
Abstract
Objective
To investigate the value of a SnapECG monitoring in diagnosing arrhythmias compared with the conventional management.
Methods
In the first phase, the SnapECG and 12-lead electrocardiogram (ECG) were simultaneously adopted to detect arrhythmias in 439 hospitalized patients. The accuracies of the SnapECG in detecting different arrhythmias were assessed. In the second phase, 62 patients with palpitations were randomized to receive the SnapECG monitoring or conventional management for 3 months. The diagnosis rate, time of diagnosis, episodes before diagnosis, associated expenses, and scores of the modified European Heart Rhythm Association (EHRA), Self-rating Anxiety Scale (SAS), and the 36-item short-form health survey questionnaire (SF-36) were compared between groups.
Results
In the first phase, the SnapECG monitoring showed a sensitivity of 83.55% and specificity of 96.79% in identifying tachyarrhythmias, and a sensitivity of 95.29% and specificity of 97.54% in identifying bradyarrhythmias. In the second phase, 1642 ECGs were recorded by the SnapECG, among which 290 abnormal ECGs were identified. Compared with the conventional management, the SnapECG monitoring increased the diagnosis rate of symptomatic arrhythmias (70.97% vs. 19.35%, P < 0.05), shortened the time of diagnosis (48.26 ± 36.78 days vs. 71.45 ± 30.01 days, P < 0.05) and consequently reduced the episodes of symptomatic arrhythmias prior to establishing diagnosis. The scores of modified EHRA, SAS, SF-36 significantly improved at 3-month compared with their baseline levels in the SnapECG group.
Conclusions
Remote monitoring with the SnapECG can achieve early diagnosis of symptomatic arrhythmias. However, its sensitivity in identifying P-wave-related arrhythmias warrants further improvement.
Introduction
As one of the most common cardiovascular diseases, arrhythmias are important causes of patient mortality and morbidities.1,2 Twelve-lead electrocardiogram (ECG) and 24-h Holter monitors are conventional methods to detect arrhythmias. However, due to short duration of monitoring, normal ECG and Holter reports cannot effectively exclude arrhythmias presenting outside the detection period,3,4 and positive reports may not identify the true symptom-related arrhythmias.
The development of telecommunication technologies has led to the intervention of novel remote monitoring devices such as smartphones 5 and wearables, 6 which enable single-lead ECG recordings at any time and any place. 7 These devices have the potential to document paroxysmal arrhythmias associated with clinical symptoms. 8
This study aimed to explore the accuracy of a handheld electrocardiograph (SnapECG) to diagnose common arrhythmias using the 12-lead ECG as gold-standard control. We also investigated the value of using the SnapECG to diagnose symptom-related arrhythmias in the outpatient setting compared with the conventional management.
Methods
Subjects
This study complied with the Declaration of Helsinki and was registered at www.clinicaltrials.gov (Unique Identifier: NCT03396133). The research protocol was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (Approval Number2018-SR-038), and written informed consent for participation in this study was obtained from each patient.
The study was performed in 2 phases. In the first phase, 439 inpatients presenting with common tachy- or bradyarrhythmias were successively enrolled. In the second phase, 87 outpatients with suspected arrhythmias (e.g. palpitations, chest discomfort) were successively screened if they had experienced at least one Holter examination within the latest 2 weeks but no arrhythmia diagnosis was established. Patients who had critical illness, dyskinesia, complications that interfere with the holding of the SnapECG device, or those who refused to participate were excluded in both phases.
Study design
In the first phase, the SnapECG and 12-lead ECG recordings were simultaneously collected in patients presenting with persistent arrhythmias. All ECGs were interpreted blindly at random order by a designated senior cardiologist without knowing the patients’ information. The sensitivity and specificity of the SnapECG for the diagnosis of common cardiac arrhythmias were calculated by using the interpretation of the 12-lead ECG as the gold-standard control.
In the second phase, eligible patients were randomly assigned into the SnapECG monitoring or conventional management groups using randomized numbers kept by an investigator blinded to the patients’ recruitment. Those in the SnapECG group were instructed to perform a detection at 20:00–21:00 daily or at least every other day and transmit the ECG (longer than 2 min) to a designated cardiologist for 3 months. Additional ECG recordings were required once arrhythmia-related symptoms were suspected. The SnapECG recordings were transmitted to the investigators through a mobile application (app) via the Internet. The designated cardiologist was responsible for interpreting all transmitted ECGs. Patients in the control group received conventional management at the discretion of the attending physicians, including the 12-lead ECG or 24-h Holter examination. The patients’ medical data were collected and their clinical information were followed up for 3 months. Patients were recommended to certain treatment once their symptom-associated arrhythmias were diagnosed. However, no anti-arrhythmic agents were allowed to be administered before their diagnoses for the symptom-associated arrhythmias were established.
In both groups, the specific symptoms, number of symptomatic episodes, duration of each episode, and medical expenses for arrhythmia-related symptoms were recorded. The diagnosis rate of symptom-related arrhythmia, days from enrollment to diagnosis (the time for diagnosis was regarded as 90 days if a patient's diagnosis had not been reached at 3-month follow-up), episodes before establishing diagnosis, related medical expenses, and scale scores including modified European Heart Rhythm Association (EHRA), Self-rating Anxiety Scale (SAS), Patient Health Questionnaire (PHQ)-9, SF-36 physiological component summary (PCS), and SF-36 mental component summary (MCS) were compared between the two groups.
Characteristics of the SnapECG device
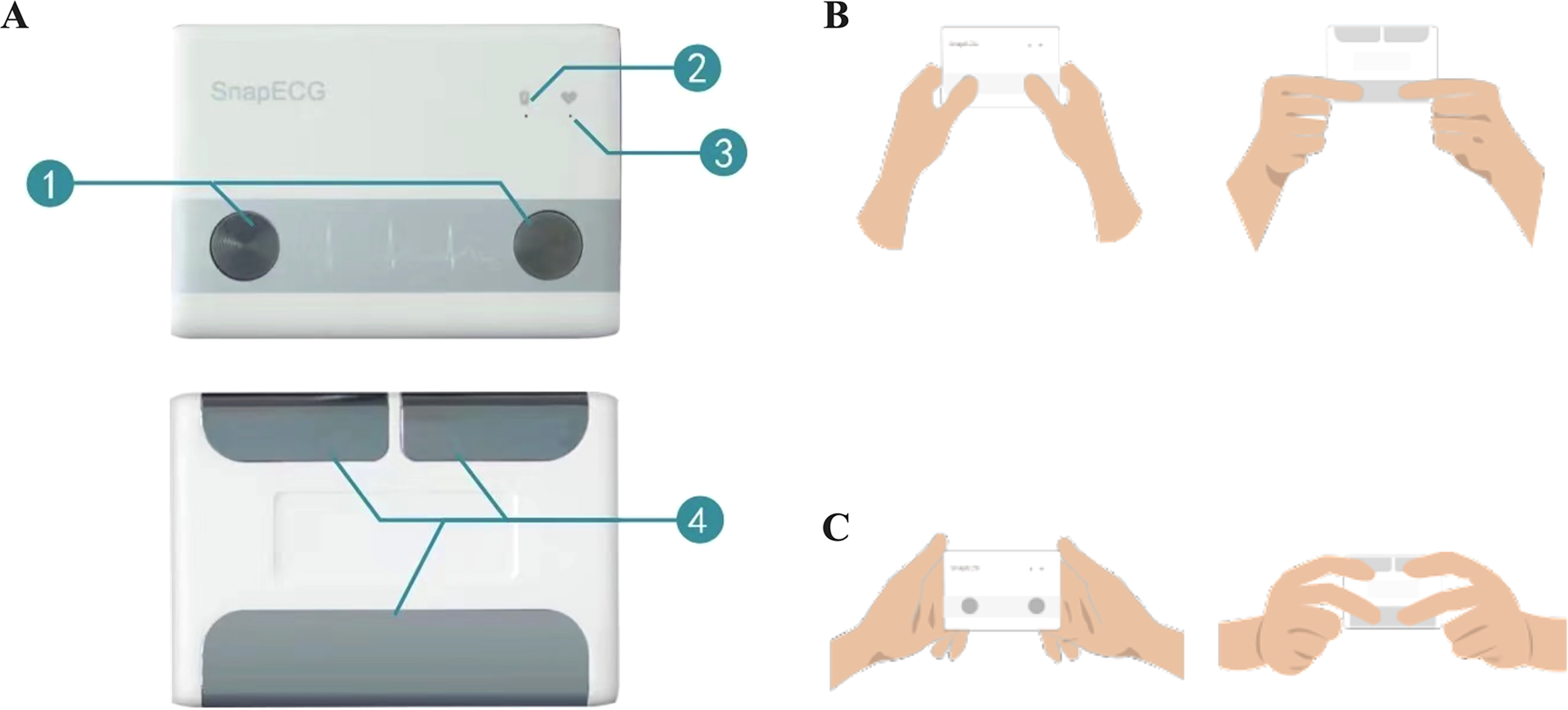
The SnapECG (Nanjing Xijian Information Technology Co.,Ltd Nanjing, China) is a chargeable, portable, ambulatory, and single-lead recorder that collects users’ electrocardiosignals (Figure 1A). There are two methods available to detect the electrocardiosignals (Figure 1B, 1C), and the Method 1 was required to be adopted in this study. The recording time of SnapECG can be set as 30 s, 1, 3, or 5 min. Patients in the SnapECG group were instructed to perform detections longer than 2 min (3 or 5 min). The electrocardiosignals can be transmitted to an app on patients’ smartphones via Bluetooth, and the app has the capability to generate and display ECG waveforms, store data, and generate and send portable document format (PDF) files to the designated cardiologist via the Internet.
Definitions of the arrhythmias
The arrhythmias were defined referring to the American Heart Association/American College of Cardiology/Heart Rhythm Society (AHA/ACC/HRS) recommendations for the standardization and interpretation of the electrocardiogram 9 and the European Heart Rhythm Association (EHRA) consensus on the management of asymptomatic arrhythmias. 10 Specifically, sinus tachycardia, sinus arrhythmia, sinus bradycardia, and single ectopic beat were all considered arrhythmias. Besides, the complete left and right bundle branch blocks were diagnosed if the QRS morphology followed that in Lead I of the 12-lead ECG described in the corresponding definitions.
Statistical analysis
As a pilot study, we set a sample size of 420 cases (35 in each arrhythmia) for the first phase. PASS version 15.al0 (NCSS, LLC., Kaysville, UT, USA) was used to calculate the sample size for the second phase: a two-tail α = 0.05 and β = 0.20 were set for the analysis. The diagnosis rates of the symptom-associated arrhythmias were set as 15% for the control group, and 50% for the SnapECG group referring to the historical data, 11 and the sample allocation ratio was set as 1.0. As a result, 29 cases were required for each group. Considering a drop-out rate of 5%, at least 31 cases were required for each group.
SPSS version 26.0 (SPSS, Inc., Chicago, IL, USA) was used for statistical analysis. Continuous variables conformity to normal distribution are expressed as mean ± standard deviation (SD), non-normally distributed data are expressed as median (interquartile ranges), and categorical variables are expressed as frequencies or percentages. The independent Student t test, Mann-Whitney U test, or Chi-square test was used for the comparison between groups as appropriate. Paired sample t test or Mann-Whitney U test was used to evaluate intragroup differences. A 2-tailed value of P < 0.05 was considered statistically significant for all analyses.
Results
Sensitivity and specificity of the SnapECG monitoring in diagnosing common arrhythmias
In the first phase, a total of 439 cases of arrhythmia ECGs were collected, including 231 cases of tachyarrhythmias and 208 cases of bradyarrhythmias (Table 1, Supplementary Figure 1A: a, b, c).
Sensitivity and specificity of the diagnosis by the SnapECG for common arrhythmias.

Based on the interpretation of 12-lead ECG, the overall sensitivity and specificity of the SnapECG monitoring in the diagnosis of common tachyarrhythmias were 83.55% and 96.79%, respectively. The overall sensitivity and specificity of the SnapECG monitoring in the diagnosis of common bradyarrhythmias were 87.50% and 99.13%, respectively. The SnapECG monitoring showed poor sensitivity in the diagnosis of atrial tachycardia (AT), atrial flutter (AFL) (Supplementary Figure 1B: a-1, a-2, b-1, b-2), and first-degree or second-degree atrioventricular block (55%, 24%, 67%, and 44%, respectively) (Table 1, Supplementary Figure 1B: c-1, c-2).
The positive predictive values (PPV), negative predictive values (NPV), positive likelihood ratios (PLR), negative likelihood ratios (NLR), overall accuracy, and receiver operating characteristic curves (ROC) of the diagnoses by SnapECG monitoring for common arrhythmias are shown in Supplementary Table 1 and Supplementary Figure 2 respectively.
Diagnosis of symptom-related arrhythmias
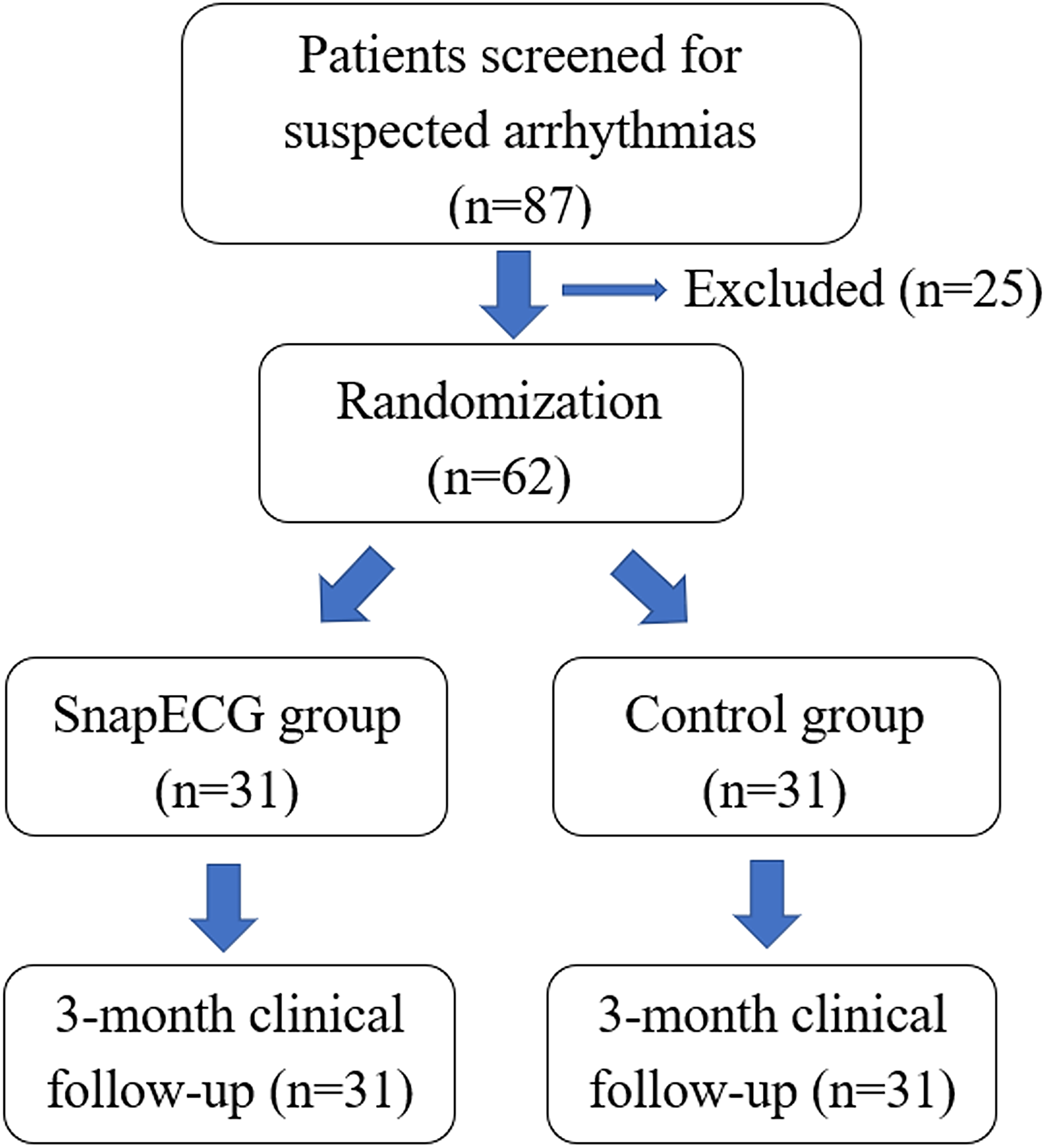
In the second phase, 87 patients were screened, among which 62 were successfully randomized and 25 were excluded for refusing to participate in the study. All the randomized patients completed 3-month clinical follow-up (Figure 2). The baseline clinical characteristics, as well as the baseline scale scores, were comparable between the SnapECG and the control groups (Table 2).
Baseline characteristics of the recruited patients.
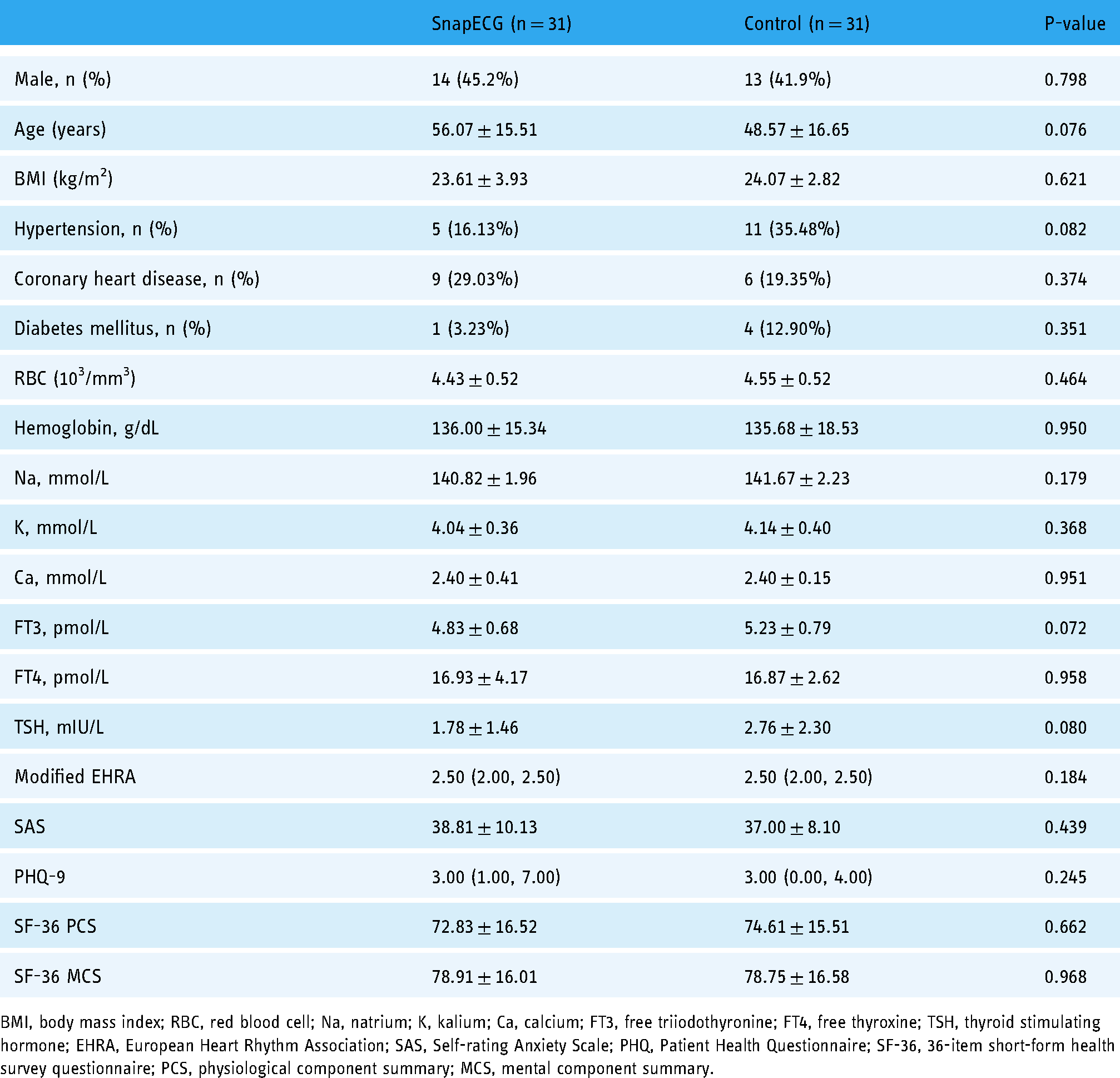
BMI, body mass index; RBC, red blood cell; Na, natrium; K, kalium; Ca, calcium; FT3, free triiodothyronine; FT4, free thyroxine; TSH, thyroid stimulating hormone; EHRA, European Heart Rhythm Association; SAS, Self-rating Anxiety Scale; PHQ, Patient Health Questionnaire; SF-36, 36-item short-form health survey questionnaire; PCS, physiological component summary; MCS, mental component summary.
During the 3-month follow-up, 1642 SnapECG recorded ECGs were transmitted by the patients, among which 1458 were recorded at 20:00–21:00 as required by the study protocol, and 184 were recorded while the patients experienced symptoms (Figure 3; Supplementary Figure 1A:d). There were 290 abnormal ECGs, including 218 asymptomatic arrhythmias, and 92 symptom-related arrhythmias (Figure 3). Asymptomatic arrhythmias included nine (4.13%) cases of sinus tachycardia, sixty-four (29.39%) cases of sinus arrhythmia, twenty-eight (12.84%) cases of sinus bradycardia, thirty-three (15.14%) cases of premature atrial contraction, fifteen (6.88%) cases of AT or supraventricular tachycardia (SVT), eighteen (8.26%) cases of AF, and fifty-one (23.39%) cases of premature ventricular contraction. By comparison, symptomatic arrhythmias included twenty-four (26.09%) cases of sinus arrhythmia, twenty-three (25.00%) cases of premature atrial contraction, nineteen (20.65%) cases of AT or SVT, fifteen (16.30%) cases of AF, and eleven (11.96%) cases of premature ventricular contraction (Figure 4).


In the control group, each patient underwent 1 to 5 ECG examinations during the follow-up period. As a result, 66 ECGs were performed. However, 55 out of the 66 (81.8%) ECGs were not performed during the episodes of the symptoms. Besides, a single 24-h Holter ECG was performed in 9 of the 31 patients. Finally, 6 patients were diagnosed with symptom-related arrhythmias by the end of follow-up. Among them, 3 were diagnosed by 12-lead ECG and another 3 by 24-h Holter examination.
Comparing the two groups, 70.97% of the patients in the SnapECG group were diagnosed with symptom-related arrhythmias versus 19.35% in the control group (P < 0.01). The time of diagnosis in the SnapECG group was significantly shorter than that in the control group (48.26 ± 36.78 days vs. 71.45 ± 30.01 days, P < 0.05). The number of the symptomatic arrhythmia episodes prior to diagnosis in the SnapECG group was significantly less than that in the control group [1.00 (0.00, 3.00) versus 4.00 (2.00, 6.00), P < 0.01]. The related medical expenses in the SnapECG group were lower than those in the control group, though without statistical significance (1248.33 ± 656.86 Yuan vs. 1679.81 ± 1102.13 Yuan, P > 0.05) (Table 3).
Comparison of the diagnosis efficacy between the two groups at 3-month follow-up.

Expenses include the costs of the SnapECG devices.
Effect of SnapECG diagnosis on the scale scores
In the SnapECG group, comparison of scale scores at baseline and at 3-month follow-up showed significant improvement in the modified EHRA score [2.50 (2.00, 2.5) versus 2.00 (2.00, 2.50); P < 0.05], SAS score (38.81 ± 10.13 vs. 33.39 ± 5.98, P < 0.05), SF-36 PCS score (72.83 ± 16.52 vs. 81.34 ± 9.97, P < 0.05) and SF-36 MCS score (78.91 ± 16.01 vs. 86.17 ± 11.35, P < 0.05). In the control group, SAS score (37.00 ± 8.10 vs. 34.01 ± 5.58, P > 0.05), PHQ-9 score [3.00 (0.00, 4,00) versus 1.50 (1.00, 2.00), P > 0.05), SF-36 PCS score (74.61 ± 15.51 vs. 76.87 ± 14.93, P > 0.05) and SF-36 MCS score (78.75 ± 16.58 vs. 80.03 ± 14.93, P > 0.05) were not statistically different at baseline and at 3-month follow-up (Table 4).
Comparison of scale scores at baseline and 3-month follow-up.

EHRA, European Heart Rhythm Association; SAS, Self-rating Anxiety Scale; PHQ, Patient Health Questionnaire; SF-36, 36-item short-form health survey questionnaire; PCS, physiological component summary; MCS, mental component summary. P1, Comparison of SnapECG group at baseline and 3-month follow-up; P2, Comparison of Control group at baseline and 3-month follow-up; P3, Comparison between SnapECG and Control groups at baseline; P4, Comparison between SnapECG and Control groups at 3-month follow-up.
There were no significant differences in modified EHRA score [2.00 (2.00, 2.50) versus 2.00 (1.50, 2.50), P > 0.05], SAS score (33.39 ± 5.98 vs. 34.01 ± 5.58, P > 0.05), PHQ-9 score [2.00 (0.00, 5.00) versus 1.50 (1.00, 2.00), P > 0.05), the SF-36 PCS score (81.39 ± 12.33 vs. 76.87 ± 14.93, P > 0.05) and MCS score (86.17 ± 11.35 vs. 80.03 ± 16.91, P > 0.05) between the two groups at 3-month follow-up (Table 4).
Discussion
The time delay from experiencing symptomatic arrhythmias to seeking medical attention for patients is mainly attributed to the inconsistent locations, frequency, and duration of these paroxysmal arrhythmia episodes. 12 Conventional diagnostic methods (12-lead ECG, 24-h Holter, etc.) often fail to timely capture symptom-related arrhythmias. Although the popularization of the 24-h Holter has improved the detective rate of arrhythmia to certain extent, patients with suspected arrhythmia still lack established ECG evidence because of infrequent symptoms, and others could not be diagnosed for months to years due to atypical symptoms. 10
In this study, a new-type remote ECG monitoring system named SnapECG was innovated and adopted, providing physicians with a tool for remote consultation and rapid real-time diagnosis of arrhythmias. The data acquisition system of SnapECG includes a 16-bit analog-to-digital converter (ADC), which allows it to detect a minimal signal intensity of 50μV. The SnapECG follows the international standard of IEC 60601-2-47 and the Chinese standard of YY 0885-2013, and was approved by Shenzhen Huatongwei International Inspection Co., Ltd (No: TRS17090169).
To improve the signal quality and waveform stability, three electrodes, instead of two electrodes as in the competing device, 13 were designed for SnapECG. At the same time, the electrodes are produced with a large surface area to ensure contact stability and quality, and improve the convenience and stability of handheld for elderly patients. Besides, a corresponding algorithm was designed to stabilize the baseline of ECG, filter out the interference waveforms, and maximally maintain the low amplitude waveforms and waveform features.
To ensure rapid real-time diagnosis of the arrhythmias, only three steps were required before the cardiologist received the ECG waveforms. 1) Patients were instructed to use the SnapECG to detect electrocardiosignals immediately when the suspected symptoms, such as palpitation, presented at anytime and anywhere. 2) The recorded ECG signals were transmitted instantly to the patient's mobile app via Bluetooth, and a time-labeled ECG acquisition data was generated simultaneously. 3) The collected ECG data were automatically or manually uploaded by the patient in the preset mode and transmitted to the hospital platform or the doctor's mobile app through the Internet.
In the first phase, we found that the overall sensitivity and specificity of the SnapECG monitoring in diagnosing common tachyarrhythmias were 83.6% and 96.8%, and the overall sensitivity and specificity of the SnapECG monitoring in diagnosing common bradyarrhythmias were 87.5% and 99.1%, respectively. According to the analysis of various arrhythmias, the diagnosis by SnapECG monitoring was highly specific for bradyarrhythmia, up to 100%. In contrast, the sensitivity for some arrhythmias needs to be improved, especially those related to P waves, such as AT, AFL, Ι°, and ΙΙ° atrioventricular block (AVB) (Supplementary Figure 1B: a1-a2, b1-b2). As the diagnosis of AF depends on the disappearance of the P wave and the irregular interval of the R-R waves, which is different from other atrial arrhythmias’ characteristics, the sensitivity for atrial fibrillation was up to 100%. However, 26 cases of other arrhythmias (PAC, AT or AFL, ΙΙ° AVB, sinus tachycardia, and sinus arrhythmia) were misdiagnosed as AF (Supplementary Figure 1B: c1-c2), resulting in its decreased diagnostic specificity (84.97%). The possible reasons are as follows: (i) the collected ECG signals were too weak to create clear atrial-related waves from the SnapECG; and (ii) during recording ECG, interference waves were generated by external factors which were mistaken for AF waves by the SnapECG.
In the second phase, we found that the SnapECG monitoring significantly improved the diagnosis rate of symptom-related arrhythmias, shortened the time of diagnosis, and consequently decreased the episodes of symptoms prior to establishing diagnosis at 3 months compared with the conventional management. Compared with the baseline scale scores, the modified EHRA, SAS, SF-36 PCS, and SF-36 MCS scores in the SnapECG group significantly improved at 3- month follow-up, indicating an improvement in patients’ symptom, emotion, and quality of life.
The SnapECG monitoring also helped to identify the asymptomatic arrhythmias. Regarding the AF, the atrium loses the ability to contract effectively and patients with poor ventricular function may experience shortness of breath, dizziness, and other symptoms. 14 In contrast, if the ventricles are in normal function when AF occurs, patients can maintain stable cardiac output and avoid significant symptoms unless the heart rate is too fast or slow. Our results showed that the diagnosis by SnapECG monitoring reached a sensitivity of 100% for AF, and by using our study protocol, the SnapECG monitoring could record both symptomatic and asymptomatic AF, and help to initiate early intervention to reduce the risk of stroke and other AF-related complications. 15
Compared with the Kardia Mobile (KM) (AliveCor, Inc., Mountain View, CA, USA), the SnapECG device is larger, and the electrodes are bigger, which enable it to be more steadily held and pressed by the elderly patients to ensure collecting stable signals. Moreover, three electrodes were constructed in the SnapECG to increase the signal quality, while only two electrodes were included in the KM. 13
Comparing the study results of SnapECG and KM, both have their advantages and disadvantages. As no head-to-head comparison has been investigated, it is uncertain whether the following differences would be significant. The sensitivities and specificities are 100% and 84.97% respectively by SnapECG, while 82% and 92% respectively by KM for AF; 16 54.55% and 99.09% respectively by SnapECG, while 26% and 98% respectively by KM for AT; 16 44.44% and 100% respectively for second-degree atrioventricular block, 80.00% and 98.91% respectively for third-degree atrioventricular block by SnapECG, while 70% and 100% respectively for high-degree atrioventricular block by KM. 16
Some studies have found that long-term anxiety can cause arrhythmias,17–19 and patients with arrhythmias often have symptoms of anxiety or depression. 20 Although there is no clear conclusion from relevant studies on the association between arrhythmia and anxiety or depressive symptoms, 21 we cannot exclude the psychological effect of earlier diagnosis and treatment achieved by the SnapECG monitoring on the improvement in patients’ symptoms, emotion, and quality of life.
Regarding the medical expenses, although there were no statistically significant differences between the two groups, the related medical expenses in the SnapECG group were numerically lower than that in the control group, and the expenses included the costs of the SnapECG devices. We believe that the difference between the two groups would be enlarged if the follow-up duration were prolonged, as more than 80% of the patients in the control group, while only 30% of the patients in the SnapECG group, had not been diagnosed at the end of the study.
To the best of our knowledge, this is the first study that systematically investigated the sensitivity and specificity of the diagnosis by SnapECG monitoring for common arrhythmias. Besides, we first analyzed the composition of both asymptomatic and symptomatic arrhythmias, and innovatively evaluated the effect of the SnapECG monitoring on the patients’ symptoms, emotions, and life quality by modified EHRA, SAS, PHQ-9, and SF-36 scales.
Study limitations
First, this study did not include malignant arrhythmias such as ventricular tachycardia, ventricular flutter, and ventricular fibrillation. Thus, the value of the SnapECG for diagnosing such arrhythmias cannot be concluded. Second, the number of AT and ΙΙ° AVB was relatively insufficient in the first phase, which may affect the assessment of their sensitivities and specificities. Third, although the SnapECG monitoring significantly improved the early diagnosis rate of the symptomatic arrhythmias compared with the conventional management, due to its nonwearable characteristics, less episodes of the paroxysmal arrhythmias would be recorded by the SnapECG if compared with the wearable smartwatch. 22 However, as the SnapECG collects signals from two hands, it may be more accurate in diagnosing the P-wave-associated arrhythmias compared with the smartwatch which can only collect the signals from one wrist. Fourth, 97 out of the 184 (52.7%) symptom-related ECGs were normal in this study, which could be explained by the following reasons: 1) the patients’ symptoms were not arrhythmia-related; 2) the symptom-related arrhythmias were not captured because of short paroxysmal arrhythmias; 3) missed diagnoses cannot be excluded due to the low sensitivity to P-wave-associated arrhythmias by the SnapECG. Fifth, the interference waves generated by external factors were unavoidable. For example, the elderly patients would have difficulty holding the devices steadily, and interference waves would occur while the patients’ hands trembled. At the present stage, we could not ensure 100% accuracy of the diagnosis by SnapECG. However, as presented in the phase 1 study, specificities of more than 96% were reached for all common arrhythmias except AF. We suggest that the SnapECG detected ECGs should be interpreted by senior cardiologists, and additional examinations should be adopted before prescribing any treatment if there is a doubt remaining on the diagnosis.
Conclusion
Remote motoring through the SnapECG is valuable to early diagnosis of suspected arrhythmias, which leads to improvement in patients’ symptom, emotion, and quality of life. However, the sensitivity, specificity, and practical convenience of the SnapECG for arrhythmia diagnosis need to be further improved by improving the P wave amplitude, increasing detection stability, and providing automatic diagnosis function.
Supplemental Material
sj-tif-1-dhj-10.1177_20552076221113393 - Supplemental material for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias
Supplemental material, sj-tif-1-dhj-10.1177_20552076221113393 for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias by Qian Gu, Zengguang Chen, Jiazheng Ma, Yaqing Zhou, Jinshuang Li, Lianghong Ying, Rui Hua, Wenhao Zhang, Ran Li, Fengwei Zou, Xiaoxuan Gong, Yiyang Zhan and Chunjian Li in Digital Health
Supplemental Material
sj-tif-2-dhj-10.1177_20552076221113393 - Supplemental material for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias
Supplemental material, sj-tif-2-dhj-10.1177_20552076221113393 for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias by Qian Gu, Zengguang Chen, Jiazheng Ma, Yaqing Zhou, Jinshuang Li, Lianghong Ying, Rui Hua, Wenhao Zhang, Ran Li, Fengwei Zou, Xiaoxuan Gong, Yiyang Zhan and Chunjian Li in Digital Health
Supplemental Material
sj-TIF-3-dhj-10.1177_20552076221113393 - Supplemental material for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias
Supplemental material, sj-TIF-3-dhj-10.1177_20552076221113393 for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias by Qian Gu, Zengguang Chen, Jiazheng Ma, Yaqing Zhou, Jinshuang Li, Lianghong Ying, Rui Hua, Wenhao Zhang, Ran Li, Fengwei Zou, Xiaoxuan Gong, Yiyang Zhan and Chunjian Li in Digital Health
Supplemental Material
sj-docx-4-dhj-10.1177_20552076221113393 - Supplemental material for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias
Supplemental material, sj-docx-4-dhj-10.1177_20552076221113393 for Use of handheld electrocardiograph (SnapECG) for the remote monitoring of arrhythmias by Qian Gu, Zengguang Chen, Jiazheng Ma, Yaqing Zhou, Jinshuang Li, Lianghong Ying, Rui Hua, Wenhao Zhang, Ran Li, Fengwei Zou, Xiaoxuan Gong, Yiyang Zhan and Chunjian Li in Digital Health
Footnotes
Acknowledgement
Not applicable.
Conflicts of Interest
There was no relevant conflict of interest
Contributorship
GQ, CZ, MJ, ZY, LJ, YL, GX, ZY, and LC researched literature and conceived the study. HR, ZW, LR, and ZF were involved in protocol development, gaining ethical approval, patient recruitment, and data analysis. GQ, CZ, MJ, and ZY wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
The ethics committee of Nanjing Medical University approved this study (REC number2018-SR-038).
Funding
This work was supported by grants from the National Natural Science Funding of China (82170351), the Jiangsu Province's Key Provincial Talents Program (ZDRCA2016013), and the Special Fund for Key R & D Plans (Social Development) of Jiangsu Province (BE2019754).
Guarantors
LC and ZY.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.