
Abstract
Case summary
A 6-year-old castrated male domestic shorthair cat was evaluated for recurrent pleural effusion, atrial fibrillation and suspected congestive heart failure. During thoracocentesis, the fenestrated over-the-needle catheter became fractured and a catheter fragment remained in the patient’s left pleural space. Later in the course of treatment, the patient acutely decompensated and was euthanized. There were no immediately observed complications associated with the retained catheter fragment.
Relevance and novel information
To the authors’ knowledge, there are no reports of over-the-needle catheter fractures with retained pleural catheter fragments in veterinary medicine. Similar cases in humans have been successfully managed with and without removal of catheter fragments. In veterinary medicine, the decision to attempt removal of a catheter fragment must consider both the likelihood of related morbidity and the patient’s ability to tolerate an invasive procedure.
Keywords
Introduction
Pleural space disease causes hypoxemia and dyspnea by restricting lung inflation and decreasing tidal volume and functional residual capacity. Thoracocentesis is performed to stabilize patients with respiratory distress and obtain fluid samples to aid in diagnosis. 1 The procedure is carried out using a hypodermic needle or over-the-needle catheter and can be performed blindly at an anatomic window or using ultrasound guidance. Complications associated with thoracocentesis include pneumothorax, hemothorax, re-expansion pulmonary edema, vagal events, infection and equipment failure, such as kinking or fracture of the catheter. Though complications can occur, they are infrequent and often clinically insignificant.2,3
Catheter fracture is a rare complication associated with catheter-based procedures. Sporadic reports have described device fractures and emboli, most commonly with vascular catheters in human and veterinary medicine.4,5 Pleural catheter fracture has also been documented in human patients.2,6 To the authors’ knowledge, there are no documented cases of intrathoracic catheter fracture during thoracocentesis in veterinary species. The goal of this report is to describe a case of fenestrated over-the-needle catheter fracture during thoracocentesis in a cat and to summarize the available literature to aid decision-making for cases with similar complications.
Case description
A 6-year-old castrated male domestic shorthair cat, weighing 4.7 kg, was presented to the emergency service for evaluation of respiratory distress and pleural effusion. Before referral, the patient was diagnosed with pleural effusion and therapeutic thoracocentesis was performed three times using an unknown technique. Cytologic analysis was consistent with chylous effusion, although triglyceride and cholesterol concentrations were not measured. No neoplastic cells were identified. A point-of-care feline proBNP test (SNAP Feline proBNP Test; IDEXX Laboratories) was abnormal, no abnormalities were present on a complete blood count, and a serum biochemical panel demonstrated hyperglycemia (193 mg/dl, reference interval [RI] 70–150 ml/dl; 10.7 mmol/l, RI 3.9–8.3 mmol/l). No abnormal heart sounds on auscultation were documented. On the day of presentation, the patient was evaluated by an emergency veterinarian who administered clopidogrel 4 mg/kg PO, pimobendan 0.27 mg/kg PO and gabapentin 10.6 mg/kg PO, and furosemide 1.9 mg/kg IV to treat suspected congestive heart failure.
On presentation, the patient was tachypneic (54 breaths/min) with increased respiratory effort. The heart rate was normal (200 beats/min) upon arrival, then became markedly increased to 330 beats/min shortly thereafter. Heart and lung sounds were muffled, but there were no other abnormalities on examination. Point-of-care ultrasound confirmed moderate bilateral pleural effusion with soft tissue stranding and an estimated left atrial to aorta diameter ratio of 3:1. An electrocardiogram (ECG) confirmed atrial fibrillation. The patient was placed on oxygen, administered pimobendan 0.27 mg/kg PO and diltiazem 1.6 mg/kg PO, and furosemide 1.1 mg/kg IV.
After hospital admission, it was elected to perform thoracocentesis to improve radiographic evaluation of the heart and pulmonary parenchyma. The patient was sedated with butorphanol 0.42 mg/kg IV and alfaxalone 2.1 mg/kg IM. Supplemental oxygen was provided. Throughout the procedure, ECG and pulse oximetry monitoring demonstrated atrial fibrillation and an oxygen saturation of 100%, respectively. After confirming the site of maximal depth of effusion with ultrasound, the left hemithorax was prepared in an aseptic manner.
A local anesthetic block using lidocaine was performed and a 2 mm skin incision was made with a #11 scalpel blade. The first thoracocentesis attempt was performed with a 16 g × 7.5 cm fenestrated catheter (Fenestrated centesis catheter; Mila International) using a routine technique, allowing removal of only 15 ml of chylous fluid. After confirming that moderate effusion remained at the site, a second attempt was made using a new 16 g fenestrated catheter, removing 5 ml of fluid. The catheter was removed without resistance; however, it was noted to be fractured, with an irregular distal margin. Body wall palpation did not identify any foreign material within the subcutaneous tissues. As a result of the persistent ultrasonographic evidence of moderate-volume effusion, a 20 g non-fenestrated catheter was utilized for a third attempt, but was unsuccessful. No attempts were performed with direct ultrasound guidance. Further attempts at thoracocentesis were discontinued since the patient’s respiratory effort was only mildly increased, having improved after sedation.
Three-view thoracic radiographs were taken using a routine technique (Figure 1). In the ventrodorsal view, an intact fenestrated catheter was collimated into view next to the patient to determine its radiopacity. Radiographs confirmed moderate pleural effusion, mild pneumothorax and a 9 mm catheter fragment superimposed with structures in the left caudal thorax. Thoracic radiographs also demonstrated marked cardiomegaly and an unstructured interstitial to alveolar pattern in all lung lobes. The owner was informed about the complication during thoracocentesis and updated with results of diagnostic testing. It was elected to continue treatment for congestive heart failure and atrial fibrillation overnight, with echocardiography and thoracocentesis planned for the next morning. The patient was continued on pimobendan, diltiazem and furosemide therapy, and spironolactone was added.

Thoracic radiographs performed after attempted thoracocentesis. The solid white arrows point to the catheter fragment on the (a) ventrodorsal and (b) right lateral views. The open white arrow demonstrates the intact fenestrated catheter that was placed beside the patient to determine radiodensity
Several hours into hospitalization, the patient developed acute obtundation, vocalization, hypothermia (93.6°F, 34.2°C) and hypotension (Doppler blood pressure 60 mmHg). Owing to the suspected advanced nature of cardiac disease and poor long-term prognosis, the patient was humanely euthanized. A necropsy was declined by the family. A post-mortem thoracic ultrasound (Figure 2 and supplementary material) demonstrated aerated lung tissue and moderate anechoic pleural effusion. Caudal to the tip of the lung tissue, a double-walled, hyperechoic foreign object of approximately the same length as the fractured catheter tip was located within a soft tissue mass, suspected to be fibrin based on its amorphous and mobile nature.
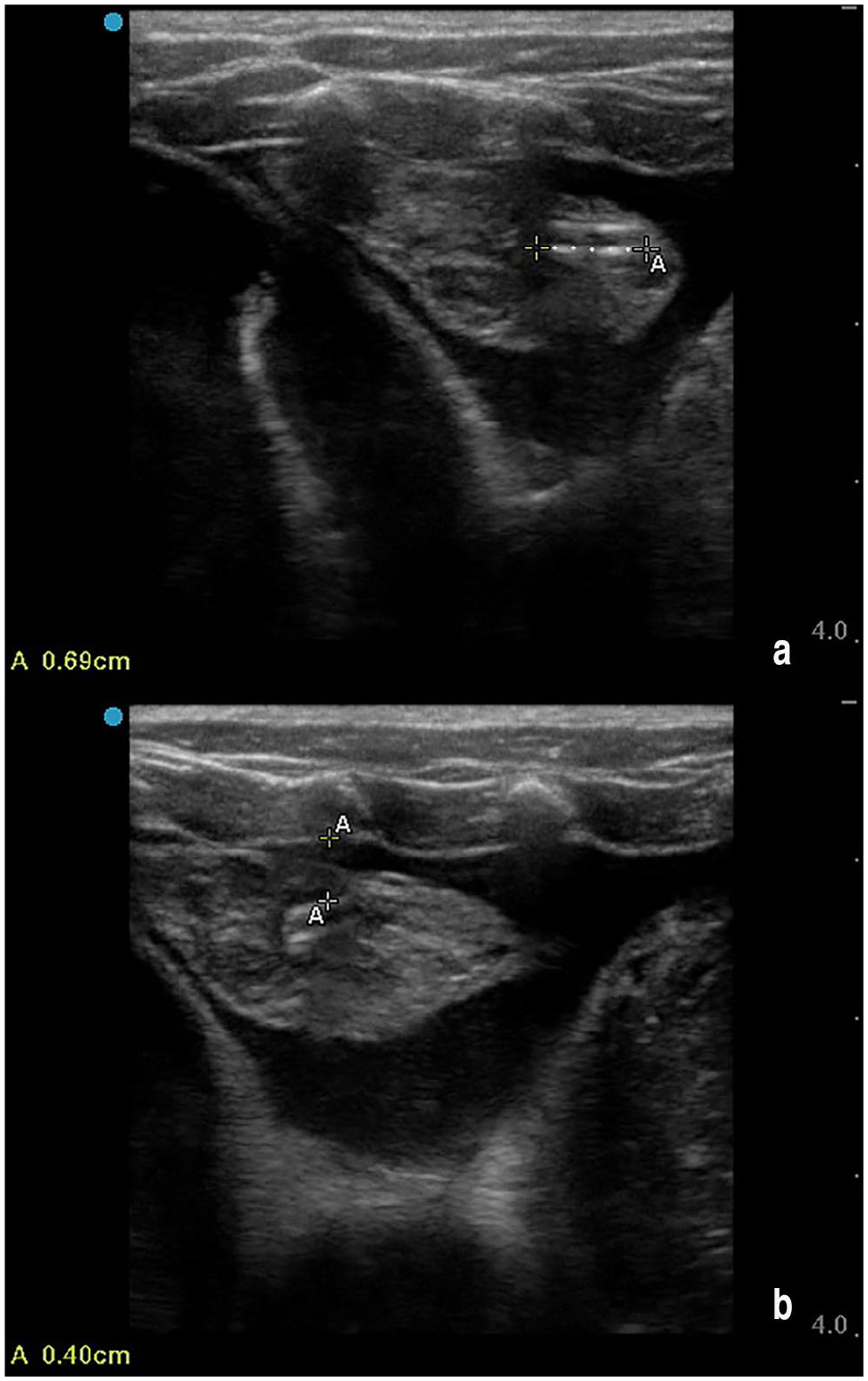
Post-mortem ultrasound images of the left mid-hemithorax. The catheter fragment was identified using point-of-care ultrasound. Measurements were performed to demonstrate (a) the approximate length of the fragmented piece and (b) the approximate distance from the body wall. The catheter fragment was embedded in a soft tissue structure, suspected to be fibrin
Discussion
The use of over-the-needle catheters is ubiquitous in human and veterinary medicine for applications including, but not limited to, vascular catheterization, thoracocentesis, abdominocentesis and epidural injections. Device fracture has been reported with vascular and, less frequently, other applications of over-the-needle catheter use.7 –9 Fracture of the catheter used for thoracocentesis in this patient represents an uncommon complication encountered during a routine procedure. Factors contributing to catheter fracture include improper technique upon insertion or removal of the catheter, or fatigue of catheter materials. 5
The authors hypothesize that the catheter fracture reported here could have occurred for a variety of reasons. The chronicity of the patient’s condition likely led to the development of fibrinous material in the effusion, causing tension on the device during removal and contributing to fracture at a weak point in the catheter. While the thoracocentesis procedure was routine, an inappropriate technique during placement, such as retraction of the catheter onto the stylet, shearing of the catheter with the sharp bevel or forcefully feeding of the catheter into fibrinous material, may have led to device fracture. A manufacturing defect may also have decreased the catheter’s tensile strength. In this case, there was no retraction of the catheter onto the stylet or resistance met on catheter insertion or removal. Based on imaging findings, the device fracture was suspected to be associated with placement into fibrinous material, which increased stress at a weak point in the catheter.
Fractures of over-the-needle catheters placed in venous or arterial sites are well reported in the human and veterinary literature.4,7,8 Although up to 24% of cases involving venous catheter embolization were asymptomatic in a systematic review of human patients, severe complications may result, such as arrhythmias, pain, cough, dyspnea, septicemia, thrombosis and myocardial wall necrosis.4,10 Unlike vascular catheter fragment embolization, the result of a fracture fragment within a body cavity is not easily predicted.
There are no known reports published about intrathoracic fracture of over-the-needle catheters in cats and dogs, despite the discussion of risk. A retrospective study of wire-guided thoracotomy tube use in 156 cats and dogs did not report any introducer catheter or tube fractures. 11 One report describes the fracture of a Jackson-Pratt drain after a cat struggled during its removal from the thoracic cavity. 12 Although the drain fragment was removed surgically in this case, 12 it is unclear if all retained drain fragments must be removed. In humans with intrathoracic device fractures, the majority of patients experience no adverse events; however, pain has been reported.6,13,14
While removal of a vascular foreign object can be accomplished by less invasive techniques, removal of a pleural catheter fragment requires thoracoscopy or thoracotomy. 5 There is presently no standard recommendation for intervention in human patients with fractured intrathoracic catheters, such as indwelling pleural catheters (IPCs), despite the reported incidence of IPC fracture during removal being as high as 17.6%.14,15 An IPC fracture is likely more common because of adhesion formation during prolonged use and the required dissection around the integral cuff, which prevents dislodgment and infection by stimulating tissue ingrowth.14,16 Various techniques have been used in humans, based on patient symptoms, stability and the size of the retained fragment.14,16 Many retained IPC fragments are left in place without long-term complications.6,14 While the literature describing fracture of catheters used temporarily for thoracocentesis is limited, this has been reported in humans.17,18 In these reports, which describe a total of three cases, the fragment was immediately removed using thoracoscopy, removed after 1 week via thoracotomy, and left in the pleural space undisturbed in the respective patients.17,18
When considering treatment for a veterinary patient with an intrathoracic catheter fragment, there is similarly no established standard of care. Reflecting on the mixed evidence in human medicine, patient stability, as well as the size and location of the retained fragment, should be considered when devising a therapeutic plan. If care were continued in this patient, given his comorbidities, retrieval of the fractured device would likely not have been considered unless associated clinical signs were present. It is possible that long-term sequelae would not develop, given the small size and presumed non-pulmonary location of the catheter fragment.
Preventive measures should be prioritized during thoracocentesis. After identifying soft tissue strands throughout the effusion in this case, a needle could have been used as a more durable device. Ultrasound-guided placement of the needle or catheter tip into an area with less flocculent material may have helped avoid contact or obstruction with fibrin. If catheter obstruction occurred during effusion drainage, a small volume of effusion could be reinfused into the thorax to dislodge obstructive material. All attempts at catheter repositioning should be slow and gentle to reduce traction forces on the device.
Although not done in this case, the product manufacturer should be notified when a device failure is suspected. While standard liability clauses relieve the company of damages associated with product failure, notification could lead to removal of defective products from the supply chain and/or inform improvements in manufacturing and quality control. The authors acknowledge this case report is limited by the short duration of patient treatment after catheter fracture and the lack of post-mortem examination to confirm the precise location of the catheter fragment and the presence or absence of associated inflammation or hemorrhage.
Conclusions
This report documents an uncommon complication of thoracocentesis in a cat. The authors suggest that veterinarians faced with a decision to remove an intrathoracic catheter fragment should weigh the benefits of fragment removal against the risks of performing an invasive procedure in a potentially fragile patient.
Footnotes
Acknowledgements
The authors wish to acknowledge Drs Graham Rossi and Sonja Tjostheim who provided consultation in support of the case described here.
Supplementary material
The following file is available as supplementary material: Ultrasound cine loop demonstrating intrathoracic foreign material.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for the procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.