
Abstract
Background
Prior to the COVID-19 pandemic, about half of patients from populations that sought care in neurology tried complementary and integrative therapies (CITs). With the increased utilization of telehealth services, we sought to determine whether patients also increased their use of virtual CITs.
Methods
We examined datasets from two separate cross-sectional surveys that included cohorts of patients with neurological disorders. One was a dataset from a study that examined patient and provider experiences with teleneurology visits; the other was a study that assessed patients with a history of COVID-19 infection who presented for neurologic evaluation. We assessed and reported the use of virtual (and non-virtual) CITs using descriptive statistics, and determined whether there were clinical characteristics that predicted the use of CITs using logistic regression analyses.
Findings
Patients who postponed medical treatment for non-COVID-19-related problems during the pandemic were more likely to seek CITs. Virtual exercise, virtual psychotherapy, and relaxation/meditation smartphone applications were the most frequent types of virtual CITs chosen by patients. In both studies, age was a key demographic factor associated with mobile/virtual CIT usage.
Interpretations
Our investigation demonstrates that virtual CIT-related technologies were utilized in the treatment of neurologic conditions during the pandemic, particularly by those patients who deferred non-COVID-related care.
Introduction
Patients with neurological disorders may have concerns regarding standard pharmacological treatments due to their high costs and potential side effects. 1 Consequently, patients often employ non-pharmacological interventions, such as complementary and integrative treatments (CITs), for relief. 2 CITs for neurological conditions are often divided into two broad categories: (1) behavioral interventions and (2) supplemental interventions. 3 Behavioral treatments include biofeedback and relaxation 2 ; supplemental interventions include vitamins, minerals, and herbs. Prior to the COVID-19 pandemic, approximately 50% of adults with neurologic conditions turned to CITs. 2
Due to the COVID-19 pandemic, healthcare delivery has dramatically changed. A 154% increase in telehealth visits was reported during March 2020 as compared to March 2019. 4 Studies show that this increase in teleneurology usage may be partly due to pandemic social-distancing guidelines and the broad applicability and comfort of getting medical help from one’s device.5–7 With a demonstrated increase in virtual medical care, patients might also specifically seek mobile/virtual/telehealth CITs at increasing rates to address their neurologic problems. However, many studies demonstrated that the usage of virtual platforms for medical care has been limited to specific populations, and thus may not be generalizable to all populations.5–7 Therefore, more research on the use of virtual health care, in this case, CITs, on different patient populations is significant. Several studies suggest that CITs delivered by telehealth are effective in multiple fields of medicine, including neurology, rehabilitation, and oncology. However, these studies had small sample sizes with select patient populations, and many only focused on specific CIT applications such as tai chi and stretching, there is a clear gap in the literature on the use of mobile/virtual/telehealth CITs as a whole across larger patient populations.8–12 Hence, it becomes increasingly important to assess overall CIT usage in more patient populations.
With decreased access to in-person healthcare and the vast increase in the use of telehealth services associated with the pandemic, we sought to evaluate CIT use in patients who presented to a large urban tertiary care neurology practice and to examine predictors of CIT use during the pandemic.
Methods
Standard protocol approvals, registrations, and patient consent
Both primary research studies and the sub-analyses reported herein were approved by the New York University Grossman School of Medicine Internal Review Board and were conducted by faculty and research staff in the NYU Department of Neurology. The studies reported in this article are sub-analyses of larger datasets for the Teleneurology Survey Study 13 and the Post-COVID-19 Neurology Study. Verbal consent was obtained from all subjects in the reported studies.
Teleneurology methods
Eleven neurologists who were conducting telehealth (audio-video) visits for both new and established patients between 18 May 2020 and 16 July 2020, in the NYU Department of Neurology, invited patients to participate in a research study regarding their experiences with telehealth. Interested patients who provided verbal consent underwent a telephone-based survey, which included questions about patient demographics and patients’ use of complementary or alternative therapies to manage their neurological conditions. Specifically, patients were asked, “Have you used complementary or alternative therapies to help manage your neurological problem in the last 3 months (i.e. mobile applications for relaxation, online fitness classes, virtual physical therapy, etc.)?” They could respond “No” and move on or “Yes.” If they responded yes, they were asked, “What applications, therapies have helped?” For the purposes of consistency, responses to the question regarding complementary or alternative therapies will be referred to under CIT.
Patients were asked to list specific therapies they were using; the patients were not given a list of potential therapies to choose from. To reduce selection bias, neurologists were instructed to invite study participants, to obtain verbal consent, and to administer the survey consecutively to each patient seen on a select date(s) of the telehealth visit. Survey data were entered into REDCap by a study coordinator.
The study principal investigator, co-investigators, and a data analyst performed statistical analyses. Analyses were performed using SAS v9.4 (Cary, NC). Because <5% of responses were missing for each survey question, imputation for missing values was not performed. We reported descriptive analyses, including frequencies and percentages to describe categorical variables, means, and standard deviations to characterize continuous variables. For data that were not normally distributed (as assessed visually using histograms), we reported medians and interquartile ranges for any continuous variables. We examined the effects of patients’ demographic characteristics (age, sex, and race) and clinical responses, such as chief complaints and reports of postponing medical care, due to the pandemic on their use of CITs and specifically, mobile applications/virtual therapies. We also used chi-square tests (or Fisher’s exact tests when frequency counts were small (expected values <5 per cell in 2 × 2 tables)). Student’s t-tests were used to test for associations in continuous outcomes for normally distributed data. Since headache is one of the most common neurological symptoms presented in neurology practices 14 and is also one of the most common neurological symptoms following COVID-19, we examined whether headaches are associated with CIT use. Furthermore, depression is highly associated with many neurologic complaints, 15 so we examined whether depression was related to CIT use. Both headache and depression are common symptoms for which patients are known to seek CITs.2,16
Neuro-COVID-19 methods
After Institution Review Board approval was obtained on 4 November 2020, neurologists across NYU Langone Health campuses were asked to add the names of their patients to a shared list in the electronic health record system (EPIC) following standard of care visits for neurological and/or post-COVID-19 symptoms. If a patient had not specifically opted out of being contacted for research studies in EPIC, they were contacted by a study coordinator and invited to participate in an interview capturing neurological symptoms using validated scales. Electronic written informed consent was obtained for each participant who expressed willingness to complete the study. The research coordinator administered the research assessments via telephone, via WebEx, or in person. The research team captured study-related information from standardized clinical templates EPIC and entered this information into a secure and HIPAA-compliant REDCap database. The research-related scales and questionnaire data were also stored in REDCap. Questionnaires and scales captured cognition, social determinants of health, vision, and other neurological symptoms. They also included the Headache Impact Test (HIT)-617,18 and the Neuro-QOL Depression scale. 19 The use of CIT in the context of managing post-COVID-19 symptoms was also captured. The questions regarding CIT use provided multiple-choice responses, and patients could select as many as they wished.
Analyses were performed using SAS v9.4 (Cary, NC). We examined the effects of patients’ demographic characteristics (age, sex, race, and education) and clinical outcomes such as neurological symptoms related to COVID and questionnaire results on their use of CITs, and specifically mobile applications/virtual therapies. Neuro-QOL depression scores were calculated by converting raw scores ranging from 8 to 40 to t-scores ranging from 36.9 to 75 with a mean of 50 and a standard deviation of 10. Higher t-scores indicate worsening depression. A t-score of 55 or greater indicates depression symptoms. Continuous variables were described using median and interquartile ranges and used the nonparametric Kruskal–Wallis test to test for significance. Categorical variables were reported as frequencies and percentages or odds ratios and used the chi-square test Logistic regression analyses were used for multivariate models to explore associations between continuous and categorical variables.
Role of the funding source
M. T. Minen is an NIH mHealth scholar with funding from NCCIH to conduct app-based migraine research.
Results
Teleneurology study results
Among 187 patients, the mean age was 49
Characteristics of patients in the teleneurology survey study.
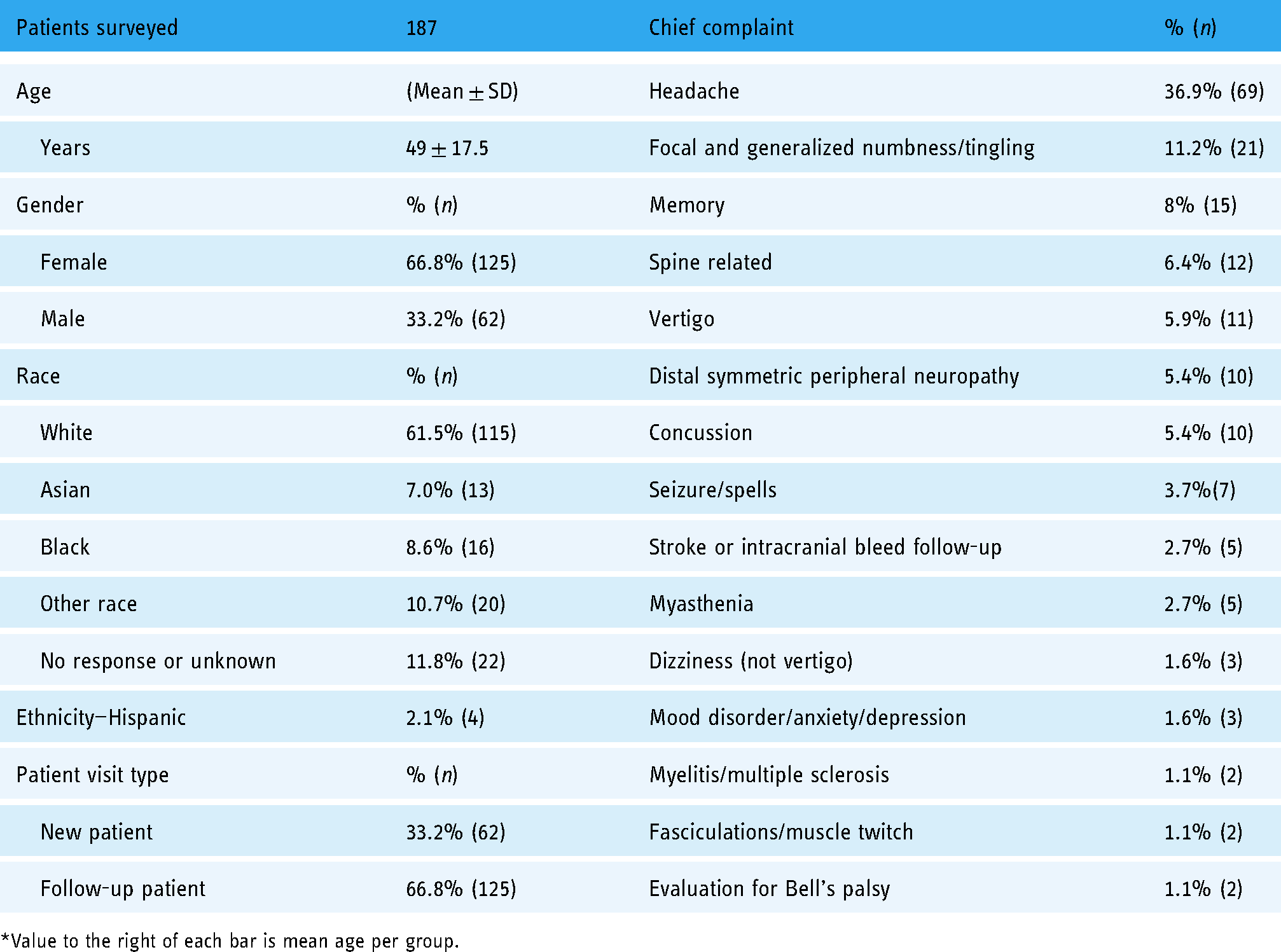
*Value to the right of each bar is mean age per group.
Use of complementary and integrative therapy (CIT) to help manage a neurological problem (teleneurology survey study).

Younger age was associated with seeking CITs more; patients who sought CITs were an average of 5.7 years younger (t = 2.2, P = .03). The most used app types were relaxation/meditation and virtual exercise programs. Relaxation app users were on average 10.5 years younger (P < .001), and virtual exercise app users were on average 7.7 years younger (P = .03). While overall CIT use occurred with similar frequencies for male and female patients (31% vs. 42%, χ2 = 2.0, P = .16), virtual exercise apps were used by female patients more (19% vs. 7% for male patients, P = .02). There were no significant associations between app use with race. However, only 15% of Asian patients reported seeking CITs, compared with 40% of Black patients and 41% of White patients. There were no associations between patient type (new vs. follow-up) and CIT use. Patients whose chief complaint was headache were more likely to have used a virtual exercise app (OR = 2.24, P = .047) and a relaxation app (OR 2.7, P = .02) (unadjusted ORs based on 2 × 2 tables) in the teleneurology study. No other chief complaints or CITs were associated with each other. Those who postponed medical treatment during the pandemic were significantly more likely to have sought CITs (OR = 2.0, 95% CI 1.0–4.0; P = .04). After adjusting for sex, race, chief complaint of headaches, and postponing treatment, age remained a significant predictor of virtual CIT use, with an estimated 4% decline per additional year of age (OR = 0.96, 95% CI 0.92–0.992; P = .02).
Post-COVID-19 neurology study results
The 76 patients who participated were also two-thirds female (67.1%) with an overall cohort mean age of 48 ± 13.8. Patients were mostly White (70.7%) (Table 3). Most patients self-reported having graduated from college or having had post-college training (83.8%). The main occupation listed for employed patients was professional/technical (61%). A third of participants (32.9%) reported having a history of neurological or ophthalmological disease(s). Patients reported using a variety of CITs (Figure 1). The most popular virtual/technology CIT involved virtual psychotherapy and mindfulness/meditation as a mobile application; these CITs were endorsed by 28.9% (n = 22) of participants. Other non-virtual CITs were also used frequently, which included exercise (n = 33, 43.4%) and vitamins/herbal remedy use (n = 33, 43.4%). Increased use of virtual CITs was significantly associated with younger age (median age 48 vs. 54 years, P = .03). There was a decline of 3.5% (P = .04) in the odds of using mobile/virtual CIT for each additional year of age. Age remained a significant (P = .04) predictor of virtual CIT use when adjusting for the effects of outdoor exercise, which is also a significant predictor of mobile app usage (0.02; OR 3.1, 95% CI: 1.2–8.1) but was not associated with age (P = .64), demographic characteristics and COVID neurological symptoms using logistic regression. Participants who used virtual CITs were also at 5.4× higher odds (95% CI 2.0–14.6) of having diet modifications since the pandemic started.
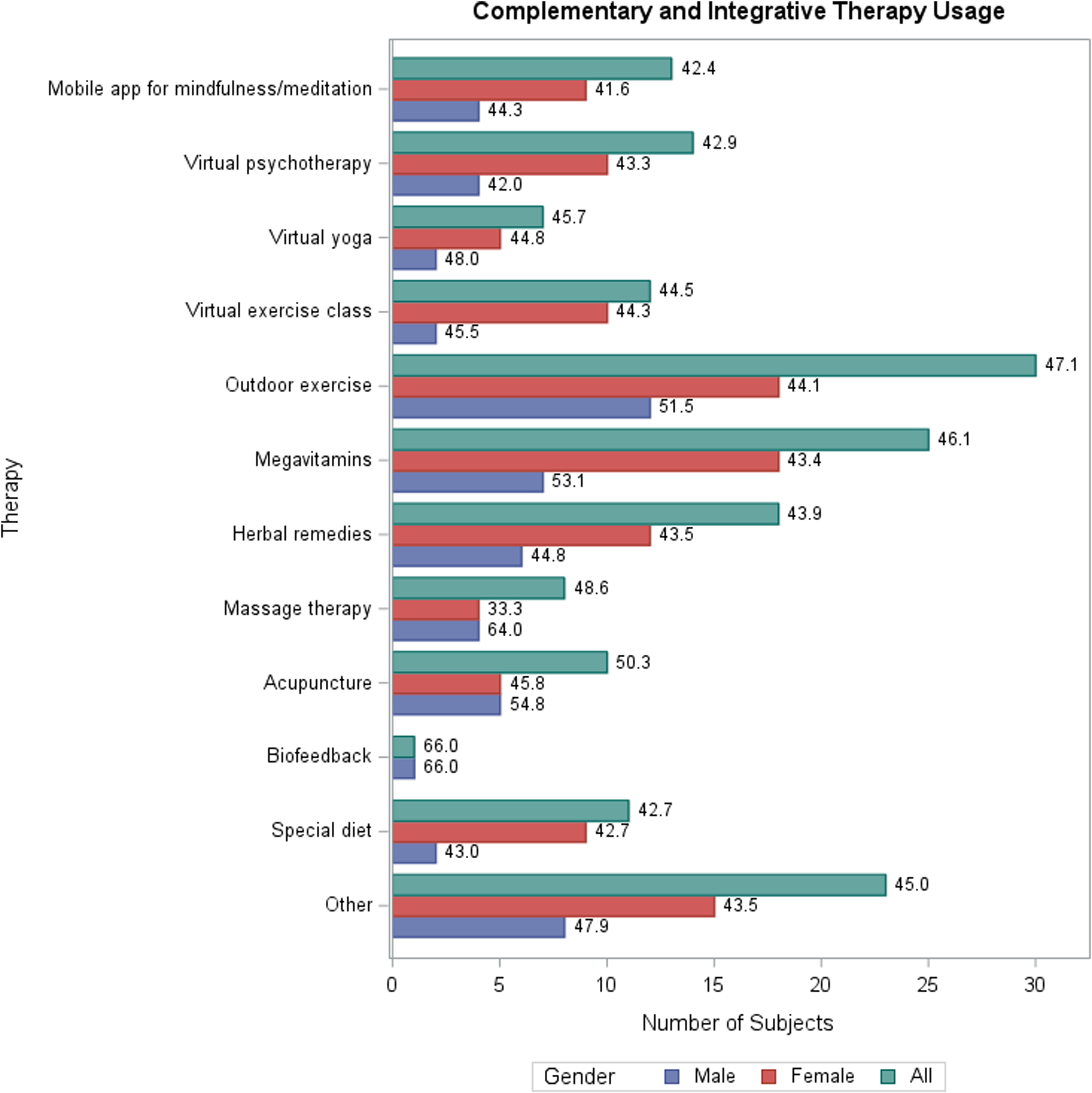
Complementary and integrative therapy use by patients presenting to a neurology practice for neuro-related COVID-19-19 symptoms* (post-COVID-19 neurology study).
Patients who presented to neurology for COVID-19-related neurology symptoms and use of virtual CIT (post-COVID-19 neurology study).

CIT: complementary and integrative therapy; RT-PCR: reverse transcription-polymerase chain reaction.
Any associations between neurological symptoms and the types of CITs patients reported using were also examined. Patients using virtual psychotherapy were more likely to report muscle aches (OR = 15.2, P = .002), memory changes (OR = 7.3, P = .006), word-finding difficulties (OR = 7.0, P = .007), and fatigue (OR = 7.3, P = .04). Using a mobile app for mindfulness/meditation was associated with a history of word-finding difficulties (OR = 4.7, P = .02) and fatigue (OR = 6.6, P = .048).
Among patients in the COVID-19 study reporting headache (n = 42), the most used virtual CITs were psychotherapy (n = 11, 26%) and a mobile app for mindfulness/meditation (n = 9, 21%). The most used non-virtual CITs were megavitamins (n = 19, 45%), outdoor exercise (n = 17, 40%), and herbal remedies (n = 13, 40%). Those reporting headache were no more likely to use a virtual CIT than they were to use a non-virtual CIT (43% vs. 32%, P = .35). Those with headaches had median HIT-6 scores of 59 (interquartile range (IQR) 54–67), indicating a substantial symptom burden. There were no significant differences in HIT-6 scores between groups of patients who used different categories of CIT. However, virtual CIT users reported significantly lower median HIT-6 scores (56.5, IQR 49–59) than non-virtual users (64, IQR 56–70) when aggregated (P = .04).
Those reporting depression (n = 11) had a median quality of life (QOL) t-scores of 59 (IQR 57.4–67.3), and their most used CITs were virtual psychotherapy (6, 54.5%), followed by other (5, 45.5%), meditation/mindfulness app (4, 36.4%), special diet (3, 27.3%), and megavitamins (3, 27.3%). Overall, those with depressive symptoms were more likely to report using a virtual CIT, with 82% of patients with depression using one or more compared to only 30% of those with no depression (OR = 10.6, P < .001).
Discussion
Prior to the pandemic, research has shown that virtual-based CITs are potentially beneficial to patients with neurological conditions who want to improve self-care and track their symptoms.8,20 Studies demonstrated that the use of virtual CITs put increased responsibility on the patient, which enabled them to feel more involved in their care and motivate them to maintain a healthy lifestyle.8,20 During the pandemic, and with the associated increased use of telehealth services, 4 we found several key observations regarding CIT use: (1) patients who reported postponing medical treatment were more likely to seek CITs; (2) younger patients were more likely to employ mobile/virtual CITs; (3) virtual exercise, virtual psychotherapy, and relaxation/meditation smartphone applications were the most reported types of virtual CITs employed; (4) patients who reported postponing medical treatment were more likely to seek complementary and integrative therapies (CITs).
It is unsurprising that in the pandemic, patients postponing treatments sought other options; the World Health Organization has focused on integrated health recently. In mass media, there has been a focus on supplement use for COVID-19 treatment.21,22 Prior research showed that patients who wish to avoid conventional treatments may seek telehealth CIT options. 2 Before the pandemic, telehealth CITs were attractive to patients who were geographically, economically, socially, and/or physically hindered from attending an office visit or who desired to avoid the potential side effects of pharmacological treatments. Due to their versatility and accessibility, telehealth CITs can reach a large patient population, and further research examining the advantage of in-person versus virtual CITs is warranted.
Younger patients were more likely to employ mobile/virtual CITs
In the teleneurology study, younger patients were more likely to utilize mobile/virtual CIT interventions. Likewise, the neuro-COVID-19 results indicate that age was the only predictor with an association with mobile/virtual CIT usage. This association may suggest a generational difference in exposure to and ability to use technology. The decrease in virtual CIT use with older patients could be attributed to a lack of comfort and access to the required technology forms of CIT. By increasing access to telehealth use in neurology, creating apps appropriate for geriatric use, and expanding resources dedicated to helping older patients understand how to use virtual CITs, the age gap in usage may be reduced.
Virtual CITs most reported by the neurology patients
The virtual exercise was the most used CIT in our teleneurology study. Aerobic exercise is beneficial to patients who experience migraine.23–27 Aerobic exercise improves cognitive function, sleep quality, and reduces depressive symptoms amongst patients with mild cognitive impairments, and provides benefits for patients with other neurological conditions, such as Parkinson’s disease.28–30 Virtual exercise apps may allow patients increased access to exercises that are more cost-effective and diverse. More studies are needed on the efficacy and adherence to virtual exercise apps. Finally, exercise does not carry the stigma associated with other virtual treatments, such as virtual psychotherapy.31–35 People may be more open about engaging in it publicly and even in a study.
In contrast, the most used virtual CIT reported in the COVID-19 study was virtual psychotherapy. Virtual psychotherapy was most used amongst patients with depression, headache, muscle aches, memory changes, word-finding difficulties, and fatigue. Virtual psychotherapy can be beneficial for patients with neurological symptoms, including those with co-morbid psychiatric conditions.36–38 One study on psychotherapy that employed virtual reality to treat young adults with mild to moderate depression found that virtual psychotherapy may influence patient adherence and efficacy because of increased engagement, thereby improving QOL as well as preventing long-term chronic depression. 39 Considering that some studies have shown that virtual psychotherapy is effective and can increase access to treatment for patients with neurological disorders, research should be conducted to determine if virtual psychotherapy has a durable benefit.
Other frequently used virtual CITs reported in both the teleneurology and neuro-COVID-19 studies were relaxation and meditation apps. Commercial meditation and relaxation apps, such as Calm, were already increasingly popular amongst smartphone users. 40 A 2018 survey revealed that most people decided to use mental health apps after finding them on social media. 41 There was a 10% increase in the number of downloads of mental health apps, primarily being meditation apps, during the pandemic. 42 As the pandemic has greatly affected mental health, online mindfulness interventions have become increasingly available and have helped to improve pandemic-related psychological conditions whilst maintaining social distancing. 43 Additional research is needed to measure the efficacy and adherence to these mobile CITs over time.44–49
Limitations
Our studies were single-site exploratory studies conducted with a small patient population and may not be generalizable to the whole population. In the teleneurology study, the investigators were also participant physicians, which may have led to bias. Participants might have responded with answers they believed investigators wished to hear. 50 The neuro-COVID-19 study was not done with consecutive recruitment; the patients were those with COVID-19 who likely had continuing symptoms, prompting them to seek further evaluation and care. Few patients were over the age of 65 years. Thus, there might be limited generalizability to older neurologic populations. Our studies were not observational and not randomized. Thus, there may not be diversity in terms of socioeconomic background, and our observations may not be generalizable to a broad population of patients. Furthermore, our study was limited to complementary and integrative treatments, which included supplements, but not pharmacologic medications used off-label for other purposes. Such oral formulations were increasingly used off-label, 51 but we focused more on how changes in technology as treatment changed health.
Future directions
There are many potential avenues for future investigation, such as education, implementing frameworks for virtual CITs in clinical care, and examining whether patients who initiate CITs continue their use over the long term. 52 Future improvements could involve improving the software to be more user-friendly and including CIT instructions for those not comfortable with using technology, especially in the older age groups. Further studies can also be conducted on the association between gender and usage of virtual exercise apps.
Exploring the preferences of stakeholders in CIT is crucial to the development and concurrent evidence-based trial of mHealth apps. Developers of future mobile app mindfulness/meditation interventions may benefit from involving patients with neurological conditions in the development process. The popularity of CIT methods amongst patients recording depression and headache in this study highlights the specific CIT types for which more evidence-based studies on virtual options are needed. One solution is the development and integration of digital clinics. Traditional health care approaches with digital health tools such as mobile apps could be advantageous. 53 This hybrid approach could be a more efficacious method to ease older patients into technology-based care. More studies would be needed to examine the transition from in-person CITs to virtual CITs and the adherence to treatment.
Just as patients turn to pharmacists for guidance on medications and supplements for various ailments, 51 patients need a well-established, trusted method for learning about technology-based complementary and integrative treatments. Given the ever-growing number of telehealth apps available, the creation and maintenance of an app evaluation framework could prove useful in determining the safety, efficacy, and feasibility of each app. In a 2019 panel, a group of mental health care providers and those with lived mental health experience convened to reform the American Psychiatric Association framework, adapting it to the new digital mental health field with a hierarchical level approach to app evaluation. 54 Developing a similar evaluation framework for neurological care mobile apps would allow patients and providers alike a more standard, accessible way to navigate the virtual marketplace and determine which apps will be able to provide the best-personalized care. Further, evidence-based virtual CIT maps might also be helpful in directing neurology patients to the best CITs. Such maps have been developed for using CITs during the COVID-19 pandemic, though they have not had a virtual focus. 55
Our study was inclusive of many neurological conditions, ranging from headache to stroke. Future studies might examine CIT use for an even wider range of neurologic conditions and with older populations. 56 The duration and frequency needed for the virtual CITs to have maximal benefit should be studied.55,57–60 As the role of telehealth continues to evolve, studies must be done to better understand their efficacy and adaptability as they are delivered in various modes virtually. For example, therapists need valid tools to determine which patients would benefit from virtual reality and augmented reality instead of manual therapy. 61 The development of evidence-based policy should take into consideration the increased use of virtual CITs. Similar to the development of virtual oncology integrative centers, 62 there may a role in the creation of virtual neurology integrative centers.
Conclusion
Virtual-based CITs will inevitably be part of the treatment plan for many neurological disorders. The adaptation will likely be faster than expected especially for patients who postponed traditional medical appointments during the pandemic. Ensuring accessibility for all populations and having a framework for such technologies is an unmet need. Providers treating patients with neurologic conditions will require knowledge of which CITs are evidence-based. Additional studies exploring adherence and the dosing needed to impact treatment outcomes are important areas for further investigation.
Footnotes
Acknowledgements
The authors thank Lisena Hasanaj for her help with data entry for both data sets. We also thank all the neurologists who participated in the teleneurology study and those who referred patients to the Neuro-COVID-19 study.
Contributorship
MTM contributed to conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, validation, writing—original draft, review, and editing. NAB contributed to conceptualization, data curation, formal analysis, investigation, and writing—original draft, review, and editing. SF contributed to data curation, formal analysis, writing—original draft, review, and editing. MC contributed to writing—original draft, review, and editing. AS contributed to writing—original draft, review, and editing. QH contributed to writing—original draft, review, and editing. KM contributed to writing—original draft, review, and editing. MS contributed to writing—original draft, review, and editing. DV contributed to writing—original draft, review, and editing. LY contributed to writing—original draft, review, and editing. F-YAF contributed to data curation and writing—review, and editing. JMB contributed to data curation and writing—review, and editing. LJB contributed to conceptualization and writing—review and editing. SLG contributed to writing—review, and editing. ST contributed to Conceptualization, data curation, formal analysis, investigation, methodology, and writing—original draft, review, and editing.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.T. Minen is an NIH mHealth scholar with funding from NCCIH to conduct app-based migraine research. M.T. Minen contributed to developing intellectual property being used in this study that is co-owned by NYU and IRODY. If the research is successful, NYU and IRODY may benefit from the outcome. N.A. Busis serves as alternate CPT advisor and has received personal compensation for speaking engagements from the American Academy of Neurology. SF reports no disclosures relevant to the manuscript; S. Friedman reports no disclosures relevant to the manuscript; J.M. Bhatt reports no disclosures relevant to the manuscript; M. Campbell, Q. Hossain, K. Maisha, A. Sahu, M. Soviero, D. Verma, and L. Yao reports no disclosures relevant to the manuscript; F.A. Foo reports no disclosures relevant to the manuscript. L.J. Balcer is editor-in-chief for the Journal of Neuro-Ophthalmology; S.L. Galetta reports no disclosures relevant to the manuscript; S.P. Thawani reports no disclosures relevant to the manuscript.
Ethical approval
Both primary research studies and the sub-analyses reported herein were approved by the New York University Grossman School of Medicine Internal Review Board and were conducted by faculty and research staff in the NYU Department of Neurology. Verbal consent was obtained from all subjects in the reported studies.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Complementary and Integrative Health (grant number K23AT009706).
Guarantor
MTM.