
Abstract
Case summary
A 5-month-old intact female Russian Blue cat presented with continuous urinary incontinence and intermittent haematuria. Retrograde vaginourethrography and contrast-enhanced CT revealed absence of distinct urethral and vaginal structures, with a single tubular lumen extending from the bladder to the vulva. Cystoscopy and exploratory laparotomy confirmed the absence of the uterine body and vagina, while bilateral uterine horns were present and both ureters inserted normally into the urinary bladder. These findings suggested partial persistent urogenital sinus (PPUS) rather than a complete form. Medical management failed to improve the incontinence, and urethral plication was performed without artificial urethral sphincter (AUS) implantation. The cat regained voluntary urination immediately, and continence was maintained for 741 days without recurrence or complications.
Relevance and novel information
To the authors’ knowledge, this is the first report of long-term urinary continence achieved in a cat with PPUS using urethral plication alone, without AUS implantation. The case highlights the practicality and cost-effectiveness of urethral plication as a minimally invasive alternative surgical technique for young or small cats.
Plain language summary
Some cats are born with abnormalities of the urinary and reproductive organs that can lead to lifelong urinary incontinence. In this report, we describe a young female cat who continuously leaked urine from an early age because of an abnormal connection between the urinary tract and reproductive tract. Detailed imaging and surgical exploration showed that the structures connecting the kidneys to the bladder were normal, but the lower part of the urinary outlet was abnormally wide. This abnormal anatomy made it difficult for the cat to retain urine normally. The cat was treated using a surgical technique called urethral plication. This procedure involves placing sutures around part of the urinary outlet to gently narrow it and improve urine control, without using any artificial devices. This approach was chosen because it is reversible, does not involve implants and may be safer in young or small animals. After surgery, the cat showed marked improvement, with no further urine leakage. The cat was followed for more than 2 years after surgery, and normal urination was maintained without complications. This case demonstrates that urethral plication can be an effective treatment option for urinary incontinence caused by congenital anatomical abnormalities in cats. It also highlights the importance of careful anatomical assessment when managing urinary disorders in young animals.
Keywords
Introduction
Among congenital urogenital malformations, congenital urogenital sinus (UGS), in which the urethra and vagina fail to separate and form a single lumen, is extremely rare in cats in veterinary medicine.1 –3 When congenital urogenital malformations are accompanied by urethral sphincter mechanism incompetence (USMI) due to structural abnormalities, urinary incontinence is typically the primary clinical sign. 4 Surgical management using an artificial urethral sphincter (AUS) has been reported relatively frequently in both dogs and cats; however, in feline patients, several challenges remain, including limitations in device size, risks of infection and other complications, and difficulties in long-term management.3,5 –7 In dogs, there has been one reported case of UGS managed solely with urethral plication; 8 however, to the authors’ knowledge, no such cases have been reported in cats.
This report describes a young cat diagnosed with UGS based on diagnostic imaging, in which long-term urinary continence was successfully achieved using urethral plication alone, without the implantation of an AUS. Embryological considerations suggested that the anomaly was more consistent with a suspected partial persistent urogenital sinus rather than a complete form.
Case description
A 5-month-old, 1.8-kg intact female Russian Blue cat was referred for continuous urinary incontinence and intermittent haematuria since birth. The referring veterinarian had diagnosed bacterial cystitis and treated the cat with multiple empirical antibiotic courses, with only temporary improvement. Physical examination revealed no gross vulvar abnormalities, but the external urethral orifice could not be identified. Haematology, biochemistry and radiographs were unremarkable, and urinalysis from spontaneous voiding showed no evidence of active infection.
Ultrasonography revealed a cystic structure dorsal to the bladder neck (Figure 1a). Retrograde vaginourethrography demonstrated a single lumen from the bladder to the vulva without urethrovaginal separation (Figure 2a). Contrast-enhanced CT confirmed these findings (Figures 1b,c and 2b).

Ultrasonographic and contrast-enhanced CT images showing a cystic structure dorsal to the bladder neck. (a) Longitudinal ultrasonographic image of the bladder demonstrating an anechoic cystic structure (arrowheads) continuous with the dorsal aspect of the bladder neck. (b) Sagittal and (c) dorsal contrast-enhanced CT images showing continuity between the dorsal bladder neck and the uterine body (arrows), forming a focal bulging structure (*)

Retrograde vaginourethrography image and contrast-enhanced CT image demonstrating absence of the vagina and a single tubular structure extending from the bladder to the vulva. (a) On retrograde vaginourethrography, contrast medium fills the single tubular structure (arrows) and flows through the dorsal bulging portion of the bladder neck into the bladder, with no evidence of a separate vaginal lumen. (b) On the sagittal CT image, only one tubular structure (arrows) is visible extending from the dorsal bulging portion of the bladder neck to the vulva
On day 25 after presentation, exploratory laparotomy and cystoscopy were performed under general anaesthesia (fentanyl 5 μg/kg IV premedication, propofol 6 mg/kg IV induction, isoflurane in oxygen maintenance with fentanyl 10 μg/kg/h constant rate infusion). The uterine horns were adherent to the dorsal bladder wall, with absence of the uterine body and vagina (Figure 3a). Cystoscopy (60003VB1; KARL STORZ Endoscopy) inserted via the vulva led directly into the bladder, confirming the absence of a urethral meatus or vestibule. A diagnosis of UGS was made and an ovariectomy was performed concurrently. Postoperative analgesia consisted of a continuous intravenous infusion of fentanyl (2.5 μg/kg/h) for 24 h.
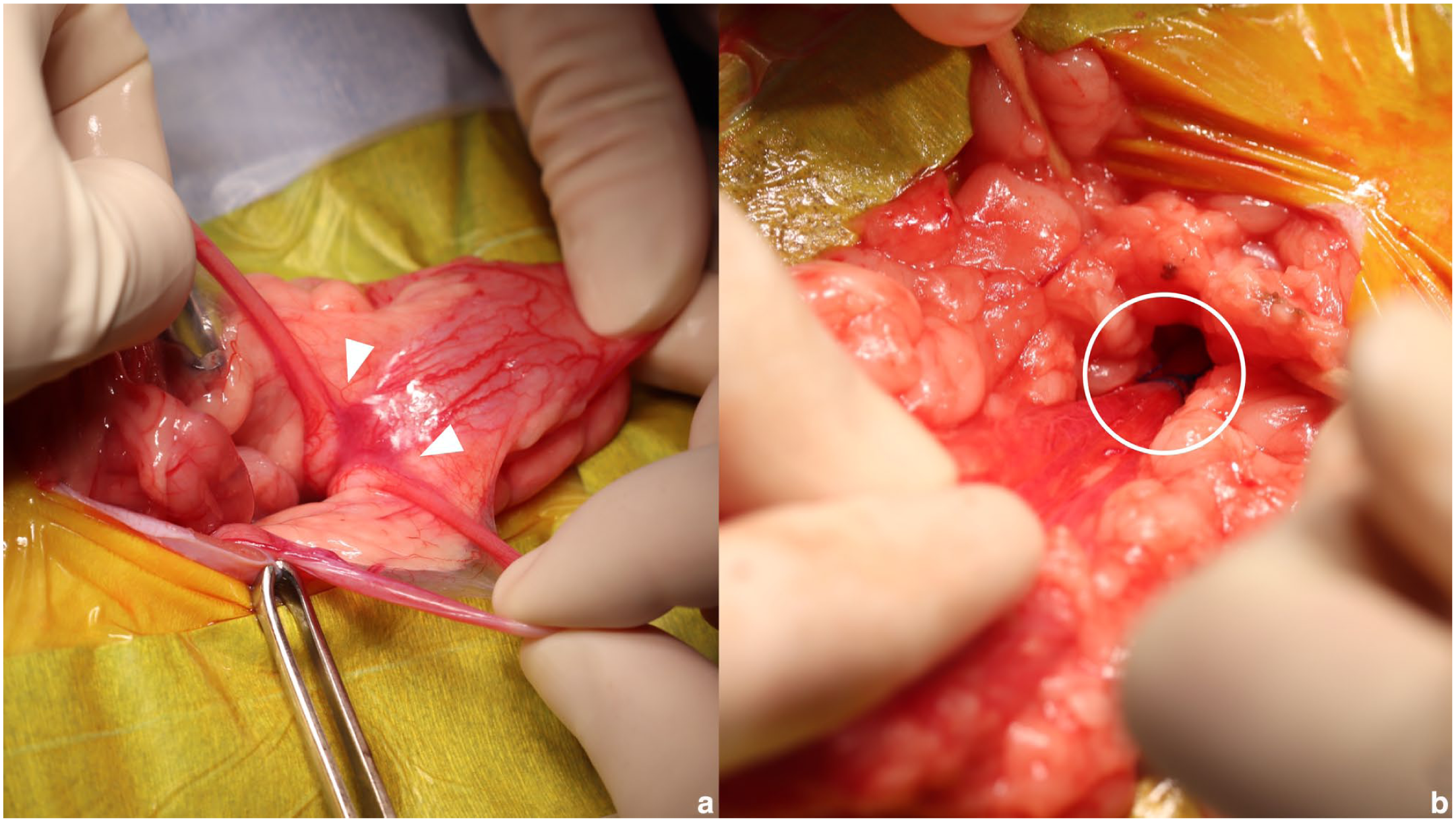
Intraoperative findings of the dorsal bladder neck and urethral plication. (a) The right and left uterine horns merge directly with the dorsal aspect of the bladder neck (arrowheads), and the bladder and uterine body appear as a single continuous structure. (b) Urethral plication was performed at the dorsal bulging portion of the bladder neck (circle)
Because urinary incontinence persisted, urethral plication was performed on day 173 under the same anaesthetic and postoperative analgesic protocols as those used for the initial surgery. A ventral midline celiotomy was performed, and the urinary bladder and proximal urethra were exposed. An 8 Fr feeding catheter (Atom Medical) was inserted from the vulva into the bladder as a guide, and the dorsal urethral wall at the bladder neck was plicated with 4-0 polypropylene sutures (PROLENE; Johnson & Johnson) by passing the sutures through the urethral wall into the urethral lumen (Figure 3b). Additional caudal plication reduced the lumen to approximately one-third of its preoperative size. Residual uterine horns were excised at their bladder attachment. Postoperative antibiotics (amoxicillin 20 mg/kg PO q12h) were given for 7 days.
Spontaneous voiding resumed immediately, with complete resolution of incontinence by day 14 postoperatively. At 741 days after surgery, continence was maintained without recurrence of urinary tract infection.
Discussion
This case describes a congenital urogenital malformation in a cat that was successfully managed without the use of an AUS, achieving long-term urinary continence through urethral plication alone. To the authors’ knowledge, this is the first reported feline case of a congenital urogenital malformation treated solely with urethral plication and followed up long term.
The urogenital sinus is a normal embryological structure that is formed during the separation of the cloaca into the urogenital and gastrointestinal tracts and contributes to development of the urinary bladder, urethra and distal vagina. In contrast, the proximal vagina, uterine body and uterine horns originate from the paramesonephric (Müllerian) ducts, which normally fuse in the midline and connect to the urogenital sinus to complete formation of the female reproductive tract. The ureters arise from ureteric buds branching from the mesonephric ducts and develop independently of the paramesonephric duct system; therefore, normal ureteral insertion into the urinary bladder may be preserved even when abnormalities of the urogenital sinus or paramesonephric duct fusion are present. 9 In the present case, bilateral uterine horns were present whereas the uterine body was absent, and both ureters inserted normally into the urinary bladder. These findings suggest preserved formation of the paramesonephric ducts with selective disruption of midline fusion and connection to the urogenital sinus, consistent with segmental aplasia of the fused paramesonephric ducts. Accordingly, the anomaly in this case was considered more consistent with a suspected partial persistent urogenital sinus rather than a complete form.
The AUS has been reported to be effective for refractory USMI in both dogs and cats, and several successful cases have been described.6,7 In feline urogenital malformations managed with AUS implantation, good urinary control has been achieved; however, multiple postoperative adjustments were required, and the procedure presupposed long-term device maintenance.3,5 Reconstruction techniques, such as partial resection of the bladder neck or bladder neck flap surgery, have also been reported; however, these are invasive procedures often associated with complications such as recurrent bacterial cystitis and immediate postoperative dysuria. 4 Conversely, in dogs, favourable outcomes have been reported with open surgical urethral plication, which increases urethral resistance and controls incontinence without the need for specialised equipment. 8 In the present case, urethral plication was chosen as a less invasive alternative to AUS. This decision was based not only on the complexity and maintenance requirements of AUS but also on the patient’s young age, which increases the risk of infection and tissue reaction associated with implanted devices.10,11 Furthermore, the high cost of AUS and the reversibility of urethral plication supported this choice, as additional procedures such as AUS implantation or partial bladder neck resection could be considered later if continence was not achieved. Therefore, urethral plication was chosen as a minimally invasive and reversible first-line treatment option.
Watanabe et al 8 determined the final urethral diameter in dogs by assessing resistance during manual bladder compression intraoperatively. However, because cats exert weaker voiding pressure compared with dogs, this method was considered less reliable for the present case. Therefore, the urethral diameter was adjusted to approximate the normal diameter in female cats to obtain physiological urethral resistance. The normal feline urethral diameter is approximately 2 mm (equivalent to 6 Fr); 12 considering postoperative inflammatory narrowing, the target diameter was set at 2.7 mm (8 Fr). Urinary incontinence resolved within 2 weeks postoperatively and did not recur during long-term follow-up, suggesting that an 8 Fr diameter was appropriate for maintaining urinary continence in this case. To evaluate urethral resistance more precisely, urethral pressure profilometry (UPP) has been used in dogs to quantitatively assess sphincter function. 13 However, the feline urethra differs morphologically from that of the dog, particularly in the orientation of the smooth muscle layers, suggesting distinct mechanisms of urethral closure. 14 Recent studies by Cohen et al 15 have demonstrated that UPP and cystometric evaluation can be performed in cats; however, these techniques require specialised equipment and are not yet practical for routine clinical application. In the present case, preoperative functional evaluation of the urethral sphincter was therefore not performed, and urethral plication was planned based on anatomical rather than functional assessment.
This case highlights the practicality and effectiveness of urethral plication as a novel therapeutic option that does not rely on AUS implantation. As a low-invasive and easily managed surgical technique, urethral plication may serve as a first-line option for selected cases of congenital urogenital malformation in cats. Nevertheless, this report describes a single case, and the generalisability of these findings is limited. In addition, age-related changes in sphincter function or hormonal status may influence future urinary control. Therefore, continued follow-up and accumulation of further cases are warranted to validate the long-term efficacy and safety of this approach.
Postoperative contrast imaging of the lower urinary tract was not performed in this case, which limits detailed anatomical assessment of the urethra and distal outflow tract. However, the absence of postoperative lower urinary tract signs and the maintenance of voluntary urination during long-term follow-up suggest that adequate urethral function was preserved after urethral plication.
Conclusions
In this rare feline case of congenital urogenital malformation associated with urinary incontinence, long-term urinary continence was successfully achieved using urethral plication alone, without AUS implantation. In young animals, it is particularly important to avoid the potential risks associated with the placement of foreign materials, such as infection and size mismatch related to growth. Considering these factors, urethral plication was selected as the initial treatment in the present case. Even if urinary control had remained inadequate, subsequent AUS implantation could have been considered; therefore, urethral plication represents a practical and effective first-line treatment option for similar cases.
Footnotes
Acknowledgements
The authors would like to thank all veterinary staff involved in the case management and care of the patient described in this report. Additionally, we would like to express our gratitude to Dr Kakishima for their dedicated care and contribution to this case.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.