
Abstract
Studies have shown COVID-19 patients may have a low oxygen saturation (SpO2) independent of visible respiratory distress, a phenomenon termed “silent hypoxia.” Silent hypoxia creates uncertainty in the outpatient setting for clinicians and patients alike. In this study, we examined the potential for pulse oximeters in identifying early signs of clinical deterioration. We report descriptive results on COVID-positive patients’ experiences with a comprehensive home monitoring tool comprised of home SpO2 measurements with a novel symptom-tracking short message service/text messaging application. Of patients who required hospitalization, 83% sought care as a result of low pulse oximeter readings. Nearly all patients who did not require hospitalization reported that having a pulse oximeter provided them with the confidence to stay at home. Essentially all patients found a home pulse oximeter useful. Keeping COVID-19-positive patients at home reduces the potential for disease spread and prevents unnecessary costs and strain on the healthcare system.
Introduction
Previous studies have shown COVID-19 patients may have a low oxygen saturation (SpO2) independent of visible respiratory distress, a phenomenon termed “silent hypoxia.”1–3 Silent hypoxia creates uncertainty in the outpatient setting for clinicians and patients alike. In a recent study, evaluating patients given pulse oximeters at emergency departments and outpatient testing sites, 50% of patients who tested positive for COVID-19 and ultimately needed hospitalization only returned to the hospital because of a low SpO2 measured at home. 4 These results suggest a role for FDA-approved pulse oximeters in both remote monitoring and triaging of COVID-19 infected outpatients. There have been a variety of remote monitoring studied for COVID,5,6 though few have assessed patient experience.
In this study, we examined the potential for pulse oximeters in identifying early signs of clinical deterioration in at risk COVID-positive patients. We report descriptive results on patients’ experiences with a comprehensive home monitoring tool comprised of home SpO2 measurements with a novel symptom-tracking short message service (SMS)/text messaging application.
Methods
We identified patients with a positive COVID-19 test in the outpatient setting within the last seven days. We preferentially selected patients for study participation if they were at high risk for deterioration due to underlying comorbidities which included all persons > age 60 years, immunocompromised, diabetes, chronic lung disease, cardiovascular disease including hypertension, obesity (body mass index > 40), chronic kidney disease or if they reported moderate to severe respiratory symptoms at the time of enrollment. We excluded patients previously hospitalized for COVID-19-related issues.
We mailed participants who consented to participation in pulse oximeters and enrolled them in a novel symptom-monitoring application offered through AIRx Health (AIRx). The patient's received a one-page description with photos of how to use the pulse oximeter. They received a daily 10 am SMS text with symptom questions including level of fatigue on a scale of 1–4, cough, fever, shortness of breath, chest pain. If new-onset chest pain, an immediate pop-up asked them to promptly seek medical advice. Data was transmitted upon their response to a dashboard that was monitoring daily by a clinician. If O2 levels < 93, worrisome symptoms, or downward trends were found, patients were called and advised to contact their clinical team and seek medical care.
We collected data daily on patients’ self-reported SpO2 and symptoms for 14 days from symptom onset. After 14 days, we sent patients a questionnaire through AIRx asking if patients received any in-person ED or hospital services during the monitoring period, what prompted them to seek care, and to describe their experiences with the remote monitoring application. We conducted a chart review on enrolled patients including their demographics, comorbidities, and hospitalization status (Figures 1 and 2).
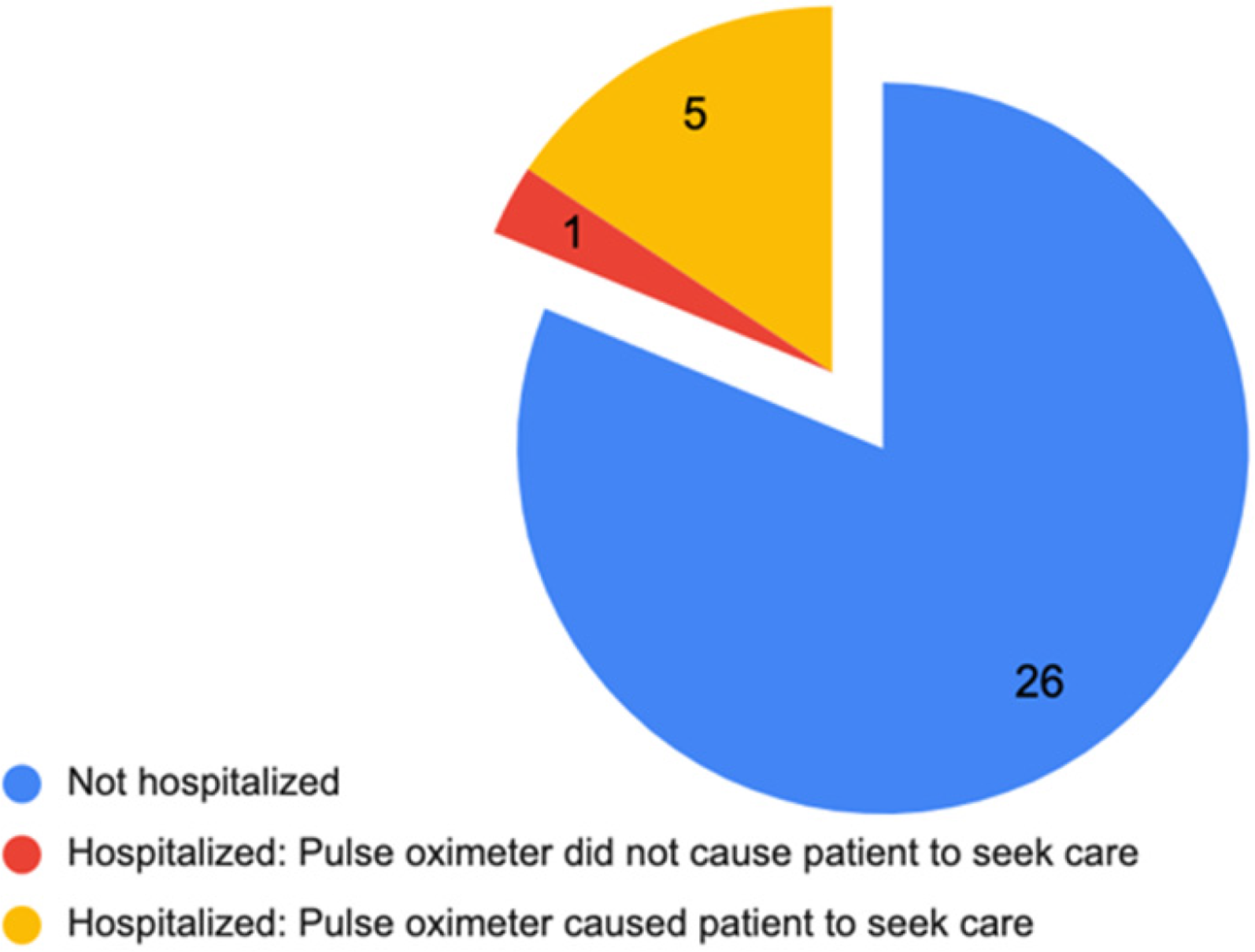
Pulse oximeter utility for seeking hospitalization.

Utility of pulse oximeter from a patient perspective.
Results
Between 24 September 2020 and 5 March 2021, 49 patients met criteria and enrolled in the study. Of enrolled participants, 30 of 49 were female, 15 identified as Hispanic/LatinX, 13 as White, 7 Asian, 2 Black, 2 other, and 10 did not state. Of these 49 patients, 32 (65%) completed the offboarding questionnaire following the remote monitoring period. Gender and racial mix of patients who completed offboarding were not statistically significantly different from the mix of those who did not.
Of the 32 participants who completed the final offboarding questions on their experience, six (19%) reported being hospitalized. Average hospital stays for those patients were 8.5 days (1–20 days). Of the hospitalized patients, five (83%) reported that a low SpO2 reading from the pulse oximeter led them to seek care. Of the 26 patients not reporting hospitalization, 25 (96%) reported that having a pulse oximeter at home gave them the confidence to safely remain at home. Almost all patients (31, 97%) reported that having a home pulse oximeter was extremely (20, 63%) or somewhat (11, 34%) useful. The one patient who answered that the pulse oximeter was not useful indicated that this was because they did not experience symptoms at any point.
Discussion
We report descriptive results on COVID-19 patients’ experiences with remote monitoring consisting of home SpO2 measurement using FDA-approved pulse oximeters and a novel symptom-tracking SMS application. Essentially all patients found a home pulse oximeter useful. Of patients who required hospitalization, 83% sought care as a result of low pulse oximeter readings. Nearly all patients who did not require hospitalization reported that having a pulse oximeter provided them with the confidence to stay at home. Keeping COVID-19-positive patients at home reduces the potential for disease spread and prevents unnecessary costs and strain on the healthcare system. As there are costs associated with obtaining and mailing pulse oximeters to patients, it is reasonable to target patients at high risk for deterioration for this intervention. This study is limited by the small number of patients enrolled and by patient self-selection bias. However, despite the small study size, these findings suggest that this may be a simple, patient-friendly intervention for implementation on a larger scale to ensure that patients receive an appropriate level of care.
Footnotes
Acknowledgments:
The authors would like to thank Airx for their role in data collection.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributorship
All authors contributed to the study design, data collection, data analysis, and critical review and approval of manuscript. LV, LE, and SS also contributed to writing of manuscript.
Compliance with ethical standards
Stanford University Protocol # IRB-57165.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Stanford RISE COVID-19 Crisis Response Faculty Seed Grant Program and The Sean N. Parker Center for Allergy and Asthma Research.