
Abstract
Case summary
A 10-year-old male neutered Abyssinian cat was presented with the chief complaint of a right pharyngeal mass. On palpation, the mass was easily palpable; it appeared well demarcated and mobile, and oval in shape. Radiographic examination showed a radiopaque pharyngeal mass, which was revealed to be a well-demarcated mass lesion with a radiopaque marginal area on CT examination. The inside of the mass was uniformly well enhanced on contrast CT examination. A three-dimensional image reconstructed from the CT images strongly suggested that the mass originated from the right stylohyoid bone. No abnormal lesions were observed in the thoracic and abdominal CT examinations. Surgical excision of the mass was scheduled 3 weeks after the first admission. The mass was bluntly separated from the surrounding musculature and resected together with the ipsilateral epihyoid bone adjacent to the mass. Histopathological examination of the resected mass showed neoplastic cells with osteoid formation, and the mass was histopathologically diagnosed as an osteosarcoma. The postoperative recovery from anaesthesia was uneventful, and the cat began feeding on its own from the third postoperative day. The 3-month postoperative CT evaluation revealed no local recurrence or distant metastasis. The cat showed no abnormal findings at the time of writing (6 months postoperatively).
Relevance and novel information
Although osteosarcoma derived from the hyoid bone has rarely been reported in the veterinary field, this report suggests that such tumours may occur in cats. In addition, partial excision of the hyoid apparatus seems to be well tolerated in cats.
Introduction
Neoplastic diseases originating from the hyoid bone are considered extremely rare. Although reports of such diseases in human medicine are quite limited, chondrosarcoma1 –6 and osteochondroma7 –10 of the hyoid bone have been described. In addition, one case of osteosarcoma 11 and one case of osteoblastoma 12 derived from the hyoid bone have been reported. To the best of our knowledge, however, no reports of tumours derived from the hyoid bone in either dogs or cats have been published to date. We encountered a case of osteosarcoma originating from the right stylohyoid bone in a cat. We have reported the clinical features of this case and the results of surgical resection of the tumour, along with a part of the hyoid apparatus.
Case description
A 10-year-old male neutered Abyssinian cat was presented to our veterinary clinic with the chief complaint of a mass lesion in the right pharyngeal region. The owner reported that the cat had started snoring while sleeping approximately 6 months previously, and the owner noticed a mass lesion 2 months before visiting our clinic. The cat had been treated with oral antibiotics at the referring veterinary clinic for 1 week (orbifloxacin, 5 mg/kg q24h; Sumitomo Pharma Animal Health) but the mass did not shrink.
At the first visit to our clinic, the cat was able to lead a normal life with a normal appetite and no dysphagia. The mass was easily palpated in the right pharyngeal region; it appeared well demarcated and mobile, and oval in shape. Radiographic examination of the skull revealed a radiopaque mass lesion approximately 2 cm in diameter in the right pharynx (Figure 1). Thoracic and abdominal radiographic examinations, a complete blood count and a biochemical examination showed no abnormal findings. A CT examination was performed with the cat intubated under general anaesthesia; the anaesthesia was induced by intravenous injection of 1–2 mg/kg of alfaxalone (Alfaxan; Meiji Seika Pharma) and maintained with sevoflurane (Sevofrane; Maruishi Pharmaceutical). The margin of the mass was observed as a radiopaque area showing Hounsfield units similar to those of normal bony tissue (Figure 2a). The inside of the mass showed a uniform soft tissue attenuation on pre-contrast examination with a marked enhancing effect on contrast-enhanced examination (Figure 2b). These CT images were suggestive that the mass was an osteogenic tumour in pharyngeal region. The three-dimensional reconstructed image from the CT images showed that no bony tissue corresponding to the right stylohyoid bone was observed (Figure 2c), suggesting that the mass was derived from the right stylohyoid bone. Fine-needle aspiration with a 23-G needle was performed; however, no useful information could be obtained because of the hard outer wall of the mass. No further invasive biopsies were performed.

Radiograph of the skull of the cat (right lateral view). A radiopaque mass lesion was present in the pharyngeal region (arrow)

CT images of the head of the cat. (a) Before contrast enhancement, the mass was seen to be surrounded by a radiopaque area (arrow), the interior of which exhibited a uniform Hounsfield unit. (b) After contrast administration, a remarkable enhancement effect was observed within the mass (asterisk). (c) Three-dimensional reconstructed image around the mass and hyoid apparatus. A continuous radiopaque mass was seen in the hyoid apparatus. The mass was continuous with the right epihyoid bone (arrowhead), and the ipsilateral stylohyoid bone could not be observed. The arrow indicates a contralateral stylohyoid bone
Three weeks after the first visit, the mass was surgically removed under the same anaesthesia protocol described above. A continuous infusion of dopamine at 5 μg/kg/min (Inovan; Kyowa Kirin) was given to maintain normal blood pressure during surgery. The cat was restrained in a dorsal recumbency, and a paramedian skin incision was made in the laryngopharyngeal region, and the mass was readily identified after blunt dissection of the right hyoglossus and digastric muscles (Figure 3a). The hypoglossal nerve was identified on the mass and was gently separated from the mass. After that, the mass was further separated from the surrounding attached muscle tissues. Intraoperative bleeding was appropriately controlled by an electrical coagulation system (Erbe electrosurgical unit, VIO300D; Medinnova). The mass was found to be attached to the right epihyoid bone (Figure 3b), and the cartilaginous joint between the epihyoid and ceratohyoid bone was sharply cut off with a number 11 scalpel (Figure 3c). The mass was separated from deeper muscles, such as the styloglossus and medial pterygoid muscles, and removed (Figure 3d). Although the surgical removal of the mass was a marginal resection, it appeared that all of the tumour tissue was resected grossly.

Gross findings at the time of surgery. (a) The mass (asterisk) was revealed by blunt dissection of the right hyoglossus and digastric muscles. (b) Further separation of the surrounding attached musculature confirmed bone tissue continuous with the mass (arrow). This bone tissue was considered to be the right epihyoid bone. (c) the connecting surface (arrow) of the epihyoid bone and the ceratohyoid bone was sharply cut to remove the mass. The preserved hypoglossal nerve can be observed in the middle of this image. (d) Macroscopic findings of the excised mass. The arrow indicates a part of the right epihyoid bone continuous with the mass
A single use of intramuscular morphine at 0.1 mg/kg (Takeda Pharmaceutical) was used for postoperative pain management. The postoperative recovery from anaesthesia was uneventful; however, the cat did not show appetite for 2 days and supportive fluid therapy was continued. The cat began feeding on its own from the third postoperative day. The cat initially seemed to take a longer time to swallow food than before the operation, but the food intake thereafter became almost normal and the cat was discharged 5 days postoperatively. The 2-week follow-up revealed no abnormalities.
Histopathological examination of the resected mass revealed that the radiopaque surrounding area confirm-ed by CT examination was relatively well-differentiated bone tissue, possibly a part of the stylohyoid bone (Figure 4a). Inside the mass, spindle-shaped or polygonal tumour cells proliferated in a storiform pattern. The tumour cells had a moderate amount of eosinophilic cytoplasm with indistinct cell boundaries, as well as normochromatic, oval, short spindle and polygonal nuclei showing anisotropy and pleomorphism. The tumour cell nuclei had hyperchromatic or distinct nucleoli. Many thin, irregularly shaped osteoids were also observed around the boundary with the surrounding bone tissue (Figure 4b). Based on these findings, the tumour was diagnosed as an osteosarcoma that had developed inside the hyoid bone and proliferated while pushing the existing bone tissue outward. The tumour mass was resected together with pre-existing bony tissue. The tumour tissue showed partial infiltration into the surrounding bone tissue microscopically; however, no vascular invasion and further invasion beyond the pre-existing bony tissue were observed. Therefore, microscopically, the tumour appeared to have been resected completely. Mitotic figures were rarely observed.
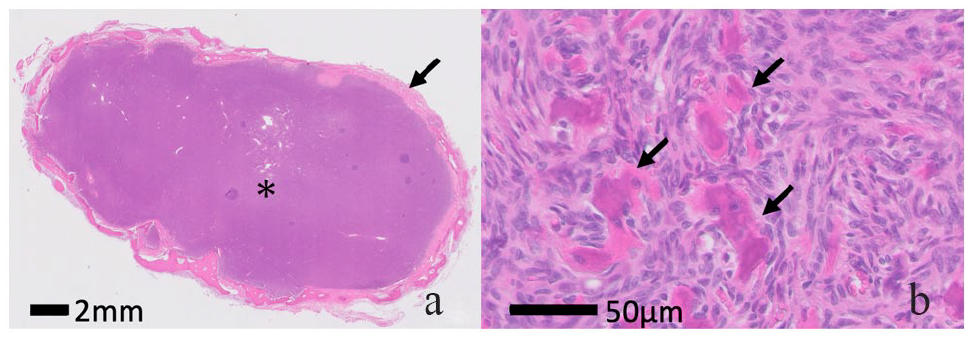
(a) Histopathological findings of the excised mass (haematoxylin and eosin staining [H&E], ×10). Basophilic tumour tissue (asterisk) was observed inside the tumour, and pre-existing bone tissue was observed at the periphery of the tumour (arrow) (H&E, ×400). (b) Spindle-shaped to polygonal tumour cells were found to be proliferating in a storiform pattern. The presence of thin, irregularly shaped osteoids (arrows) was observed
At 3 months postoperatively, the owner reported that the cat had been able to lead a normal life with normal food intake. Follow-up CT examination showed no recurrence at the surgical site and no distant metastatic lesions in the abdominal and thoracic cavities. The cat showed no abnormal findings at the time of writing (6 months postoperatively).
Discussion
The hyoid apparatus is composed of a number of individual bones, and its composition differs slightly depending on the animal species. Basically, the hyoid apparatus attaches to the base of the tongue and also functions as a suspensory mechanism for the tongue and larynx. In cats, the hyoid apparatus consists of the basihyoid bone, which attaches to the base of the tongue, and the bilateral thyrohyoid and ceratohyoid bones, which attach to each end of the basihyoid bone. 13 Furthermore, the epihyoid bone and the stylohyoid bone are connected to the ceratohyoid bone in the dorsal direction.
In this case, histopathological examination revealed that the tumour was an osteosarcoma, suggesting that it had originated in a part of the hyoid apparatus. Based on the combination of the histopathological diagnosis of osteosarcoma and the three-dimensional imaging of the primary tumour tissue, the stylohyoid bone was considered to be the primary lesion site. Primary bone tumours of cats have been considered predisposed to occur in appendicular and axial skeletal sites.14 –17 Axial osteosarcomas have been reported to occur most commonly in the oral cavity and pelvis.14,17 In contrast, reports of primary laryngopharyngeal osteogenic tumours, both in dogs and cats, have been quite limited. Ramírez et al 18 reported a case of myxochondroma derived from larynx; however, no reports of osteosarcoma originating from the hyoid bone in either dogs or cats have been published to date. Even in the field of human medicine, hyoid bone tumours are considered rare, and most are chondrosarcoma1 –6 and osteochondroma.7 –10 Reports of osteosarcoma, as in the present case, are rare, and the only such report was by Anderson and Kearney. 11 In the present case involving a cat, osteosarcoma was definitively diagnosed based on histopathological evidence of tumour cell proliferation accompanied by osteoid formation.
The bone tissue around the mass was relatively normal histopathologically, suggesting that it was part of the stylohyoid bone. It is possible that the tumour cells derived within the stylohyoid bone proliferated while pushing the cortical bone of the hyoid bone outward. Generally, osteosarcoma is considered a typical malignant tumour. 14 In this case, malignant findings such as nuclear atypia and invasive proliferation of the tumour cells were seen in some areas, leading to the definitive diagnosis of a malignant bone tumour. There were also tumour-invasive findings of bone lysis of stylohyoid bone at surgery. However, microscopic evaluation of the surgical margin showed no tumour invasion. In addition, no vascular invasion was observed, and mitotic figures within the tumour tissue were relatively rare histopathologically. Therefore, the degree of tumour malignancy was considered relatively low. Many osteosarcomas grow while destroying normal bone tissue. 14 However, because of the lower malignancy of the tumour tissue in this case, it seemed that the tumour growth pushed the cortical bone outward rather than destroying it.
The right stylohyoid and epihyoid bones were resected in this case. Before surgery, there was concern about disturbances in postoperative food intake. However, no problems developed after the operation or throughout follow-up. Limited information regarding resection of part of the hyoid bone is available in the veterinary field. Lantz and Salisbury 19 and Milovancev et al 20 reported the results of excision of ectopic thyroid cancer that had developed around the hyoid bone in dogs, including resection of part of the hyoid bone apparatus. Regarding surgery for other types of tumours in the laryngopharyngeal region, Ramírez et al 18 reported the surgical resection of cartilaginous tumours derived from larynx of a dog with an uneventful recovery. According to these reports, almost all dogs that underwent surgery showed no severe postoperative problems, suggesting that aggressive surgical resection including part of the hyoid bone may be considered when clinicians encounter malignant tumours involving the hyoid apparatus. Because the number of cases is quite limited, however, definitive conclusions cannot be reached. Further accumulation of more cases is necessary.
In the present case, no local recurrence or lung metastasis was observed 3 months after the operation. Most bone tumours in cats have been considered osteosarcoma and histologically malignant. 14 Although osteosarcomas of cats have been reported to be less metastatic compared with those of dogs,14 –16 Nakano et al 21 recently reported a high metastatic rate of feline appendicular osteosarcomas. At the time of writing (6 months postoperatively), the cat was in good health without surgical complications. However, given that the case involved a malignant bone tumour, careful follow-up is considered necessary in the future.
Conclusions
To the best of our knowledge, this is the first report of osteosarcoma derived from the hyoid bone of a cat. Surgical resection, including part of the hyoid bone, caused no adverse effects and provided a favourable prognosis in this case. Therefore, this is considered a surgical method worth considering in similar cases.
Footnotes
Acknowledgements
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.