
Abstract
Case summary
A 7-year-old male castrated Ragdoll cat was presented for chronic shoulder instability after a previous medial luxation of the right shoulder. Upon examination, there was palpable instability of the glenohumeral joint and an increased abduction angle. Surgical stabilisation was elected due to lameness and instability after closed reduction, rest and medical management. A low-profile bone-anchor and a ligament prosthesis were used to stabilise the glenohumeral joint with minimal disruption to the cat’s natural shoulder stabilisers. Clinical signs resolved after surgery and the cat remained non-symptomatic at the 12-month follow-up.
Relevance and novel information
Feline shoulder luxation is rarely described in the veterinary literature. To the authors’ knowledge, this is the first report describing stabilisation of the glenohumeral joint in a cat using a bone anchor and a ligament prosthesis.
Keywords
Introduction
Shoulder luxation and shoulder instability are rarely reported in cats.1–5 Reports describing shoulder stabilisation for chronic instability after luxation of the glenohumeral joints are scarce. This is the first report of shoulder stabilisation in a cat using a bone anchor and a prosthetic ligament.
Case description
A 7-year-old male castrated Ragdoll cat was referred for chronic right thoracic limb lameness that did not respond to a 2-week course of amoxicillin-clavulanic acid (20 mg/kg PO q12h). There was no definitive history of trauma, but the cat had access to the outdoors.
Examination revealed a right-sided grade 6/6 non-weightbearing thoracic limb lameness with mild adduction of the antebrachium. Methadone (0.3 mg/kg IM) was given before examination and crepitus was palpated during gentle range of motion of the right shoulder. Orthogonal radiographs were performed under intra-venous (IV) general anaesthetic with alfaxalone (2 mg/kg IV) (Figures 1 and 2).

Lateral radiograph of the right-sided medial shoulder luxation

Ventral dorsal radiograph of the right-sided medial shoulder luxation
Medial shoulder luxation was diagnosed, and this was reduced manually under anaesthesia, with traction and lateral pressure on the neck of the scapula. Orthogonal radiographs were repeated to confirm successful closed reduction and no crepitus was detected. The cat was fully weightbearing on the right thoracic limb without lameness the next morning. The cat was discharged with meloxicam (0.05 mg/kg PO q24h) for 7 days and strict cage rest for 8 weeks. Repeated conscious examinations at 1, 3 and 9 weeks after closed reduction were unremarkable and the cat was comfort-able, active and fully weightbearing.
Nineteen months after the original presentation, the cat re-presented for recurrence of right thoracic limb lameness. An orthopaedic examination revealed normal range of motion in all joints, including the right thoracic limb. Toe-touching grade 5/6 right thoracic limb lameness was identified.
General anaesthesia with alfaxalone (2 mg/kg IV) and isoflurane (1.5%) were administered and the cat was placed in lateral recumbency with the elbow extended and the scapular spine parallel to the table. 6 The angle between the right scapular spine and the shaft of the humerus was measured with a goniometric ruler and was determined to be between 55° and 60°. On palpation, significant instability of the right shoulder was identified both medially and laterally. Orthogonal radiographs of the right shoulder revealed medial shoulder instability with no luxation and no evidence of glenoid dysplasia. The cat was therefore diagnosed with medial and lateral shoulder instability.
Surgery to stabilise the right shoulder was performed. The cat was placed in dorsal recumbency. The right thoracic limb was held in abduction with the shaft of the humerus held abducted and parallel to the table. A medial approach to the medial aspect of the glenohumeral joint was performed by a linear incision and blunt dissection in between the pectoralis minor and pectoralis major. The glenohumeral joint capsule was identified with care to protect the brachial plexus and remaining fibres of the medial glenohumeral ligament. A bone anchor and prosthetic ligament (FASTak Suture Anchor; Arthrex) was driven into the medial aspect of the scapular neck, directed proximally away from the joint and centrally towards the spine of the scapula. A bone tunnel was then drilled with a 2.5-mm Kirshner wire, from the craniomedial aspect of the humeral neck, exiting caudolaterally 0.5 cm distal to the margin of the articular cartilage. One strand of the braided ultra-high molecular weight polyethylene suture was passed through the humeral tunnel caudally with the aid of a flexible nitinol suture passer. The suture loop was carefully assessed to avoid entrapment of the suprascapular nerve. The two strands were tightened by hand and secured with five square knots. The right thoracic limb was cycled through a normal range of motion and the glenohumeral joint was deemed to be stable against medial lateral translation. The pectoralis was repaired with 4-0 monofilament polydioxanone suture (PDS II; Ethicon). The subcutaneous layer and dermis were closed with 3-0 monofilament polydioxanone suture (PDS II; Ethicon). Orthogonal postoperative radiographs showed appropriate reduction of the glenohumeral joint, and the bone anchor was well seated into the scapular neck (Figures 3 and 4).

Postoperative mediolateral radiograph depicting the shoulder joint in a physiological position and the suture anchor placement

Postoperative craniocaudal radiograph of the right shoulder joint, depicting the shoulder joint in a physiological position and correct implant placement after joint reduction
On recovery, pain was controlled with buprenorphine (0.02 mg/kg PO q8h) and meloxicam (0.05 mg/kg PO q12h). The cat was weightbearing with no lameness and was discharged with instructions for 2 weeks of cage rest.
Physical examinations at 2, 4 and 12 weeks showed excellent recovery with full range of motion, no palpable instability or lameness. The owner reported an excellent outcome 14 months postoperatively.
A 3D printed replica of a feline shoulder was used to replicate this technique, illustrating the location of the bone anchor and the bone tunnel (Figures 5–7).

The bone anchor was placed in the central medial aspect of the scapular neck and was aimed away from the joint

A craniomedial to caudolateral bone tunnel was made in the humeral neck with a 2.5 mm Kirschner wire 0.5 cm distal to the margin of the articular cartilage
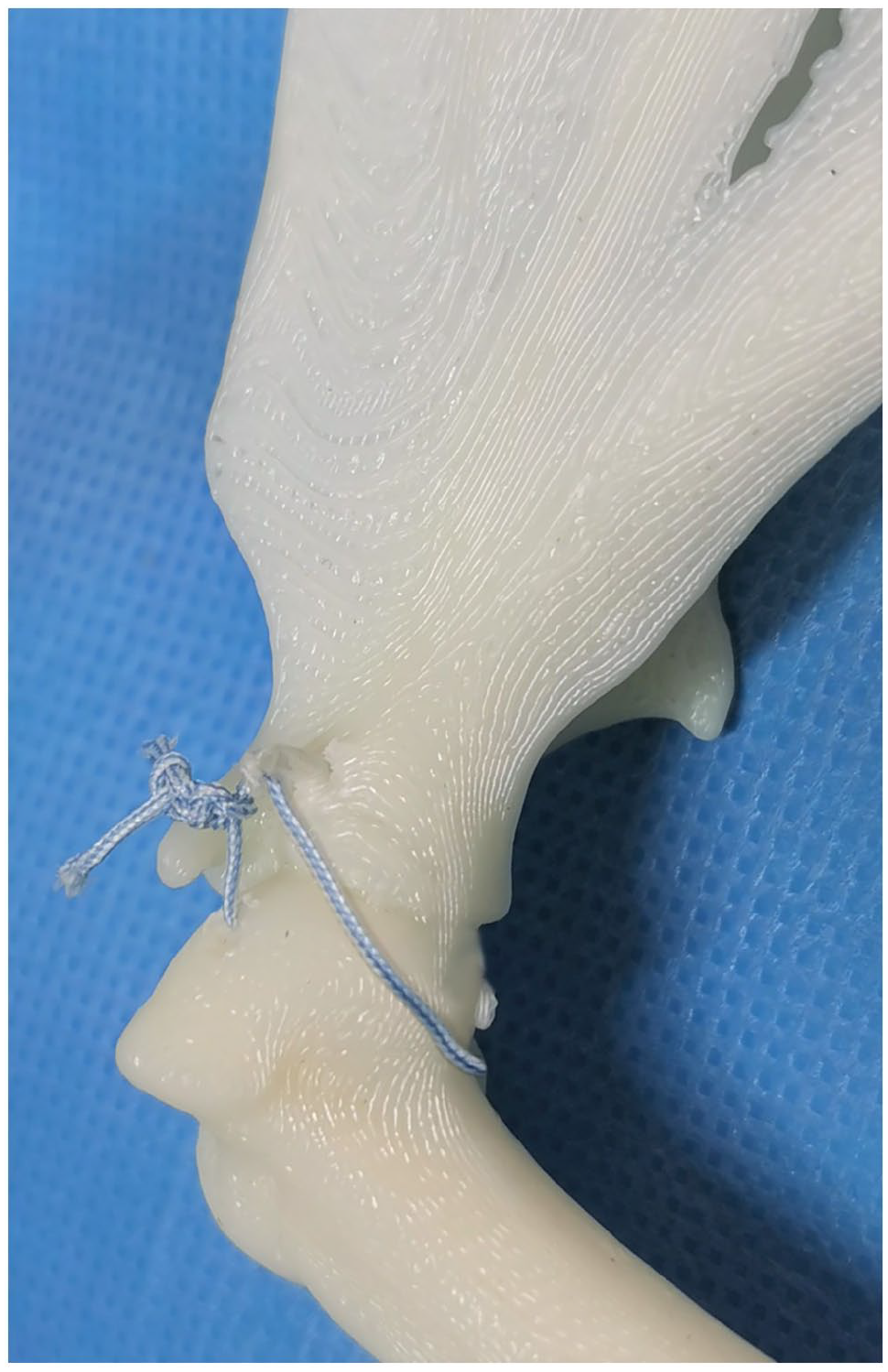
The ligament prosthesis was placed through the bone tunnel and tightened after checking for normal range of motion
Discussion
Feline shoulder luxation is uncommon.1–5 This case report described a new method of shoulder stabilisation in a cat with a history of medial shoulder luxation and subsequent instability. The aim of the surgical repair was to provide sufficient glenohumeral stability.1,2,5,6–9 Stabilisation of the shoulder joint was achieved by using a low-profile bone-anchor and a ligament prosthesis. The benefit of applying this technique was that the placement ligament prothesis mimicked the original course of the ligaments and allowed preservation of normal range of motion of the joint. In addition to stabilisation, the successful outcome may be attributed to the meticulous preservation of the existing shoulder stabilisers and the inverted V configuration prosthetic ligament that served to imitate the two diverging strands of the medial glenohumeral ligament.1,7,10
In cats, shoulder luxation is seen after extensive damage to the stabilising structures. Damage to the medial and lateral glenohumeral ligaments have been shown to significantly destabilise the glenohumeral joint.1,2,5 This may be a result of acute trauma, repetitive microtrauma or degenerative processes.1,5,7–9 The stabilising structures of the shoulder can be divided into passive and active stabilisers. Passive stabilisers consist of the glenoid, joint capsule, labrum, joint fluid cohesion, and medial and lateral glenohumeral ligaments. Active stabilisers include the biceps tendon, infraspinatus, supraspinatus, subscapularis and teres minor.1,2,7,9,11 Together, they counteract translation and avulsion forces through a wide range of motion.1–3,7,11 Therefore, preservation of these structures may reduce morbidity and improve patient outcome.
Treatment options for shoulder luxation in cats are mostly extrapolated from dogs.2,3,4,9 Techniques that involve using existing structures to impart stability include biceps tendon transposition and supraspinatus tendon transfer.6,7,8,12 In dogs, medial transposition of the biceps tendon has been reported with good to excellent outcomes.8,9,12 However, altering the anatomical location of the biceps tendon has been shown to alter the instant centre of rotation, resulting in an increased angle of abduction in comparison with a prosthetic medial glenohumeral ligament. Furthermore, the biceps tendon contributes to passive stability in its original anatomical location and releasing it from the trabecular groove may have negative effects on the congruity of the shoulder joint.7,8 In dogs, biological management options for medial shoulder instability include extracorporeal shockwave therapy, arthroscopic radiofrequency-induced thermocapsulorrhaphy and imbrication of the subscapularis tendon. Stabilisation using prosthetic ligaments can be open or via arthroscopic assistance. The prosthetic ligaments are secured using bone anchors (FASTak Suture Anchor and PushLock Anchor; Arthrex) or a prosthetic ligament combined with a toggle and a suture button (TightRope; Arthrex).10,12–14 Size restrictions and anatomical differences, such as smaller joint space and greater tubercle, may preclude the use of some of these techniques in cats.
The impact of glenohumeral luxation and instability in the cat is poorly understood. Progressive lameness, muscle atrophy and degenerative joint disease can develop if the joint is not stabilised surgically.1,6,9 Since shoulder luxation in the cat is more commonly associated with major destabilising trauma than degenerative processes, stabilisation surgery is preferred to conservative management.2,9 In this case, the cat was clinically affected by significant medial and lateral shoulder instability, despite closed reduction and conservative management.
The diagnosis of shoulder instability in cats is uncommon but can be readily made by thorough clinical examination and the measurement of abduction angles. While there are no established normal ranges of shoulder abduction angles in the cat, comparison with the intact contralateral shoulder joint aids in making a diagnosis. A cadaveric study of the feline shoulder joint reported a mean angle of abduction of 37° ± 9° in a normal shoulder. This angle increased significantly to 82° ± 20° when the medial glenohumeral ligament was fully transected. 2 This suggested that increased abduction angles are associated with the loss of vital medial shoulder stabilisers in cats.
A low-profile bone anchor with one craniocaudal bone tunnel was used in this case to minimise surgical trauma to the shoulder stabilisers and dissection around the suprascapular nerve. However, the reliance on multifilament prosthetic ligament replacement may result in a higher infection rate.5,7,11 Nevertheless, wound infection was not observed in this case at the 1-year follow-up.
The present study has some limitations. Radiographs were not repeated at the follow-up examination as the cat was clinically well with no lameness observed. The angle of abduction was also not measured at the follow-up examinations. CT was not performed to exclude mild glenoid dysplasia. The integrity of the biceps tendon, subscapularis tendon and glenohumeral ligaments could be better assessed with MRI or arthroscopy before surgical planning. Furthermore, the use of sutures in the bone tunnel as an anchoring mechanism may cause a widening of the bone tunnel and is commonly seen in the first 4–6 weeks postoperatively. However, the clinical impact of bone tunnel enlargement is not well established, hence the implications in this surgery are unknown.15,16 Lastly, being a single case report, extrapolation of the outcome cannot be reliably made. Further studies with increased case numbers and comparison with other methods of shoulder stabilisation would be required to determine the validity of this method.
Conclusions
A bone anchor and prosthetic ligament were successful in conferring stability for a cat with a history of should-er luxation and subsequent shoulder instability. No further luxation or lameness was noted at the 12-month follow-up.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (either prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.