
Abstract
Case summary
A 2-year-old spayed female domestic shorthair cat presented with tetraparesis after being involved in a road traffic accident. Survey spine radiographs revealed a C2–C3 cervical subluxation, which was confirmed by a CT scan. Surgical stabilisation was performed using screws and polymethyl methacrylate (PMMA) via a ventral approach. A postoperative CT scan demonstrated correct implant positioning and good reduction of the subluxation. After surgery, the cat rapidly recovered to a neurologically normal status.
Relevance and novel information
Trauma-induced cervical subluxation is an uncommon occurrence in cats but should be considered in the differential diagnosis. This report describes the surgical management of a C2–C3 cervical subluxation in a cat using screws and PMMA. This is the first case report of a surgically treated subaxial cervical subluxation in a cat.
Case description
A 2-year-old spayed female domestic shorthair cat (weight 5.3 kg) was referred for investigation of tetraparesis 72 h after being involved in a road traffic accident. Immediately after the collision, the cat was presented to an emergency and referral centre with severe neck pain and gait abnormalities. Initially, the cat was stabilised (administration of fluid therapy and analgesics), then the trauma assessment was performed. The AFAST ultrasonography showed no abnormalities and survey spine radiographs revealed a C2–C3 cervical subluxation resulting from the trauma suffered (Figure 1). The referring veterinarian did not observe any improvement in the cat during hospitalisation and the cat was then referred to our hospital.

Lateral radiograph of the cervical vertebral column showing C2–C3 subluxation with dorsal displacement of C3
On neurological examination, mental status was preserved. The cat presented with non-ambulatory tetraparesis, characterised by upper motor neuron (UMN) paresis, and moderate general proprioceptive (GP) ataxia. The UMN paresis was indicated by the preservation of normal spinal reflexes and muscle tone. The GP ataxia was evident through a lack of coordination and decreased postural reactions in all four limbs. Marked cervical hyperaesthesia was noted during gentle manipulation of the neck. Nociception was preserved and cranial nerves were without abnormalities. No additional findings were observed during the physical examination and neurological signs were compatible with an UMN lesion localised to the C1–C5 spinal cord segment.
The blood tests carried out (complete blood count and biochemistry) showed no abnormalities.
Premedication was performed with midazolam (0.2 mg/kg IV) (Midazolam Mylan; Mylan) and induction with alfaxolone (Alfaxan; Zoetis) was given to effect and maintained with isoflurane. Advanced imaging, including a CT scan of the cervical vertebral column, was then performed to confirm the indication for surgical stabilisation and to plan the surgery.
A subluxation of C2–C3 was confirmed, with a mild dorsal dislocation of the C3 vertebral body over C2, without rotation. The angulation between C2 and C3 was measured at an angle of 166° (compared with a normal angle of 180°), causing a slight vertebral misalignment (Figure 2).

Preoperative CT scan of the cervical vertebral column. (a) Sagittal and (b) transverse CT views showing the slight dorsal displacement of C3 in relation to C2, the probable extruded disc material (arrow) and the collapse of the C2–C3 intervertebral space
This subluxation was less marked than on the first survey radiography as a result of the supine position, which aligns the two vertebrae more correctly in relation to each other. In addition, a discrete spinal cord compression was observed at the C2–C3 intervertebral space, likely caused by traumatic disc extrusion (Figure 2).
Informed consent was obtained from the owner before proceeding with the surgical intervention. Preoperative methadone (0.2 mg/kg IV) (Comfortan; Dechra) and prophylactic antibiotics (ampicillin–sulbactam 20 mg/kg IV) (Unacim; Pfizer) were administered. The surgical procedure involved positioning the cat in dorsal recumbency, extending the cervical vertebral column and tying the thoracic limbs in a caudal extended position. A standard ventral approach was performed to reach the C2–C3 vertebral bodies and joint surfaces. Then, three 1.5 mm cortical screws were inserted into the vertebral body of C2, and two 1.5 mm cortical screws into the vertebral body of C3, parallel to the endplates (the two more cranial screws diverged slightly laterally). Pilot holes were drilled and tapped through one cortex for each screw before insertion. The screws were not fully tightened to allow for later stabilisation. Subsequently, to reduce vertebral dislocation, a non-absorbable suture (0 USP monofilament nylon) was tied around the more cranial screw positioned in C3. The cranial portion of C3 was then displaced ventrally by traction on the suture strand. The reduction was maintained, and the vertebrae were stabilised by enveloping the screws in a sleeve of polymethyl methacrylate (PMMA)-based bone cement. In order to avoid thermal damage to the soft tissues, the implant was rinsed with a generous amount of saline solution. Once the cement was consolidated, the suture strand was cut and the tissues were closed layer by layer in a routine manner.
A postoperative CT scan demonstrated correct implant positioning, good alignment of the C2 and C3 vertebrae and resolution of spinal cord compression. In particular, all screws were securely anchored in the vertebral bodies, were monocortical and the spinal canal was not entered (Figure 3). Correct positioning of the implants and reduction of the subluxation were also confirmed using postoperative radiographs (Figure 4).

Postoperative CT of the cervical vertebral column. (a) Sagittal and (b) transverse CT views showing the correct positioning of the screws in the vertebral bodies
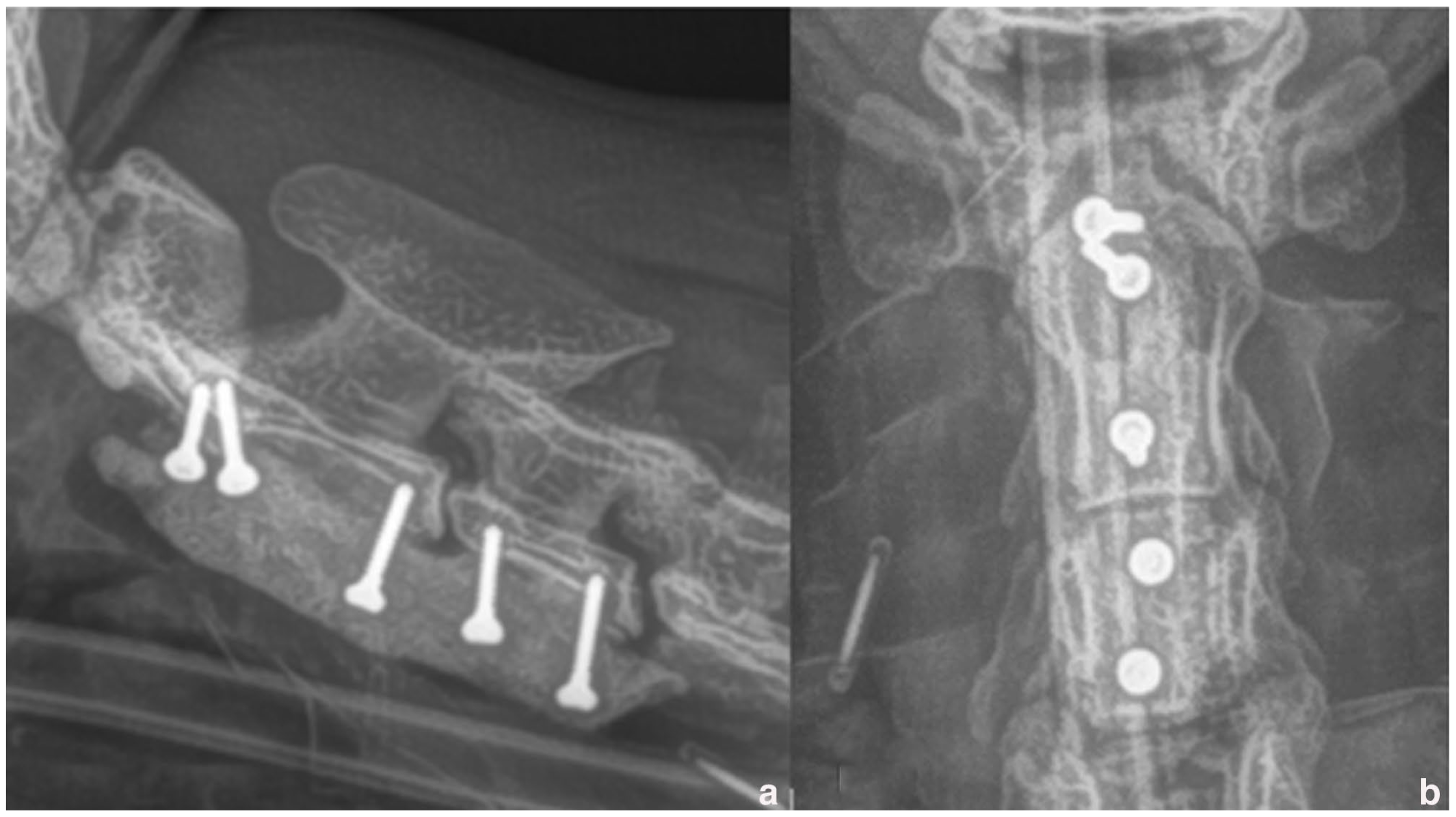
Postoperative radiographs of the cervical vertebral column. (a) Lateral and (b) ventrodorsal views confirming the correct positioning of the implants and reduction of the subluxation
Postoperative analgesia was provided using methadone (0.2 mg/kg IV q4h) (Comfortan; Dechra) and subcutaneous non-steroidal anti-inflammatory drugs (NSAIDs) during hospitalisation and oral NSAIDs for 1 week at home; antibiotics were also continued for 1 week postoperatively. Analgesics were gradually decreased beginning 48 h postoperatively, transitioning from methadone to buprenorphine (20 μg/kg q8h) (Buprecare; Axience). The cat recovered rapidly with progressive improvement in voluntary movement. On the first postoperative day, the cat exhibited cervical pain and voluntary movement but was not ambulatory. On the second day, the cat was ambulatory with difficulty. On the third day, the cat was fully ambulatory with moderate proprioceptive ataxia and no evidence of cervical pain. The cat was discharged on the third postoperative day. Upon discharge, the recommended postoperative care regimen included an 8-week period of room confinement.
The patient was comfortable and neurologically normal when re-examined at 15 days postoperatively. The cat was evaluated by the referring veterinarian at 1 and 2 months postoperatively and was neurologically normal. Radiographs were taken and confirmed proper alignment and stabilisation. As confirmed by further telephone follow-up at 8 months postoperatively, the cat remained neurologically normal and lived a normal life.
Discussion
Vertebral fractures and dislocations are typically caused by major trauma, such as road traffic collisions or falls from great heights. They can occur in any region of the spine, but the thoracolumbar region is most commonly affected.1,2
Injuries to the cervical vertebral column occur less frequently, accounting for approximately 7–20% of all vertebral fractures. 1 These injuries primarily affect young patients involved in road traffic accidents or frontal collisions. In addition, C1 and C2 fractures comprise approximately half of all cervical fractures.3,4 This is likely due to the tendency of vertebral fractures to occur at junctions between relatively dynamic and static regions of the spine, such as the atlantoaxial junction.1,4-6
Approximately 30–83% of cases of vertebral fractures/luxations are associated with other concurrent injuries (pulmonary contusions, pneumothorax, etc).1,2,7 The initial treatment aims to stabilise the patient haemodynamically and to treat the potentially life-threatening lesions. To predict recovery from spinal cord injury, accurate testing for the presence of nociception is crucial.1,2,8,9 Depending on the severity of the neurological signs and the degree of instability/dislocation and compression of the spinal cord, a combination of conservative and surgical treatment is adapted to limit primary and secondary spinal cord injuries; a treatment plan is tailored to the individual case.3,4,8
It is important to note that cervical spine stabilisation surgery is associated with a high perioperative mortality rate (10–36%) due to multifactorial causes,3,10 including respiratory muscle dysfunction and interruption of respiratory feedback mechanisms. 11 These factors must be taken into consideration during cervical spinal surgery.
In this case, we chose surgical stabilisation over external coaptation for several reasons. The severity and nature of the cervical subluxation required a more precise and immediate form of stabilisation, which surgery could provide. In addition, the patient’s overall health status and ability to tolerate surgery were favourable, making it a viable option. External coaptation, while less invasive, was deemed insufficient to provide the necessary stabilisation and alignment in this case.
Cervical fractures/luxations are uncommon in cats. 7 The literature reports two cases of traumatic atlantoaxial subluxation, 12 one case of atlantoaxial instability after trauma and three C2 fractures.4,13 We have not found any previous reports in the literature of cats with a cervical C2–C3 subluxation.
Cervical stabilisation has been previously achieved using a ventral approach with screws and PMMA for atlantoaxial stabilisation,10,14 C2 fractures4,10 and subaxial luxations in dogs. 15 Pins and PMMA have also been used for the stabilisation of two traumatic atlantoaxial luxations in cats. 12 A ventral approach and stabilisation with screws and PMMA were considered in our case to achieve adequate exposure and strong and secure stabilisation. No peri- or postoperative complications were observed.
Approximately 20% of cats with a traumatic spinal cord injury also have disc herniation secondary to the trauma. 9 In our case, disc compression at C2–C3 was detected but was not considered to be significantly responsible for the neurological signs. Therefore, additional spinal decompression surgery, such as a ventral slot, was not performed.
The rapid clinical improvement after surgical reduction and stabilisation of the C2–C3 subluxation confirmed the hypothesis that the clinical signs were caused by vertebral displacement/instability and that the rapidity of the surgical intervention once the patient was stabilised helped to minimise secondary spinal cord damage.
Conclusions
Cervical vertebral subluxations are rare in cats, but they should be considered in the differential diagnosis of cervicalgia and neurological deficits (eg, ataxia, paresis) after a traumatic injury. Surgical stabilisation through a ventral approach, using screws and PMMA, was found to be a safe and viable alternative for treating traumatic cervical subluxation in this case. However, a larger group of patients is necessary to determine the overall safety and efficacy of this surgical option in cats.
Footnotes
Acknowledgements
We would like to thank Hélène Gallois-Bride DVM for the interpretation of images.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or humans individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.