
Abstract
Case summary
A 1-year-old neutered male domestic shorthair cat was referred with suspected uroperitoneum. Ultrasonography showed peritoneal effusion. CT further revealed a bilateral sacroiliac joint disruption associated with an overlapped dislocation of the pubic symphysis, resulting in an abnormal trajectory of the urethra with extramural urethral compression. An open reduction and internal fixation of the pubis with correction of the urethral trajectory was performed under general anaesthesia. The uroperitoneum was determined to originate from a cystocentesis.
Relevance and novel information
This report describes an unusual case of urethral obstruction secondary to overlapping dislocation of the pubic symphysis with urethral entrapment and concurrent bilateral sacroiliac luxation. To the authors’ knowledge, acute urethral obstruction owing to fractures of the pubis, without urethral laceration, has never been described.
Keywords
Case description
A 1-year-old neutered male domestic shorthair cat was referred with suspected uroperitoneum. Two days before referral, the patient had been presented to a veterinary practitioner with signs of dysuria and haematuria evolving into complete anuria. Physiological parameters were reportedly within normal limits. Bruising of the caudal ventral abdomen was the only abnormality noted on physical examination, evoking a possible trauma. After a failed attempt at urethral catheterisation, a cystocentesis was performed for bladder decompression. The patient was hospitalised for fluid therapy and antibiotic and analgesic treatment (clavulanate-potentiated amoxicillin and buprenorphine, respectively). A serum biochemistry profile 24 h after admission showed an azotaemia with elevated creatinine (55.6 mg/l, reference interval [RI] 8–24 mg/l) and blood urea nitrogen (BUN; 2.44 g/l, RI 0.336–0.756 g/l). Focused abdominal sonography for trauma revealed an abundant peritoneal effusion, and the cat was sent to the referral clinic.
On arrival, the patient was bright and responsive. Physiological parameters were within normal limits. An abnormal distension of the abdomen was observed. The orthopaedic examination revealed discomfort on palpation of the pelvis.
Abdominal ultrasonography confirmed the abundant peritoneal effusion and showed a distended urinary bladder with a small fluid-filled round structure in the cranioventral bladder wall consistent with a vesicourachal diverticulum, as well as prepubic urethral dilation.
Cytological examination of the peritoneal fluid revealed a protein-poor transudate, characterised by a mixed inflammatory cell population composed of numerous non-degenerate neutrophilic granulocytes and frequent macrophages. The creatinine concentration of the abdominal effusion (1542 µmol/l) was more than three times that of the plasma (452 µmol/l), which, combined with the history, suggested a uroperitoneum.
Contrast-enhanced abdominopelvic helical CT and positive-contrast retrograde CT urography (Figures 1 and 2) were performed on the day of admission, after patient stabilisation with fluid therapy and analgesics. The patient was premedicated with 0.2 mg/kg methadone and 3 µg/kg medetomidine and induced with propofol to effect. General anaesthesia was maintained with isoflurane in oxygen. Bilateral sacroiliac joint disruptions and an overlapping pubic symphysis dislocation were noted. The left pubic bone was displaced medially and ventrally to the right pubic bone. The CT scan also identified a urethral stenosis ventral to the pubic tubercle, a distended bladder, a marked peritoneal effusion and a prepubic hernia (traumatic rupture on the pubic tubercle) with subsequent eventration of peritoneal fat. CT urography revealed an extramural urethral compression by urethral pinching at the overlap site, and the presence of a discrete leak of contrast agent at the ventral aspect of the bladder, suggesting a breach in this region.
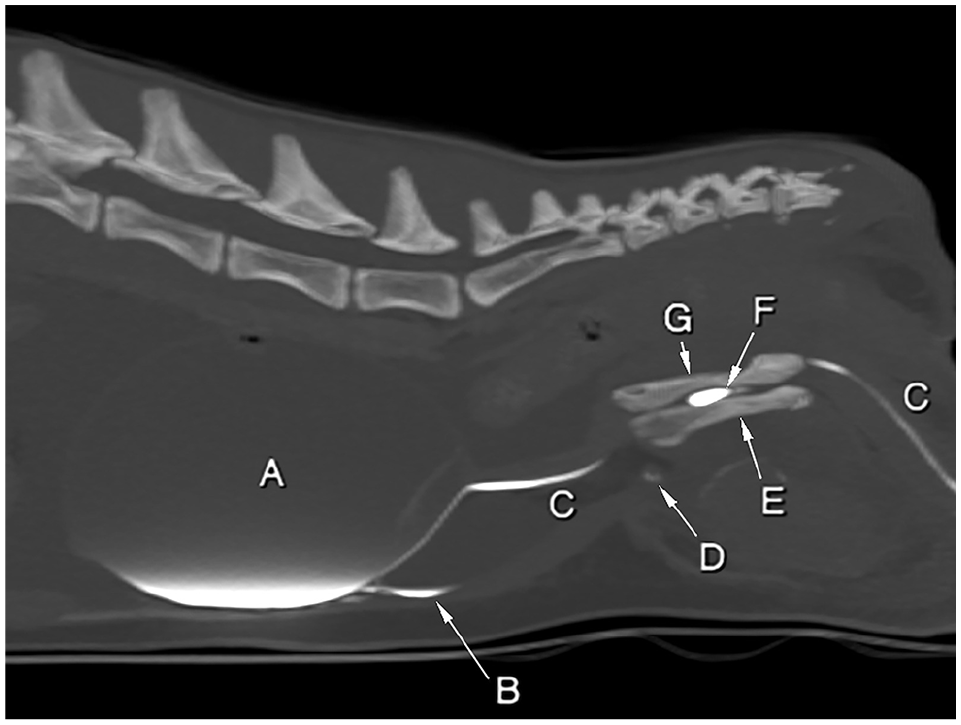
Positive-contrast retrograde urethrography sagittal multiplanar MIP CT reformatted image of the abdomen. WW = 2500, WL = 250. A = urinary bladder; B = free peritoneal contrast medium; C = urethra; D = avulsion fragment of the prepubic tendon; E = left hemipelvis; F = urethral pinching between both hemipelves overlap; G = right hemipelvis. Note the tortuous route of the urethra. MIP = minimum intensity projection; WL = window level; WW = window width
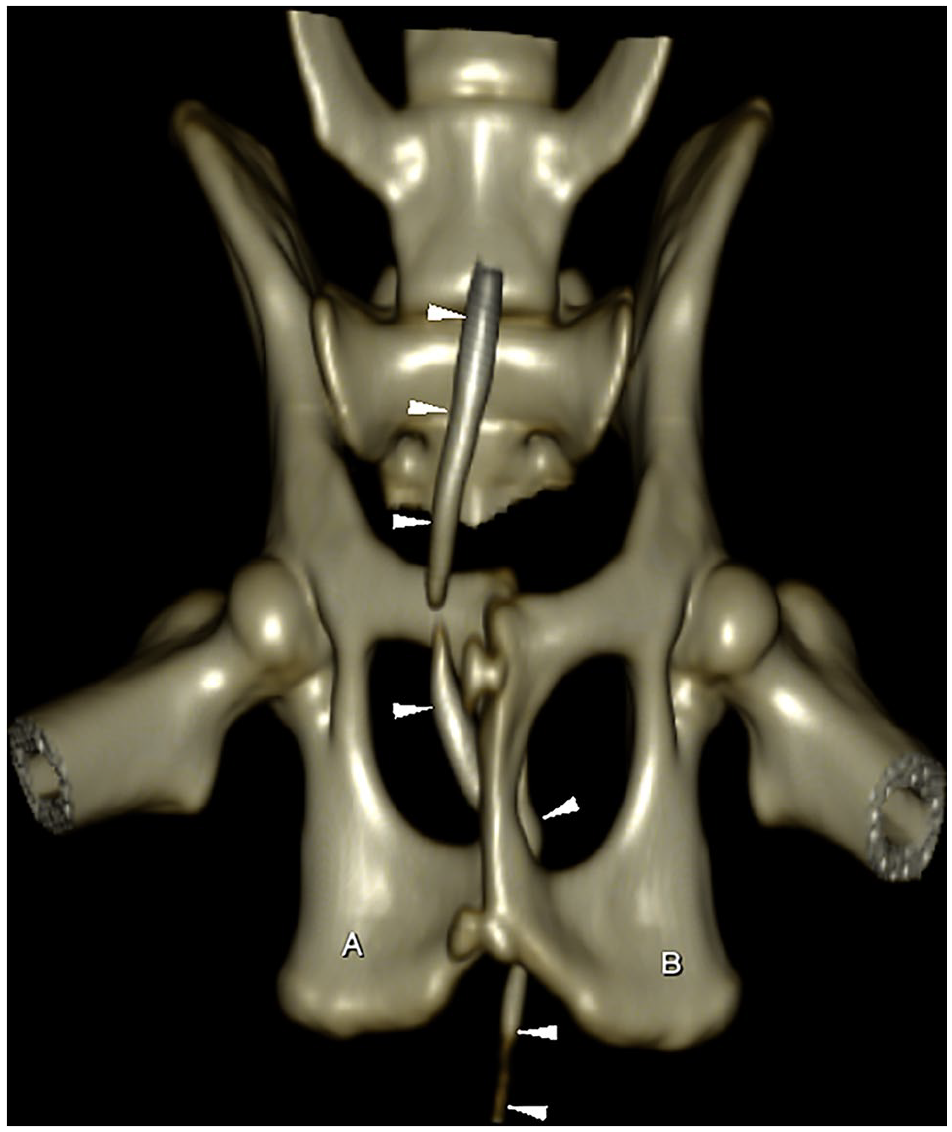
Three-dimensional CT reformatted image of the pelvic region. WW = 255, WL = 127. The urethra (outlined by the arrowheads) is seen passing ventrally to the right pubic bone and dorsally to the left pubic bone where both bony segments overlap, before resuming its normal course caudally. A = right ischiatic table; B = left ischiatic table; WL = window level; WW = window width
Surgery was carried out immediately after CT imaging. A subumbilical coeliotomy was performed extending from the umbilicus to the caudal border of the pubis. One litre of free fluid was aspirated from the abdomen. A punctiform lesion was visualised at the ventral aspect of the apex of the bladder, through which urine leaked (Figure 3). Blunt dissection of the perivesical fat was performed and the proximal portion of the abdominal urethra was observed. Palpation of the pelvic urethra was not possible. The pubis was approached by elevation of the adductor muscles on the left, allowing visualisation of the left pubic bone. The left pubic bone was retracted laterally using a pair of Allis forceps, allowing visualisation of the urethra overlapping the right pubis (Figure 4). The two pubic bones were retracted laterally, which allowed reintegration of the urethra into the pelvic canal. A retrograde leak test was performed using saline, and the urethra appeared to be intact and patent. The pubis was reconstructed using three cerclages of non-absorbable sutures (polypropylene 0) passed through holes predrilled with a 1.5 mm drill bit along the midline of each segment of the pubis. A partial cystectomy including the cystocentesis perforation site and the vesicourachal diverticulum was performed. The cystectomy was closed with a simple continuous suture pattern (glycomer 631 3-0) and augmented with omentum. Abundant abdominal lavage was performed before prepubic hernia repair and routine closure of the abdomen. Holes were predrilled using a 1.5 mm drill bit in the cranial brim of the pubis. Sutures of 2-0 polydioxanone were preplaced through the avulsed portion of the prepubic tendon and through the predrilled holes and tied successively. A urinary catheter with a closed collection system was placed to evaluate urine output in the immediate postoperative period and adapt fluid therapy. No intraoperative complications occurred.

The cystocentesis puncture through which urine leaked can be seen on the ventral aspect of the bladder

The urethra (outlined by the arrowheads and the haemostat) can be seen emerging from the caudal abdomen, passing ventrally to the right pubic bone and dorsally to the left pubic bone (*)
Surgical treatment of the bilateral sacroiliac joint disruptions was not elected by the owner.
Postoperative treatment included fluid therapy, antibiotic (30 mg/kg cefazolin IV q12h) and analgesics (0.3 mg/kg methadone IV q4h).
The urinary catheter was removed the next day, and spontaneous urination was observed. Normalisation of serum creatinine values occurred rapidly after surgery (117 µmol/l 1 day postoperatively and 91 µmol/l 2 days postoperatively, RI 71–159 µmol/l). The patient recovered well from anaesthesia and surgery, and maintained physiological parameters within normal limits. Owing to a high state of stress and limited spontaneous food intake during hospitalisation, the patient was discharged from the hospital 2 days postoperatively. At-home treatment included meloxicam (0.05 mg/kg PO q24h for 5 days) and tramadol (2 mg/kg PO q8h, as needed, for 5 days). Instructions included strict cage rest for 6 weeks and a check-up, including radiography of the pelvis, at 2 months postoperatively (to assess for potential pelvic canal narrowing due to conservative treatment of the bilateral sacroiliac joint disruptions).
At 3 months postoperatively, the owner was satisfied with the recovery and outcome. At 1 year postoperatively, the outcome was still considered satisfactory by the owner, with no evidence of urinary complications.
Discussion
This report describes a case of pelvic fracture with overlapping pubic symphysis dislocation and secondary urethral entrapment, which, in association with bilateral sacroiliac luxation, indicated that surgical repair would be required.
Pelvic fractures are common injuries in dogs and cats, representing 20–30% of all trauma-induced fractures. 1 They are often multiple and frequently associated with extrapelvic skeletal or soft-tissue injuries. 2 In cats, the most common pelvic fractures involve the pelvic floor (occurring in 90% of cases in one study). 2 Pelvic floor fractures may be classified as symphyseal separations, or as unilateral or bilateral fractures of the pubic body and ramus or ischial body. 3 In more than 50% of cats, they are concurrent with unilateral or bilateral sacroiliac luxation or unilateral iliac fractures. 2
Pelvic stenosis is the most common secondary complication, leading to dyschezia and obstipation. 4 Overlapping pubic symphysis dislocation has been described in humans as an uncommon type of pelvic ring injury. The majority of human patients reported are haemodynamically stable; however, 55% present with urethral injuries. In these cases, the urethra is subjected to crushing and shearing forces produced by the overlapping and partial displacement of the pubic bones. 5
In feline medicine, pelvic fractures are also frequently associated with injuries of the urinary tract. 6 Bladder rupture is reported to be the most common soft-tissue injury associated with pelvic fractures. 7 Performing a positive-contrast retrograde urethrocystogram is recommended if free urine is identified within the abdomen or if there is suspicion of urethral trauma. 6 To the author’s knowledge, urethral obstruction owing to fractures of the pubis, without urethral laceration, has never been described.
In this case, the origin of the uroperitoneum was iatrogenic owing to the decompressive cystocentesis and subsequent absence of possible urinary outflow: the pressure in the bladder caused by urethral obstruction prevented healing of the hole created by the needle, thus allowing urine to flow out of the bladder through it.
Decompressive cystocentesis can be recommended in cases of overdistension of the urinary bladder as a result of obstruction to urine flow, when catheterisation of the urethra is not feasible. Extravasation of urine into the peritoneal cavity has been described as a possible rare complication of cystocentesis. 8
Urethral trauma is relatively infrequent in cats and is typically linked to factors such as urethral catheterisation, bite wounds, pelvic fractures, gunshot injuries, blunt abdominal trauma and urolithiasis. Among these causes, vehicular trauma and iatrogenic damage resulting from attempted catheterisation are the most prevalent factors contributing to urethral injuries in cats.9,10
The range of urethral injuries can vary from contusions and lacerations to complete transections, and in severe cases, may involve urethral avulsion from the urinary bladder.11,12
Urethral obstruction is a prevalent condition, representing 4.6% of all feline cases and 8.1% of all male cat cases seen in an emergency setting. 13 Underlying causes reported in cats include idiopathic obstructions (54%), urethral plugs (20%), urolithiasis (20%) and other mechanical obstructions, such as strictures and neoplasia (<5% of cases).14,15 Although pelvic trauma has been associated with urethral rupture and with urethral bruising in the literature, 7 it has not yet been added to the differential diagnosis of acute urinary tract obstruction.
Surgical or conservative treatments are available for the management of sacroiliac luxations in cats. Conservative treatment may be considered in minor luxations with minimal instability, minimal pain, and absence of neurological deficits or pelvic canal narrowing.3,16 Surgery is indicated if there are signs of pain, the cat is non-ambulatory, exhibits severe neurological deficits or severe pelvic canal narrowing, and if concurrent orthopaedic injuries exist.17,18
Bilateral sacroiliac luxation, when associated with pelvic floor fractures, contributes to instability of both hemipelves. In such cases, surgical repair of simple pelvic floor fractures may re-establish or enhance the stability of the pelvic ring and may make reduction of sacroiliac luxation easier, preventing collapse of the pelvic ring. 19 It also allows adequate rotational realignment of both hemipelves, and may avoid the entrapment of soft tissue, such as the urethra in this case, between the bone fragments, and possibly reduce pain during recovery.20,21 In our case, surgical repair of the bilateral sacroiliac luxation was not elected by the owner for financial reasons and because the cat was ambulatory with minimal pain and no neurological deficits, with minimally displaced ilia.
The presence of urinary retention over a duration of several days with multiple cystocenteses and abdominocenteses, and the initiation of preoperative antibiotic therapy, combined with prolonged anaesthetic times, motivated the use of antibiotics for 3 days postoperatively. The authors recognise, however, that a more appropriate antibiotic stewardship would have been to perform a bacterial and culture sensitivity test after lavage of the abdominal cavity, and resume antibiotic therapy only if necessary.
This case report further demonstrates the vital importance of assessing for urinary tract injury during pelvic trauma. If surgical correction of the sacroiliac luxations had been attempted on an undiagnosed urethral entrapment by the pubic bones, urethral injury could have been more severe than the simple compression found in our case.
Conclusions
This report describes an unusual case of urethral obstruction secondary to overlapping dislocation of the pubic symphysis with urethral entrapment and concurrent bilateral sacroiliac luxation. After open reduction and internal fixation of the pubis and correction of the urethral trajectory, the patient showed restored normal urine flow and had a favourable condition without any complications. Urethral obstruction owing to pubic fractures without urethral laceration should be added to the differential diagnosis for lower urinary tract obstruction in the presence of a possible trauma.
Footnotes
Author’s Note
Tiffany Pereira is now affiliated to Southfields Veterinary Specialists, Cranes Point, Gardiners Ln S, Basildon SS14 3AP, UK.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.