

Parents responded on a 4-point Likert scale with the response options being 1 = Never, 2 = Rarely, 3 = Occasionally and 4 = Often. Bold p-values denote a significant difference from pre to post intervention.
Programme influence
The Step it Up Family programme influence reported by parents at post-intervention is shown in Figure 2. Parents (n = 12) repeatedly reported that the Step it Up Family programme increased their awareness of physical (in)activity in the family: We did realise how unfit we are, but we didn’t realise how bad it was. [Mother 16]
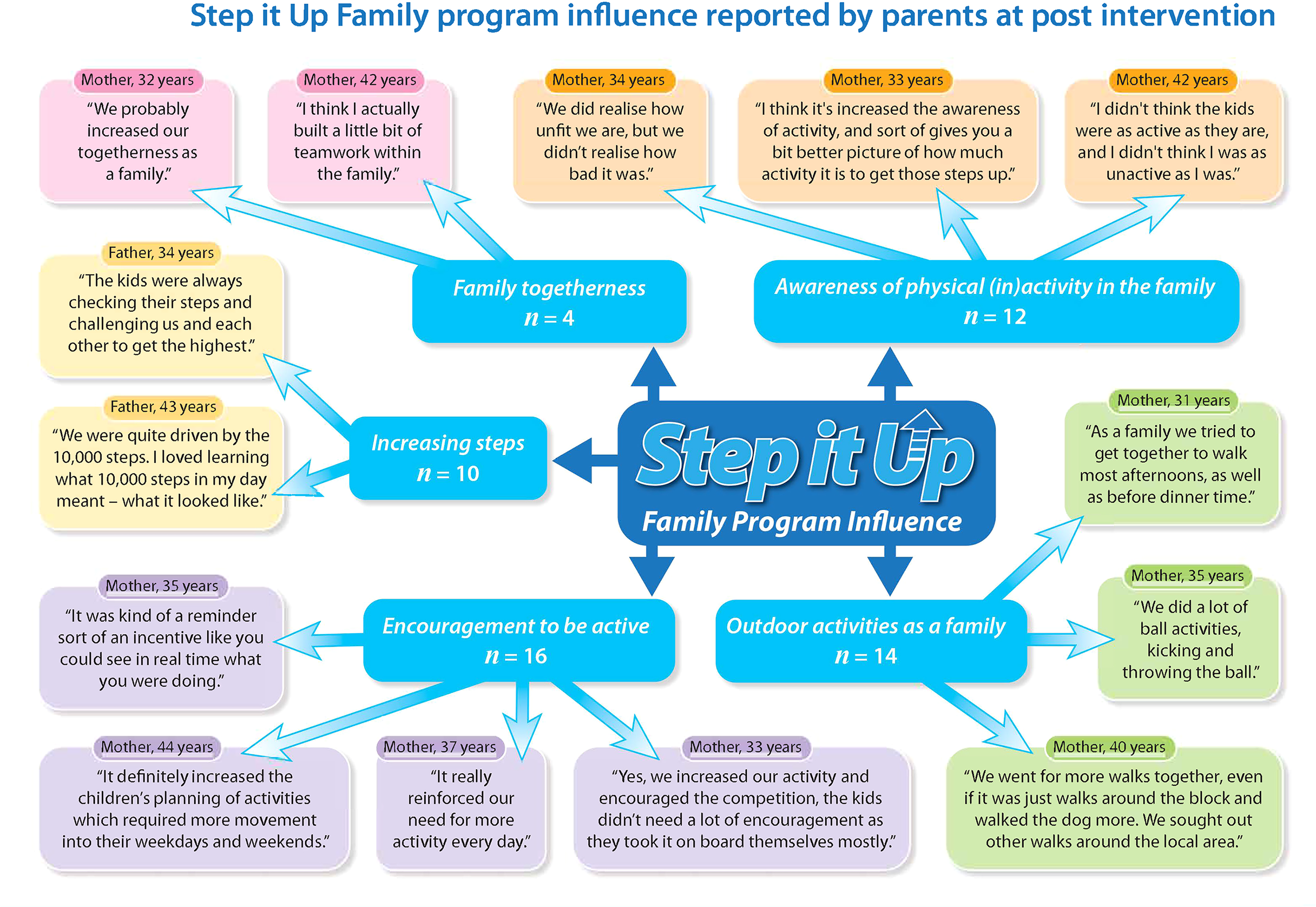
Step it Up Family programme influence reported by parents at post-intervention.
Families (n = 16) noted that the Step it Up Family programme encouraged their families to be active: Yes, we increased our activity and encouraged the competition, the kids didn’t need a lot of encouragement as they took it on board themselves mostly. [Mother 12]
Families (n = 10) further reported how the Step it Up Family programmw helped them to increase the steps: The kids were always checking their steps and challenging us and each other to get the highest (Father 10)
Families (n = 14) stated they did more outdoor physical activities as a family, such as walking (n = 10), cycling (n = 2), doing ball games (n = 3) and playing actively at the beach (n = 2). We went for more walks together, even if it was just walks around the block and walked the dog more. We sought out other walks around the local area. (Father 10)
Some families (n = 4) also noted that the Step it Up Family programmw promoted family togetherness: We probably increased our togetherness as a family. [Mother 64]
Discussion
This study examined the feasibility of using activity trackers and apps in an intervention to increase physical activity in whole families. Overall, the process data showed that families’ reported usage of the Garmin activity trackers was high (i.e. nearly 24/7 during the 6 weeks intervention period). Families also used the Garmin apps designed for children and parents regularly (i.e. mostly 2–6 times per week). Further, most mothers and half of fathers read the motivational mobile text messages. Usability of the Garmin activity trackers and apps was also rated high, as well as acceptability of the information provided in the introductory session. Most mothers and fathers rated the perceived usefulness of the Garmin activity trackers and apps high for increasing physical activity in children and parents. In both parents, the use of physical activity self-management strategies had significantly increased from pre to post-intervention (6 weeks). In post-intervention telephone interviews, families repeatedly noted that the Step it Up Family programmw had increased their awareness of physical (in)activity in the family, provided encouragement to be active (particularly by increasing steps) and promoted outdoor activities as a family.
The most popular intervention component in the Step it Up Family programme were the Garmin activity trackers and apps used by children and parents. This was reflected in the high ratings regarding usage, usability and perceived usefulness. The need to charge activity trackers is often considered burdensome by participants. 43 The Garmin Vivofit activity trackers used in this study required no charging, and they were waterproof. Furthermore, they displayed the numbers of steps active minutes in real time. Additionally, the Garmin Vivofit Jr worn by the children displayed, in the form of a circle, whether a child reached the recommended 60 minutes of physical activity per day. Each of these design features of the Garmin activity trackers may have contributed to their high usage throughout the 6-week intervention period. Worth noting is that parents’ self-reports of high Garmin activity tracker usage (i.e. activity tracker worn on average 5.8 weeks) corresponded with the objectively measured activity tracker usage data (i.e. step recordings on average 38 days out of 42 intervention days) we published earlier on this study. 23
Usability ratings of the Garmin Vivofit 3 activity tracker and app by parents were high overall, with no significant differences between parents. Except, significantly more mothers (89%) than fathers (62%) said they would like to continue to use the Garmin activity tracker frequently in the future. Perhaps the activity tracker design was less appealing to fathers in whom another device model would encourage long-term usage. It may also be that using an activity tracker to increase steps appeals more to mothers than fathers. This is in line with other research 44 showing that activity trackers are more popular in women than men.
Most mothers and fathers found the Garmin activity trackers and apps highly useful for increasing physical activity in children and parents. In contrast, very few parents considered the family steps challenge log poster useful for increasing physical activity. Also, whilst most parents read the motivational mobile text messages, less than a half of parents found them useful for increasing physical activity. These findings raise the question of whether using an activity tracker and app alone would be sufficient for promoting physical activity in families. Currently, there are two large-scale activity tracker programmes available in Australia, that is, 10,000 Steps Australia 45 and Heart Foundation Walking. 46 To date, these programmes have not been specifically targeted and delivered to families. Given the positive findings in this study, 23 it is worth exploring the feasibility and efficacy of delivering the existing 10,000 Steps Australia and Heart Foundation Walking programmes in families.
The use of physical activity self-management strategies had significantly increased in both mothers and fathers at post-intervention. This is an important positive finding as self-management strategies, also referred to as behaviour change techniques, 28 have repeatedly shown to significantly increase physical activity behaviour.47,48 A key component in the Step it Up Family programme was to encourage the use of physical activity self-management strategies within the family unit, in particular self-monitoring and goal setting (regarding steps, active minutes), social support (e.g. praising family members for reaching step goals, facilitating outdoor walks), role modelling (e.g. being physically active in front of the child or together as a family). Our study findings suggest that the Step it Up Family programme was successful in helping parents to use these self-management strategies more frequently.
In post-intervention telephone interviews, parents repeatedly reported that the Step it Up Family programme had increased their awareness of physical (in)activity in the family. This is consistent with the findings from a similar study conducted in the UK (i.e. Families Reporting Every Step to Health/FRESH) 12 which examined the use of pedometers to increase physical activity in the whole family. In the FRESH study, parents also stated that the programme made their family more aware of the amount of physical activity they do, and that it encouraged the family to engage in more physical activities. 12
Strengths, limitations and future research
This study informs the field of family-based physical activity interventions by addressing important research gaps. Few family-based physical activity interventions have been delivered online 10 and utilised activity trackers and apps in young children (6–10 years). 43 Further, few studies12,13 have specifically targeted whole families (mothers, fathers, children) in a physical activity intervention. Other strengths of this study include the use of proven health behaviour change techniques28,29 and theories,30,31 and the assessment of process evaluation outcomes in both mothers and fathers. The study also has several limitations that need to be noted. Despite its innovation and promising findings, results from this feasibility study are limited by the reliance on solely parent/self-reported measurement (which is prone to overreporting and social desirability bias), a relatively small sample size (n = 40 families comprising 130 study participants), a short intervention period (6 weeks) and lack of a control group. Future research may address these limitations by testing the feasibility, uptake and efficacy of an activity tracker and app intervention in a larger, more diverse family population (including single parents, same-sex parents, grandparents), with a longer-term intervention period (e.g. 3 months) and using randomised controlled trial and/or ecological trial designs.
Conclusions
In conclusion, the high usage, acceptability, usability and perceived usefulness ratings reported in this study by both parents are encouraging and demonstrate the feasibility of using activity trackers and apps to increase physical activity in whole families, at least in the short term. The significant increase in the use of physical activity self-management strategies in both parents suggests that their application works well in an activity tracker and app-based physical activity intervention for families. Our findings support the implementation of the Step it Up Family programme in a larger, randomised controlled trial to determine its long-term efficacy. Additionally, further testing is needed in more diverse family populations including single parents, same-sex parents and grandparents, as well as families with heterogenous sociodemographic characteristics (e.g. education, income, ethnicity and urbanisation).
Supplemental Material
sj-docx-1-dhj-10.1177_20552076221129083 - Supplemental material for Feasibility of using activity trackers and apps to increase physical activity in whole families: The Step it Up Family intervention
Supplemental material, sj-docx-1-dhj-10.1177_20552076221129083 for Feasibility of using activity trackers and apps to increase physical activity in whole families: The Step it Up Family intervention by Stephanie Schoeppe, Jo Salmon, Susan Williams, Deborah Power, Kim Waters, Stephanie Alley, Amanda L. Rebar, Melanie Hayman, Mitch J Duncan and Corneel Vandelanotte in Digital Health
Footnotes
Acknowledgements
The authors would like to thank research assistant Emma Power for her assistance with participant recruitment. Further, we like to thank all families who participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
SS, CV, JS and SW conceptualised and designed the study and SA, ALR, MH and MJD contributed to the development of the intervention. DP conducted the recruitment, intervention, data collection and data cleaning, with input from SS, CV, JS and SW. KW analysed the telephone interview data with supervision from SS. SS analysed the survey data and drafted and wrote the manuscript. All authors were involved in the interpretation of data and critically revising the manuscript, and they read and approved the final manuscript.
Ethical approval
Ethical approval for the study was received from the Central Queensland University Human Ethics Committee in May 2017 (H17/03-041).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a New Staff Research Grant by the Central Queensland University and an Advance Queensland Women's Academic Fund by the Queensland Government. SS is supported by an Early Career Fellowship from the National Health and Medical Research Council of Australia (GNT1125586) and was supported by a Postdoctoral Fellowship from the National Heart Foundation of Australia (Award ID 101240). MJD is supported by a Career Development Fellowship (APP1141606) from the National Health and Medical Research Council of Australia. JS is supported by an Investigator Grant Leadership Level 2 (APP1176885) from the National Health and Medical Research Council of Australia. CV is supported by an Australian Research Council Future Fellowship (FT210100234).
Guarantor
SS.
Informed consent
Informed participant consent was obtained online from both mothers and fathers, and one parent provided consent on behalf of the participating children.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.