
Abstract
Case summary
A 4-month-old castrated male Birman kitten (2.2 kg) presented with a recent history of non-weightbearing lameness in the right hindlimb after blunt trauma. Significant orthopaedic examination findings included instability at the right proximal intertarsal joint level. Radiographic abnormalities included a medial slab fracture of the right calcaneus. Further evaluation with a three-dimensional CT scan revealed a comminuted, intra-articular calcaneal fracture. Images from three-dimensional CT fracture reconstruction were used for surgical planning. Partial tarsal arthrodesis was performed using two 1.1 mm Kirschner wires and a 22 G tension band wire. Additional 24 G cerclage was applied around the distal calcaneus to augment stability. Radiographs at 6 weeks confirmed bone union, and the implants were removed. Nine months after the accident, the cat was fully active with no residual lameness as assessed by the owner.
Relevance and novel information
Calcaneal fractures in cats are rare and surgically challenging, particularly in skeletally immature animals. This report documents successful surgical stabilisation of a traumatic, comminuted calcaneal fracture using CT-guided planning. It highlights the utility of three-dimensional imaging for accurate fracture classification and surgical planning, particularly in an unusual feline orthopaedic case.
Plain language summary
A 4-month-old Birman kitten became lame on its right hindleg after blunt trauma. Examination localised the pain to the hock. Radiographs showed a fracture of the heel bone (calcaneus), but a three-dimensional CT scan could further evaluate the true fracture severity. On CT, the bone was broken into several pieces and the fracture line extended to the joint surface. Surgery was planned using the three-dimensional CT images. The surgeons chose a technique called partial tarsal arthrodesis, where part of the ankle joint is fused to stabilise the joint while preserving hock motion. They used two thin metal pins (Kirschner wires), a tension band wire and a small wire loop. At 6 weeks, new bone growth had united the fragments and the pins were removed. Nine months later, the cat was fully active with no limp, according to the owner. Fractures of the heel bone are uncommon in cats. Repair in this location is difficult because of joint and tendon proximity, and small bone size in cats. This case highlights how three-dimensional CT is valuable in such cases because it evaluates the fracture configuration more accurately than radiographs alone and can be used for surgical planning. The report adds to limited veterinary literature on feline calcaneal fractures by documented CT-guided planning combined with appropriate fixation, leading to a good outcome, even in a very young cat with a complex joint fracture.
Keywords
Introduction
Traumatic calcaneal fractures are rare in cats and management guidelines are limited. 1 Falls or road traffic accidents may cause hindlimb fractures but seldom involve the calcaneus, 2 and large-scale feline fracture studies often omit it.3 –5 Non-traumatic calcaneal fractures due to osteopathy have been identified in cats but are uncommon. 1
Calcaneal fractures often impair common calcaneal tendon function and usually require surgical repair to prevent permanent lameness.6 –8 Surgery aims to realign calcaneal fragments and counteract distraction forces.6,9
Repair techniques include tension-band wiring, lag screws and bone plating. 10 Factors such as fracture configuration, concomitant fractures, ligamentous injury and cost influence decision-making.6,10,11 In immature cats, potential damage to open physes causing growth disturbances requires consideration when planning implant placement. 12
Accurate characterisation of fracture morphology is therefore essential for determining the optimal surgical approach. 13 Three-dimensional CT provides superior visualisation of complex fractures and has guided calcaneal fracture repair in humans. 14
This report describes a kitten with a complex calcaneal fracture where three-dimensional CT imaging was instrumental in delineating the fracture configuration, enabling successful surgical management. The case highlights the clinical value of advanced imaging techniques in managing complex feline orthopaedic injuries.
Case description
A 4-month-old castrated male Birman kitten (weighing 2.2 kg) was referred after sustaining blunt trauma to the hindlimbs when a mirror fell on him. He became acutely non-weightbearing on the right hindlimb (RHL).
The referring veterinarian noted tarsal joint tenderness and a plantigrade stance. Radiographs demonstrated a calcaneal medial slab fracture with proximal intertarsal joint instability (Figure 1). Meloxicam (0.05 mg/kg PO) was administered before transfer.

Preoperative radiographs of the right tarsus: (a) dorsoplantar view and (b) mediolateral view with the hock stressed in dorsiflexion. There is soft tissue swelling around the hock. (a) The calcaneal body shows lateral deviation with an oblique medial slab fracture from the region of the calcaneoquartal joint to the mid-body, proximal to the sustentaculum tali. (b) Dorsiflexion at the proximal intertarsal joint (arrow) indicates plantar-ligament disruption and a possible intra-articular calcaneoquartal joint fracture. The radiolucent calcaneal physis is normal for a 4-month-old kitten
On presentation, orthopaedic examination confirmed non-weightbearing grade 3 lameness of the RHL. 15 The right hock was mildly swollen, with no visible skin damage or bruising. Palpation and manipulation of the tarsal joint evoked a pain response but no crepitus. The kitten was otherwise healthy.
A CT scan (Brilliance Big Bore RT CT Scanner 16 Slice; Phillips Australia) was performed under sedation with medetomidine (10 µg/kg IM) and morphine (0.2 mg/kg IM).
Two-dimensional CT images revealed a complex calcaneal fracture (Figure 2). Three-dimensional reconstruction provided superior delineation of the comminuted medial slab fracture and intra-articular calcaneoquartal component (Figures 3 and 4). Dorsal subluxation of the distal calcaneus was evident at the calcaneoquartal joint. Fracture lines extended through the calcaneal base both medially and laterally. Medially, an undisplaced slab fracture involved the sustentaculum tali anchored to the talus via talocalcaneal ligaments. Laterally, an incomplete fracture extended proximally from the calcaneoquartal joint into the plantarolateral calcaneal base. The calcaneal body was angulated and displaced laterally, widening the calcaneal sulcus within the sinus tarsi but the talocalcaneal articulations remained congruent. Manipulation of the limb under sedation confirmed proximal intertarsal joint instability.

Two-dimensional CT images of the right tarsal joint. (a) Sagittal views show fracture lines through the calcaneal body. (b) Coronal views show lateral displacement of the main calcaneal body and inclusion of the sustentaculum tali in the medial fragment, which remains aligned with the talus. (c) Axial views confirm lateral translation of the calcaneal body
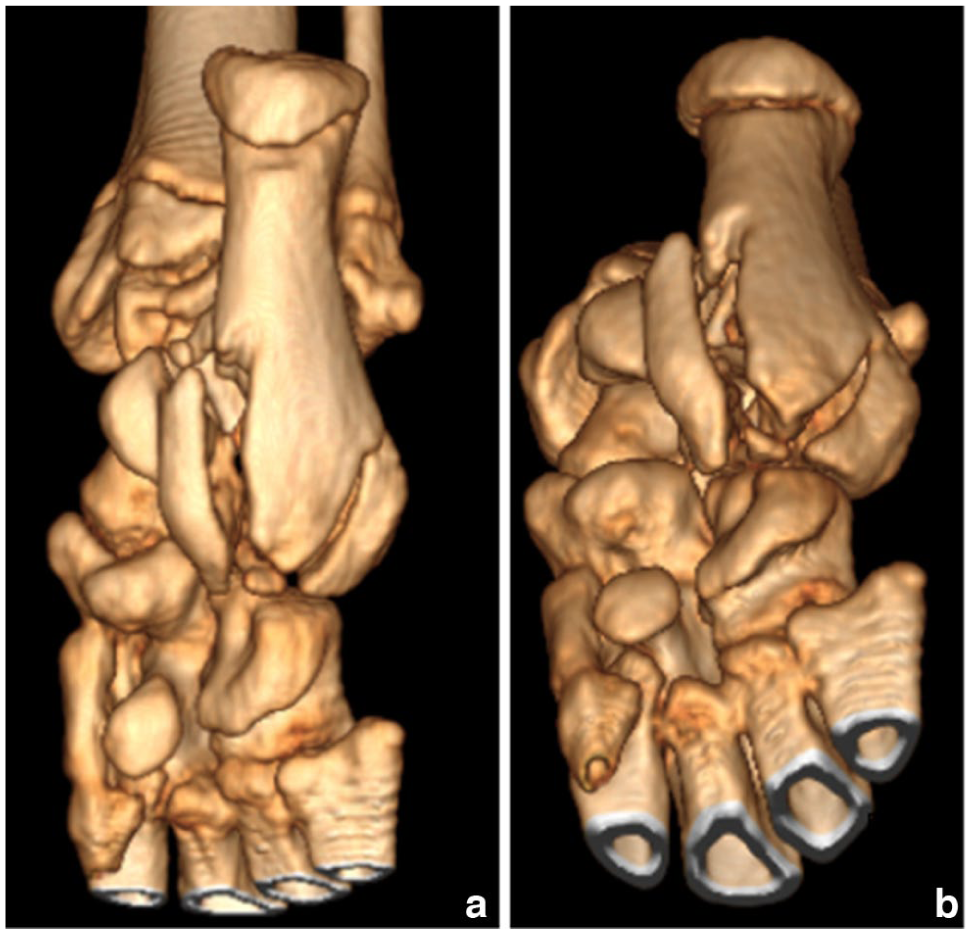
Three-dimensional CT reconstructions of the right calcaneal fracture: (a) plantar and (b) plantar-oblique views. A comminuted intra-articular fracture is seen at the calcaneoquartal joint. The main calcaneal body is deviated laterally by unopposed traction of the common calcaneal tendon and associated ligaments. The medial slab fracture incorporates the sustentaculum tali

Three-dimensional CT reconstructions of the right calcaneal fracture: (a) medial, (b) lateral and (c) dorsal views. (a) The medial slab fracture is undisplaced, with intact anterior and middle talocalcaneal joints (facies articularis talaris media and distalis). (b) The fracture extends into the proximal talocalcaneal articulation (facies articularis talaris dorsalis) but joint congruency is preserved. (c) The calcaneal sulcus is widened within the sinus tarsi; the calcaneal body is displaced laterally with dorsal subluxation at the facies articularis cuboidae and an intra-articular calcaneoquartal fracture
Surgical stabilisation was performed the following day. Open reduction and internal fixation were achieved via a lateral approach. 16 With the patient in sternal recumbency and the RHL extended caudally, a skin incision was made lateral to the common calcaneal tendon extending from proximal to the tuber calcanei to the fourth tarsal bone (T4). Soft tissues were reflected to expose the deep calcaneal fascia, which was incised lateral to the superficial digital flexor muscle and lateral retinaculum, exposing the calcaneus. The superficial digital flexor tendon (SDFT) was medially reflected.
The major calcaneal fragments were anatomically realigned using point-to-point bone-reduction forceps. Two 1.1 mm × 230 mm stainless steel Kirschner (K)-wires (IMEX) were inserted normograde through the calcaneal tuberosity. The lateral K-wire was advanced normograde through the body of the calcaneus and T4 into metatarsal V. The medial K-wire was placed caudal to the first, extending through T4 into metatarsal III.
A figure-of-eight tension-band construct using 22 G cerclage wire (IMEX) was applied and secured with two tightening twists. The proximal loop was positioned cranially over both K-wires and the distal loop passed through an osseous tunnel drilled through T4. The K-wires were bent caudally and cut short.
An additional 24 G cerclage wire was passed obliquely around the calcaneal body from the dorsodistal to mid-plantar calcaneus, maintaining reduction of the calcaneal body to the medial fragment and resisting rotational and shear forces (Figure 5).

Immediate postoperative (a) dorsoplantar and (b) mediolateral radiographs of the right tarsus after calcaneal fracture repair. Kirschner (K)-wires extend from the calcaneal tuberosity, through the calcaneal body, fourth tarsal bone and the proximal ends of metatarsals V and III. The calcaneoquartal joint is now congruent. The calcaneal body has been realigned with the medial fragment. The proximal ends of the K-wires are bent caudally. The plantar figure-of-eight tension band wire and additional oblique cerclage wire around the distal to mid calcaneus, running dorso-distal to plantar-medial, can be seen
The wound was closed in three layers with 4-0 poliglecaprone 25 (Monocryl Ethicon) in simple continuous, continuous subcutaneous and intradermal patterns. No perioperative antibiotics were administered. A soft padded bandage (removed after 5 days) and Elizabethan collar were applied. Postoperative analgesia included meloxicam (0.1 mg/kg SC, then 0.05 mg/kg PO q24h for 3 days).
The kitten was discharged 2 days postoperatively with instructions for 4 weeks of crate confinement, then 2 weeks indoors and Elizabethan collar for 6 weeks prophylactically in case of implant irritation triggering self-trauma.
At the 6-week follow-up, the incision was well healed and both tarsal joints were stable on manipulation. Right hock dorsiflexion was 25° less than the left hock (40° and 15°, respectively). There was a mild lameness of the RHL that resolved after several steps. These findings were attributed to transient joint stiffness from reduced activity. Radiographs under general anaesthesia confirmed calcaneoquartal joint congruency, correct calcaneal alignment and bridging callus formation (Figure 6).

Six-week postoperative (a) dorsoplantar-oblique, (b) dorsoplantar and (c) mediolateral radiographs of the right tarsus after calcaneal fracture repair. Soft tissue swelling has resolved. There is no periosteal reaction suggestive of infection. The position of the Kirschner wires is unchanged, the calcaneal body maintains correct anatomical alignment and the calcaneoquartal joint articulation remains congruent. Bridging callus formation (arrow) is evident between the calcaneal body and the medial fragment. The radiolucent line indicating an open calcaneal physis is not seen
While the cat was anaesthetised, the K-wires and tension-band wire knots were removed via two small incisions: one over the calcaneal tubercle for K-wire removal, and laterally over the calcaneal body to access the tension-band knots. The cerclage twists were gripped low down with wire twisters and further twisted until they broke off flush with the underlying bone and were removed. The remaining wire was left in situ. The skin was closed with 2-0 polydioxanone (PDS Ethicon) in a simple interrupted pattern. Lidocaine (0.5 ml SC) was administered locally and meloxicam (0.05 mg/kg PO q24h for 6 days) prescribed for postoperative analgesia. An Elizabethan collar was maintained until skin suture removal at 14 days, with restricted activity for 2 weeks.
Nine months after the accident, the owner, contacted by telephone, reported the cat was fully active with no lameness.
Discussion
This case describes the successful surgical management of a traumatic calcaneal fracture in a skeletally immature young cat, planned using three-dimensional CT reconstruction.
In humans, calcaneal fractures represent approximately 1% of all fractures, 17 typically from feet-first falls. Cats that fall from heights tend to land with flexed limbs or horizontally. 18 High-rise syndrome (HRS) describes the typical injury pattern in cats after falling two or more storeys. Although hindlimb long bone fractures are common in HRS, tarsal fractures are rare, often involving the talus19,20 or an unspecified tarsal bone.21 –24 In the largest published HRS study, 977 cases revealed 50 unspecified tarsal fractures and 19 tarsal dislocations, only one of which involved a calcaneal articulation. 24
In small animals, calcaneal fractures are often stress-related and may be classified as fatigue or insufficiency types. 25 Fatigue fractures predominate in racing Greyhounds from repetitive tarsal loading,11,26 whereas insufficiency-type fractures have been attributed to trauma of unknown origin. 1 In cats with patellar fracture and dental anomaly syndrome (PADS), approximately 5% of non-patellar fractures involve the calcaneus. 27
Despite the atypical signalment in this case, it was considered important to exclude an early presentation of PADS, 28 which would have influenced owner counselling regarding the risks of further fractures. 27 No typical PADS features (sclerotic margins, persistent deciduous teeth) were present. The history and the comminuted fracture configuration supported a traumatic aetiology.
There are diagnostic challenges posed by the complex anatomy of the tarsus. Although radiographs can demonstrate the presence of a tarsal bone fracture, the severity may be underestimated 29 and superimposed bones can obscure small fracture lines.30,31 Additional views or contralateral comparisons may help 32 but may not improve diagnostic sensitivity. 31 Such diagnostic limitations can result in inadequate treatment and long-term morbidity. 13
In this case, radiographs identified a single fracture line whereas a two-dimensional CT scan revealed comminution. Three-dimensional reconstruction enabled full identification of the fracture configuration and extent of intra-articular involvement. Such imaging affords spatial orientation and is recommended for orthopaedic surgery planning in small animals. 33 Most modern CT units include software for three-dimensional reconstruction without additional costs or radiation exposure. 14
Calcaneal fracture repair in cats and non-racing dogs carries high complication risks due to suboptimal reduction or implant issues. 1 Surgical goals include restoring articular congruency, counteracting common calcaneal tendon traction and avoiding implant-caused irritation.10,11,28 Here, an intra-articular chip at the calcaneoquartal joint was not reconstructable; therefore, partial tarsal arthrodesis was chosen to preserve hock motion while ensuring stability. 34
Additional complexity arose from the patient’s age. Physeal damage in skeletally immature cats can cause growth deformities. 35 In cats, the physis between the calcaneal apophysis and tuber is radiographically visible as a radiolucent line until fusion, 12 typically at 30–52 weeks of age, 36 but may be influenced by genetic or hormonal factors.37,38 This physis was apparent preoperatively, but was not visible 6 weeks postoperatively. It is unknown whether this was due to the radiographic misalignment, early closure due to surgical trauma or normal physiological variation. 37
Bone debridement is usually performed to facilitate ankylosis. 9 However, minimal to no debridement in low-motion joints such as the tarsometatarsal joints has been demonstrated to still result in bone bridging. 39 In this case, no debridement was performed.
The AO (Arbeitsgemeinschaft für Osteosynthesefragen) principles emphasise anatomical reduction and stable fixation of articular fractures. 16 However, this was prohibited by the comminuted nature of the fracture. Since the talocrural joint was unaffected, a partial tarsal arthrodesis of the calcaneoquartal joint using K-wires and a tension band wire was performed. The plantar approach allowed accurate realignment of the calcaneoquartal joint and calcaneal fragments, while K-wires provided longitudinal stability. 10 Plate fixation was avoided because of small bone dimensions and limited screw purchase. Normally, the proximal ends of the K-wires in this repair are bent cranially flush over the calcaneal tuberosity to reduce irritation of the SDFT.8,10 In this case, the wires were bent at a distance from the bone to avoid compression of the growing calcaneus; therefore, caudal bending was chosen to minimise SDFT irritation in this position.
The figure-of-eight tension-band construct counteracted tensile forces from the common calcaneal tendon. 9 An oblique cerclage wire further stabilised the medial and lateral fragments against rotational and shear forces. Although two cerclages are often recommended, 10 the stability achieved with a single wire was sufficient.
Overall, the combination of detailed three-dimensional imaging, surgical stabilisation and careful postoperative management led to a successful medium-term outcome.
Conclusions
To the authors’ knowledge, this is the first reported case describing successful surgical management of a traumatic calcaneal fracture in a kitten using three-dimensional CT-guided planning. This case highlights the diagnostic value of CT, particularly three-dimensional reconstruction, in accurately defining fracture morphology and guiding optimal surgical strategy. Even in skeletally immature patients, this approach can result in excellent functional outcomes.
Footnotes
Acknowledgements
The authors would like to thank the Massey University Veterinary Teaching Hospital radiology team for acquiring and reviewing the three-dimensional CT images (Nikki Moffat, Theresa Hardisty and Dr Paul Whiteman) and Vets4Pets New Plymouth for the preoperative radiographs.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedures(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.